
A Systematic Review of Studies Examining Associations between Sleep Characteristics with Dietary Intake and Eating Behaviors during Pregnancy
 ,
,
Abstract
:1. Introduction
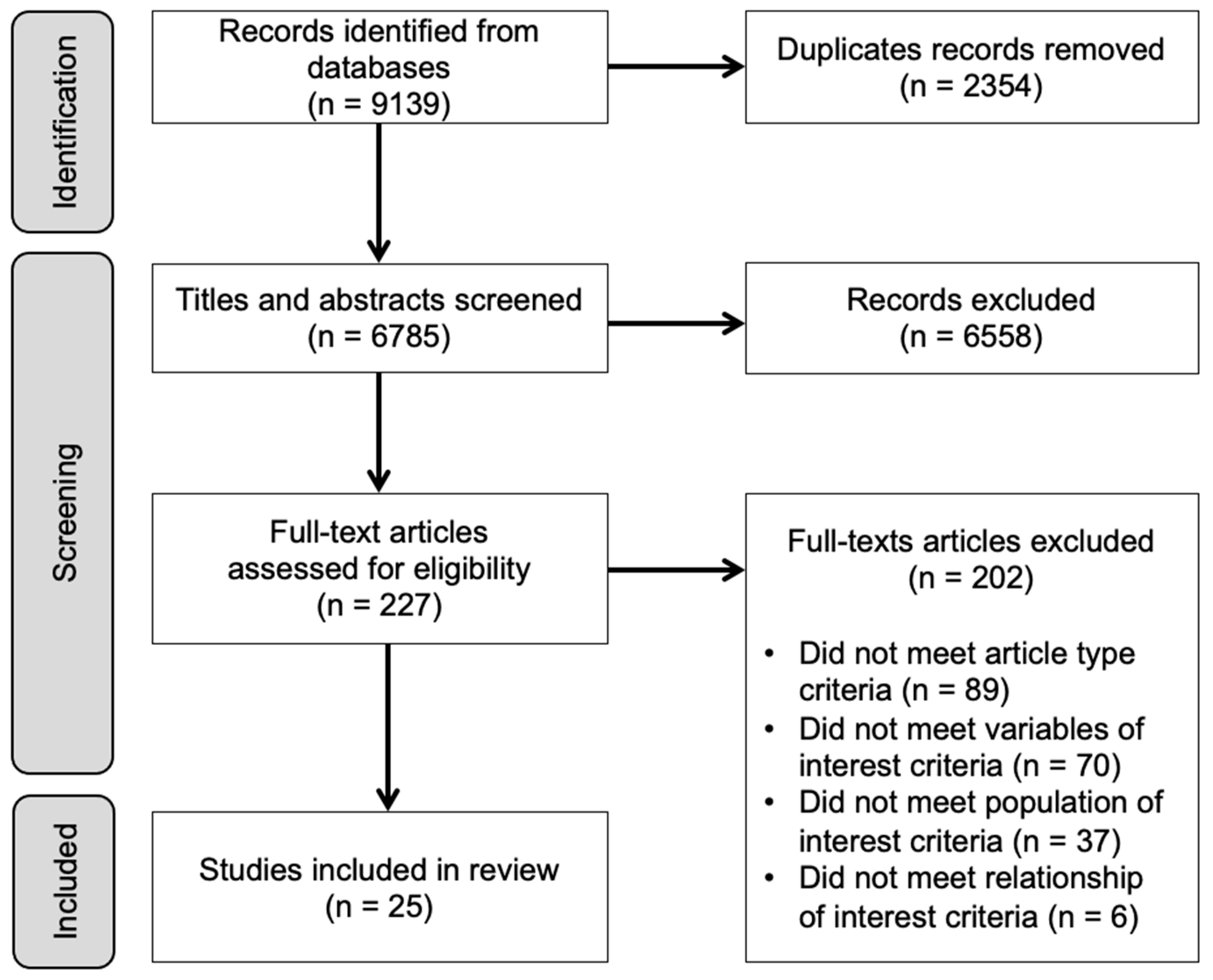
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Screening and Eligibility Criteria
2.4. Data Extraction
3. Results
3.1. Maternal Sleep with Energy or Nutrient Intake (N = 12)
3.2. Sleep Variables and Energy Intake
3.3. Sleep Variables and Nutrient Intake
3.4. Maternal Sleep with Dietary Patterns (N = 9 Studies)
3.5. Maternal Sleep with Eating Behaviors (N = 11 Studies)
3.6. Maternal Exposures with Fetal/Infant Outcomes (N = 5 Studies)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy
| 1 | Birthing Centers/(819) |
| 2 | Maternal Health/(1765) |
| 3 | exp Maternal Health Services/(52223) |
| 4 | Maternal-Fetal Relations/(925) |
| 5 | Maternal-Child Nursing/(1939) |
| 6 | exp Pregnancy/(920493) |
| 7 | exp Pregnancy Complications/(438930) |
| 8 | Pregnant Women/or Surrogate Mothers/(11325) |
| 9 | exp delivery, obstetric/(83094) |
| 10 | (antenatal or gestat* or maternal* or maternity or perinatal or pregnan* or prenatal or surroga*).ti,ab,kf. (933301) |
| 11 | or/1–10 (1331767) |
| 12 | exp Sleep/(83550) |
| 13 | exp Sleep Wake Disorders/(94508) |
| 14 | Sleep Medicine Specialty/(387) |
| 15 | sleepiness/(455) |
| 16 | (sleep* or slept or somnolen*).ti,ab,kf. (201971) |
| 17 | (dream* or REM or rapid eye movement* or non-REM or NREM).ti,ab,kf. (31925) |
| 18 | (drowsy or drowsiness).ti,ab,kf. (7064) |
| 19 | or/12–18 (248547) |
| 20 | exp “diet, food, and nutrition”/(1778723) |
| 21 | exp Plants, Edible/(46593) |
| 22 | exp Dietary Services/(7054) |
| 23 | exp “Feeding and Eating Disorders”/(31946) |
| 24 | exp Nutrition Therapy/(104976) |
| 25 | nutritional sciences/or dietetics/or nutrigenomics/(18726) |
| 26 | exp Nutrition Policy/(11681) |
| 27 | exp Food Industry/(190037) |
| 28 | (diet* or supplement*).ti,ab,kf. (875322) |
| 29 | (eat or eaten or eats or eating or ate or cook*).ti,ab,kf. (143528) |
| 30 | (food* or fed or feed*).ti,ab,kf. (1035612) |
| 31 | (calorie* or caloric or high-calorie* or low-calorie* or high-caloric* or low-caloric*).ti,ab,kf. (46685) |
| 32 | (macro-nutrient* or macronutrient* or nutrition* or nutrient* or nutritive*).ti,ab,kf. (449174) |
| 33 | (consume? or consuming or consumption).ti,ab,kf. (475613) |
| 34 | energy.ti,ab,kf. (687974) |
| 35 | (intake or ingest*).ti,ab,kf. (373987) |
| 36 | (carbohydrate* or high-carb* or low-carb* or sugar*).ti,ab,kf. (266900) |
| 37 | (fat or fats or fat-rich or fat-heavy or fatty or high-fat* or low-fat* or omega-3* or omega-6* or oil or oils).ti,ab,kf. (657162) |
| 38 | (amino acid* or high-protein* or low-protein* or protein*).ti,ab,kf. (3425839) |
| 39 | (cholesterol or high-cholesterol or HDL or low-cholesterol or LDL or lipoprotein*).ti,ab,kf. (334576) |
| 40 | (dairy or fish or fruit* or vegetable* or meat or seafood or vegan* or vegetarian* or nonvegetarian* or non-vegetarian* or paleo* or pescatarian or keto* or mediterranean or meal or meals).ti,ab,kf. (648313) |
| 41 | (butter* or ghee* or milk*).ti,ab,kf. (149412) |
| 42 | (superfood* or probiotic*).ti,ab,kf. (28331) |
| 43 | (hunger or hungry or malnutrition).ti,ab,kf. (55056) |
| 44 | or/20–43 (7595460) |
| 45 | 11 and 19 and 44 (2520) |
| S48 | S11 AND S18 AND S47 |
| S47 | S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 OR S34 OR S35 OR S36 OR S37 OR S38 OR S39 OR S40 OR S41 OR S42 OR S43 OR S44 OR S45 OR S46 |
| S46 | TI (hunger or hungry or malnutrition) OR AB (hunger or hungry or malnutrition) |
| S45 | TI (superfood* or probiotic*) OR AB (superfood* or probiotic*) |
| S44 | TI (butter* or ghee* or milk*) OR AB (butter* or ghee* or milk*) |
| S43 | TI (dairy or fish or fruit* or vegetable* or meat or seafood or vegan* or vegetarian* or nonvegetarian* or non-vegetarian* or paleo* or pescatarian or keto* or mediterranean or meal or meals) OR AB (dairy or fish or fruit* or vegetable* or meat or seafood or vegan* or vegetarian* or nonvegetarian* or non-vegetarian* or paleo* or pescatarian or keto* or mediterranean or meal or meals) |
| S42 | TI (cholesterol or high-cholesterol or HDL or low-cholesterol or LDL or lipoprotein*) OR AB (cholesterol or high-cholesterol or HDL or low-cholesterol or LDL or lipoprotein*) |
| S41 | TI (amino acid* or high-protein* or low-protein* or protein*) OR AB (amino acid* or high-protein* or low-protein* or protein*) |
| S40 | TI (fat or fats or fat-rich or fat-heavy or fatty or high-fat* or low-fat* or omega-3* or omega-6* or oil or oils) OR AB (fat or fats or fat-rich or fat-heavy or fatty or high-fat* or low-fat* or omega-3* or omega-6* or oil or oils) |
| S39 | TI (carbohydrate* or high-carb* or low-carb* or sugar*) OR AB (carbohydrate* or high-carb* or low-carb* or sugar*) |
| S38 | TI (intake or ingest*) OR AB (intake or ingest*) |
| S37 | TI energy OR AB energy |
| S36 | TI (consume# or consuming or consumption) OR AB (consume# or consuming or consumption) |
| S35 | TI (macro-nutrient* or macronutrient* or nutrition* or nutrient* or nutritive*) OR AB (macro-nutrient* or macronutrient* or nutrition* or nutrient* or nutritive*) |
| S34 | TI (calorie* or caloric or high-calorie* or low-calorie* or high-caloric* or low-caloric*) OR AB (calorie* or caloric or high-calorie* or low-calorie* or high-caloric* or low-caloric*) |
| S33 | TI (food* or fed or feed*) OR AB (food* or fed or feed*) |
| S32 | TI (eat or eaten or eats or eating or ate or cook*) OR AB (eat or eaten or eats or eating or ate or cook*) |
| S31 | TI (diet* or supplement*) OR AB (diet* or supplement*) |
| S30 | (MH “Food Security”) |
| S29 | (MH “Food Industry+”) |
| S28 | (MH “Nutrition Policy+”) |
| S27 | (MH “Sports Nutritional Sciences”) OR (MH “Dietetics”) OR (MH “Research, Dietetics”) OR (MH “Nutrigenomics+”) |
| S26 | (MH “Diet Therapy+”) |
| S25 | (MH “Eating Disorders+”) |
| S24 | (MH “Nutrition Services+”) |
| S23 | (MH “Plants, Edible+”) |
| S22 | (MH “Eating Behavior+”) OR (MH “Drinking Behavior+”) |
| S21 | (MH “Nutritional Physiology”) OR (MH “Nutritive Value+”) OR (MH “Digestive System Physiology+”) |
| S20 | (MH “Food and Beverages+”) |
| S19 | (MH “Nutrition+”) |
| S18 | S12 OR S13 OR S14 OR S15 OR S16 OR S17 |
| S17 | TI ((drowsy or drowsiness)) OR AB ((drowsy or drowsiness)) |
| S16 | TI ((dream* or REM or “rapid eye movement*” or non-REM or NREM)) OR AB ((dream* or REM or “rapid eye movement*” or non-REM or NREM)) |
| S15 | I ((sleep* or slept or somnolen*)) OR AB ((sleep* or slept or somnolen*)) |
| S14 | (MH “Sleepiness”) |
| S13 | (MH “Sleep Disorders+”) |
| S12 | (MH “Sleep+”) |
| S11 | S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 |
| S10 | TI ((antenatal or gestat* or maternal* or maternity or perinatal or pregnan* or prenatal or surroga*)) OR AB ((antenatal or gestat* or maternal* or maternity or perinatal or pregnan* or prenatal or surroga*)) |
| S9 | (MH “Delivery, Obstetric+”) |
| S8 | (MH “Expectant Mothers”) OR (MH “Surrogate Mothers”) |
| S7 | (MH “Pregnancy Complications+”) |
| S6 | (MH “Pregnancy+”) |
| S5 | (MH “Maternal-Child Nursing”) OR (MH “Obstetric Nursing”) OR (MH “Perinatal Nursing”) |
| S4 | (MH “Prenatal Bonding”) |
| S3 | (MH “Maternal Health Services+”) |
| S2 | (MH “Obstetric Care+”) |
| S1 | (MH “Delivery Rooms+”) |
References
- Cai, S.; Tan, S.; Gluckman, P.D.; Godfrey, K.M.; Saw, S.M.; Teoh, O.H.; Chong, Y.-S.; Meaney, M.J.; Kramer, M.S.; Gooley, J.J.; et al. Sleep Quality and Nocturnal Sleep Duration in Pregnancy and Risk of Gestational Diabetes Mellitus. Sleep 2017, 40, zsw058. [Google Scholar] [CrossRef] [Green Version]
- Rawal, S.; Hinkle, S.N.; Zhu, Y.; Albert, P.S.; Zhang, C. A longitudinal study of sleep duration in pregnancy and subsequent risk of gestational diabetes: Findings from a prospective, multiracial cohort. Am. J. Obstet. Gynecol. 2017, 216, 399.e1–399.e8. [Google Scholar] [CrossRef] [Green Version]
- Sedov, I.D.; Cameron, E.E.; Madigan, S.; Tomfohr-Madsen, L.M. Sleep quality during pregnancy: A meta-analysis. Sleep Med. Rev. 2018, 38, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Pengo, M.F.; Won, C.H.; Bourjeily, G. Sleep in Women Across the Life Span. Chest 2018, 154, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Pauley, A.M.; Moore, G.A.; Mama, S.K.; Molenaar, P.; Symons Downs, D. Associations between prenatal sleep and psychological health: A systematic review. J. Clin. Sleep Med. 2020, 16, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Paine, S.J.; Signal, T.L.; Sweeney, B.; Priston, M.; Muller, D.; Smith, A.; Huthwaite, M.; Gander, P.; Lee, K. Maternal sleep disturbances in late pregnancy and the association with emergency caesarean section: A prospective cohort study. Sleep Health 2020, 6, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Zhang, X.; Wang, Y.; Li, J.; Xu, Y.; Song, X.; Su, S.; Zhu, X.; Vitiello, M.V.; Shi, J.; et al. Sleep disturbances during pregnancy and adverse maternal and fetal outcomes: A systematic review and meta-analysis. Sleep Med. Rev. 2021, 58, 101436. [Google Scholar] [CrossRef]
- Bourjeily, G.; Danilack, V.A.; Bublitz, M.H.; Lipkind, H.; Muri, J.; Caldwell, D.; Tong, I.; Rosene-Montella, K. Obstructive sleep apnea in pregnancy is associated with adverse maternal outcomes: A national cohort. Sleep Med. 2017, 38, 50–57. [Google Scholar] [CrossRef]
- Bourjeily, G.; Raker, C.A.; Chalhoub, M.; Miller, M.A. Pregnancy and fetal outcomes of symptoms of sleep-disordered breathing. Eur. Respir. J. 2010, 36, 849–855. [Google Scholar] [CrossRef] [Green Version]
- Facco, F.L.; Parker, C.B.; Reddy, U.M.; Silver, R.M.; Koch, M.A.; Louis, J.M.; Basner, R.C.; Chung, J.H.; Nhan-Chang, C.-L.; Pien, G.W.; et al. Association Between Sleep-Disordered Breathing and Hypertensive Disorders of Pregnancy and Gestational Diabetes Mellitus. Obstet. Gynecol. 2017, 129, 31–41. [Google Scholar] [CrossRef]
- Louis, J.M.; Mogos, M.F.; Salemi, J.L.; Redline, S.; Salihu, H.M. Obstructive sleep apnea and severe maternal-infant morbidity/mortality in the United States, 1998–2009. Sleep 2014, 37, 843–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bublitz, M.H.; Sharp, M.; Freeburg, T.; Sanapo, L.; Nugent, N.R.; Sharkey, K.; Bourjeily, G. Sleep Disordered Breathing Measures in Early Pregnancy Are Associated with Depressive Symptoms in Late Pregnancy. Diagnostics 2021, 11, 858. [Google Scholar] [CrossRef] [PubMed]
- Bourjeily, G.; Danilack, V.A.; Bublitz, M.H.; Muri, J.; Rosene-Montella, K.; Lipkind, H. Maternal obstructive sleep apnea and neonatal birth outcomes in a population based sample. Sleep Med. 2020, 66, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Kendle, A.M.; Salemi, J.L.; Jackson, C.L.; Buysse, D.J.; Louis, J.M. Insomnia during pregnancy and severe maternal morbidity in the united states: Nationally representative data from 2006 to 2017. Sleep 2022, 45, zsac175. [Google Scholar] [CrossRef] [PubMed]
- Izci Balserak, B.; Hermann, R.; Hernandez, T.L.; Buhimschi, C.; Park, C. Evening blue-light exposure, maternal glucose, and infant birthweight. Ann. N. Y. Acad. Sci. 2022, 1515, 276–284. [Google Scholar] [CrossRef]
- Facco, F.L.; Parker, C.B.; Hunter, S.; Reid, K.J.; Zee, P.P.; Silver, R.M.; Pien, G.; Chung, J.H.; Louis, J.M.; Haas, D.M.; et al. Later sleep timing is associated with an increased risk of preterm birth in nulliparous women. Am. J. Obstet. Gynecol. MFM 2019, 1, 100040. [Google Scholar] [CrossRef]
- Procter, S.B.; Campbell, C.G. Position of the Academy of Nutrition and Dietetics: Nutrition and lifestyle for a healthy pregnancy outcome. J. Acad. Nutr. Diet. 2014, 114, 1099–1103. [Google Scholar] [CrossRef]
- Tsakiridis, I.; Kasapidou, E.; Dagklis, T.; Leonida, I.; Leonida, C.; Bakaloudi, D.R.; Chourdakis, M. Nutrition in Pregnancy: A Comparative Review of Major Guidelines. Obstet. Gynecol. Surv. 2020, 75, 692–702. [Google Scholar] [CrossRef]
- Rahmati, S.; Azami, M.; Badfar, G.; Parizad, N.; Sayehmiri, K. The relationship between maternal anemia during pregnancy with preterm birth: A systematic review and meta-analysis. J. Matern. Fetal Neonatal Med. 2020, 33, 2679–2689. [Google Scholar] [CrossRef]
- Shi, H.; Chen, L.; Wang, Y.; Sun, M.; Guo, Y.; Ma, S.; Wang, X.; Jiang, H.; Wang, X.; Lu, J.; et al. Severity of Anemia During Pregnancy and Adverse Maternal and Fetal Outcomes. JAMA Netw. Open 2022, 5, e2147046. [Google Scholar] [CrossRef]
- Caut, C.; Leach, M.; Steel, A. Dietary guideline adherence during preconception and pregnancy: A systematic review. Matern. Child Nutr. 2020, 16, e12916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keats, E.C.; Haider, B.A.; Tam, E.; Bhutta, Z.A. Multiple-micronutrient supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2019, 3, CD004905. [Google Scholar] [CrossRef] [PubMed]
- Wikoff, D.; Welsh, B.T.; Henderson, R.; Brorby, G.P.; Britt, J.; Myers, E.; Goldberger, J.; Lieberman, H.R.; O’Brien, C.; Peck, J.; et al. Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem. Toxicol. 2017, 109 Pt 1, 585–648. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, R.; Dreibelbis, C.; Kingshipp, B.L.; Wong, Y.P.; Abrams, B.; Gernand, A.D.; Rasmussen, K.M.; Siega-Riz, A.M.; Stang, J.; O Casavale, K.; et al. Dietary patterns before and during pregnancy and maternal outcomes: A systematic review. Am. J. Clin. Nutr. 2019, 109 (Suppl. 7), 705s–728s. [Google Scholar] [CrossRef]
- Raghavan, R.; Dreibelbis, C.; Kingshipp, B.L.; Wong, Y.P.; Abrams, B.; Gernand, A.D.; Rasmussen, K.M.; Siega-Riz, A.M.; Stang, J.; O Casavale, K.; et al. Dietary patterns before and during pregnancy and birth outcomes: A systematic review. Am. J. Clin. Nutr. 2019, 109 (Suppl. 7), 729s–756s. [Google Scholar] [CrossRef]
- Shapiro, A.L.; Kaar, J.L.; Crume, T.L.; Starling, A.P.; Siega-Riz, A.M.; Ringham, B.M.; Glueck, D.H.; Norris, J.M.; A Barbour, L.; E Friedman, J.; et al. Maternal diet quality in pregnancy and neonatal adiposity: The Healthy Start Study. Int. J. Obes. (Lond.) 2016, 40, 1056–1062. [Google Scholar] [CrossRef] [Green Version]
- Khaled, K.; Hundley, V.; Tsofliou, F. Poor Dietary Quality and Patterns Are Associated with Higher Perceived Stress among Women of Reproductive Age in the UK. Nutrients 2021, 13, 2588. [Google Scholar] [CrossRef]
- Hanson, M.A.; Bardsley, A.; De-Regil, L.M.; Moore, S.E.; Oken, E.; Poston, L.; Ma, R.C.; McAuliffe, F.M.; Maleta, K.; Purandare, C.N.; et al. The International Federation of Gynecology and Obstetrics (FIGO) recommendations on adolescent, preconception, and maternal nutrition: “Think Nutrition First”. Int. J. Gynaecol. Obstet. 2015, 131 (Suppl. 4), S213–S253. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence, Royal College of Obstetricians & Gynaecologists. Antenatal Care (NG201) National Institute for Health and Care Excellence. 2021. Available online: www.nice.org.uk/guidance/ng201 (accessed on 29 April 2023).
- O’Connor, D.L.; Blake, J.; Bell, R.; Bowen, A.; Callum, J.; Fenton, S.; Gray-Donald, K.; Rossiter, M.; Adamo, K.; Brett, K.; et al. Canadian Consensus on Female Nutrition: Adolescence, Reproduction, Menopause, and Beyond. J. Obstet. Gynaecol. Can. 2016, 38, 508–554.e18. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience Geneva; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/publications/i/item/9789241549912 (accessed on 29 April 2023).
- Abdollahi, S.; Soltani, S.; de Souza, R.J.; Forbes, S.C.; Toupchian, O.; Salehi-Abargouei, A. Associations between Maternal Dietary Patterns and Perinatal Outcomes: A Systematic Review and Meta-Analysis of Cohort Studies. Adv. Nutr. 2021, 12, 1332–1352. [Google Scholar] [CrossRef]
- Chia, A.R.; Chen, L.W.; Lai, J.S.; Wong, C.H.; Neelakantan, N.; van Dam, R.M.; Chong, M.F.-F. Maternal Dietary Patterns and Birth Outcomes: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 685–695. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Nahm, S.; Marchesoni, J.; Maity, A.; Maguire, R.L.; House, J.S.; Tucker, R.; Atkinson, T.; Murphy, S.K.; Hoyo, C. Maternal Mediterranean Diet Adherence and Its Associations with Maternal Prenatal Stressors and Child Growth. Curr. Dev. Nutr. 2022, 6, nzac146. [Google Scholar] [CrossRef] [PubMed]
- Dayi, T.; Ozgoren, M. Effects of the Mediterranean diet on the components of metabolic syndrome. J. Prev. Med. Hyg. 2022, 63 (Suppl. 3), E56–E64. [Google Scholar]
- AlAufi, N.S.; Chan, Y.M.; Waly, M.I.; Chin, Y.S.; Mohd Yusof, B.N.; Ahmad, N. Application of Mediterranean Diet in Cardiovascular Diseases and Type 2 Diabetes Mellitus: Motivations and Challenges. Nutrients 2022, 14, 2777. [Google Scholar] [CrossRef] [PubMed]
- Zaragoza-Marti, A.; Ruiz-Rodenas, N.; Herranz-Chofre, I.; Sanchez-SanSegundo, M.; Serrano Delgado, V.C.; Hurtado-Sanchez, J.A. Adherence to the Mediterranean Diet in Pregnancy and Its Benefits on Maternal-Fetal Health: A Systematic Review of the Literature. Front. Nutr. 2022, 9, 813942. [Google Scholar] [CrossRef] [PubMed]
- Jeukendrup, A.E. Periodized Nutrition for Athletes. Sports Med. 2017, 47 (Suppl. 1), 51–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tahara, Y.; Shibata, S. Chrono-biology, chrono-pharmacology, and chrono-nutrition. J. Pharmacol. Sci. 2014, 124, 320–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peuhkuri, K.; Sihvola, N.; Korpela, R. Diet promotes sleep duration and quality. Nutr. Res. 2012, 32, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Pot, G.K. Sleep and dietary habits in the urban environment: The role of chrono-nutrition. Proc. Nutr. Soc. 2018, 77, 189–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Khatib, H.K.; Harding, S.V.; Darzi, J.; Pot, G.K. The effects of partial sleep deprivation on energy balance: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2017, 71, 614–624. [Google Scholar] [CrossRef]
- Pauley, A.M.; Moore, G.A.; Mama, S.K.; Molenaar, P.; Downs, D.S. Systematic review of the associations between prenatal sleep behaviours and components of energy balance for regulating weight gain. J. Sleep Res. 2023, 32, e13619. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Melnyk, B.M.F.; Fineout-Overholt, E. Box 1.3: Rating system for the hierarchy of evidence for intervention/treatment questions. In Evidence-Based Practice in Nursing & Healthcare: A Guide to Best Practice, 3rd ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2015; p. 11. [Google Scholar]
- Pauley, A.M.; Hohman, E.E.; Leonard, K.S.; Guo, P.; McNitt, K.M.; Rivera, D.E.; Savage, J.S.; Downs, D.S. Short Nighttime Sleep Duration and High Number of Nighttime Awakenings Explain Increases in Gestational Weight Gain and Decreases in Physical Activity but Not Energy Intake among Pregnant Women with Overweight/Obesity. Clocks Sleep 2020, 2, 487–501. [Google Scholar] [CrossRef]
- Phelan, S.; Wing, R.R.; Brannen, A.; McHugh, A.; Hagobian, T.A.; Schaffner, A.; Jelalian, E.; Hart, C.N.; O Scholl, T.; Munoz-Christian, K.; et al. Randomized controlled clinical trial of behavioral lifestyle intervention with partial meal replacement to reduce excessive gestational weight gain. Am. J. Clin. Nutr. 2018, 107, 183–194. [Google Scholar] [CrossRef] [Green Version]
- Allison, K.C.; Wrotniak, B.H.; Paré, E.; Sarwer, D.B. Psychosocial Characteristics and Gestational Weight Change among Overweight, African American Pregnant Women. Obstet. Gynecol. Int. 2012, 2012, 878607. [Google Scholar] [CrossRef] [Green Version]
- Bennett, C.J.; Cain, S.W.; Blumfield, M.L. Monounsaturated fat intake is associated with improved sleep quality in pregnancy Short Nighttime Sleep Duration and High Number of Nighttime Awakenings Explain Increases in Gestational Weight Gain and Decreases in Physical Activity but Not Energy Intake among Pregnant Women with Overweight/Obesity. Midwifery 2019, 78, 64–70. [Google Scholar]
- Chang, M.W.; Brown, R.; Nitzke, S.; Smith, B.; Eghtedary, K. Stress, sleep, depression and dietary intakes among low-income overweight and obese pregnant women. Matern. Child Health J. 2015, 19, 1047–1059. [Google Scholar] [CrossRef] [PubMed]
- Devoe, L.D.; Murray, C.; Arnaud, M. Maternal caffeine consumption and fetal behavior in normal third-trimester pregnancy. Am. J. Obstet. Gynecol. 1993, 168, 1105–1111; discussion 1111–1112. [Google Scholar] [CrossRef] [PubMed]
- Diego, M.F.T.; Hernandez-Reif, M.; Vera, Y.; Gil, K.; Gonzalez-Garcia, A. Caffeine Use Affects Pregnancy Outcome. J. Child Adolesc. Subst. Abus. 2008, 17, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Du, M.; Liu, J.; Han, N.; Zhao, Z.; Luo, S.; Wang, H. Association between sleep duration in early pregnancy and risk of gestational diabetes mellitus: A prospective cohort study. Diabetes Metab. 2021, 47, 101217. [Google Scholar] [CrossRef]
- Du, M.; Liu, J.; Han, N.; Zhao, Z.; Yang, J.; Xu, X.; Luo, S.; Wang, H. Maternal sleep quality during early pregnancy, risk factors and its impact on pregnancy outcomes: A prospective cohort study. Sleep Med. 2021, 79, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Duke, C.H.; Williamson, J.A.; Snook, K.R.; Finch, K.C.; Sullivan, K.L. Association Between Fruit and Vegetable Consumption and Sleep Quantity in Pregnant Women. Matern. Child Health J. 2017, 21, 966–973. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, E.W.; Most, J.; Broskey, N.T.; Altazan, A.D.; Beyl, R.A.; Keadle, S.K.; Drews, K.L.; Singh, P.; Redman, L.M. Identification of changes in sleep across pregnancy and the impact on cardiometabolic health and energy intake in women with obesity. Sleep Med. 2021, 77, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Flor-Alemany, M.; Nestares, T.; Alemany-Arrebola, I.; Marin-Jimenez, N.; Borges-Cosic, M.; Aparicio, V.A. Influence of Dietary Habits and Mediterranean Diet Adherence on Sleep Quality during Pregnancy. The GESTAFIT Project. Nutrients 2020, 12, 3569. [Google Scholar] [CrossRef]
- Gontijo, C.A.; Cabral, B.B.M.; Balieiro, L.C.T.; Teixeira, G.P.; Fahmy, W.M.; Maia, Y.C.P.; Crispim, C.A. Time-related eating patterns and chronotype are associated with diet quality in pregnant women. Chronobiol. Int. 2019, 36, 75–84. [Google Scholar] [CrossRef]
- Gordon, L.K.; Mason, K.A.; Mepham, E.; Sharkey, K.M. A mixed methods study of perinatal sleep and breastfeeding outcomes in women at risk for postpartum depression. Sleep Health 2021, 7, 353–361. [Google Scholar] [CrossRef]
- Loy, S.L.; Cheung, Y.B.; Cai, S.; Colega, M.T.; Godfrey, K.M.; Chong, Y.S.; Shek, L.; Tan, K.H.; Chong, M.F.-F.; Yap, F.; et al. Maternal night-time eating and sleep duration in relation to length of gestation and preterm birth. Clin. Nutr. 2020, 39, 1935–1942. [Google Scholar] [CrossRef]
- Quach, D.T.; Le, Y.T.; Mai, L.H.; Hoang, A.T.; Nguyen, T.T. Short Meal-to-Bed Time Is a Predominant Risk Factor of Gastroesophageal Reflux Disease in Pregnancy Association Between Fruit and Vegetable Consumption and Sleep Quantity in Pregnant Women: A mixed methods study of perinatal sleep and breastfeeding outcomes in women at risk for postpartum depression. J. Clin. Gastroenterol. 2021, 55, 316–320. [Google Scholar]
- Santos, I.S.; Matijasevich, A.; Domingues, M.R. Maternal caffeine consumption and infant nighttime waking: Prospective cohort study. Pediatrics 2012, 129, 860–868. [Google Scholar] [CrossRef] [Green Version]
- Sugimori, N.; Hamazaki, K.; Matsumura, K.; Kasamatsu, H.; Tsuchida, A.; Inadera, H.; Japan Environment and Children’s Study Group. Association between maternal fermented food consumption and infant sleep duration: The Japan Environment and Children’s Study. PLoS ONE 2019, 14, e0222792. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, G.P.; Balieiro, L.C.T.; Gontijo, C.A.; Fahmy, W.M.; Maia, Y.C.P.; Crispim, C.A. The association between chronotype, food craving and weight gain in pregnant women Time-related eating patterns and chronotype are associated with diet quality in pregnant women Sleep disturbances and binge eating disorder symptoms during and after pregnancy. J. Hum. Nutr. Diet. 2020, 33, 342–350. [Google Scholar] [PubMed]
- Ulman, T.F.; Von Holle, A.; Torgersen, L.; Stoltenberg, C.; Reichborn-Kjennerud, T.; Bulik, C.M. Sleep disturbances and binge eating disorder symptoms during and after pregnancy. Sleep 2012, 35, 1403–1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Lee, L.; Chia, A.R.; Loy, S.L.; Colega, M.; Tham, E.K.H.; Cai, S.; Yap, F.; Godfrey, K.M.; Teoh, O.H.; Goh, D.; et al. Sleep and Dietary Patterns in Pregnancy: Findings from the GUSTO Cohort. Int. J. Environ. Res. Public Health 2017, 14, 1409. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.L.; Libby, B.A.; Moore Simas, T.A.; Waring, M.E. Sugar-Sweetened Beverage Consumption and Sleep Duration and Quality Among Pregnant Women. J. Nutr. Educ. Behav. 2021, 53, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Wołyńczyk-Gmaj, D.; Różańska-Walędziak, A.; Ziemka, S.; Ufnal, M.; Brzezicka, A.; Gmaj, B.; Januszko, P.; Fudalej, S.; Czajkowski, K.; Wojnar, M. Insomnia in Pregnancy Is Associated With Depressive Symptoms and Eating at Night. J. Clin. Sleep Med. 2017, 13, 1171–1176. [Google Scholar] [CrossRef] [PubMed]
- Zhan, Y.; Ma, H.; Feng, Y.; Wang, Y.; Wu, S.; Cai, S.; Shi, Y.; Chen, Y.; Ma, L.; Jiang, Y. Dietary patterns in relation to gestational depression and sleep disturbance in Chinese pregnant women Identification of changes in sleep across pregnancy and the impact on cardiometabolic health and energy intake in women with obesity. J. Obstet. Gynaecol. Res. 2020, 77, 120–127. [Google Scholar]
- Betts, G.M.; Lipsky, L.M.; Temmen, C.D.; Siega-Riz, A.M.; Faith, M.S.; Nansel, T.R. Poorer mental health and sleep quality are associated with greater self-reported reward-related eating during pregnancy and postpartum: An observational cohort study. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 58. [Google Scholar] [CrossRef]
- Dashti, H.S.; Scheer, F.A.; Jacques, P.F.; Lamon-Fava, S.; Ordovas, J.M. Short sleep duration and dietary intake: Epidemiologic evidence, mechanisms, and health implications. Adv. Nutr. 2015, 6, 648–659. [Google Scholar] [CrossRef] [Green Version]
- Sejbuk, M.; Mironczuk-Chodakowska, I.; Witkowska, A.M. Sleep Quality: A Narrative Review on Nutrition, Stimulants, and Physical Activity as Important Factors. Nutrients 2022, 14, 1912. [Google Scholar] [CrossRef]
- Zhao, M.; Tuo, H.; Wang, S.; Zhao, L. The Effects of Dietary Nutrition on Sleep and Sleep Disorders. Mediat. Inflamm. 2020, 2020, 3142874. [Google Scholar] [CrossRef]
- Gangwisch, J.E.; Hale, L.; St-Onge, M.P.; Choi, L.; LeBlanc, E.S.; Malaspina, D.; Opler, M.G.; Shadyab, A.H.; Shikany, J.M.; Snetselaar, L.; et al. High glycemic index and glycemic load diets as risk factors for insomnia: Analyses from the Women’s Health Initiative. Am. J. Clin. Nutr. 2020, 111, 429–439. [Google Scholar] [CrossRef]
- St-Onge, M.P.; Mikic, A.; Pietrolungo, C.E. Effects of Diet on Sleep Quality. Adv. Nutr. 2016, 7, 938–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Callaghan, F.; Muurlink, O.; Reid, N. Effects of caffeine on sleep quality and daytime functioning. Risk Manag. Healthc. Policy 2018, 11, 263–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snel, J.; Lorist, M.M. Effects of caffeine on sleep and cognition. Prog. Brain Res. 2011, 190, 105–117. [Google Scholar] [PubMed]
- Noorwali, E.; Hardie, L.; Cade, J. Bridging the Reciprocal Gap between Sleep and Fruit and Vegetable Consumption: A Review of the Evidence, Potential Mechanisms, Implications, and Directions for Future Work. Nutrients 2019, 11, 1382. [Google Scholar] [CrossRef] [Green Version]
- Jansen, E.C.; Prather, A.; Leung, C.W. Associations between sleep duration and dietary quality: Results from a nationally-representative survey of US adults. Appetite 2020, 153, 104748. [Google Scholar] [CrossRef]
- Deng, M.G.; Nie, J.Q.; Li, Y.Y.; Yu, X.; Zhang, Z.J. Higher HEI-2015 Scores Are Associated with Lower Risk of Sleep Disorder: Results from a Nationally Representative Survey of United States Adults. Nutrients 2022, 14, 873. [Google Scholar] [CrossRef]
- Godos, J.; Grosso, G.; Castellano, S.; Galvano, F.; Caraci, F.; Ferri, R. Association between diet and sleep quality: A systematic review. Sleep Med. Rev. 2021, 57, 101430. [Google Scholar] [CrossRef]
- Scoditti, E.; Tumolo, M.R.; Garbarino, S. Mediterranean Diet on Sleep: A Health Alliance. Nutrients 2022, 14, 2998. [Google Scholar] [CrossRef]
- Kant, A.K.; Graubard, B.I. Association of self-reported sleep duration with eating behaviors of American adults: NHANES 2005-2010. Am. J. Clin. Nutr. 2014, 100, 938–947. [Google Scholar] [CrossRef] [Green Version]
- Boege, H.L.; Bhatti, M.Z.; St-Onge, M.P. Circadian rhythms and meal timing: Impact on energy balance and body weight. Curr. Opin. Biotechnol. 2021, 70, 1–6. [Google Scholar] [CrossRef]
- Neuhouser, M.L.; Tinker, L.F.; Thomson, C.; Caan, B.; Horn, L.V.; Snetselaar, L.; Parker, L.M.; Patterson, R.E.; Robinson-O’brien, R.; Beresford, S.A.A.; et al. Development of a glycemic index database for food frequency questionnaires used in epidemiologic studies. J. Nutr. 2006, 136, 1604–1609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manasse, S.M.; Lampe, E.W.; Gillikin, L.; Trainor, C.M.; Abber, S.R.; Fitzpatrick, B.; Sanchez, H.; Juarascio, A.S. An examination of daily sleep characteristics and subsequent eating disorder behavior among individuals with binge-spectrum eating disorders. Eat. Weight. Disord. 2022, 27, 3743–3749. [Google Scholar] [CrossRef]
- Da Luz, F.Q.; Sainsbury, A.; Salis, Z.; Hay, P.; Cordas, T.; Morin, C.M.; Paulos-Guarnieri, L.; Pascoareli, L.; El Rafihi-Ferreira, R. A systematic review with meta-analyses of the relationship between recurrent binge eating and sleep parameters. Int. J. Obes. (Lond.) 2023, 47, 145–164. [Google Scholar] [CrossRef] [PubMed]
- Plano, S.A.; Soneira, S.; Tortello, C.; Golombek, D.A. Is the binge-eating disorder a circadian disorder? Front. Nutr. 2022, 9, 964491. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.L.; Schnepp, J.; Tucker, R.M. Increased Hunger, Food Cravings, Food Reward, and Portion Size Selection after Sleep Curtailment in Women Without Obesity. Nutrients 2019, 11, 663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, W.; Finlayson, G.; Dando, R. Sleep, food cravings and taste. Appetite 2018, 125, 210–216. [Google Scholar] [CrossRef]
- Vidafar, P.; Cain, S.W.; Shechter, A. Relationship between Sleep and Hedonic Appetite in Shift Workers. Nutrients 2020, 12, 2835. [Google Scholar] [CrossRef]
- Kracht, C.L.; Chaput, J.P.; Martin, C.K.; Champagne, C.M.; Katzmarzyk, P.T.; Staiano, A.E. Associations of Sleep with Food Cravings, Diet, and Obesity in Adolescence. Nutrients 2019, 11, 2899. [Google Scholar] [CrossRef] [Green Version]
- Lai, P.P.; Say, Y.H. Associated Factors of Sleep Quality and Behavior among Students of Two Tertiary Institutions in Northern Malaysia. Med. J. Malays. 2013, 68, 195–203. [Google Scholar]
- Meule, A.; Roeser, K.; Randler, C.; Kubler, A. Skipping breakfast: Morningness-eveningness preference is differentially related to state and trait food cravings. Eat. Weight. Disord. 2012, 17, e304–e308. [Google Scholar] [PubMed]
- Yang, C.L.; Tucker, R.M. Snacking behavior differs between evening and morning chronotype individuals but no differences are observed in overall energy intake, diet quality, or food cravings Skipping breakfast: Morningness-eveningness preference is differentially related to state and trait food cravings Associated Factors of Sleep Quality and Behavior among Students of Two Tertiary Institutions in Northern Malaysia. Chronobiol. Int. 2022, 39, 616–625. [Google Scholar] [PubMed]


{kind=link}
| Author, Year, Country | Study Design, Melnyk Level of Evidence | Sample Size | Maternal Age at Baseline (Mean ± SD or % Distribution) | Time of Recruitment | Parity (Mean ± SD or % Multiparous) | BMI/Weight Status of Sample (Mean BMI ± SD or % Distribution) | Special Population (Yes/No) | Eligibility Criteria |
|---|---|---|---|---|---|---|---|---|
| Devoe et al., 1993, USA [51] | cohort, 3 | 20 | high consumers (n = 10): 23.8 + 5.6; low consumers (n = 10): 26.2 + 7.2 (p < 0.01) | 1st and 2nd trim | high consumers (n = 10): 0.7 ± 0.8; low consumers (n = 10): 1.5 ± 2.4 (p < 0.01) | not reported | no | singleton, normal glucose tolerance, no evident maternal or obstetric complications, no exposure to smoking or medications, normal fetal growth and amniotic fluid volumes |
| Diego et al., 2008, USA [52] | cohort, 3 | 128 | not reported | 2nd and 3rd trim | not reported | not reported | no | no pregnancy complications including preeclampsia and gestational diabetes, no HIV or any other infectious disease, no psychotropic medications or recreation drugs during pregnancy |
| Allison et al., 2012, USA [48] | cross-sectional, 4 | 120 | 25.2 + 5.1 | 2nd trim | 68.3% multiparous | 32.4 + 7.8 | yes (low-SES African American women with a pre-pregnancy BMI ≥ 25 kg/m2) | African American, ≥18 years of age, pre-pregnancy BMI of ≥25 kg/m2, singleton pregnancy, no preexisting diabetes mellitus, autoimmune disorder, or regular use of steroid treatment |
| Santos et al., 2012, Brazil [62] | cohort, 3 | 885 | 19.3% < 20, 70.8% 20–35, 9.8% > 35 | at delivery | 55.9% multiparous | not reported | no | singleton pregnancy |
| Ulman et al., 2012, Norway [65] | cohort, 3 | 72,435 | not reported | 2nd trim | 44% multiparous | 3.2% < 18.5, 66.0% 18.5 < BMI < 25, 21.5% 25 < BMI < 30, 9.3% > 30 | no | singleton pregnancy |
| Chang et al., 2015, USA [50] | cross-sectional, 4 | 213 | 1st trim (n = 75): 26.08 + 5.70; 2nd trim (n = 68): 26.07 + 5.38; 3rd trim (n = 68): 25.70 + 5.59 (non-sig.) | any trim | not reported | 1st trim (n = 75): 33.60 + 7.09; 2nd trim (n = 68): 31.60 + 4.71; 3rd trim (n = 68): 31.97 + 5.54 (non-sig.) | yes (low-SES with a pre-pregnancy BMI ≤ 25 kg/m2) | ≥18 years of age, speak and understand English, enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) |
| Duke et al., 2017, USA [55] | cross-sectional, 4 | 2951 | 30% 18–24, 53% 25–34, 17% 35–44 | any trim | not reported | not reported | no | pregnant Behavioral Risk Factor Surveillance System (BRFSS) participant, 18–44 years of age |
| van Lee et al., 2017, Singapore [66] | cross-sectional, 4 | 497 | good sleepers (n = 271): 30.8 + 4.5; poor sleepers (n = 226): 30.7 + 5.0 (non-sig.) | 1st trim | good sleepers (n = 271): 56.8% multiparous; poor sleepers (n = 226): 53.1% multiparous (non-sig.) | good sleepers (n = 271): 22.8 + 4.2; poor sleepers (n = 226): 22.5 + 4.5 (non-sig.) | no | part of larger cohort, intention to deliver in one of the two major study hospitals in Singapore, agree to donate placenta, cord, and cord blood at delivery, spouse had homogenous parental background of Chines, Malaysian, or Indian descent, no serious health conditions (e.g., type 1 diabetes, cancer, or psychological disorders), no probable major depression |
| Wolynczyk-Gmaj et al., 2017, Poland [68] | cross-sectional, 4 | 266 | 30.56 ± 4.95 | 3rd trim | not reported | with insomnia (n = 42): 28.8 (25.2, 31.6); without insomnia (n = 160): 26.4 (24.3, 28.9) (non-sig.) | no | in 3rd trimester |
| Gontijo et al., 2019, Brazil [58] | cross-sectional, 4 | 100 | 27.3 ± 5.7 | 1st trim | not reported | pre-pregnancy: 24.0 ± 4.4; current: 24.7 + 4.6 | no | healthy pregnant woman, singleton, ≥18 yrs of age, had prenatal visit no later than 12 wks gestation, no positive test for HIV, syphilis, toxoplasmosis, rubella, cytomegalovirus, or varicella |
| Phelan et al., 2018, USA [47] | RCT (behavioral lifestyle intervention with partial meal replacement to reduce GWG), 2 | 257 | 30.3 ± 5.42 | 1st and 2nd trim | 72.7% multiparous | 32.5 ± 5.3 | yes (overweight or obese) | gestational age between 9 and 16 wks at enrollment, BMI ≥ 25, English or Spanish speaking, age ≥ 18 yrs, singleton pregnancy, glycated hemoglobin < 6.5, no major health diseases (e.g., heart disease, cancer, renal disease, diabetes), no current substance abuse, no current treatment for a serious psychological disorder (e.g., schizophrenia, bipolar disorder), no contraindications to aerobic exercise |
| Bennett et al., 2019, Australia [49] | cross-sectional, 4 | 437 | 33.5 ± 1.4 | any trim | LC1 (n = 167): median 2 (IQR:1–3); LC2 (n = 173): median 2 (IQR:1–2); LC3 (n = 97): median 2 (IQR:2–3) (p < 0.01.) | LC1 (n = 167): median 23.1 (IQR:20.8–26.5); LC2 (n = 173): median 23.5 (IQR:20.8–26.4); LC3 (n = 97): median 24.1 (IQR:21.7–28.2) (non-sig.) | no | pregnant women part of larger cohort, sleep duration between 3 and 12 h, energy intake between 4500 and 20,000 kJ |
| Loy et al., 2020, Singapore [60] | cross-sectional, 4 | 673 | 30.9 ± 5.0 | 1st trim | not reported | 53.2% < 23, 46.8% ≥ 23 | no | attended antenatal care in 1st trimester, ≥18 yrs of age, homogenous parental ethnic groups (Chinese, Malay, or Indian), no chemotherapy or psychotropic drugs, no type 1 diabetes, singleton pregnancy, plausible total daily energy intake (500–3500 kcal) |
| Sugimori et al., 2019, Japan [63] | cohort, 3 | 72,624 | 31.5 at delivery | 1st and 2nd trim | 58.8% multiparous | 4.9% < 18.5, 79.6% 18.5-< 25, 15.4% ≥ 25 | no | resident in study area, expected to reside continually in Japan for foreseeable future, expected delivery between August 2011 and mid 2014, able to understand Japanese and complete self-administered questionnaires, live singleton birth |
| Du et al., 2021, China [53] | cross-sectional, 4 | 3692 | median: 29 (IQR: 27–32) | 1st and 2nd trim | 37% multiparous | median: 22 (IQR: 20–24) (pre-pregnancy) | no | 18–45 yrs of age, <14 wks gestation at recruitment, resident of study area with no plans to move, intention to undergo prenatal care and delivery at specific hospital, no cognitive mental disorders, no pre-pregnancy diabetes or hypertension, no cardiovascular, liver, kidney, or autoimmune disease, singleton pregnancy |
| Flanagan et al., 2021, USA [56] | cohort, 3 | 52 | 27.4 ± 0.7 | 1st and 2nd trim | 52% multiparous | 36.3 ± 0.7 | yes: obese | 18–40 yrs of age, BMI ≥ 30 kg/m2 at recruitment, no smoking, no alcohol or drug use, no hypertension, no diabetes, no use of medications that may affect body weight or energy intake |
| Flor-Alemany et al., 2020, Spain [57] | cross-sectional, 4 | 150 | 32.9 ± 4.6 | 1st trim | 40% multiparous | 24.9 ± 4.1 | no | singleton pregnancy, not engaged in >300 min/wk of physical activity, 14–18 weeks at first evaluation, no pregnancy risk factors (e.g., vaginal bleeding) |
| Pauley et al., 2020, USA [46] | RCT (behavioral lifestyle intervention with calorie and physical activity goals to reduce GWG), 2 | 24 | 30.6 ± 3.2 | 1st trim | 25% multiparous | 31.8 ± 3.2 | yes (overweight or obese) | 18–40 yrs of age, with overweight or obesity, singleton pregnancy, >8 wks gestation, physician’s consent, English speaking, residing in or near Central Pennsylvania, no diabetes, no sever allergies or dietary restrictions, no contradictions to prenatal physical activity |
| Teixeira et al., 2020, Brazil [64] | cross-sectional, 4 | 245 | median 25 (IQR 19–35) | any trim | 58.2% previous pregnancy | median 24.6 (IQR 19.2–3.4) | no | attending prenatal clinic in the public health service, ≥18 years of age, not a shift worker, no use of illegal substances, no HIV or disease with toxoplasmosis, syphilis, varicella, rubella, or cytomegalovirus |
| Zhan et al., 2020, China [69] | cross-sectional, 4 | 7615 | 28.6 ± 4.3 | 1st trim | 46.3% multiparous | 22.0 ± 3.6 (pre-pregnancy) | no | part of larger cohort, ≥16 yrs of age, 5–13 wks gestation at recruitment, able to complete questionnaires, permanent residents in study locations, no serious chronic diseases, no psychosis |
| Betts et al., 2021, USA [70] | cohort, 3 | 373 | 30.8 ± 4.6 | 1st trim | not reported | 26.6 ± 6.6 | no | plan to deliver at specific hospital and remain in area until one year postpartum, singleton pregnancy, BMI > 18.5 kg/m2, 18–45 yrs of age, read and write English, access to internet and email, no psychiatric or eating disorder, no pre-existing diabetes or other medical condition contraindicating study participation |
| Du et al., 2021, China [54] | cross-sectional, 4 | 4352 | median: 29 (IQR: 24–35) | 1st and 2nd trim | not specified (gravidity-58% yes) | 7.4% < 18.5, 69.7% 18.5–24.9, 18.5% 25–29.9, 4.4% > 30 | no | 18–45 yrs of age, <14 wks gestation at recruitment, resident of study area with no plans to move, intention to undergo prenatal care and delivery at specific hospital, no cognitive mental disorders, no pre-pregnancy diabetes or hypertension, no cardiovascular, liver, kidney, or autoimmune disease, singleton pregnancy |
| Gordon et al., 2021, USA [59] | cohort, 3 | 48 | 28.2 ± 4.9 | 3rd trim | 64.6% multiparous | not reported | yes (history of major depression or bipolar disorder) | history of MDD or MPD but not meeting criteria for a current mood episode at enrollment, no primary Axis I diagnosis other than MDD or BPD, no diagnosed sleep disorder, no report of high-risk pregnancy, no current alcohol or drug dependence, no use of hypnotic medications, not a night shift worker |
| Quach et al., 2021, Vietnam [61] | cross-sectional, 4 | 400 | median: 29 (IQR: 26–32) | any trim | 63.5% multiparous | median: 20.5 (IQR: 19.2–22.4) (pre-pregnancy); 23.2 (IQR: 21.1–25.5 (at baseline) | no | ≥18 yrs of age, no mental disorders preventing answering questions |
| Wang et al., 2021, USA [67] | cross-sectional, 4 | 108 | median: 30 (IQR: 26–33) | 2nd and 3rd trim | 62% multigravida | 55.6% normal weight, 25.0% overweight, 19.4% obese (pre-pregnancy) | no | >18 yrs of age, singleton pregnancy, <36 wks gestation at enrollment, pre-pregnancy body mass index of 18.5–40 kg/m2, planned to deliver at study hospital, comfortable reading and writing in English, able and willing to provide informed consent, no chronic medical conditions impacting body weight (e.g., pregestational diabetes, HIV/AIDS, chronic hepatitis, autoimmune disease), no current use of medication associated with. significant weight change or to treat opioid dependence, no previous weight loss surgery or current participation in a weight loss program |
| First Author, Year | Diet Var. | Measure/ Method | Variable Type/Specification | Time of Measurement (Weeks’ Gestation/Months Postpartum) | Sleep Var. | Measure(s) (Method) | Variable Type(s)/ Specification | Time of Measurement (Weeks’ Gestation/ Months Postpartum) | Statistical Analysis | Adjustment | Results |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Diego et al., 2008 [52] | caffeine consumption | questionnaire (single item) | continuous: number of drinks per day | baseline (20–28 wks gestation) | Effectiveness; disturbance; supplementary sleep | Verran and Snyder-Halperin (1988) Sleep Scale | continuous | unclear | Pearson’s correlation | no | caffeine use was correlated with having less sleep effectiveness (r = −0.25, p < 0.01), with non-sig. findings for sleep disturbance and supplementary sleep |
| Chang et al., 2015 [50] | fat intake | 24-item Rapid Food Screener (17 items for fat intake) | continuous (higher score indicates higher intake) | either 1st, 2nd, or 3rd trimester | duration; disturbance; quality; latency | Pittsburgh Sleep Quality Index (PSQI) (1 item for duration, 9 items for disturbance, 1 item for quality, 2 items for latency) | duration- categorical (>7 h, 6–7 h, 5–6 h, 3 < 5 h); disturbance- continuous (higher score indicates more sleep disturbance); quality- categorical (very good, good, bad, very bad); latency- continuous (higher score indicates longer sleep latency) | either 1st, 2nd, or 3rd trimester | Pearson’s correlation and path analysis | no | fat intake was correlated with nighttime sleep disturbance (p < 0.01), with non-sig. findings for sleep duration, quality, and latency; from path analysis, fat intake was associated with sleep disturbance in (standardized parameter estimate: 5.19, p < 0.01) |
| van Lee et al., 2017 [66] | energy intake; energy from discretionary foods | single 24 h recall face to face with 5 stage multiple pass method | continuous; sum of energy from caloric beverages (≥5 kcal; excluding plain water, diet soda, and unsweetened coffee, tea, and cow’s milk), local cakes, desserts, and snacks | at baseline (26–28 wks gestation) | quality; duration | Pittsburgh Sleep Quality Index (PSQI) (full index for quality, single item for duration) | quality—dichotomous (poor (defined as a global PSQI score > 5)/good); duration—dichotomous (short (defined as <6 h)/normal) | at baseline (26–28 wks gestation) | t-tests, chi-square tests, linear regression | yes 1 | non-sig. findings |
| Wolynczyk-Gmaj et al., 2017 [68] | coffee drinking | structured non- validated questions | not specified | at baseline (35.0 + 3.7 wks gestation) | insomnia; sleepiness | Athens Insomnia Scale; Epworth Sleepiness Scale | insomnia—continuous (higher score indicating higher severity), dichotomous (yes/no (using 8 point cutoff)); sleepiness—continuous (higher score indicating greater sleepiness) | at baseline (35.0 ± 3.7 wks gestation) | t-tests, chi-square tests, logistic regression | yes 2 | non-sig. findings |
| Phelan et al., 2018 [47] | behavioral lifestyle intervention with partial meal replacement | treatment group (randomly assigned) | dichotomous (meal replacement intervention/control) | at baseline and 35 wks gestation | duration | Actigraph (GT3X+) worn for 1 wk | continuous (h per day) | at baseline and 35 wks gestation | linear mixed effects models | yes 3 | non-sig. findings |
| Bennett et al., 2019 [49] | energy intake, carbohydrate, protein, total fat, saturated fat, monounsaturated fat, polyunsaturated fat, fiber, and sugar intake; protein to carbohydrate ratio; glycemic index; glycemic load | Dietary Questionnaire for Epidemiological Studies version 2 (DQESv2), which is a food frequency questionnaire | energy intake—continuous (kJ), carbohydrates, protein, total fat, saturated fat, monounsaturated fat, polyunsaturated fat, fiber, sugars—continuous (% energy); protein to carbohydrate ratio (kJ:kJ); glycemic index- continuous; glycemic load—continuous | at baseline (1st, 2nd, or 3rd trimester) | sleeping behavior pattern | questionnaire (combined duration (on workdays and non-workdays) and sleep disorder symptoms (restless sleep past wk, difficulty falling asleep past month, severe tiredness past 12 months, difficulty sleeping past 12 months)) | categorical: average sleep with no adverse sleep-related symptoms (LC1), average sleep with adverse sleep symptoms (LC2), short sleep with adverse sleep symptoms (LC3) (identified using latent class analysis) | at baseline (1st, 2nd, or 3rd trimester) | linear regression | yes 4 | in crude models, compared to LC1, LC2 was associated with energy intake (B: 0.063, p < 0.05), monounsaturated fat intake (B: −0.034, p < 0.05), and glycemic load (B: 0.082, p < 0.01), while LC3 was associated with glycemic load only (B: 0.073, p < 0.05), non-sig. findings for all other dietary outcomes; after adjustment (including additional adjustment for pre-pregnancy BMI), LC2 was associated with fat intake (B: −0.032, p < 0.05), monounsaturated fat intake (B: −0.050, p < 0.01), and carbohydrate intake (B: 0.033, p < 0.05); non-sig. findings for all other dietary outcomes as well as for LC3 and all dietary outcomes |
| Loy et al., 2020 [60] | energy intake | 24 h recall (5-stage multiple-pass interviewing technique) | continuous (kJ) | 26–28 wks gestation | duration (nighttime); bedtime | questionnaire (single item); not specified | duration- dichotomous (short sleep (defined as < 6 h per night)/sufficient sleep); bedtime—continuous | 26–28 wks gestation | t-tests | no | non-sig. findings |
| Du et al., 2020 [53] | caloric intake | 24 h dietary recall (2 non-consecutive days) | continuous (kcal/day) and dichotomous (< or > 2300) | at baseline (<14 wks gestation) | duration | questionnaire (single (PSQI) item) | categorical: short (<7 h/night), normal (7–9 h/night), long (>9 h/night) | at baseline (<14 wks gestation) | chi-square (Kruskal–Wallis and Fisher’s exact) | no | non-sig. findings |
| Flanagan et al., 2021 [56] | energy intake | calculated as the sum of total daily energy expenditure and changes in energy stores by the energy-balance method | continuous (kcals across pregnancy) | 13–16 and 35–37 wks gestation | change to habitual sleep (time spent in bed and total sleep time) | Actigraphy (GTX3+, wrist-worn for 6 consecutive nights) at two time points (change defined as change of one-half of the standard deviation of time spent in bed and total sleep time across 6 consecutive nights from early pregnancy) | categorical: increased, same, decreased | 13–16 and 35–37 wks gestation | linear mixed models | yes 5 | women who increased time in bed had lower energy intake across pregnancy compared to those who decreased (3078 ± 103 vs. 2538 ± 128, p < 0.01); non-sig. findings for total sleep time |
| Pauley et al., 2020 [46] | energy intake | estimated using a validated back-calculation method that uses weight (measured by participant with scale) and resting and active energy (physical activity—measured via activity monitor) each day | continuous (weekly average) | 8–36 wks gestation | duration (nighttime and daytime); awakenings | wrist worn activity monitor (Jawbone) | duration—continuous (weekly average min per day); awakenings—continuous (weekly average number per night) | 8–36 wks gestation | multi-level modeling | yes 6 | non-sig. findings |
| Du et al., 2021 [54] | caloric intake | 24 h dietary recall (2 non-consecutive days) | dichotomous (< or > 2300) | at baseline (<14 wks gestation) | quality | Pittsburgh Sleep Quality Index (PSQI) | dichotomous: poor (defined as >5 on the PSQI)/not | at baseline (<14 wks gestation) | chi-square tests and logistic regression | yes 7 | non-sig. findings |
| Wang et al., 2021 [67] | sugar-sweetened beverage consumption | 24 h recall (3 days (2 weekdays and 1 weekend day), via phone, interview with multiple pass technique) | continuous: average 8 oz servings per day | baseline (median: 23.9 wks (IQR: 18.9–30.6)) | duration; quality | Pittsburgh Sleep Quality Index (PSQI) | duration—dichotomous (short sleep (defined as <7 h per night)/sufficient sleep); quality—dichotomous (poor (defined as PSQI score >5)/not) | baseline (median: 23.9 wks (IQR: 18.9–30.6)) | logistic regression | yes 8 | each additional serving of a sugar-sweetened beverage was associated with higher odds of short sleep (adjusted OR:1.6, 1.1–2.5) and poor sleep quality (adjusted OR:2.1, 1.2–3.6) |
| First Author, Year | Diet Var. | Measure/ Method | Variable Type/ Specification | Time of Measurement (Weeks’ Gestation/ Months Postpartum) | Sleep Var. | Measure(s) (Method) | Variable Type(s)/Specification | Time of Measurement (Weeks’ Gestation/ Months Postpartum) | Statistical Analysis | Adjustment | Results |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Chang et al., 2015 [50] | fruit and vegetable intake | 24-item Rapid Food Screener (7 items for fruit and vegetable intake) | continuous (higher score indicates higher intake) | either 1st, 2nd, or 3rd trimester | duration; disturbance; quality; latency | Pittsburgh Sleep Quality Index (PSQI) (1 item for duration, 9 items for disturbance, 1 item for quality, 2 items for latency) | duration- categorical (>7 h, 6–7 h, 5–6 h, 3 < 5 h); disturbance- continuous (higher score indicates more sleep disturbance); quality—categorical (very good, good, bad, very bad); latency—continuous (higher score indicates longer sleep latency) | either 1st, 2nd, or 3rd trimester | Pearson’s correlation and path analysis | no | non-sig. correlations between fruit and vegetable intake with sleep duration, quality, latency, and disturbance; from path analysis, fruit and vegetable intake was associated with sleep latency (standardized parameter estimate: 1.47, p < 0.05) |
| Duke et al., 2017 [55] | fruit and vegetable consumption | questionnaire (4 items: consumption of fruit, dark green vegetables, orange-colored vegetables, and other vegetables during the past month) | continuous (consumption per day for each item and summed for total daily fruit and vegetable consumption) | not specified | duration | questionnaire (single item) | continuous (h per day) and categorical (inadequate sleep—<6 h, recommended sleep—7–9 h, over recommended sleep—>10 h) | not specified | analysis of variance, linear and logistic regression | yes 1 | in crude analyses, sleep recommendation categories were associated with other vegetable (p < 0.01), fruit (p < 0.01), and total fruit and vegetable (p < 0.05) consumption; in adjusted models, orange (B: −0.19 (−0.38, −0.01)) and green (B: −0.20 (−0.33, −0.08)) vegetable consumption were associated with sleep duration, non-sig. findings for total and other daily fruit and vegetable consumption; odds of meeting or exceeding sleep time recommendations increased slightly with each unit increase in total fruit and vegetable consumption (OR:1.05 (1.002,1.092) and for every unit increase in fruit consumption (OR:1.12 (1.038,1.208), non-sig. findings for green, orange, and other vegetable consumption |
| van Lee et al., 2017 [66] | diet quality; dietary pattern | single 24 h recall face to face with 5 stage multiple pass method | quality—continuous (using the Healthy Eating Index for pregnant women in Singapore (HEI-SGP)) and dichotomous (poor/good); pattern—categorical (vegetables-fruit-rice, seafood-noodles, pasta-cheese-meat); | at baseline (26–28 wks gestation) | quality; duration | Pittsburgh Sleep Quality Index (PSQI) (full index for quality, single item for duration) | quality—dichotomous (poor (defined as a global PSQI score >5)/good); duration—dichotomous (short (defined as <6 h)/normal) | at baseline (26–28 wks gestation) | t-tests, chi-square tests, linear regression | yes 2 | In adjusted analyses, good sleep quality compared to poor sleep quality was associated with better diet quality (mean HEI-SGP 54.6 vs. 52.0, p < 0.05), greater adherence to the vegetables-fruit-rice pattern (mean 0.03 vs. −0.15, p < 0.05), and lesser adherence to the seafood-noodle pattern (mean −0.14 vs. 0.03, p < 0.05, also significant after further adjustment for anxiety); non-sig. findings for pasta-cheese-meat pattern; non-sig. findings for short compared to normal sleep for diet quality, nor any dietary pattern |
| Gontijo et al., 209 [58] | quality (overall and individual components) | 3 24 h recalls on nonconsecutive days including one on the weekend (by interview) | continuous (average consumption across 3 days, evaluated using the Brazilian Health Eating Index-Revised (BHEI-R), overall and 12 components) | at baseline (<12 wks gestation) | chronotype | questionnaire (items asking about usual bedtime, usual wake time, sleep-onset latency, and usual sleep duration on weekdays and weekends during pregnancy) | categorical—morning type, intermediate type, evening type (using mid-sleep time on free days on weekends, with a further correction for sleep debt (calculated as the difference between average sleep duration on weekend and weekdays)) | at baseline (<12 wks gestation) | linear regression | yes 3 | chronotype was associated with total grains (B: 0.169, p < 0.01) and total fruit (B: −0.236, p < 0.05), non-sig. findings for all other Brazilian Healthy Eating Index Revised components |
| Du et al., 2021 [53] | type of diet | not specified | categorical (balanced, more meat, veggie-rich, vegan) | at baseline (<14 wks gestation) | duration | questionnaire (single (PSQI) item) | categorical: short (<7 h/night), normal (7–9 h/night), long (>9 h/night) | at baseline (<14 wks gestation) | chi-square (Kruskal–Wallis and Fisher’s exact) | no | type of diet was associated with sleep duration (p < 0.05), with short and long sleep durations more likely to be observed in vegans |
| Flanagan et al., 2021 [56] | diet quality | 2015 Healthy Eating Index (HEI) based on 6 days of food and plate waste photographs (SmartIntake phone App) | continuous | 13–16 and 35–37 wks gestation | change to habitual sleep (time spent in bed and total sleep time) | Actigraphy (GTX3+, wrist-worn for 6 consecutive nights) at two time points (change defined as change of one-half of the standard deviation of time spent in bed and total sleep time across 6 consecutive nights from early pregnancy) | categorical: increased, same, decreased | 13–16 and 35–37 wks gestation | linear mixed models | yes 4 | non-sig. findings |
| Flor-Alemany et al., 2020 [57] | Mediterranean diet adherence and components | Food Frequency Questionnaire (by interview) | Mediterranean adherence score- continuous and tertile (using Mediterranean Food Pattern, total score and 8 elements: olive oil, fiber, fruit, vegetables, fish, cereals, meat, alcohol) | 16 and 34 wks gestation | sleep quality | Pittsburgh Sleep Quality Index (PSQI) | continuous (lower values indicate better sleep quality) and dichotomous (good/bad using cutoff of 5) | 16 and 34 wks gestation | Spearman correlation, Kruskal–Wallis test | no | Mediterranean Food Pattern as a continuous variable was associated with better sleep quality at 16 (p < 0.05) and 34 wks (p < 0.01) gestation; similar findings for tertiles (p < 0.05 at 16 wks and p < 0.01 at 34 wks); fruit consumption was associated with better sleep quality at 16 wks gestation (p < 0.01); olive oil consumption and Mediterranean Diet adherence were associated with better sleep quality at 16 (p < 0.05) and 34 wks (p < 0.05) gestation; red meat and subproduct consumption was associated with worse sleep quality at 34 wks gestation (p < 0.05) |
| Zhan et al., 2020 [69] | dietary pattern (plant-based, vitamin-rich, high-fat, animal protein-rich, bean products) | Qualitative Food Frequency Questionnaire (Q-FFQ), with patterns derived via factor analysis | quartiles | at baseline (5–13 wks gestation) | quality | Pittsburgh Sleep Quality Index (PSQI) | dichotomous: sleep disturbance (defined as >5 on the PSQI)/normal | at baseline (5–13 wks gestation) | logistic regression | yes 5 | in the fully adjusted model, participants with the highest quartile in plant-based (OR: 0.80, 0.68–0.93) and vitamin-rich (OR: 0.76, 0.65–0.89) patterns had less sleep disturbance, while those in the highest quartile for high-fat pattern (OR:1.43, 1.22–1.67) has more sleep disturbance; non-sig. findings for animal protein-rich and bean products patterns in the fully adjusted model, but bean product patterns was associated with less sleep disturbance in the crude and partially adjusted models |
| Du et al., 2021 [54] | type of diet | not specified | categorical (balanced, more meat, more vegetables, vegetarian) | at baseline (<14 wks gestation) | quality | Pittsburgh Sleep Quality Index (PSQI) | dichotomous: poor (defined as >5 on the PSQI)/not | at baseline (<14 wks gestation) | chi-square tests and logistic regression | yes 6 | those with a vegetarian diet type (OR:2.18, 1.54–3.08) and those with a more vegetables diet type (OR:1.32, 1.14–1.52) were more likely to have poor sleep compared to those with a balanced diet |
| First Author, Year | Diet Var. | Measure/Method | Variable Type/ Specification | Time of Measurement (Weeks’ Gestation/ Months Postpartum) | Sleep Var. | Measure(s) (Method) | Variable Type(s)/ Specification | Time of Measurement (Weeks’ Gestation/ Months Postpartum) | Statistical Analysis | Adjustment | Results |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Allison et al., 2012 [48] | nighttime eating; disordered eating; cognitive restraint over eating; overeating at meals; snacking between meals; snacking after dinner; eating due to physical hunger; eating due to cravings; eating when anxious, bored, stressed, angry, depressed/upset, or alone | Night Eating Questionnaire (NEQ); Eating Disorders Examination-Questionnaire (EDE-Q) sections on objective overeating, binge eating, and purging; item 51 of the Eating Inventory to assess cognitive restraint over eating; Weight and Lifestyle Inventory | continuous: higher scores indicating more severe pathology | baseline (14–24 wks gestation) | duration; latency; quality | Pittsburgh Sleep Quality Index (PSQI) questions 1–6 | duration—continuous: h/night; latency—continuous: minutes; quality—categorical (very bad, fairly bad, fairly good, very good) | baseline (14–24 wks gestation) | Pearson’s correlation | no | sleep duration was correlated with night eating (r = −0.28, p < 0.01), with non-sig. findings for restraint, overeating episodes, and binge episodes; latency was correlated with night eating (r = 0.25, p < 0.05) and overeating episodes (r = 0.24, p < 0.05), with non-sig. findings for restraint and binge episodes; quality was correlated with night eating (r = −0.43, p < 0.01), overeating episodes (r = −0.25, p < 0.05), and binge episodes (r = −0.26, p < 0.01), with non-sig. findings for restraint |
| Ulman et al., 2012 [65] | binge eating symptoms | questionnaire (items addressing DSM-IV eating disorder criteria, questions addressing both eating an unusually large amount of food and feeling out of control) | categorical: binge eating disorder symptoms before and during pregnancy, symptoms before pregnancy that remitted during pregnancy, incident binge eating disorder symptoms during pregnancy, no reported symptoms before or during pregnancy | at baseline (~17.1 wks gestation) | sleep problems during first 18wks of pregnancy; sleep duration during the 3rd trimester; sleep disatisfaction 18 months after birth | questionnaire (single items) | sleeping problems- dichotomous (yes/no); duration- categorical (<6 h, 6–9 h, >10 h); sleep disatisfaction- yes/no | sleeping problems—median 17.1 wks gestation); duration—median 30.1 wks gestation; satisfaction—median 18.7 months postpartum | logistic regression | yes 1 | in both crude and adjusted models, all binge eating disorder symptom groups were more likely to report sleep problems during the first 18wks of pregnancy than the no symptoms group (adjusted ORs:1.26–1.42, p < 0.05); in crude models, all binge eating disorder symptom groups were more likely to sleep 10+ h or <6 h than the no symptoms groups, with the association persisting in the adjusted model for the incident binge eating disorder symptoms group (adjusted OR for 10+ h: 1.49, p < 0.01; adjusted OR for <6 h:1.58, p < 0.01); in both crude and adjusted models, all binge eating disorder symptom groups had higher odds of reporting sleep dissatisfaction at 18 months after birth than the no symptoms group (adjusted ORs:1.28–1.47, p < 0.01) |
| van Lee et al., 2017 [66] | longest night-time fasting interval; frequency of consumption occasions; nighttime eating | single 24 h recall face to face with 5 stage multiple pass method | continuous: longest fasting interval from 19:00 h to 06:59 h; number of eating occasion providing ≥50 kcal with 15 min time interval between occasions | at baseline (26–28 wks gestation) | quality; duration | Pittsburgh Sleep Quality Index (PSQI) (full index for quality, single item for duration) | quality- dichotomous (poor (defined as a global PSQI score >5)/good); duration—dichotomous (short (defined as <6 h)/normal) | at baseline (26–28 wks gestation) | t-tests, chi-square tests, linear regression | yes 2 | non-sig. findings |
| Wolynczyk-Gmaj et al., 2017 [68] | eating at night | structured non-validated questions | not specified | at baseline (35.0 + 3.7 wks gestation) | insomnia; sleepiness | Athens Insomnia Scale; Epworth Sleepiness Scale | insomnia- continuous (higher score indicating higher severity), dichotomous (yes/no (using 8 point cutoff)); sleepiness—continuous (higher score indicating greater sleepiness) | at baseline (35.0 ± 3.7 wks gestation) | t-tests, chi-square tests, logistic regression | yes 3 | women with insomnia during pregnancy were more likely to eat at night (chi-square = 18.15, df = 1, p < 0.01); from logistic regression, after adjustment, eating at night was associated with insomnia during pregnancy (OR: 2.935, 1.22, 7.07) |
| Gontijo et al., 2019 [58] | nightly fasting; eating duration; time of the first meal; time of the last meal; number of meals | 3 24 h recalls on nonconsecutive days including one on the weekend (by interview) | continuous | at baseline (<12 wks gestation) | chronotype | questionnaire (items asking about usual bedtime, usual wake time, sleep-onset latency, and usual sleep duration on weekdays and weekends during pregnancy) | categorical—morning type, intermediate type, evening type (using mid-sleep time on free days on weekends, with a further correction for sleep debt (calculated as the difference between average sleep duration on weekend and weekdays)) | at baseline (<12 wks gestation) | linear regression | yes 4 | non-sig. findings |
| Loy et al., 2020 [60] | nighttime eating; number of eating episodes | 24 h recall (5-stage multiple-pass interviewing technique) | nighttime eating—dichotomous: yes/no (defined as consuming >50% of total energy intake from 7 a.m.–7 p.m.); eating episodes—continuous (defined as events that provide >120 kJ (~50 kcal) with time intervals between eating episodes of >15 min) | 26–28 wks gestation | duration (nighttime); bedtime | questionnaire (single item); not specified | duration—dichotomous (short sleep (defined as <6 h per night)/sufficient sleep); bedtime—continuous | 26–28 wks gestation | t-tests | no | those with night-eating had later bedtimes (2307 ± 0133 vs. 2336 ± 0222, p < 0.05); non-sig. finding for sleep duration and daily eating episodes |
| Flanagan et al., 2021 [56] | disinhibition, dietary restraint, perceived hunger, food cravings, mindful eating | Eating Inventory (EI, for disinhibition, dietary restraint, and perceived hunger); Food Craving Inventory (FCI); Mindful Eating Questionnaire (MEQ) | continuous | 13–16 and 35–37 wks gestation | change to habitual sleep (time spent in bed and total sleep time) | Actigraphy (GTX3+, wrist-worn for 6 consecutive nights) at two time points (change defined as change of one-half of the standard deviation of time spent in bed and total sleep time across 6 consecutive nights from early pregnancy) | categorical: increased, same, decreased | 13–16 and 35–37 wks gestation | linear mixed models | yes 5 | women who increased time in bed reported an increase in food craving (23.8 ± 4.4% increase) compared to those who decreased (5.07 ± 6.4% increase, p = 0.05) across pregnancy; non-sig. findings for mindful eating, disinhibition, dietary restraint, and perceived hunger; non-sig. findings for total sleep time |
| Teixeira et al., 2020 [64] | food cravings | Food Craving Questionnaire Trait (FCQ-T) total score and 9 subscales (intentions and plans to consume food, anticipation of positive reinforcement that may result from eating, anticipation of relief from negative states and feeling as a result of eating, lack of control over eating, thoughts and preoccupations with food, craving as a physiological state, emotions that may be experienced before or during food craving, guilt from craving and/or from giving into them; Food Craving Questionnaire States (FCQ-S) total score and 5 subscales (intense desire to eat, anticipation of positive reinforcement that may result from eating, anticipation of relief from negative states and feelings as a result of eating, lack of control of eating, craving as a physiological state) | continuous (higher scores indicate more frequent and intense cravings) | 4–40 wks | chronotype | questionnaire (reported usual bed and wake times on weekdays and weekends) | continuous and categorical- morning type, intermediate type, non-evening type (morning and intermediate), evening type (calculated using mid-sleep time on free days with a further correction for calculated sleep debt) | 4–40 wks | generalized linear models | yes 6 | evening types had higher scores on 2 of 9 FCQ-T subscales: anticipation of relief from negative states and feelings as a result of eating compared to morning (B: 0.180, p < 0.5) and non-evening types (B: 0.150, p < 0.05) and anticipation of positive reinforcement that may result from eating compared to morning types (B: 0.132, p < 0.05); evening types had lower scores on 2 of 5 FCQ-S subscales: intense desire to eat compared to morning (B: −0.188, p < 0.05) and non-evening types (B: −0.184, p < 0.01) and anticipation of positive reinforcement that may result from eating than non-evening types (B: −0.152, p < 0.05); chronotype score was associated with anticipation of relief from negative states and feelings as a result of eating (p < 0.01), anticipation of positive reinforcement that may result from eating as a usual behavior (p < 0.05), and intense desire to eat as a sporadic behavior (p < 0.05) |
| Betts et al., 2021 [70] | addictive-like eating; hedonic hunger; cravings (frequency and intensity) | Yale Food Addiction Scale; Power of Food Scale; items developed by study investigators (assessed most craved food foods and frequency and intensity of overall and specific food cravings) | addictive-like eating—categorical (for cross-sectional analyses): did not meet threshold for any items, met threshold for 1 item, met threshold for 2 or more items, continuous (for change scores); hedonic hunger—continuous (calculated as the mean of three component scores); cravings—frequency and intensity calculated as highest response across foods | baseline (<12 wks gestation) and 6 months postpartum (cravings only assessed during pregnancy) | quality | Pittsburgh Sleep Quality Index (PSQI) | continuous | baseline (<12 wks gestation) and 6 months postpartum | Pearson’s correlation, linear and logistic regression | yes 7 | during pregnancy sleep quality was correlated with hedonic hunger (r = 0.15, p < 0.05), addictive-like eating (r = 0.20, p < 0.05), craving frequency (r = 0.23, p < 0.01) and craving strength (r = 0.24, p < 0.01); non-sig. findings for postpartum correlations; in regression analyses, worse sleep quality during pregnancy was associated with greater addictive-like eating (OR:1.09, 1.00–1.18), hedonic hunger (B: 0.03 (SE: 0.01)), and more frequent (B: 0.11 (SE: 0.03)) and intense (B: 0.13 (SE: 0.03)) cravings during pregnancy, while worse sleep quality postpartum was associated with greater addictive-like eating only (OR:1.13, 1.03–1.23); non-sig. findings for association between change in sleep quality with change in addictive-like eating or hedonic hunger |
| Quach et al., 2021 [61] | meal-to-bed time (daytime, nighttime, daytime and/or nighttime) | questionnaire (single item) | dichotomous: short (sleep within 2 h of finishing a meal on more than 2/3 of days during wk)/not short | baseline (median: 22.1 (IQR: 12.0–33.0)) | insomnia (reflux-related) | questionnaire (single item) | dichotomous: yes/no (during past 7 days) | baseline (median: 22.1 (IQR: 12.0–33.0)) | logistic regression | yes 8 | in both univariate (OR:4.60, 1.64–12.92) and multivariate analyses (OR:3.68, 1.14–11.85), meal-to-bed time was a risk factor for reflux-related insomnia |
| First Author, Year | Diet Var. | Measure/ Method | Variable Type/ Specification | Time of Measurement (Weeks’ Gestation/ Months Postpartum) | Sleep Var. | Measure(s) (Method) | Variable Type(s)/ Specification | Time of Measurement (Weeks’ Gestation/ Months Postpartum) | Statistical Analysis | Adjustment | Results |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Devoe et al., 1993 [51] | maternal caffeine consumption | questionnaire (multiple items) | dichotomous: high consumer (>500 mg/day) and low consumers (<200 mg/day) | baseline | infant fetal behavioral state | 2 h ultrasonographic observations of body, breathing, and eye movements | categorical: quiet sleep, active sleep, quiet wakefulness, arousal, no state | biweekly from 30–40 wks gestation | analysis of variance | no | infants in both groups spent similar mean time in a quiet sleep state, but infants of high consumers spend less mean time in active sleep |
| Diego et al., 2008 [52] | maternal caffeine consumption | questionnaire (single item) | continuous: number of drinks per day | baseline (20–28 wks gestation) | infant sleep-wake behavior; maternal sleep effectiveness and disturbance | 45 min live recording during inter-feeding interval; Verran and Snyder-Halperin (1988) Sleep Scale | categorical using Thoman’s Sleep State Criteria to assign state: quiet sleep, active sleep, REM, drowsy, awake alert, fussy, crying; continuous | within 24 h post-delivery; unclear | Pearson’s correlation | no | newborns of women who used more caffeine spent more time REM sleep (r = 0.24, p < 0.01, with non-sig. findings for quiet sleep, active sleep, drowsy, and awake alert states; caffeine use was correlated with having less sleep effectiveness (r = −0.25, p < 0.01), with non-sig. findings for sleep disturbance and supplementary sleep |
| Santos et al., 2012 [62] | maternal caffeine consumption | questionnaire (asked about instant and ground coffee and mate (a hot tea like beverage)) | dichotomous: heavy consumption (>300 mg/day) or not | at hospital after delivery | infant daytime sleep duration; night wakings | maternal report | daytime sleep duration- categorical (tertiles based on hours/day); night wakings—dichotomous (yes/no for >3 times per night in the previous 15 days) | 3 months of age | Poisson regression | yes 1 | non-sig. findings |
| Sugimori et al., 2019 [63] | maternal fermented food intake | Food Frequency Questionnaire (items about miso soup, yogurt, cheese, and Japanese fermented soybean intake) | quartiles based on estimated daily intake | 2nd and 3rd trimesters | infant duration | maternal report | dichotomous: <11 h or >11 h | 1 year of age | logistic regression | yes 2 | in crude and adjusted models, miso intake was associated with risk of sleeping <11 h for quartiles 2, 3, and 4, compared to 1 (adjusted ORs: 0.87–0.92, p < 0.01); yogurt intake was only associated with risk of sleeping <11 h in the crude analysis for quartile 3 compared to 1 (OR:0.91 (0.85, 0.98); cheese intake was associated with risk of sleeping <11 h in the crude analysis for quartiles 2 (OR:0.92 (0.86, 0.99) and 3 (OR:0.88 (.82, 0.95) compared to 1, but just for quartile 3 in the adjusted model (OR: 0.92 (0.85, 0.99); fermented bean intake was only associated with risk of sleeping <11 h in the crude analysis for quartile 3 compared to 1 (OR: 0.91 (0.85, 0.98) |
| Gordon et al., 2021 [59] | infant feeding status | daily diaries | categorical: exclusive breastfeeding, mixed (breastfeeding and formula), no breastfeeding, and dichotomous: any breastfeeding (exclusive or mixed)/no breastfeeding | 2 and 16 wks postpartum | maternal sleep disturbance/efficiency; chronotype | disturbance/efficiency- actigraphy (Micro Motionlogger Watch (AMI), wrist worn for one week) complimented by sleep diary) and Pittsburgh Sleep Quality Index (PSQI); chronotype-Horne-Ostberg Morningness-Eveningness Questionnaire (MEQ) | objective disturbance-efficiency- dichotomous: lower sleep efficiency/higher sleep efficiency (based on median split); subjective disturbance/efficiency- continuous; chronotype-continuous | 33 wks gestation | chi-square, t-tests | no | mothers with low sleep efficiency during pregnancy were less likely than high sleep efficiency mothers to initiate breastfeeding (45.8% vs. 16.7% no breastfeeding, p < 0.05); trend for similar results at 16 wks postpartum (chi-square (df = 2) = 4.61, p = 0.10); non-sig. findings for subjective sleep disturbance and chronotype with feeding status |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
von Ash, T.; Sanapo, L.; Bublitz, M.H.; Bourjeily, G.; Salisbury, A.; Petrillo, S.; Risica, P.M. A Systematic Review of Studies Examining Associations between Sleep Characteristics with Dietary Intake and Eating Behaviors during Pregnancy. Nutrients 2023, 15, 2166. https://doi.org/10.3390/nu15092166
von Ash T, Sanapo L, Bublitz MH, Bourjeily G, Salisbury A, Petrillo S, Risica PM. A Systematic Review of Studies Examining Associations between Sleep Characteristics with Dietary Intake and Eating Behaviors during Pregnancy. Nutrients. 2023; 15(9):2166. https://doi.org/10.3390/nu15092166
Chicago/Turabian Stylevon Ash, Tayla, Laura Sanapo, Margaret H. Bublitz, Ghada Bourjeily, Amy Salisbury, Sophia Petrillo, and Patricia Markham Risica. 2023. "A Systematic Review of Studies Examining Associations between Sleep Characteristics with Dietary Intake and Eating Behaviors during Pregnancy" Nutrients 15, no. 9: 2166. https://doi.org/10.3390/nu15092166