Vitamin D Intake and Serum 25-Hydroxyvitamin D Levels in Korean Adults: Analysis of the 2009 Korea National Health and Nutrition Examination Survey (KNHANES IV-3) Using a Newly Established Vitamin D Database

Abstract
:1. Introduction
2. Results
2.1. General Characteristics
2.2. Energy and Vitamin D Intake and Serum 25(OH)D Concentrations
2.3. Food Sources of Vitamin D
3. Discussion
4. Materials and Methods
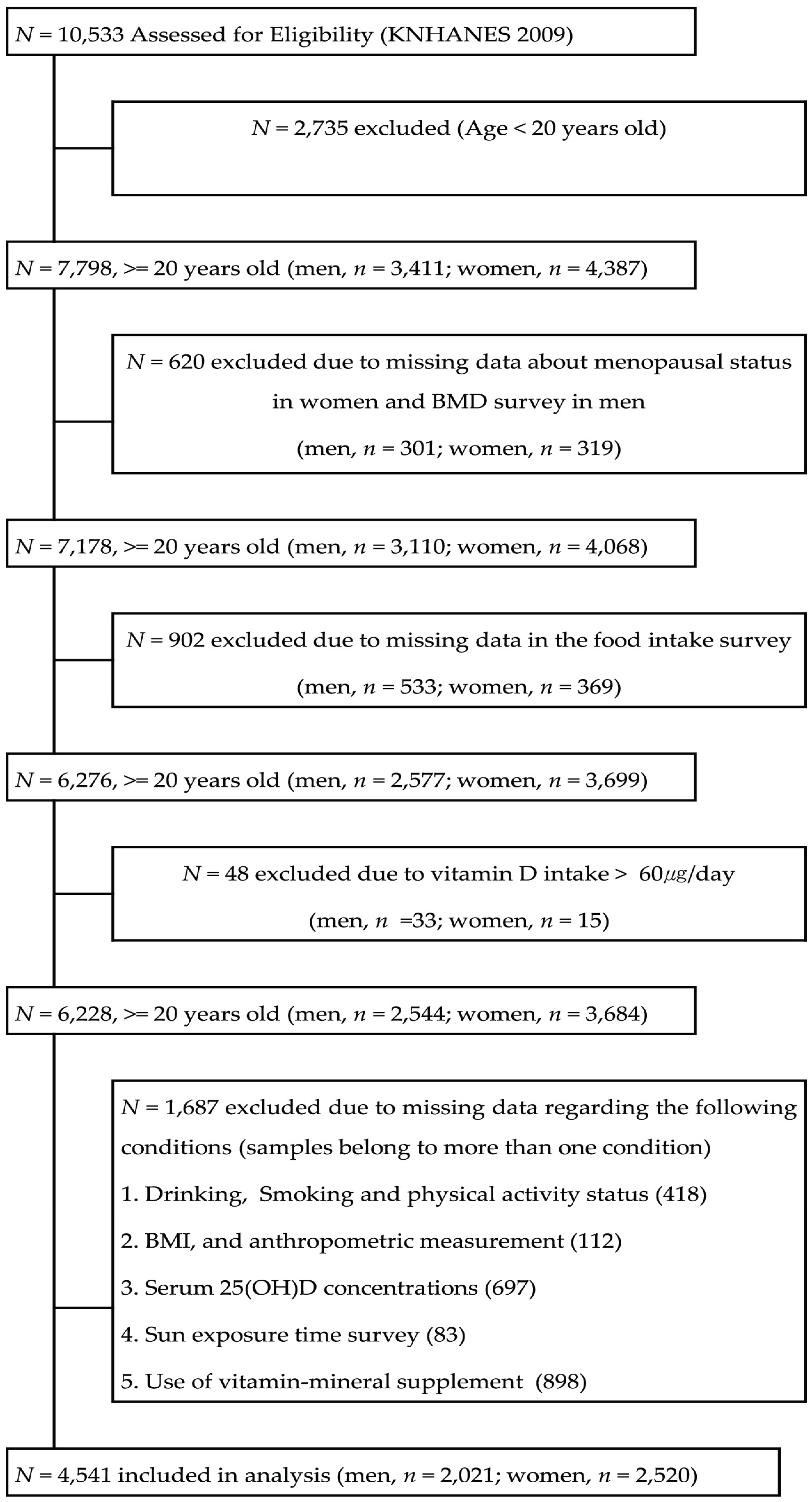
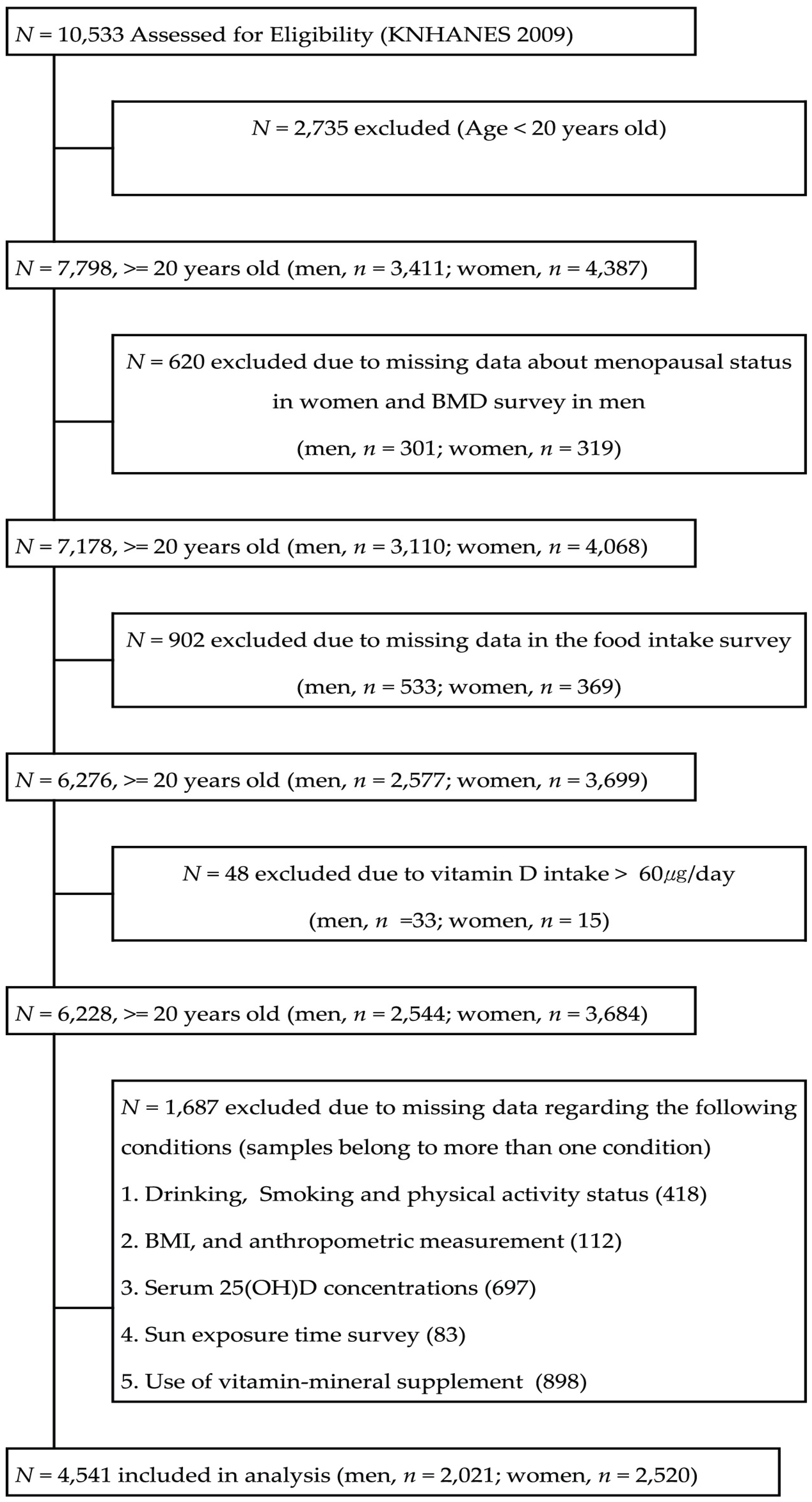
4.1. Study Data and Design
4.2. Vitamin D Database
4.3. General Characteristics
4.4. Energy and Vitamin D Intake, Main Food Source of Vitamin D, and Serum 25(0H)D Concentrations
4.5. Statistical Analyses
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Forman, J.P.; Giovannucci, E.; Holmes, M.D.; Bischoff-Ferrari, H.A.; Tworoger, S.S.; Willett, W.C.; Curhan, G.C. Plasma 25-hydroxyvitamin D levels and risk of incident hypertension. Hypertension 2007, 49, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am. J. Clin. Nutr. 2004, 80, 1678S–1688S. [Google Scholar] [PubMed]
- Wang, T.J.; Pencina, M.J.; Booth, S.L.; Jacques, P.F.; Ingelsson, E.; Lanier, K.; Benjamin, E.J.; D’Agostino, R.B.; Wolf, M.; Vasan, R.S. Vitamin D deficiency and risk of cardiovascular disease. Circulation 2008, 117, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Chiu, K.C.; Chu, A.; Go, V.L.; Saad, M.F. Hypovitaminosis D is associated with insulin resistance and beta cell dysfunction. Am. J. Clin. Nutr. 2004, 79, 820–825. [Google Scholar] [PubMed]
- Grant, W.B. An estimate of the global reduction in mortality rates through doubling vitamin D levels. Eur. J. Clin. Nutr. 2011, 65, 1016–1026. [Google Scholar] [CrossRef] [PubMed]
- Armas, L.A.; Dowell, S.; Akhter, M.; Duthuluru, S.; Huerter, C.; Hollis, B.W.; Lund, R.; Heaney, R.P. Ultraviolet-B radiation increases serum 25-hydroxyvitamin D levels: The effect of UVB dose and skin color. J. Am. Acad. Dermatol. 2007, 57, 588–593. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.J.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; Kovacs, C.S.; et al. IOM committee members respond to endocrine society vitamin D guideline. J. Clin. Endocrinol. Metab. 2012, 97, 1146–1152. [Google Scholar] [CrossRef] [PubMed]
- Weaver, C.M.; Fleet, J.C. Vitamin D requirements: Current and future. Am. J. Clin. Nutr. 2004, 80, 1735S–1739S. [Google Scholar] [PubMed]
- Henry, H.L.; Bouillon, R.; Norman, A.W.; Gallagher, J.C.; Lips, P.; Heaney, R.P.; Vieth, R.; Pettifor, J.M.; Dawson-Hughes, B.; Lamberg-Allardt, C.J.; et al. 14th vitamin D workshop consensus on vitamin D nutritional guidelines. J. Steroid Biochem. Mol. Biol. 2010, 121, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Van Schoor, N.M.; Lips, P. Worldwide vitamin D status. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Mithal, A.; Wahl, D.A.; Bonjour, J.P.; Burckhardt, P.; Dawson-Hughes, B.; Eisman, J.A.; El-Hajj Fuleihan, G.; Josse, R.G.; Lips, P.; Morales-Torres, J. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos. Int. 2009, 20, 1807–1820. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.S.; Oh, H.J.; Choi, H.; Choi, W.H.; Kim, J.G.; Kim, K.M.; Kim, K.J.; Rhee, Y.; Lim, S.K. Vitamin D insufficiency in Korea—A greater threat to younger generation: The Korea National Health and Nutrition Examination Survey (KNHANES) 2008. J. Clin. Endocrinol. Metab. 2011, 96, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Flicker, L.; Mead, K.; MacInnis, R.J.; Nowson, C.; Scherer, S.; Stein, M.S.; Thomasx, J.; Hopper, J.L.; Wark, J.D. Serum vitamin D and falls in older women in residential care in Australia. J. Am. Geriatr. Soc. 2003, 51, 1533–1538. [Google Scholar] [CrossRef] [PubMed]
- Portela, M.L.; Monico, A.; Barahona, A.; Dupraz, H.; Sol Gonzales-Chaves, M.M.; Zeni, S.N. Comparative 25-OH-vitamin D level in institutionalized women older than 65 years from two cities in Spain and Argentina having a similar solar radiation index. Nutrition 2010, 26, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Nanri, A.; Foo, L.H.; Nakamura, K.; Hori, A.; Poudel-Tandukar, K.; Matsushita, Y.; Mizoue, T. Serum 25-hydroxyvitamin D concentrations and season-specific correlates in Japanese adults. J. Epidemiol. 2011, 21, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Harnack, L.J.; Steffen, L.; Zhou, X.; Luepker, R.V. Trends in vitamin D intake from food sources among adults in the Minneapolis-St Paul, MN, Metropolitan area, 1980–1982 through 2007–2009. J. Am. Diet. Assoc. 2011, 111, 1329–1334. [Google Scholar] [CrossRef] [PubMed]
- Lamberg-Allardt, C.; Brustad, M.; Meyer, H.E.; Steingrimsdottir, L. Vitamin D—A systematic literature review for the 5th edition of the Nordic Nutrition Recommendations. Food Nutr. Res. 2013, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health Labour and Welfare. Health Japan 21 (the Second Term) Analysis and Assessment Project. Available online: http://www.mhlw.go.jp/seisakunitsuite/bunya/kenkou_iryou/kenkou/kenkounippon21/en/eiyouchousa/kekka_eiyou_chousa.html (accessed on 2 August 2016).
- National Diet and Nutrition Survey: Results from Years 1 to 4 (Combined) of the Rolling Programme for 2008 and 2009 to 2011 and 2012. Available online: https://www.gov.uk/government/statistics/national-diet-and-nutrition-survey-results-from-years-1-to-4-combined-of-the-rolling-programme-for-2008-and-2009-to-2011-and-2012 (accessed on 2 August 2016).
- Fisberg, R.M.; Marchioni, D.M.; Castro, M.A.; Verly, E., Jr.; Araujo, M.C.; Bezerra, I.N.; Pereira, R.A.; Sichieri, R. Inadequate nutrient intake among the Brazilian elderly: National Dietary Survey 2008–2009. Rev. Saude Publica 2013, 47, 222S–230S. [Google Scholar] [CrossRef] [PubMed]
- Jungert, A.; Spinneker, A.; Nagel, A.; Neuhauser-Berthold, M. Dietary intake and main food sources of vitamin D as a function of age, sex, vitamin D status, body composition, and income in an elderly German cohort. Food Nutr. Res. 2014, 58, 23632. [Google Scholar] [CrossRef] [PubMed]
- Lips, P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: Consequences for bone loss and fractures and therapeutic implications. Endocr. Rev. 2001, 22, 477–501. [Google Scholar] [CrossRef] [PubMed]
- Avenell, A.; Gillespie, W.J.; Gillespie, L.D.; O’Connell, D. Vitamin D and vitamin D analogues for preventing fractures associated with involutional and post-menopausal osteoporosis. Cochrane Database Syst. Rev. 2009, 20, Cd000227. [Google Scholar]
- Suzuki, Y.; Maruyama-Nagao, A.; Sakuraba, K.; Kawai, S. Erratum to: Milk fortified with vitamin D could reduce the prevalence of vitamin D deficiency among Japanese female college students. Arch. Osteoporos. 2015, 10, 18. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.E.; Dangour, A.D.; Tedstone, A.E.; Chalabi, Z. Does fortification of staple foods improve vitamin D intakes and status of groups at risk of deficiency? A United Kingdom modeling study. Am. J. Clin. Nutr. 2015, 102, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Biancuzzo, R.M.; Young, A.; Bibuld, D.; Cai, M.H.; Winter, M.R.; Klein, E.K.; Ameri, A.; Reitz, R.; Salameh, W.; Chen, T.C.; et al. Fortification of orange juice with vitamin D(2) or vitamin D(3) is as effective as an oral supplement in maintaining vitamin D status in adults. Am. J. Clin. Nutr. 2010, 91, 1621–1626. [Google Scholar] [CrossRef] [PubMed]
- Laaksi, I.T.; Ruohola, J.P.; Ylikomi, T.J.; Auvinen, A.; Haataja, R.I.; Pihlajamaki, H.K.; Tuohimaa, P.J. Vitamin D fortification as public health policy: Significant improvement in vitamin D status in young Ffinnish men. Eur. J. Clin. Nutr. 2006, 60, 1035–1038. [Google Scholar] [CrossRef] [PubMed]
- MacLaughlin, J.; Holick, M.F. Aging decreases the capacity of human skin to produce vitamin D3. J. Clin. Investig. 1985, 76, 1536–1538. [Google Scholar] [CrossRef] [PubMed]
- Chailurkit, L.O.; Aekplakorn, W.; Ongphiphadhanakul, B. Regional variation and determinants of vitamin D status in sunshine-abundant Thailand. BMC Public Health 2011, 11, 853. [Google Scholar] [CrossRef] [PubMed]
- Black, L.J.; Seamans, K.M.; Cashman, K.D.; Kiely, M. An updated systematic review and meta-analysis of the efficacy of vitamin D food fortification. J. Nutr. 2012, 142, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Cranney, A.; Horsley, T.; O’Donnell, S.; Weiler, H.; Puil, L.; Ooi, D.; Atkinson, S.; Ward, L.; Moher, D.; Hanley, D.; et al. Effectiveness and safety of vitamin D in relation to bone health. Evid. Rep. Technol. Assess (Full Rep.) 2007, 1–235. [Google Scholar]
- Cashman, K.D.; Fitzgerald, A.P.; Kiely, M.; Seamans, K.M. A systematic review and meta-regression analysis of the vitamin D intake-serum 25-hydroxyvitamin D relationship to inform European recommendations. Br. J. Nutr. 2011, 106, 1638–1648. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.M.; Jonnalagadda, S.S.; Albertson, A.M.; Joshi, N.A.; Weaver, C.M. Top food sources contributing to vitamin D intake and the association of ready-to-eat cereal and breakfast consumption habits to vitamin D intake in Canadians and United States Americans. J. Food Sci. 2012, 77, H170–H175. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, L.; Stepien, M.; Gibney, M.J.; Nugent, A.P.; Brennan, L. The potential role of vitamin D enhanced foods in improving vitamin D status. Nutrients 2011, 3, 1023–1041. [Google Scholar] [CrossRef] [PubMed]
- Pietinen, P.; Paturi, M.; Reinivuo, H.; Tapanainen, H.; Valsta, L.M. Findiet 2007 survey: Energy and nutrient intakes. Public Health Nutr. 2010, 13, 920–924. [Google Scholar] [CrossRef] [PubMed]
- Burgaz, A.; Akesson, A.; Oster, A.; Michaelsson, K.; Wolk, A. Associations of diet, supplement use, and ultraviolet B radiation exposure with vitamin D status in Swedish women during winter. Am. J. Clin. Nutr. 2007, 86, 1399–1404. [Google Scholar] [PubMed]
- Nakamura, K.; Nashimoto, M.; Hori, Y.; Yamamoto, M. Serum 25-hydroxyvitamin D concentrations and related dietary factors in peri- and postmenopausal Japanese women. Am. J. Clin. Nutr. 2000, 71, 1161–1165. [Google Scholar] [PubMed]
- Spiro, A.; Buttriss, J.L. Vitamin D: An overview of vitamin D status and intake in Europe. Nutr. Bull. 2014, 39, 322–350. [Google Scholar] [CrossRef] [PubMed]
- ANSES-French Agency for Food Environmental and Occupational Health and Safety. Vitamin D-Presentation, Food Sources and Nutritional Needs. Available online: http://www.anses.fr/en/content/vitamin-d (accessed on 2 August 2016).
- Serra-Majem, L.; Ribas-Barba, L.; Salvador, G.; Jover, L.; Raido, B.; Ngo, J.; Plasencia, A. Trends in energy and nutrient intake and risk of inadequate intakes in Catalonia, Spain (1992–2003). Public Health Nutr. 2007, 10, 1354–1367. [Google Scholar] [CrossRef] [PubMed]
- Kenkyukai, K.E.J. The National Health and Nutrition Survey in Japan; Daiichi-shuppan: Tokyo, Japan, 2010. [Google Scholar]
- Nakamura, K.; Nashimoto, M.; Okuda, Y.; Ota, T.; Yamamoto, M. Fish as a major source of vitamin D in the Japanese diet. Nutrition 2002, 18, 415–416. [Google Scholar] [CrossRef]
- Goulding, A.; Taylor, R.W.; Keil, D.; Gold, E.; Lewis-Barned, N.J.; Williams, S.M. Lactose malabsorption and rate of bone loss in older women. Age Ageing 1999, 28, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Labour and Welfare. Dietary Reference Intakes for Japaneses. Available online: http://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/Overview.pdf (accessed on 2 August 2016).
- Lai, J.K.; Lucas, R.M.; Banks, E.; Ponsonby, A.L. Variability in vitamin D assays impairs clinical assessment of vitamin D status. Intern. Med. J. 2012, 42, 43–50. [Google Scholar] [CrossRef] [PubMed]
- The Korean Nutrition Society. Food Values; The Korean Nutrition Society: Seoul, Korea, 2009. [Google Scholar]
- National Rural Living Science Institute, R.D.A. Food Composition Table; National Rural Living Science Institute, R.D.A: Seoul, Korea, 2006.
- National Academy of Agriculture Science, R.D.A. Functional Food Composition Table; National Academy of Agriculture Science, R.D.A: Seoul, Korea, 2009.
- Hostani, N. Standard Tables of Food Composition in Japan; Japan Association of Training Colleges for Cooks: Tokyo, Japan, 2004. [Google Scholar]
- U.S. Department of Agriculture. USDA Food Composition Databases. Available online: https://ndb.nal.usda.gov/ndb/nutrients/report/nutrientsfrm?max=25&offset=0&totCount=0&nutrient1=328&nutrient2=&nutrient3=&subset=0&sort=c&measureby=g (accessed on 27 November 2015).
- Dawson-Hughes, B.; Heaney, R.P.; Holick, M.F.; Lips, P.; Meunier, P.J.; Vieth, R. Estimates of optimal vitamin D status. Osteoporos. Int. 2005, 16, 713–716. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Total | Men | Women | X2-Value |
|---|---|---|---|---|
| (n = 4541) | (n = 2021) | (n = 2520) | ||
| Smoking: Yes | 28.1 (995) | 47.0 (864) | 5.9 (131) | 943.75 *** |
| Drinking: Yes | 59.8 (2434) | 75.9 (1467) | 41.0 (967) | 569.64 *** |
| Physical activity (high) *:, Yes | 18.9 (773) | 22.1 (412) | 15.2 (361) | 34.36 *** |
| Physical activity (mod.) *: Yes | 14.4 (678) | 15.3 (314) | 13.3 (364) | 3.41 |
| Physical activity (walking) *: Yes | 45.6 (2062) | 46.8 (972) | 44.2 (1090) | 3.13 |
| Sun exposure time, >5 h | 25.7 (1320) | 34.0 (796) | 16.1 (524) | 188.32 *** |
| Vitamin/mineral supplements: Yes | 20.4 (923) | 17.1 (335) | 24.3 (588) | 35.476 *** |
| Gender | Age (Years (n)) | Energy Intake (kcal/Day) | Vitamin D Intake (µg/Day) | AI (µg) | Less than AI (% (n)) | Serum 25(OH)D (ng/mL) | 25(OH)D Deficiency Ratio (% (n)) | |
|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted for Energy | |||||||
| Men | 20–29 (281) | 2380.76 ± 63.94 | 3.72 ± 0.42 | 3.67 ± 0.41 | 5 | 80.1 (225) | 16.43 ± 0.50 | 76.8 (208) |
| 30–49 (798) | 2455.26 ± 31.62 | 4.72 ± 0.28 | 4.59 ± 0.28 | 5 | 74.6 (595) | 18.76 ± 0.39 | 64.2 (496) | |
| 50–64 (555) | 2238.57 ± 41.07 | 4.29 ± 0.33 | 4.42 ± 0.33 | 10 | 90.5 (502) | 20.92 ± 0.40 | 48.7 (257) | |
| 65–74 (290) | 1970.43 ± 60.34 | 3.70 ± 0.35 | 4.17 ± 0.33 | 10 | 90.3 (262) | 21.16 ± 0.55 | 49.0 (133) | |
| ≥75 (97) | 1719.45 ± 70.69 | 2.38 ± 0.43 | 3.16 ± 0.49 | 10 | 95.9 (93) | 21.65 ± 0.80 | 40.9 (39) | |
| Total (2021) | 2152.89 ± 28.03 | 3.76 ± 0.19 | 4.00 ± 0.17 | 19.78 ± 0.33 | 61.8 (1133) | |||
| F-value | 30.149 *** | 6.270 *** | 2.376 | 23.522 *** | ||||
| Women | 20–29 (298) | 1724.42 ± 50.40 | 2.48 ± 0.17 | 2.42 ± 0.17 | 5 | 86.6 (258) | 14.71 ± 0.35 | 86.1 (258) |
| 30–49 (1074) | 1703.78 ± 20.37 | 3.02 ± 0.15 | 2.98 ± 0.15 | 5 | 84.5 (907) | 16.07 ± 0.28 | 78.8 (829) | |
| 50–64 (666) | 1655.69 ± 30.78 | 2.97 ± 0.24 | 2.97 ± 0.23 | 10 | 93.8 (625) | 17.92 ± 0.29 | 67.7 (441) | |
| 65–74 (350) | 1435.24 ± 34.18 | 2.25 ± 0.22 | 2.47 ± 0.21 | 10 | 96.3 (337) | 18.48 ± 0.50 | 62.7(208) | |
| ≥75 (132) | 1374.52 ± 62.41 | 2.10 ± 0.34 | 2.39 ± 0.35 | 10 | 95.5 (126) | 18.32 ± 0.69 | 64.0 (85) | |
| Total (2520) | 1578.73 ± 19.41 | 2.56 ± 0.10 | 2.64 ± 0.10 | 17.10 ± 0.26 | 75.4 (1821) | |||
| F-value | 17.331 *** | 3.668 ** | 2.302 | 16.741 *** | ||||
| Subjects | Gender (n) | β | 95% CI | R2 | F-Value |
|---|---|---|---|---|---|
| Total subjects (n = 4541) | 0.044 | 0.009~0.079 | 0.089 | 6.196 * | |
| <50 years old | Total (2451) | 0.049 | 0.005~0.093 | 0.072 | 4.837 * |
| Men (1079) | 0.016 | −0.039~0.071 | 0.094 | 0.328 | |
| Women (1372) | 0.06 | −0.003~0.012 | 0.02 | 3.571 | |
| ≥50 years old | Total (2090) | 0.015 | −0.043~0.072 | 0.059 | 0.25 |
| Men (942) | −0.017 | −0.088~0.054 | 0.046 | 0.234 | |
| Women (1148) | 0.052 | −0.050~0.154 | 0.046 | 1.01 | |
| Food Groups | Total | Vitamin D Intake (Contribution) | F-Value | |
|---|---|---|---|---|
| ( n = 4541) | Man ( n = 2021) | Women ( n = 2520) | ||
| Fish & shellfish | 2.42 ± 0.10 | 2.81 ± 0.17 (71.69) | 2.02 ± 0.10 (62.35) | 13.790 *** |
| Eggs | 0.67 ± 0.02 | 0.68 ± 0.03 (17.05) | 0.65 ± 0.03 (20.05) | 0.691 |
| Milk & dairy products | 0.20 ± 0.01 | 0.16 ± 0.02 (4.12) | 0.24 ± 0.02 (7.41) | 6.146 * |
| Meat & meat products | 0.14 ± 0.02 | 0.12 ± 0.01 (3.22) | 0.17 ± 0.03 (5.25) | 3.336 |
| Mushrooms | 0.13 ± 0.02 | 0.11 ± 0.02 (2.94) | 0.13 ± 0.03 (4.01) | 0.2 |
| Grain products & others | 0.04 ± 0.00 | 0.04 ± 0.01 (0.98) | 0.03 ± 0.01 (0.93) | 0.575 |
| Rank | Men ( n = 2021) | Women ( n = 2520) | ||||
|---|---|---|---|---|---|---|
| Food | Con (%) | Acc-con (%) | Food | Con (%) | Acc-Con (%) | |
| 1 | Anchovy | 23.58 | 23.58 | Anchovy | 23.91 | 23.91 |
| 2 | Mackerel | 15.08 | 38.66 | Egg | 14.61 | 38.52 |
| 3 | Egg | 13.74 | 52.4 | Mackerel | 14.17 | 52.69 |
| 4 | Bastard halibut | 7.34 | 59.75 | Pacific saury | 6.26 | 58.96 |
| 5 | Pacific saury | 6.41 | 66.16 | Milk | 5.59 | 64.55 |
| 6 | Hairtail | 4.81 | 70.97 | Hairtail | 4.97 | 69.51 |
| 7 | Eel | 3.52 | 74.49 | Bastard halibut | 4.28 | 73.8 |
| 8 | Milk | 3.07 | 77.56 | Eel | 3.37 | 77.17 |
| 9 | Chum salmon | 2.1 | 79.67 | Chum salmon | 2.22 | 79.39 |
| 10 | Tuna | 2.09 | 81.75 | Oak mushroom | 2.04 | 81.43 |
| 11 | Pork | 1.79 | 83.54 | Jew’s-ear | 1.91 | 83.35 |
| 12 | Loach | 1.69 | 85.23 | Filefish | 1.88 | 85.23 |
| 13 | Filefish | 1.57 | 86.79 | Tuna | 1.83 | 87.06 |
| 14 | Jew’s-ear | 1.49 | 88.28 | Pork | 1.72 | 88.78 |
| 15 | Yellow croaker | 1.3 | 89.58 | Shrimp | 1.11 | 89.89 |
| 16 | Oak mushroom | 0.97 | 90.55 | Yellow croaker | 1.09 | 90.98 |
| 17 | Puffer | 0.77 | 91.32 | Loach | 0.83 | 91.81 |
| 18 | Shrimp | 0.76 | 92.07 | Spanish mackerel | 0.74 | 92.54 |
| 19 | Seabream | 0.74 | 92.82 | Angler | 0.67 | 93.21 |
| 20 | Spanish mackerel | 0.72 | 93.53 | Oyster mushroom | 0.65 | 93.86 |
| 21 | Trout | 0.51 | 94.04 | Alaska pollock | 0.53 | 94.39 |
| 22 | Angler | 0.49 | 94.54 | Puffer | 0.44 | 94.82 |
| 23 | Cereal | 0.45 | 94.98 | Common Mullet | 0.4 | 95.22 |
| 24 | Gizzard shad | 0.43 | 95.42 | Gizzard shad | 0.4 | 95.62 |
| Total | 95.42 | 95.62 | ||||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, K.; Cho, J.; Ly, S. Vitamin D Intake and Serum 25-Hydroxyvitamin D Levels in Korean Adults: Analysis of the 2009 Korea National Health and Nutrition Examination Survey (KNHANES IV-3) Using a Newly Established Vitamin D Database. Nutrients 2016, 8, 610. https://doi.org/10.3390/nu8100610
Yoo K, Cho J, Ly S. Vitamin D Intake and Serum 25-Hydroxyvitamin D Levels in Korean Adults: Analysis of the 2009 Korea National Health and Nutrition Examination Survey (KNHANES IV-3) Using a Newly Established Vitamin D Database. Nutrients. 2016; 8(10):610. https://doi.org/10.3390/nu8100610
Chicago/Turabian StyleYoo, Kyoungok, Jinah Cho, and Sunyung Ly. 2016. "Vitamin D Intake and Serum 25-Hydroxyvitamin D Levels in Korean Adults: Analysis of the 2009 Korea National Health and Nutrition Examination Survey (KNHANES IV-3) Using a Newly Established Vitamin D Database" Nutrients 8, no. 10: 610. https://doi.org/10.3390/nu8100610