1. Introduction
The prevalence of overweight and obesity has become a public health problem worldwide [
1]. International organizations [
2,
3] and previous epidemiological cross-sectional studies [
4,
5] have suggested that individuals with a large accumulation of excess body fat are at greater risk of the development of adverse health consequences, including hypertension, cardiovascular disease, metabolic disorders, osteoarthritis, gallbladder stone disease and asthma, as well as multiple malignancies [
2,
3,
4,
5,
6,
7]. To estimate the magnitude of this problem, direct indicators were used to assess various anthropometric indicators, such as body mass index (BMI) [
6], waist circumference (WC) [
7], and double thicknesses of skin and subcutaneous fat, measured as skinfold thickness [
8]. Skinfold thickness measurements are widely used to assess body fat because the measurements are non-invasive, simple, and less expensive than laboratory-based techniques [
9]; however, standardization and experience are required to achieve precise measurement [
9,
10].
There are a number of cross-sectional studies showing that high subcutaneous fat in youth is independently associated with higher cardio-metabolic risk [
11,
12,
13]. In addition, longitudinal studies have shown that a healthy body composition in childhood and adolescence is associated with a healthier cardio-metabolic profile later on in life [
14,
15]. These findings have been replicated in clinical adult populations with diabetes mellitus, hypertension, metabolic syndrome, and several types of cancer [
16,
17]. The two most frequently taken skinfold measurements are from triceps and subscapular sites [
9,
18]. Expert panels from the USA suggest measurement of these two skinfolds as a part of in-depth medical assessments for adolescents with increased BMI [
19]. However, Kromeyer-Hauschild et al. [
18] found that the additional information provided by skinfolds varies substantially according to BMI levels.
Sex- and age-specific normative values for two skinfolds in youth have been published [
18,
20,
21,
22]. However, the majority of the published skinfold thickness reference values are for schoolchildren from high-income countries in North America [
20] and Europe [
18,
21,
22]. There is a scarcity of reference values for children, using harmonized measures of body composition, in Latin America [
23,
24] and other low-middle income countries (LMICs) undergoing rapid epidemiologic and nutrition transitions [
25], making it impossible to evaluate secular trends within these regions and identify high risk groups for which risk reduction interventions should be prioritized. In particular, no population-based studies have been conducted to assess skinfold thickness for youths living in Bogotá, Colombia.
The aims of this study were to establish Colombian smoothed centile charts and LMS (L (Box–Cox transformation), M (median), and S (coefficient of variation)) tables for triceps, subscapular, and triceps + subscapular skinfolds, to develop appropriate cut-offs using receiver operating characteristic analysis, based on a population-based sample of 9- to 17-year-old children in Bogotá, Colombia, and to compare them with international studies.
4. Discussion
The results obtained in this study presented for the first time smoothed reference values for the triceps and subscapular skinfold thicknesses of a large, population-based sample of schoolchildren from Bogotá, Colombia. Although the boys had higher weight and height values, the girls had a higher BMI. In addition, a greater prevalence of normal weights among boys was shown, followed by a higher rate of overweight and obesity in girls. These results coincide with those obtained by Freedman et al. [
35], who performed a prospective study of 6866 boys and girls, 5–17.9 years of age, in Louisiana (USA). In this research, the BMI values of the girls were considerably higher than those of the boys.
In contrast, our results differed somewhat from Aristizabal et al. [
36]. According to their study of 232 schoolchildren in Medellín (Colombia), there was a higher prevalence of normal weight and overweight among girls, whereas higher values of obesity were detected among boys (as both BMI and
z-score BMI). A possible explanation for this partial divergence in results could be the age difference between our sample population and theirs. More specifically, the schoolchildren in Medellín were younger than the children in our sample.
In regard to subcutaneous fat distribution, striking differences were observed in triceps and subscapular skinfold thickness, as well as in the sum of both values (T + SS). In fact, these values were significantly higher for girls in the study than for boys. This coincides with the findings of Aristizabal et al. [
36] in Medellín (Colombia). Our results also agreed with those reported by Nagy et al. [
37] for a sample of 16,228 boys and girls from different European countries (Sweden, Germany, Hungary, Italy, Cyprus, Spain, Belgium, and Estonia), where girls also had higher scores for triceps and subscapular skinfold thickness, as well as the sum of both (T + SS).
In the case of WC, there were significant differences between both sexes, with higher values for boys. These results agree with those of Hirschler et al. [
38] in a population of Argentinian children, in which the boys were found to have a larger WC than the girls [
38]. Since our data are not longitudinal, we do not know whether WC increases progressively with age. Nevertheless, modification of subcutaneous fat distribution over time is widely documented in the literature. More specifically, with age, subcutaneous fat tends to move from the periphery to the trunk, which increases the risk of cardiovascular disorders at an earlier age [
39,
40].
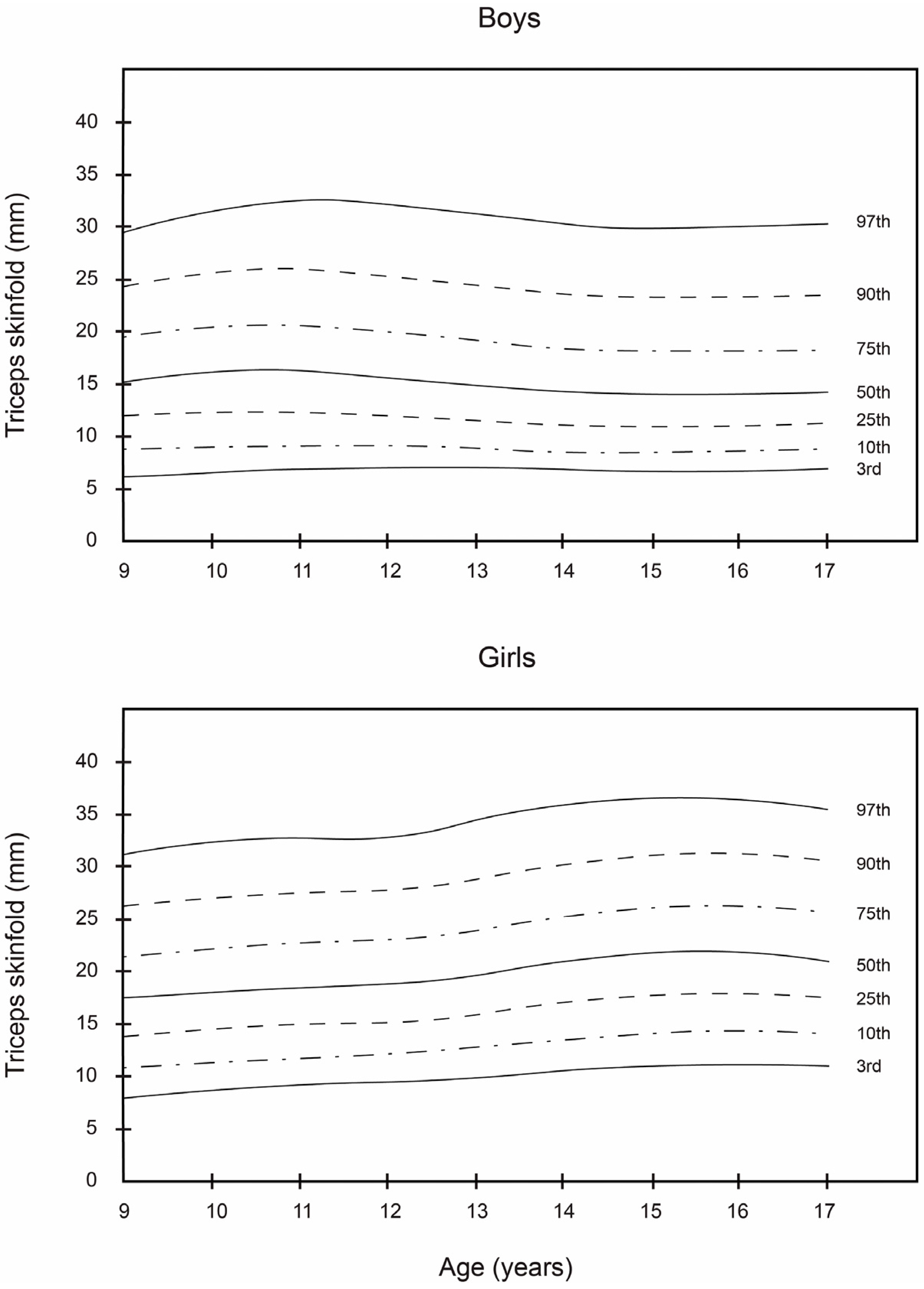
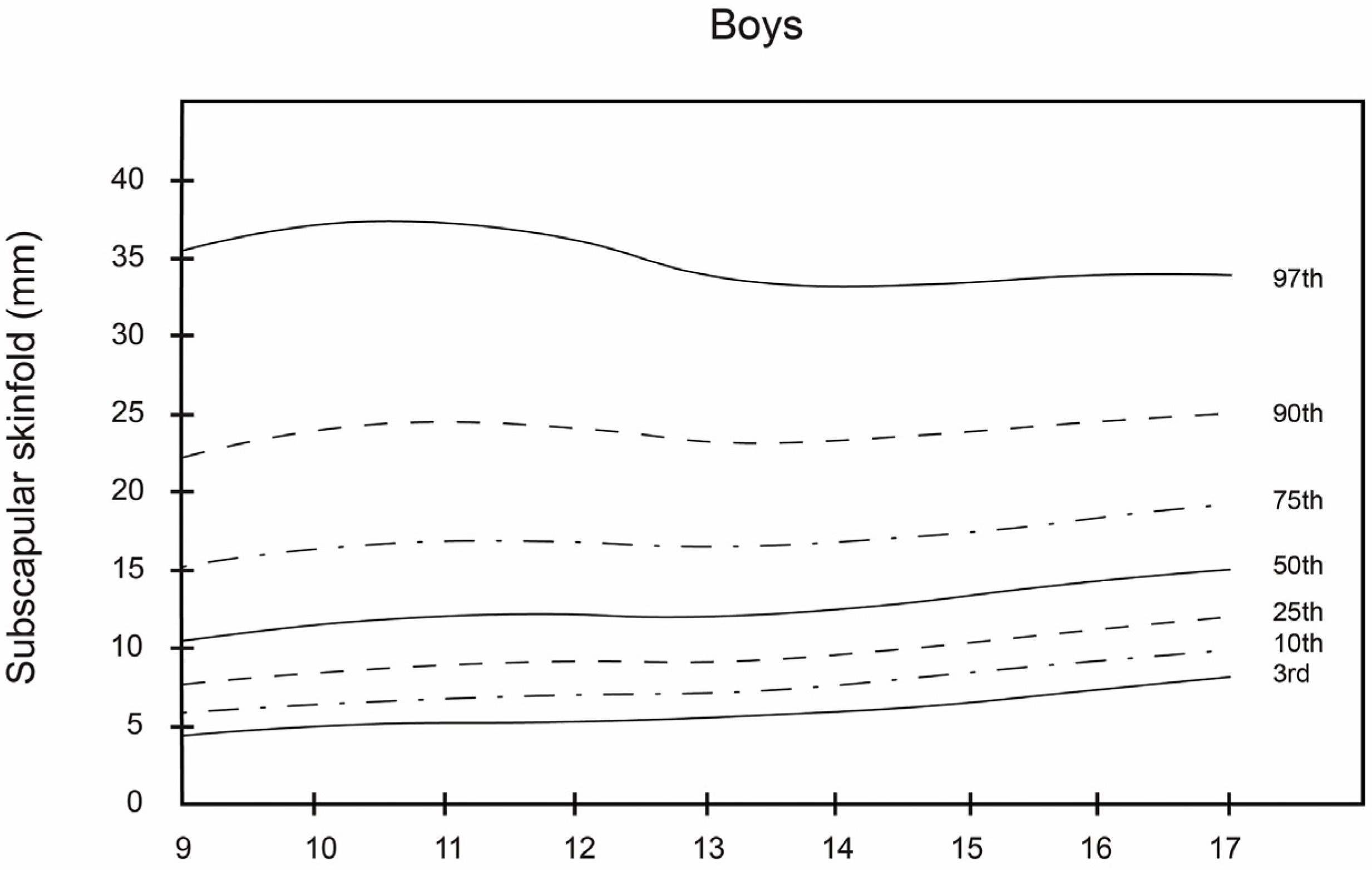
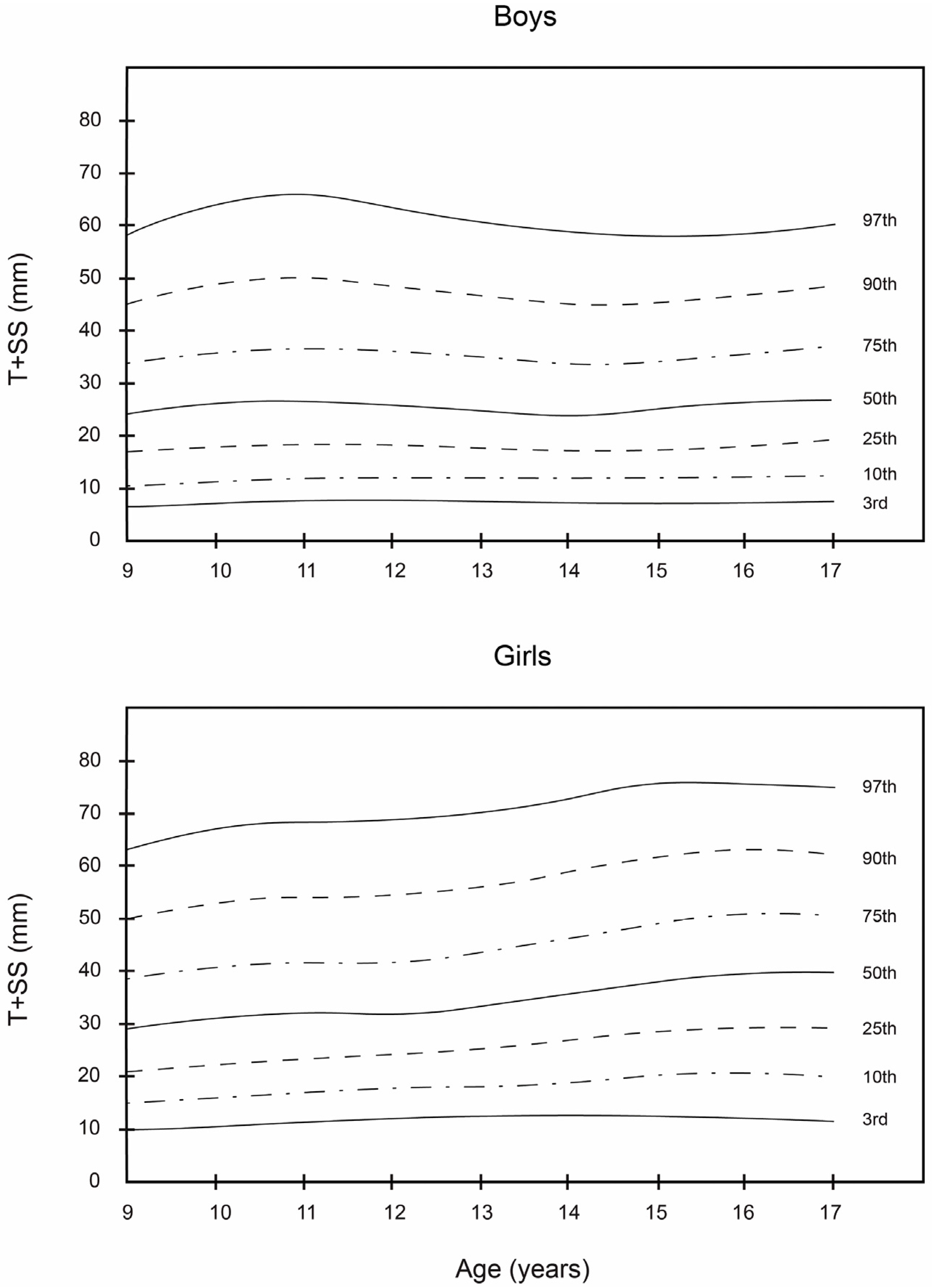
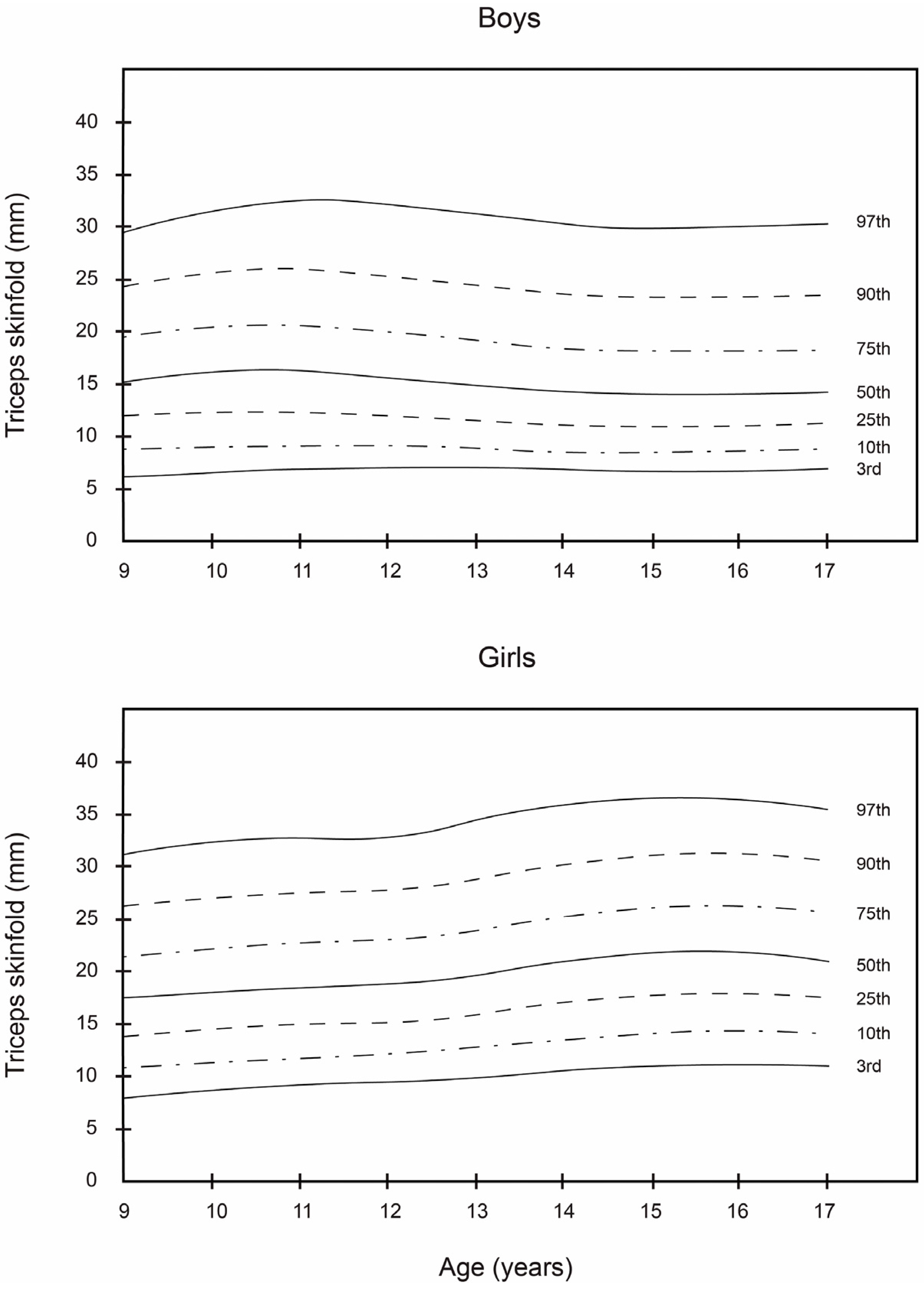
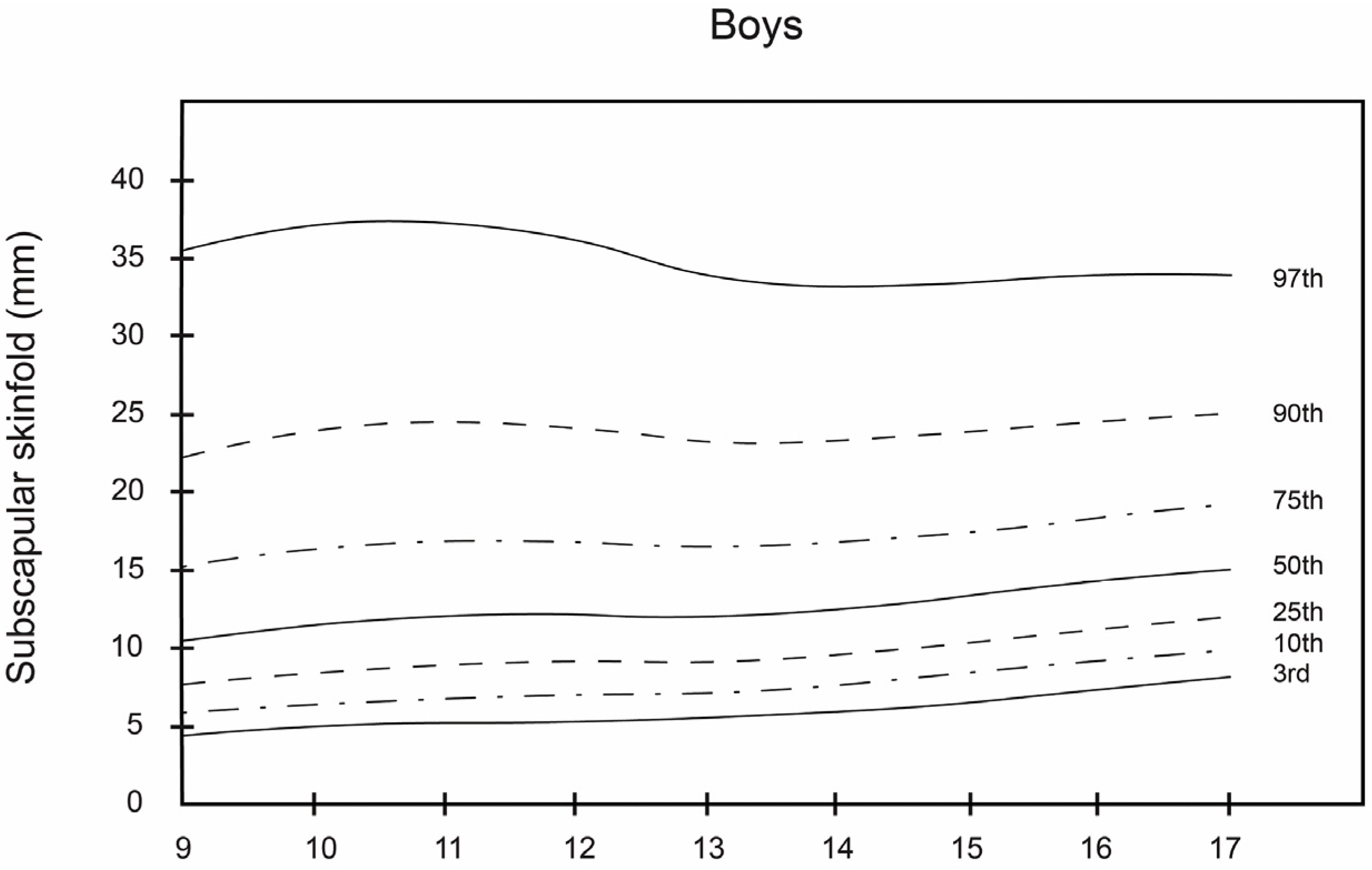
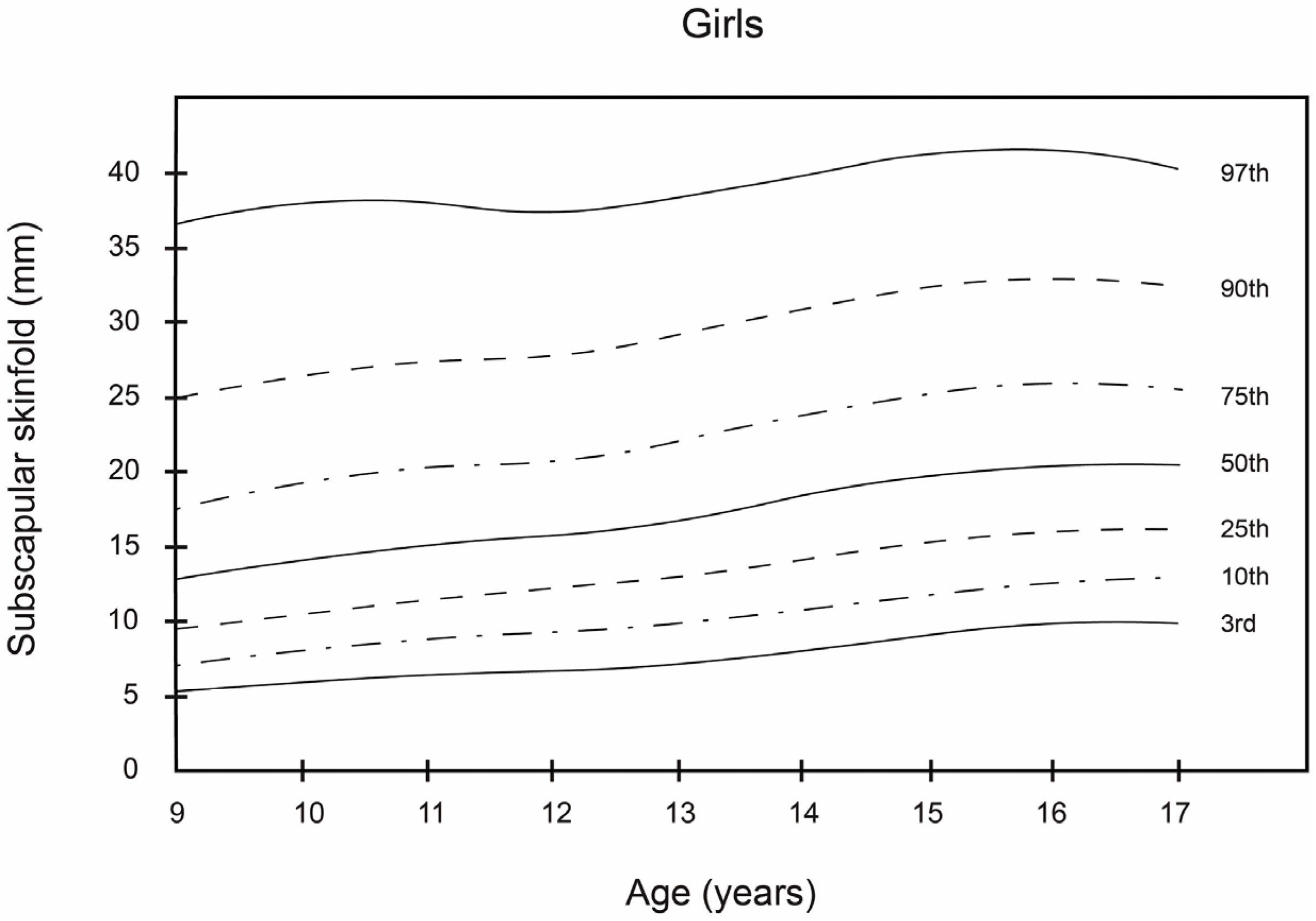
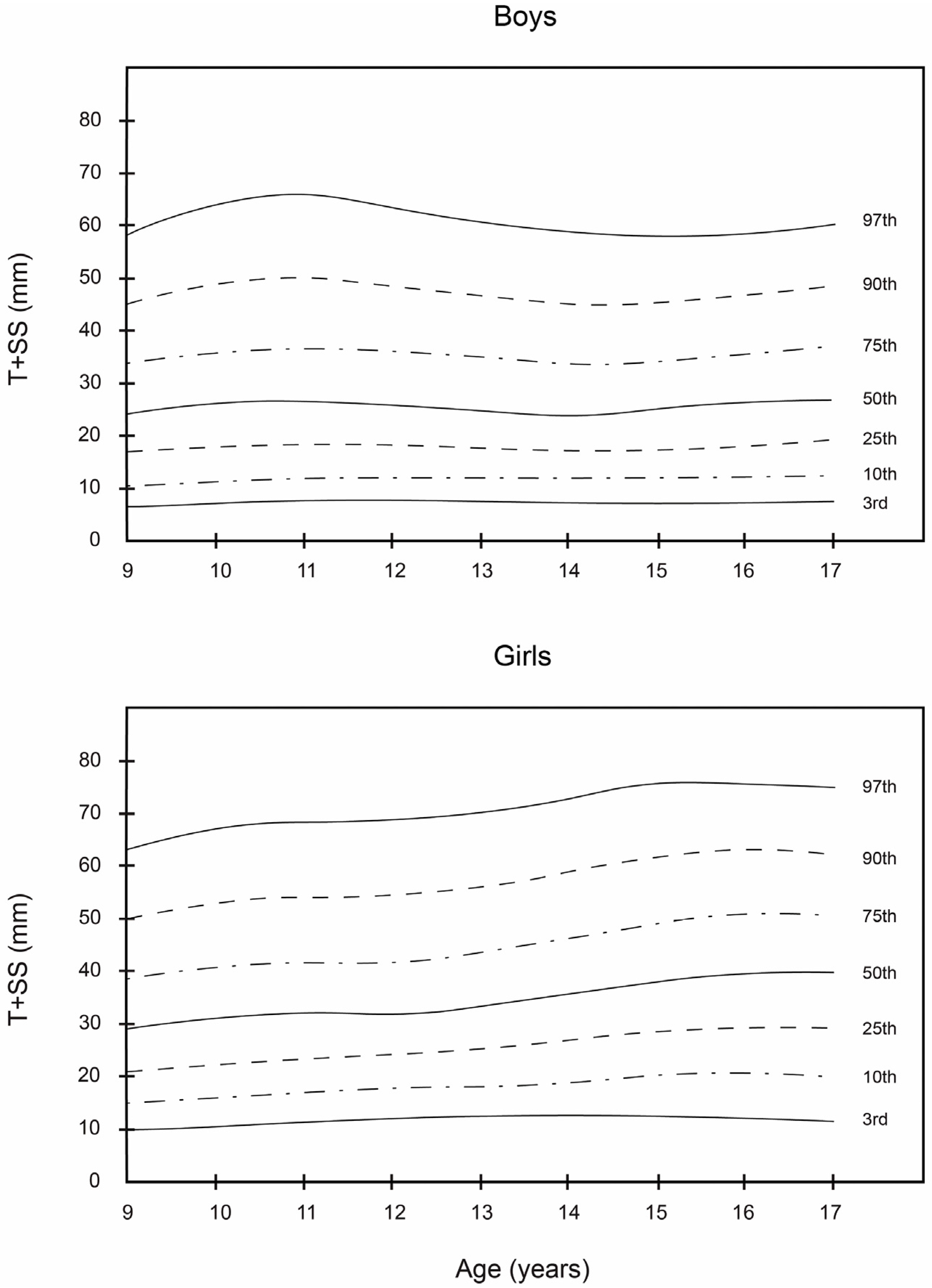
As can be observed, the smoothed LMS curves show higher values for triceps and subscapular skinfold thickness and T + SS for girls, regardless of age, in comparison with boys. These results are similar to those reported by Kromeyer-Hauschild et al. [
18] for a population of 2132 boys and girls in the city of Jena (Germany). In this study, the girls in all age groups had the highest mean values for these skinfolds. In regard to the boys, the 50th percentile of the triceps and subscapular skinfold thickness and T + SS varied from 10.0 to 14.0 mm, from 10.0 to 15.0 mm, and from 23.0 to 28.0 mm, respectively. Among the girls, the 50th percentile for these same skinfold thicknesses ranged from 17.0 to 22.0 mm, from 12.0 to 21.0 mm, and from 28.0 to 42.0 mm, respectively.
As reported by Aristizabal et al. [
36] and Addo and Himes [
20], girls in this study had higher mean values for these skinfolds than boys in all age groups. Among boys, triceps skinfold reached a maximum value of 31 mm at the age of 13.9 years, after which it decreased. In contrast, for girls, the values of these skinfolds increased progressively. As for subscapular skinfold thickness, it increased steadily in both sexes from 9 to 14 years of age. Similar findings were reported in previous studies of schoolchildren, though in other geographic areas, namely Warsaw [
41], Krakow [
42], and Turkey [
43]. In the case of T + SS, the percentage distribution of the values was more dispersed, with higher values for the girls. These results differed somewhat from those of Moreno et al. [
21], who obtained higher T + SS values for boys in their study of 2160 Spanish adolescents, 13–18 years of age.
ROC analysis showed that triceps, subscapular, and T + SS had a high discriminating power to detect overweight and obesity. This coincided with Cickek et al. [
44] and their study of a population of Turkish children and adolescents. In the overweight category for boys, 9–11.9 years of age, the cut-off value for the triceps skinfold was 18.1 mm, whereas for girls in the same age group the cut-off value was 20.1 mm. These results agreed with those of Brannsether et al. [
45] and their study of 4606 Norwegian children, in which higher cut-off values were reported for girls in all age groups. Similar results were obtained by Khadilkar et al. [
46], who studied a population of 13,375 schoolchildren in India.
In the obesity category for boys aged 15–17.9 years, the cut-off value for subscapular skinfold was 21.8 mm. In contrast, for girls of the same age, the cut-off value was considerably higher (28.7 mm). These results were similar to those of Kromeyer-Hauschild et al. [
18] for a sample population of 213 school children in Jena (Germany). In our study, the overweight and obesity cut-off values of the subscapular skinfold were much higher for girls, which reflected that girls had a higher level of subcutaneous adiposity than boys.
In addition, the sensitivity of subscapular skinfold to detect overweight in body fat composition with respect to BMI is 49.4% in girls and 74.6% in boys. However, the specificity is 84.1% in girls and 70.6% in boys. Therefore, using the subscapular skinfold there is a significant percentage of girls who, despite having normal levels of fat, would be categorized in the group of excessive fat. Taking into account this observation, the criteria for selecting a cut-off value (i.e., accepting or rejecting) should be considered when sensitivity is above 80%. In fact, ROC curves represent the rate of true positives versus the rate of false positives and are used to determine a more precise cut-off. Furthermore, the cut-off point for T + SS in both the overweight and obesity categories (especially in the 15–17.9 age group) was higher for girls. This could be explained by the marked sexual dimorphism in regard to the development and accumulation of subcutaneous fat, which increased as the subjects’ age increased [
47,
48,
49,
50]. In the obesity category for boys 15–17.9 years old, the cut-off point of 39.9 mm for T + SS provides a sensitivity of 76.5% and specificity of 81.4%. In girls, the cut-off point of 53.7 mm provides a sensitivity of 67.4% and a specificity of 83.5%. The area under the ROC curve is also considered in the analysis of ROC curves. This area under the ROC curve is a measure of how well a parameter can distinguish between two diagnostic groups.
Cross-cultural comparisons were conducted between the triceps and subscapular skinfold data from this study in Colombia with those from Spain [
18], Germany [
21], the UK [
22], and the USA [
20]. These countries were selected to represent European and American regions, respectively, for comparison with our data for the South American region. This comparative study based on non-fitted raw data showed that both boys and girls in Bogotá had higher values for tricipital and subscapular skinfolds in all of the age groups than children of similar ages in Spain, the UK, Germany, and the USA. This signifies that this sample population of children and adolescents in Bogotá generally had higher levels of adiposity than similar samples in other studies in other countries. Children and adolescents from different ethnic populations vary in their rate of proportional growth and body fat patterning. Our own results indicate differences between ethnic groups for both triceps and subscapular skinfolds. This ethnic difference in body fat distribution has also been observed in adolescents and pre-pubertal children mainly from the South America region, again highlighting the importance of ethnicity-specific studies.
Evidently, this is an important public health problem in Colombia. For this reason, it is necessary to carry out new studies that will help to identify and control the factors leading to this higher level of adiposity among schoolchildren in Bogotá. Moreover, these results should serve as a wake-up call for the Colombian government, which needs to implement policies that will encourage healthier lifestyles among young people, such as regular physical exercise and a balanced diet from early childhood.
This study had some limitations. First, it includes participants from only a single region in Colombia; therefore, inferences for all Colombian children and adolescents should be made cautiously. This study includes participants from public schools in one city and thus the data are not fully representative of the full population either of the city or of the country. However, Bogotá is the largest urban centre in Colombia, comprising about 15% of the country’s population. It includes a mix of locally born residents and people born elsewhere. The FUPRECOL study was deployed in collaboration with the Bogotá District Education Department, which only has jurisdiction among public schools. However, the public system constitutes the majority of school offering in the city, with 85% of school-age children enrolled in the city public school system. Second, we have not considered the potential impact of recognized determinants, such as socioeconomic, dietary, and physical activity patterns and ethnic factors that modulate growth and levels of adiposity. Third, this study includes use of skinfold thickness as a measure of adiposity to define pediatric obesity from BMI and has not used expensive tools that are sometimes difficult to transport to the field (e.g., dual-energy X-ray absorptiometry, air displacement plethysmography, and bioelectrical impedance). Nonetheless, BMI is widely recognized as an appropriate tool to screen obese children and adolescents and to define overweight status, as a state of excessive weight relative to height, regardless of body composition. This could suppose an important advantage for BMI over dual-energy X-ray absorptiometry, bioelectrical impedance, or both. Fourth, the sensitivity and specificity of the skinfolds were calculated using BMI as the gold standard, and BMI is not a measure of body fat. In addition, when a diagnosis tool has low sensitivity, it has an important number of false negatives (in this case, girls that should be considered obese but are incorrectly classified as not obese by skinfold measurement). Finally, these curves should only be used for Colombian children. However, such limitations do not compromise the results obtained when validating our results.
This study also has various strong points that should be highlighted. The results presented, for the first time, smoothed reference values for triceps and subscapular skinfold thickness among a large, population-based sample of schoolchildren from Bogotá, Colombia. Additionally worth mentioning is the use of the LMS method to smooth the percentile values. This allowed an accurate description of body composition and the pattern of fat distribution in the sample population, as well as its variation, depending on sex and age.

 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}