Dietary Pattern Is Associated with Obesity in Older People in China: Data from China Health and Nutrition Survey (CHNS)



Abstract
:1. Introduction
2. Methods
2.1. China Health and Nutrition Survey (CHNS)
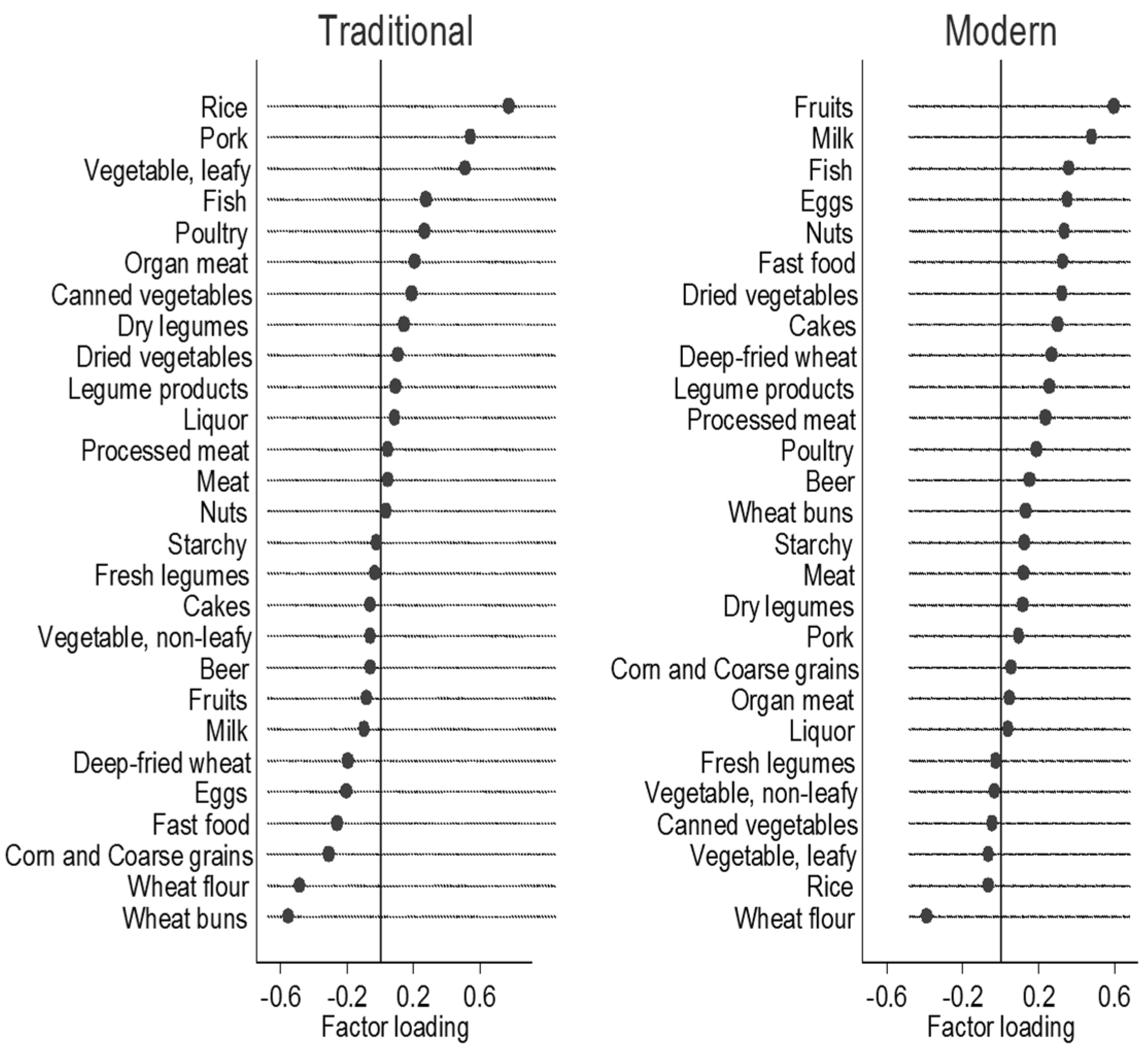
2.2. Dietary Assessment and Food Grouping
2.3. Outcome Variable-Body Composition
2.4. Other Variables
2.5. Statistical Analysis
3. Results

{kind=link}
{kind=link}
{kind=link}
| Factor | Men | Women | p Value | N (% of Participants) |
|---|---|---|---|---|
| 1300 (47.4%) | 1445 (52.6%) | 2745 | ||
| Age | ||||
| Median (IQR) | 67.0 (63.0, 74.0) | 69.0 (63.0, 74.0) | 0.06 | 2745 (100%) |
| Physical activity (MET) | ||||
| Median (IQR) | 84.1 (62.4; 132.6) | 101.8 (79.6; 133.3) | <0.001 | 2745 (100%) |
| Marital status * | ||||
| Married | 1103 (85.6%) | 926 (64.7%) | <0.001 | 2721 (99%) |
| Other marital status | 186 (14.4%) | 506 (35.3%) | ||
| Work status * | ||||
| No | 865 (66.9%) | 1145 (79.6%) | <0.001 | 2731 (99%) |
| Yes | 428 (33.1%) | 293 (20.4) | ||
| Education level * | ||||
| Illiteracy | 176 (13.7%) | 642 (44.8%) | <0.001 | 2721 (99%) |
| Low | 573 (44.5%) | 539 (37.6%) | ||
| Medium | 282 (21.9%) | 140 (9.8%) | ||
| High | 256 (19.9%) | 113 (7.9%) | ||
| Smoking status * | ||||
| No | 711 (54.9%) | 1351 (93.6%) | <0.001 | 2739 (99%) |
| Yes | 585 (45.1%) | 92 (6.4%) | ||
| Urbanization | ||||
| Low | 455 (35.1%) | 475 (32.9%) | 0.39 | 2739 (99%) |
| Medium | 424 (32.7%) | 473 (32.8%) | ||
| High | 417 (32.2%) | 495 (34.3%) | ||
| BMI * | ||||
| Underweight | 101 (8.2%) | 121 (8.8%) | <0.001 | 2609 (95%) |
| Normal | 669 (54.3%) | 672 (48.8%) | ||
| Overweight | 380 (30.8%) | 417 (30.3%) | ||
| Obesity | 83 (6.7%) | 166 (12.1%) | ||
| Central obesity | ||||
| No | 834 (64.4%) | 469 (32.5%) | <0.001 | 2739 (99%) |
| Yes | 462 (35.7%) | 974 (67.5%) | ||
| Food items (Liang per day) | Q1 | Q2 | Q3 | Q4 | p for Trend | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Intake of traditional food pattern | |||||||||
| Men | |||||||||
| Rice | 1.36 | 1.64 | 3.89 | 2.07 | 5.22 | 2.07 | 8.01 | 3.65 | <0.001 |
| Pork | 0.49 | 0.67 | 0.80 | 0.88 | 1.35 | 0.98 | 2.20 | 1.68 | <0.001 |
| Fresh vegetable, leafy | 1.61 | 1.69 | 2.01 | 2.11 | 2.97 | 1.86 | 4.60 | 2.73 | <0.001 |
| Fish | 0.18 | 0.55 | 0.54 | 0.97 | 0.78 | 1.15 | 1.12 | 1.58 | <0.001 |
| Poultry | 0.11 | 0.37 | 0.13 | 0.46 | 0.21 | 0.54 | 0.48 | 0.94 | <0.001 |
| Organ meat | 0.02 | 0.16 | 0.03 | 0.17 | 0.06 | 0.22 | 0.14 | 0.40 | <0.001 |
| Corn and coarse grains | 1.03 | 1.76 | 0.41 | 1.07 | 0.23 | 0.72 | 0.11 | 0.42 | <0.001 |
| Wheat flour | 3.66 | 3.27 | 1.37 | 1.37 | 1.21 | 1.13 | 0.57 | 0.91 | <0.001 |
| Wheat buns | 2.94 | 2.87 | 0.99 | 1.68 | 0.37 | 0.81 | 0.17 | 0.47 | <0.001 |
| Oil (g) | 60.4 | 219.8 | 45.0 | 65.3 | 44.8 | 45.5 | 52.5 | 140.5 | 0.35 |
| Energy (kJ per day) | 8542 | 8631 | 7940 | 3284 | 8679 | 2776 | 10616 | 6149 | 0.14 |
| Intake of traditional food pattern | |||||||||
| Women | |||||||||
| Rice | 3.89 | 2.07 | 3.52 | 1.84 | 4.79 | 1.77 | 7.19 | 3.31 | <0.001 |
| Pork | 0.39 | 0.54 | 0.74 | 0.79 | 1.31 | 0.90 | 2.27 | 1.70 | <0.001 |
| Fresh vegetable, leafy | 1.50 | 1.67 | 2.01 | 1.76 | 3.09 | 1.96 | 4.62 | 3.13 | <0.001 |
| Fish | 0.13 | 0.41 | 0.36 | 0.76 | 0.69 | 1.06 | 1.11 | 1.74 | <0.001 |
| Poultry | 0.05 | 0.20 | 0.11 | 0.38 | 0.23 | 0.54 | 0.51 | 0.92 | <0.001 |
| Organ meat | 0.02 | 0.19 | 0.02 | 0.13 | 0.05 | 0.19 | 0.15 | 0.40 | <0.001 |
| Corn and coarse grains | 0.91 | 1.70 | 0.34 | 0.85 | 0.15 | 0.48 | 0.12 | 0.52 | <0.001 |
| Wheat flour | 2.87 | 2.51 | 1.25 | 1.24 | 0.88 | 0.97 | 0.47 | 0.76 | <0.001 |
| Wheat buns | 2.25 | 2.27 | 0.65 | 1.19 | 0.27 | 0.66 | 0.19 | 0.55 | <0.001 |
| Oil (g) | 52.4 | 178.7 | 37.3 | 39.9 | 39.2 | 28.5 | 53.9 | 157.0 | 0.82 |
| Energy (kJ per day) | 8140 | 6967 | 6797 | 2454 | 7442 | 2066 | 10616 | 6149 | <0.001 |
| Intake of modern food pattern | |||||||||
| Men | |||||||||
| Fruit | 0.04 | 0.21 | 0.23 | 0.68 | 0.80 | 1.34 | 2.45 | 2.81 | <0.001 |
| Milk | 0.0 | 0.0 | 0.0005 | 0.009 | 0.14 | 0.61 | 1.07 | 1.87 | <0.001 |
| Fast food | 0.01 | 0.12 | 0.14 | 0.54 | 0.43 | 0.88 | 0.92 | 1.70 | <0.001 |
| Eggs | 0.24 | 0.42 | 0.48 | 0.58 | 0.72 | 0.76 | 1.01 | 1.06 | <0.001 |
| Nuts | 0.003 | 0.02 | 0.04 | 0.17 | 0.07 | 0.26 | 0.29 | 0.74 | <0.001 |
| Cakes | 0.008 | 0.07 | 0.02 | 0.14 | 0.07 | 0.28 | 0.32 | 1.15 | <0.001 |
| Dried vegetable | 0.009 | 0.06 | 0.01 | 0.07 | 0.06 | 0.20 | 0.16 | 0.41 | <0.001 |
| Fish | 0.12 | 0.38 | 0.53 | 0.89 | 0.92 | 1.25 | 1.13 | 1.63 | <0.001 |
| Deep-fried wheat | 0.003 | 0.04 | 0.03 | 0.15 | 0.15 | 0.39 | 0.55 | 1.22 | <0.001 |
| Processed meat | 0.002 | 0.02 | 0.03 | 0.16 | 0.08 | 0.30 | 0.17 | 0.58 | <0.001 |
| Wheat buns | 0.35 | 1.25 | 0.74 | 1.62 | 1.28 | 2.29 | 1.78 | 2.29 | <0.001 |
| Legume products | 0.68 | 1.03 | 0.91 | 1.32 | 1.06 | 1.32 | 1.72 | 1.88 | <0.001 |
| Rice | 5.91 | 4.29 | 5.29 | 3.12 | 4.62 | 3.43 | 3.63 | 2.87 | <0.001 |
| Wheat flour | 2.85 | 3.29 | 1.50 | 1.67 | 1.35 | 1.57 | 0.95 | 1.34 | <0.001 |
| Oil (g) | 54.3 | 136.4 | 42.0 | 30.4 | 55.5 | 161.0 | 24.6 | 170.0 | 0.85 |
| Energy (kJ per day) | 9440 | 6171 | 8460 | 2806 | 9447 | 6526 | 10231 | 6769 | 0.001 |
| Intake of modern food pattern | |||||||||
| Women | |||||||||
| Fruit | 0.07 | 0.33 | 0.33 | 0.80 | 0.74 | 1.31 | 3.28 | 3.36 | <0.001 |
| Milk | 0.005 | 0.09 | 0.0012 | 0.016 | 0.13 | 0.55 | 1.21 | 1.94 | <0.001 |
| Fast food | 0.01 | 0.10 | 0.12 | 0.46 | 0.47 | 0.85 | 0.97 | 1.80 | <0.001 |
| Eggs | 0.19 | 0.36 | 0.49 | 0.55 | 0.67 | 0.63 | 0.94 | 0.88 | <0.001 |
| Nuts | 0.006 | 0.05 | 0.03 | 0.13 | 0.05 | 0.18 | 0.20 | 0.56 | <0.001 |
| Cakes | 0.001 | 0.02 | 0.02 | 0.12 | 0.06 | 0.23 | 0.25 | 0.73 | <0.001 |
| Dried vegetable | 0.005 | 0.04 | 0.01 | 0.07 | 0.07 | 0.23 | 0.16 | 0.39 | <0.001 |
| Fish | 0.12 | 0.39 | 0.38 | 0.71 | 0.66 | 1.10 | 1.06 | 1.68 | <0.001 |
| Deep-fried wheat | 0.02 | 0.15 | 0.03 | 0.14 | 0.21 | 0.48 | 0.27 | 0.54 | <0.001 |
| Processed meat | 0.005 | 0.04 | 0.03 | 0.15 | 0.05 | 0.20 | 0.13 | 0.39 | <0.001 |
| Wheat buns | 0.19 | 0.75 | 0.69 | 1.41 | 1.41 | 2.08 | 1.25 | 1.63 | <0.001 |
| Legume products | 0.55 | 0.80 | 0.73 | 1.12 | 1.16 | 1.42 | 1.42 | 1.81 | <0.001 |
| Rice | 4.67 | 3.36 | 4.41 | 2.73 | 3.53 | 2.89 | 3.30 | 2.77 | <0.001 |
| Wheat flour | 2.33 | 2.53 | 1.39 | 1.57 | 1.15 | 1.30 | 0.73 | 0.95 | <0.001 |
| Oil (g) | 45.3 | 94.1 | 39.1 | 48.6 | 51.7 | 146.2 | 44.8 | 159.0 | 0.70 |
| Energy (kJ per day) | 7597 | 4375 | 7355 | 3096 | 8148 | 5849 | 8719 | 3504 | <0.001 |
| BMI | Q1 | Q2 | Q3 | Q4 | p for Trend |
|---|---|---|---|---|---|
| (a) Intake of Traditional Dietary Pattern Quartiles | |||||
| RRRs | |||||
| Men | |||||
| Model 1 | |||||
| Normal | 1 | 1 | 1 | 1 | |
| Underweight | 1 | 1.98 (0.97; 4.02) | 1.89 (0.95; 3.76) | 1.80 (0.91; 3.53) | 0.36 |
| Overweight | 1 | 0.73 (0.51; 1.06) | 0.61 (0.42; 0.87) | 0.66 (0.47; 0.93) | 0.002 |
| Obesity | 1 | 0.94 (0.50; 1.77) | 0.61 (0.31; 1.18) | 0.68 (0.36; 1.26) | 0.26 |
| Model 2 a | |||||
| Normal | 1 | 1 | 1 | 1 | |
| Underweight | 1 | 1.46 (0.69; 3.08) | 1.64 (0.81; 3.32) | 1.75 (0.87; 3.51) | 0.20 |
| Overweight | 1 | 0.69 (0.47; 1.02) | 0.58 (0.40; 0.84) | 0.64 (0.45; 0.92) | 0.001 |
| Obesity | 1 | 0.77 (0.39; 1.51) | 0.48 (0.24; 0.98) | 0.66 (0.34; 1.27) | 0.20 |
| Model 3 | |||||
| Normal | 1 | 1 | 1 | 1 | |
| Underweight | 1 | 1.55 (0.73; 3.31) | 1.78 (0.87; 3.67) | 1.91 (0.94; 3.86) | 0.15 |
| Overweight | 1 | 0.65 (0.43; 0.96) | 0.54 (0.36; 0.79) | 0.61 (0.42; 0.87) | <0.001 |
| Obesity | 1 | 0.66 (0.33; 1.31) | 0.40 (0.19; 0.83) | 0.55 (0.28; 1.08) | 0.09 |
| (a) Intake of Traditional Dietary Pattern Quartiles | |||||
| PRs | |||||
| Central obesity | |||||
| Model 1 | |||||
| No | 1 | 1 | 1 | 1 | |
| Yes | 1 | 0.82 (0.66; 1.02) | 0.69 (0.55; 0.86) | 0.80 (0.66; 0.99) | 0.01 |
| Model 2 a | |||||
| No | 1 | 1 | 1 | 1 | |
| Yes | 1 | 0.82 (0.66; 1.02) | 0.70 (0.55; 0.87) | 0.82 (0.67; 1.01) | 0.009 |
| Model 3 | |||||
| No | 1 | 1 | 1 | 1 | |
| Yes | 1 | 0.78 (0.63; 0.98) | 0.66 (0.52; 0.83) | 0.80 (0.64; 0.97) | 0.003 |
| Women | |||||
| Model 1 | |||||
| Normal | 1 | 1 | 1 | 1 | |
| Underweight | 1 | 1.13 (0.62; 2.04) | 1.90 (1.09; 3.32) | 1.51 (0.83; 2.76) | 0.18 |
| Overweight | 1 | 0.93 (0.67; 1.29) | 0.83 (0.59; 1.17) | 0.92 (0.64; 1.31) | 0.28 |
| Obesity | 1 | 0.81 (0.52; 1.28) | 0.72 (0.44; 1.15) | 0.79 (0.48; 1.29) | 0.05 |
| Model 2 a | |||||
| Normal | 1 | 1 | 1 | 1 | |
| Underweight | 1 | 1.02 (0.55; 1.89) | 1.75 (0.97; 3.14) | 1.96 (1.03; 3.72) | 0.05 |
| Overweight | 1 | 0.97 (0.69; 1.37) | 0.86 (0.60; 1.23) | 0.80 (0.55; 1.17) | 0.06 |
| Obesity | 1 | 0.83 (0.52; 1.33) | 0.72 (0.44; 1.19) | 0.70 (0.42; 1.18) | 0.02 |
| Model 3 | |||||
| Normal | 1 | 1 | 1 | 1 | |
| Underweight | 1 | 1.12 (0.60; 2.10) | 1.97 (1.08; 3.59) | 2.14 (1.12; 4.11) | 0.03 |
| Overweight | 1 | 0.91 (0.64; 1.30) | 0.80 (0.55; 1.15) | 0.76 (0.52; 1.11) | 0.03 |
| Obesity | 1 | 0.77 (0.48; 1.25) | 0.67 (0.40; 1.12) | 0.68 (0.40; 1.14) | 0.01 |
| PRs | |||||
| Central obesity | |||||
| Model 1 | |||||
| No | 1 | 1 | 1 | 1 | |
| Yes | 1 | 0.87 (0.80; 0.96) | 0.84 (0.76; 0.93) | 0.82 (0.74; 0.92) | <0.001 |
| Model 2 a | |||||
| No | 1 | 1 | 1 | 1 | |
| Yes | 1 | 0.88 (0.80; 0.96) | 0.84 (0.76; 0.93) | 0.81 (0.72; 0.90) | <0.001 |
| Model 3 | |||||
| No | 1 | 1 | 1 | 1 | |
| Yes | 1 | 0.87 (0.79; 0.96) | 0.84 (0.76; 0.93) | 0.81 (0.72; 0.90) | <0.001 |
| (b) Intake of Modern Dietary Pattern Quartiles | |||||
| RRRs | |||||
| Men | |||||
| Model 1 | |||||
| Normal | 1 | 1 | 1 | 1 | |
| Underweight | 1 | 1.16 (0.69; 1.95) | 0.76 (0.42; 1.36) | 0.41 (0.21; 0.82) | 0.002 |
| Overweight | 1 | 1.44 (0.98; 2.12) | 2.03 (1.40; 2.94) | 2.17 (1.51; 3.13) | 0.001 |
| Obesity | 1 | 2.83 (1.27; 6.33) | 2.59 (1.14; 5.89) | 4.28 (1.99; 9.21) | <0.001 |
| Model 2 b | |||||
| Normal | 1 | 1 | 1 | 1 | |
| Underweight | 1 | 1.04 (0.60; 1.79) | 0.88 (0.48; 1.63) | 0.65 (0.31; 1.37) | 0.07 |
| Overweight | 1 | 1.51 (1.01; 2.26) | 1.86 (1.26; 2.76) | 1.78 (1.20; 2.65) | 0.05 |
| Obesity | 1 | 3.00 (1.31; 6.88) | 2.02 (0.86; 4.75) | 2.97 (1.31; 6.74) | 0.02 |
| Model 3 | |||||
| Normal | 1 | 1 | 1 | 1 | |
| Underweight | 1 | 1.03 (0.59; 1.78) | 0.98 (0.52; 1.87) | 0.78 (0.35; 1.73) | 0.22 |
| Overweight | 1 | 1.43 (0.95; 2.15) | 1.69 (1.12; 2.53) | 1.58 (1.03; 2.41) | 0.21 |
| Obesity | 1 | 2.59 (1.12; 6.00) | 1.53 (0.64; 3.70) | 2.07 (0.88; 4.90) | 0.17 |
| PRs | |||||
| Central obesity | |||||
| Model 1 | |||||
| No | 1 | 1 | 1 | 1 | |
| Yes | 1 | 1.13 (0.86; 1.48) | 1.48 (1.15; 1.90) | 1.89 (1.50; 2.39) | <0.001 |
| Model 2 b | |||||
| No | 1 | 1 | 1 | 1 | |
| Yes | 1 | 1.15 (0.88; 1.50) | 1.35 (1.04; 1.74) | 1.60 (1.25; 2.04) | <0.001 |
| Model 3 | |||||
| No | 1 | 1 | 1 | 1 | |
| Yes | 1 | 1.10 (0.84; 1.44) | 1.24 (0.95; 1.60) | 1.42 (1.10; 1.67) | <0.001 |
| Women | |||||
| Model 1 | |||||
| Normal | 1 | 1 | 1 | 1 | |
| Underweight | 1 | 0.68 (0.42; 1.10) | 0.81 (0.49; 1.33) | 0.16 (0.06; 0.37) | <0.001 |
| Overweight | 1 | 1.04 (0.73; 1.48) | 1.77 (1.25; 2.51) | 1.70 (0.19; 2.42) | 0.004 |
| Obesity | 1 | 1.02 (0.61; 1.70) | 1.62 (0.98; 2.66) | 2.00 (1.23; 3.25) | 0.004 |
| Model 2 b | |||||
| Normal | 1 | 1 | 1 | 1 | |
| Underweight | 1 | 0.64 (0.39; 1.06) | 0.95 (0.56; 1.61) | 0.21 (0.08; 0.52) | 0.005 |
| Overweight | 1 | 1.01 (0.70; 1.45) | 1.62 (1.12; 2.34) | 1.43 (0.97; 2.12) | 0.16 |
| Obesity | 1 | 0.96 (0.57; 1.62) | 1.34 (0.80; 2.26) | 1.47 (0.87; 2.51) | 0.20 |
| Model 3 | |||||
| Normal | 1 | 1 | 1 | 1 | |
| Underweight | 1 | 0.67 (0.41; 1.11) | 1.06 (0.62; 1.83) | 0.24 (0.09; 0.63) | 0.03 |
| Overweight | 1 | 0.98 (0.68; 1.41) | 1.50 (1.02; 2.18) | 1.29 (0.86; 1.95) | 0.43 |
| Obesity | 1 | 0.90 (0.53; 1.53) | 1.21 (0.71; 2.08) | 1.32 (0.76; 2.30) | 0.37 |
| PRs | |||||
| Central obesity | |||||
| Model 1 | |||||
| No | 1 | 1 | 1 | 1 | |
| Yes | 1 | 1.15 (1.02; 1.29) | 1.18 (1.05; 1.32) | 1.28 (1.14; 1.43) | 0.001 |
| Model 2 b | |||||
| No | 1 | 1 | 1 | 1 | |
| Yes | 1 | 1.14 (1.01; 1.28) | 1.12 (1.00; 1.25) | 1.19 (1.06; 1.33) | 0.09 |
| Model 3 | |||||
| No | 1 | 1 | 1 | 1 | |
| Yes | 1 | 1.13 (1.01; 1.27) | 1.11 (0.98; 1.25) | 1.18 (1.04; 1.33) | 0.14 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix
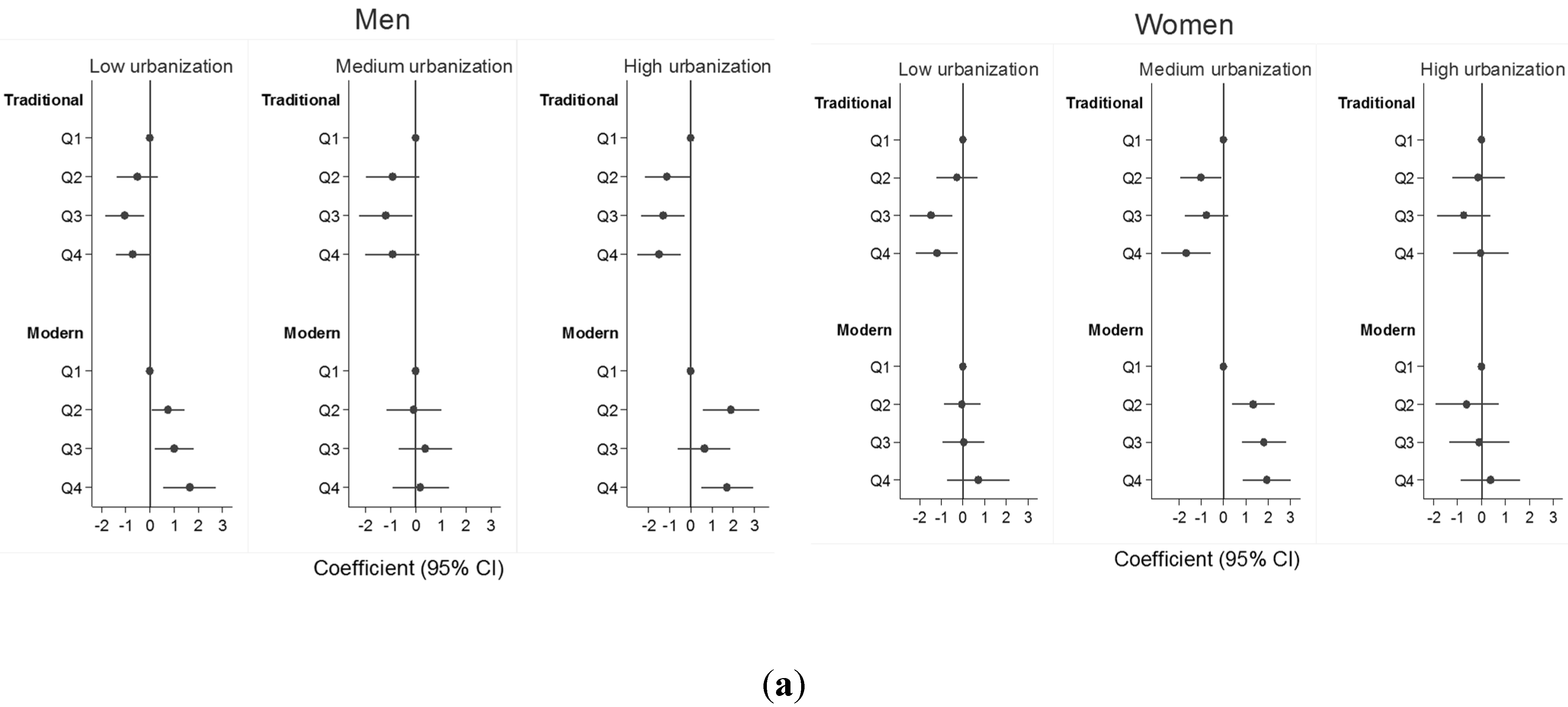
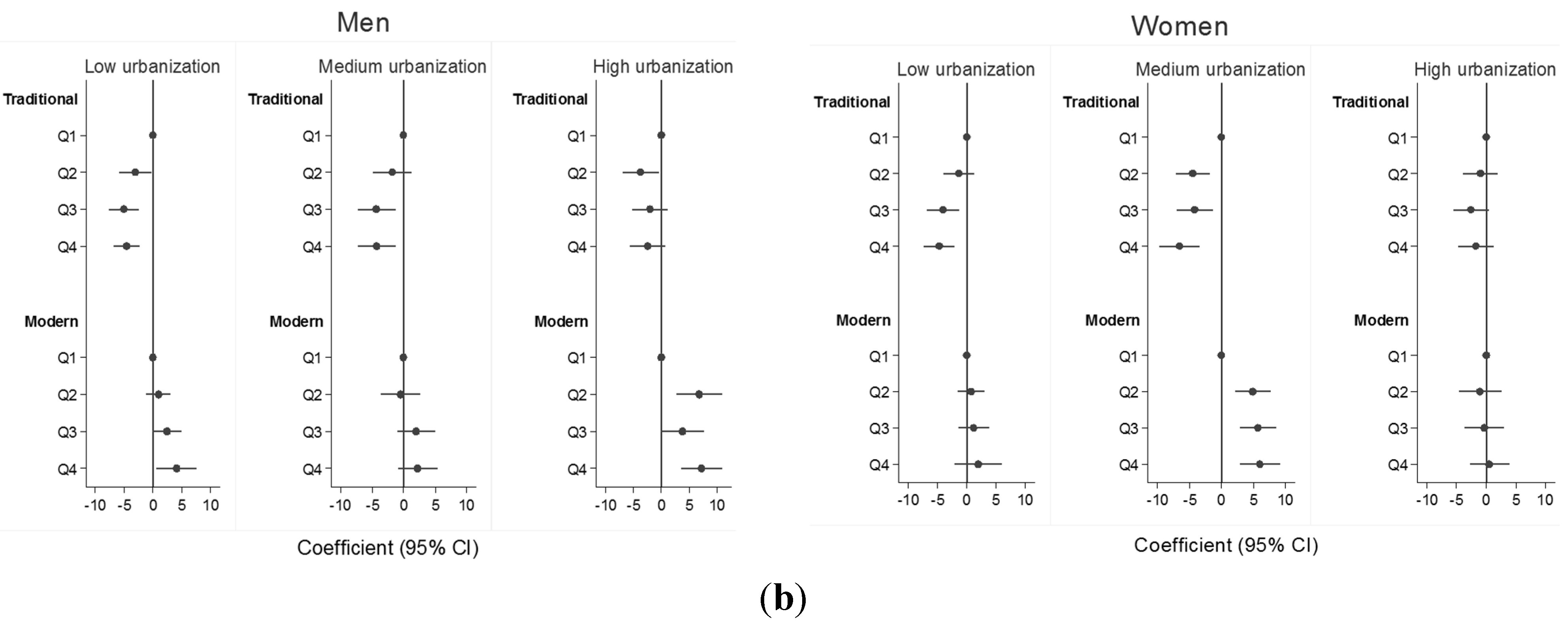
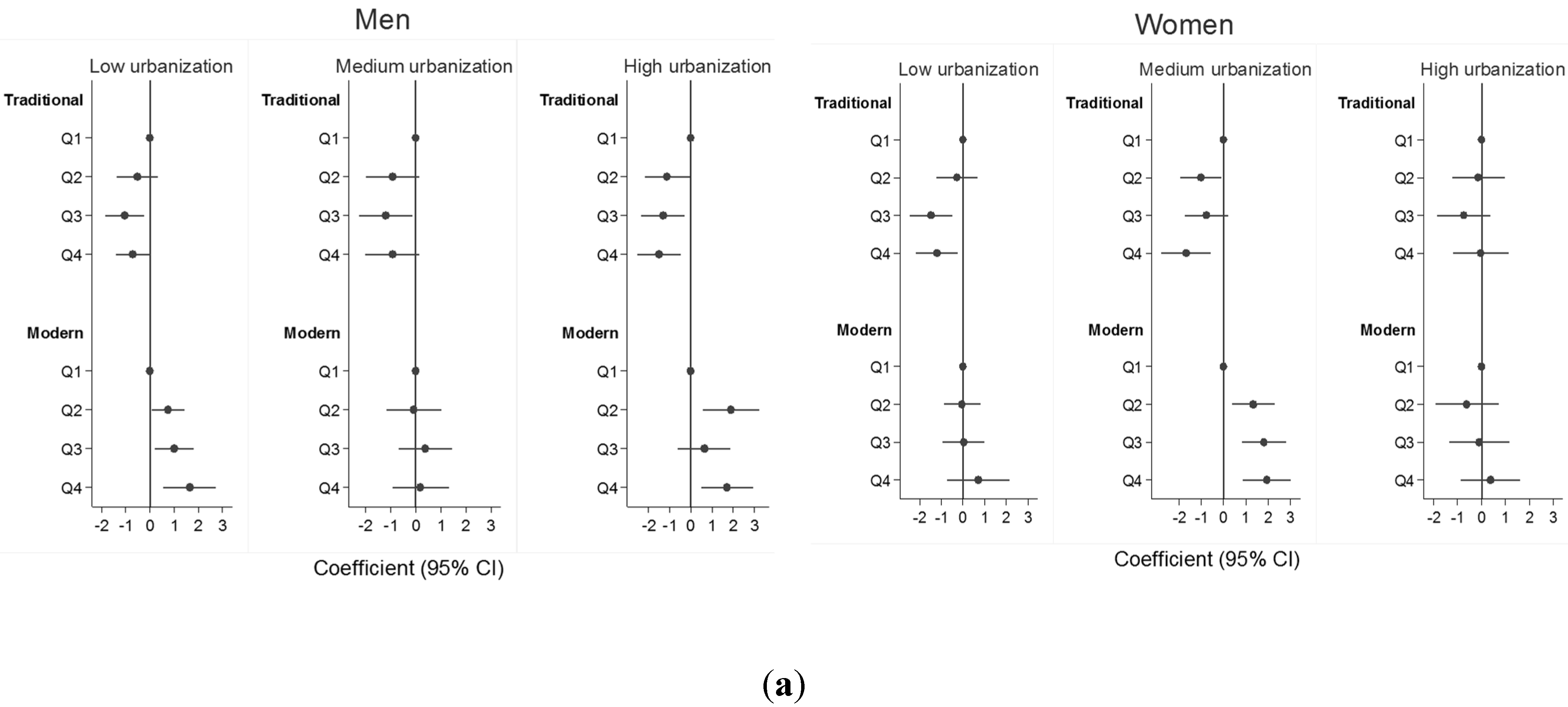
| Coefficients (95% CI) | |||||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | p for trend | |
| (a) Intake of traditional dietary pattern quartiles | |||||
| BMI * | |||||
| Men | |||||
| Mode1 1 a | 1 | −0.79 (−1.35; −0.24) | −1.14 (−1.68; −0.61) | −0.92 (−1.43; −0.41) | <0.001 |
| Model 1 a + WC | −0.01 (−0.38; 0.36) | −0.06 (−0.42; 0.30) | 0.11 (−0.23; 0.45) | 0.31 | |
| Women | |||||
| Mode1 1 a | 1 | −0.66 (−1.22; −0.10) | −1.09 (−1.67; −0.51) | −1.06 (−1.66; −0.46) | <0.001 |
| Model 1 a + WC | 0.002 (−0.38; 0.39) | −0.09 (−0.49; 0.31) | 0.11 (−0.31; 0.52) | 0.96 | |
| WC * | |||||
| Men | |||||
| Model 1 a | 1 | −3.13 (−4.81; −1.45) | −4.11 (−5.74; −2.48) | −3.81 (−5.35; −2.26) | <0.001 |
| Model 1 a + BMI | −1.30 (−2.41; −0.18) | −1.74 (−2.82; −0.65) | −1.94 (−2.96; −0.91) | <0.001 | |
| Women | |||||
| Model 1 a | 1 | −2.69 (−4.24; −1.14) | −3.76 (−5.36; −2.15) | −4.39 (−6.05; −2.72) | <0.001 |
| Model 1 a + BMI | −1.17 (−2.23; −0.11) | −1.49 (−2.59; −0.38) | −2.19 (−3.33; −1.04) | <0.001 | |
| (b) Intake of modern dietary pattern quartiles | |||||
| BMI * | |||||
| Men | |||||
| Model 1 b | 1 | 0.81 (0.28; 1.34) | 0.81 (0.26; 1.36) | 1.26 (0.68; 1.85) | <0.001 |
| Model 1 b + WC | 0.38 (0.03; 0.73) | 0.07 (−0.30; 0.43) | 0.15 (−0.24; 0.54) | 0.77 | |
| Women | |||||
| Model 1 b | 1 | 0.29 (−0.27; 0.85) | 0.64 (0.05; 1.23) | 1.04 (0.39; 1.69) | 0.02 |
| Model 1 b + WC | −0.04 (−0.42; 0.34) | 0.11 (−0.30; 0.52) | 0.27 (−0.18; 0.71) | 0.68 | |
| WC * | |||||
| Men | |||||
| Model 1 b | 1 | 1.74 (0.15; 3.34) | 2.72 (1.05; 4.40) | 4.27 (2.51; 6.04) | <0.001 |
| Model 1 b + BMI | −0.09 (−1.15; 0.97) | 1.09 (−0.01; 2.20) | 1.61 (0.44; 2.78) | <0.001 | |
| Women | |||||
| Model 1 b | 1 | 1.65 (0.10; 3.21) | 2.33 (0.70; 3.97) | 3.22 (1.42; 5.03) | 0.002 |
| Model 1 b + BMI | 0.81 (−0.26; 1.87) | 0.85 (−0.27; 1.97) | 0.95 (−0.29; 2.19) | 0.07 | |
References
- World Health Organization. Country Health Information Profiles—China. Available online: http://www.wpro.who.int/countries/chn/5CHNpro2011_finaldraft.pdf?ua=1 (accessed on 1 August 2014).
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Disease: Report of a Joint WHO/FAO Expert Geneva. Available online: http://whqlibdoc.who.int/trs/who_trs_916.pdf (accessed on 21 June 2014).
- Lonardo, A.; Ballestri, S.; Marchesini, G.; Angulo, P.; Loria, P. Nonalcoholic fatty liver disease: A precursor of the metabolic syndrome. Dig. Liver Dis. 2015, 47, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Bertolotti, M.; Lonardo, A.; Mussi, C.; Baldelli, E.; Pellegrini, E.; Ballestri, S.; Romagnoli, D.; Loria, P. Nonalcoholic fatty liver disease and aging: Epidemiology to management. World J. Gastroenterol. 2014, 20, 14185–14204. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Kong, L.; Zhao, W.; Wan, X.; Zhai, Y.; Chen, L.; Koplan, J.P. Emergence of chronic non-communicable diseases in China. Lancet 2008, 372, 1697–1705. [Google Scholar] [CrossRef]
- Shi, Z.; Hu, X.; Yuan, B.; Hu, G.; Pan, X.; Dai, Y.; Byles, J.E.; Holmboe-Ottesen, G. Vegetable-rich food pattern is related to obesity in China. Int. J. Obes. 2008, 32, 975–984. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, L.; Jiang, Y.; Zhang, M.; Wang, L. Risk factors for noncommunicable chronic diseases in women in China: Surveillance efforts. Bull. World Health Organ. 2013, 91, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Sriboonchitta, S.; Zi, C.; Yang, Y. A study on whether economic development and urbanization of areas are associated with prevalence of obesity in Chinese adults: Findings from 2009 China Health and Nutrition Surveys. Model. Depend. Econ. 2014, 251, 289–305. [Google Scholar]
- WHO. Obesity and Overweight. Available online: http://www.who.int/dietphysicalactivity/media/en/gsfs_obesity.pdf (accessed on 6 January 2015).
- Chan, R.; Chan, D.; Lau, W.; Lo, D.; Li, L.; Woo, J. A cross-sectional study to examine the association between dietary patterns and risk of overweight and obesity in Hong Kong Chinese adolescents aged 10–12 years. J. Am. Coll. Nutr. 2014, 33, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Shang, X.; Li, Y.; Liu, A.; Zhang, Q.; Hu, X.; Du, S.; Ma, J.; Xu, G.; Li, Y.; Guo, H.; et al. Dietary pattern and its association with the prevalence of obesity and related cardiometabolic risk factors among Chinese children. PLoS ONE 2012, 7, e43183. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Buys, N.J.; Hills, A.P. Dietary pattern and its association with the prevalence of obesity, hypertension and other cardiovascular risk factors among Chinese older adults. Int. J. Environ. Res. Public Health 2014, 11, 3956–3971. [Google Scholar] [CrossRef] [PubMed]
- Batis, C.; Mendez, M.A.; Gordon-Larsen, P.; Sotres-Alvarez, D.; Adair, L.; Popkin, B. Using both principal component analysis and reduced rank regression to study dietary patterns and diabetes in Chinese adults. Public Health Nutr. 2015. [Google Scholar] [CrossRef]
- Xu, X.; Byles, J.E.; Shi, Z.; Hall, J.J. Evaluation of older Chinese people’s macronutrient intake status: Results from the China Health and Nutrition Survey. Br. J. Nutr. 2015, 113, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Hall, J.; Byles, J.; Shi, Z. Do older Chinese people’s diets meet the Chinese Food Pagoda guidelines? Results from the China Health and Nutrition Survey 2009. Public Health Nutr. 2015, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. Urbanization, lifestyle changes and the nutrition transition. World Dev. 1999, 27, 1905–1916. [Google Scholar] [CrossRef]
- Carolina Population Center. China Health and Nutrition Survey. Available online: http://www.cpc.unc.edu/projects/china (accessed on 1 December 2013).
- Liu, F. New trends in China’s regional economic development. In Regional Economic Development in China; Swee-Hock, S., Wong, J., Eds.; Singapore Institute of Southeast Asian Studies: Kent Ridge, Singapore, 2009; pp. 9–14. [Google Scholar]
- Li, Y.; He, Y.; Zhai, F.; Yang, X.; Hu, X.; Zhao, W.; Ma, G.S. Comparison of assessment of food intakes by using 3 dietary survey methods. Clin. J. Prev. Med. 2006, 40, 273–280. [Google Scholar]
- Batis, C.; Sotres-Alvarez, D.; Gordon-Larsen, P.; Mendez, M.A.; Adair, L.; Popkin, B. Longitudinal analysis of dietary patterns in Chinese adults from 1991 to 2009. Br. J. Nutr. 2014, 111, 1441–1451. [Google Scholar] [CrossRef] [PubMed]
- China Institute of Nutrition and Food Safety, China CDC. China Food Composition Table; Peking University Medical Press: Beijing, China, 2002. [Google Scholar]
- Zhou, B. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults: Study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed. Environ. Sci. 2002, 15, 83–96. [Google Scholar] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, J.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Zuo, H.; Shi, Z.; Yuan, B.; Dai, Y.; Hu, G.; Wu, G.; Hussain, A. Interaction between physical activity and sleep duration in relation to insulin resistance among non-diabetic Chinese adults. BMC Public Health 2012, 12, 247. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Li, J.; Li, S.; Zhang, B.; Du, S.; Gordon-Larsen, P.; Adair, L.; Popkin, B. The expanding burden of cardiometabolic risk in China: The China Health and Nutrition Survey. Obes. Rev. 2012, 13, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, K.; Thomassin, P.J. Economic impact of adopting a healthy diet in Canada. J. Public Health 2012, 20, 639–652. [Google Scholar] [CrossRef]
- Thompson, M.L.; Myers, J.; Kriebel, D. Prevalence odds ratio or prevalence ratio in the analysis of cross sectional data: What is to be done? Occup. Environ. Med. 1998, 55, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Barros, A.J.; Hirakata, V.N. Alternatives for logistic regression in cross-sectional studies: An empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 2003, 3, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stata Statistical Software: Release 13, StataCorp LP: College Station, TX, USA, 2013.
- Shi, Z.; Yuan, B.; Hu, G.; Dai, Y.; Zuo, H.; Holmboe-Ottesen, G. Dietary pattern and weight change in a 5-year follow-up among Chinese adults: Results from the Jiangsu Nutrition Study. Br. J. Nutr. 2011, 105, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Villegas, A.; Bes-Rastrollo, M.; Martinez-Gonzalez, M.; Serra-Majem, L. Adherence to a Mediterranean dietary pattern and weight gain in a follow-up study: The SUN cohort. Int. J. Obes. 2005, 30, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Cheung, B.; Ho, S.; Sham, A.; Lam, T. Influence of dietary pattern on the development of overweight in a Chinese population. Eur. J. Clin. Nutr. 2007, 62, 480–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chinese Nutrition Society. Pagoda Illustration. Available online: http://www.cnsoc.org/en/nutrition.asp?s=9&nid=806 (accessed on 6 April 2014).
- Hu, E.; Pan, A.; Malik, V.; Sun, Q. White rice consumption and risk of type 2 diabetes: Meta-analysis and systematic review. BMJ 2012, 344, e1457. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Jo, I.; Joung, H. A rice-based traditional dietary pattern is associated with obesity in Korean adults. J. Acad. Nutr. Diet. 2012, 112, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Kolahdouzan, M.; Khosravi-Boroujeni, H.; Nikkar, B.; Zakizadeh, E.; Abedi, B.; Ghazavi, N.; Ayoobi, N.; Vatankhah, M. The association between dietary intake of white rice and central obesity in obese adults. ARYA Atheroscler. 2013, 9, 140–144. [Google Scholar] [PubMed]
- Shi, Z.; Taylor, A.W.; Hu, G.; Gill, T.; Wittert, G.A. Rice intake, weight change and risk of the metabolic syndrome development among Chinese adults: The Jiangsu Nutrition Study (JIN). Asia Pac. J. Clin. Nitr. 2012, 21, 35–43. [Google Scholar]
- Hooper, L.; Abdelhamid, A.; Moore, H.J.; Douthwaite, W.; Skeaff, C.M.; Summerbell, C.D. Effect of reducing total fat intake on body weight: Systematic review and meta-analysis of randomised controlled trials and cohort studies. BMJ 2012, 345, e7666. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Hall, J.; Byles, J.; Shi, Z.; The University of Newcastle, New Lambton Heights, NSW, Australia. Unpublished work. 2015.
- Brownie, S. Why are elderly individuals at risk of nutritional deficiency? Int. J. Nurs. Pract. 2005, 12, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Hall, J.; Byles, J.; Shi, Z. Assessing dietary quality of older Chinese people using the Chinese Diet Balance Index (DBI). PLoS ONE 2015, 10, e0121618. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, X.; Hall, J.; Byles, J.; Shi, Z. Dietary Pattern Is Associated with Obesity in Older People in China: Data from China Health and Nutrition Survey (CHNS). Nutrients 2015, 7, 8170-8188. https://doi.org/10.3390/nu7095386
Xu X, Hall J, Byles J, Shi Z. Dietary Pattern Is Associated with Obesity in Older People in China: Data from China Health and Nutrition Survey (CHNS). Nutrients. 2015; 7(9):8170-8188. https://doi.org/10.3390/nu7095386
Chicago/Turabian StyleXu, Xiaoyue, John Hall, Julie Byles, and Zumin Shi. 2015. "Dietary Pattern Is Associated with Obesity in Older People in China: Data from China Health and Nutrition Survey (CHNS)" Nutrients 7, no. 9: 8170-8188. https://doi.org/10.3390/nu7095386