


Does a Plant-Based Diet Stand Out for Its Favorable Composition for Heart Health? Dietary Intake Data from a Randomized Controlled Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dietary Intervention
2.2. Dietary Intake and Monitoring
2.3. Anthropometric/Laboratory Data and Blood Pressure
2.4. Statistical Analysis
- Data are presented as means ± standard deviations and 95% confidence interval
- For laboratory data the Shapiro–Wilk test was used to determine normality.
- When normality was confirmed, participants characteristics and biochemistry was analyzed with a two samples t-test to assess differences between groups.
- Dietary nutrient intake was compared within the groups with the related-samples Wilcoxon signed rank test.
- Treatment effect and p-value between groups was determined using the Mann–Whitney-U test, comparing the difference of nutrient intake (Δ = intake at baseline vs. intake after 8 weeks). The difference is depicted as mean and 95% confidence interval (CI).
3. Results
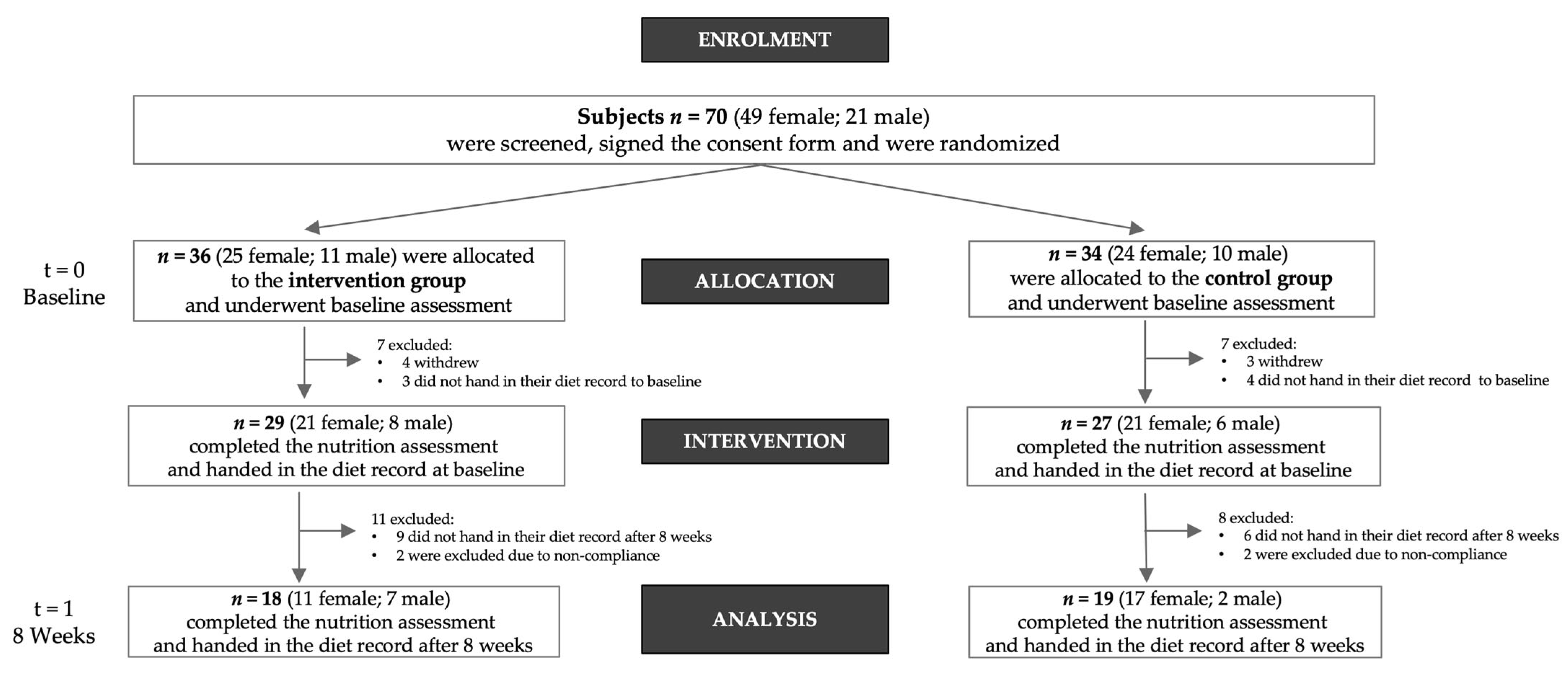
3.1. Randomization/Participants
3.2. Anthropometric/Laboratory Data and Blood Pressure
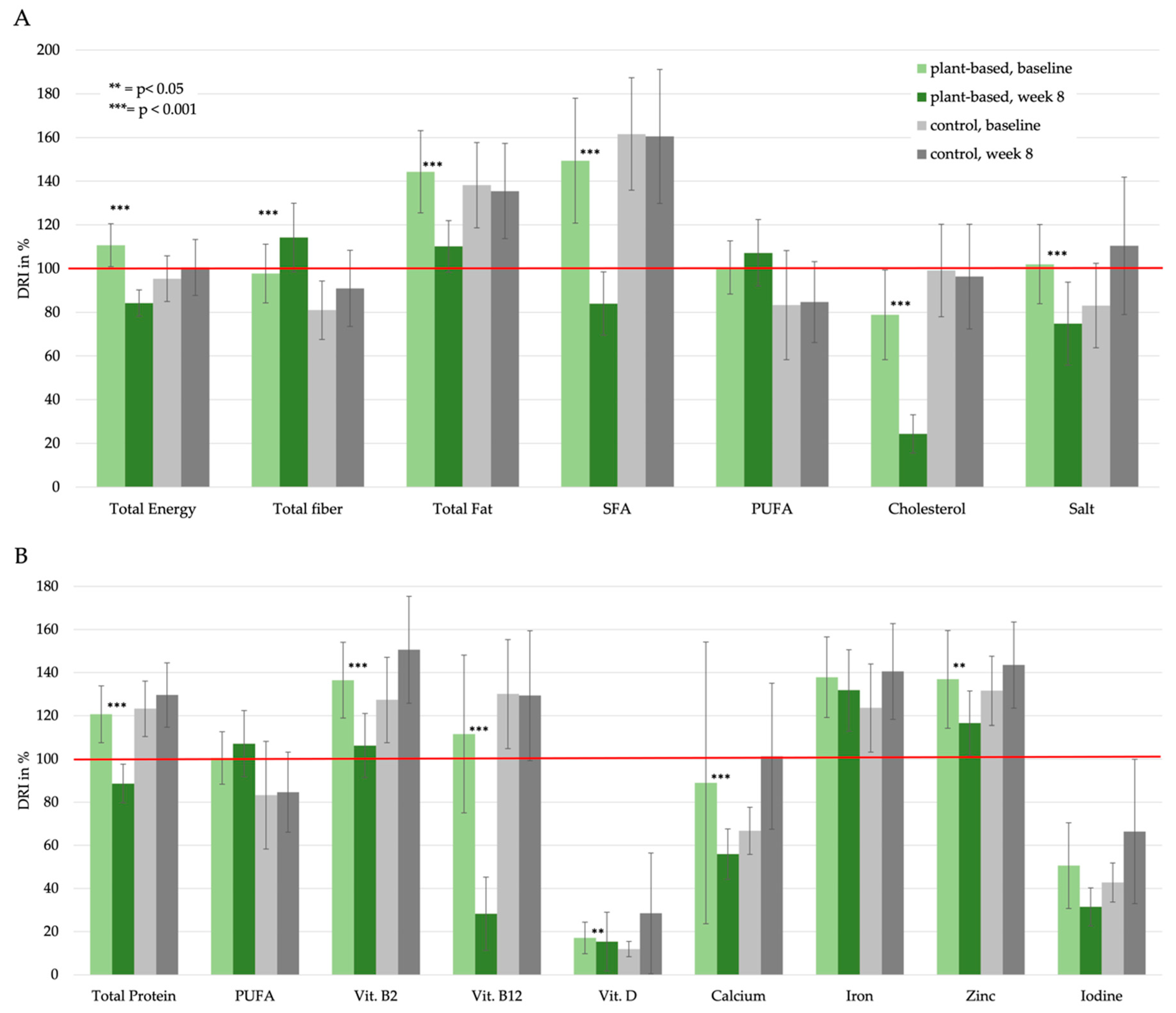
3.3. Results of the Dietary Intake Data
3.4. Macronutrient Intake
3.5. Micronutrient Intake/Vitamins
3.6. Micronutrient Intake/Minerals
4. Discussion
4.1. Potential Beneficial Nutrient Intake in a PBD
4.1.1. Energy Intake
4.1.2. Dietary Fiber Intake
4.1.3. Saturated Fatty Acids (SFA) and Cholesterol Intake
4.1.4. Salt Intake
4.2. Potential Critical Nutrients in a PBD
4.2.1. Protein Intake
4.2.2. Critical Micronutrients
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ALA | α-Linolenic Acid |
| ABPM | Ambulatory blood pressure monitoring |
| BMI | Body Mass Index |
| BLS | German Nutrient Data Base; german: Bundeslebensmittelschlüssel |
| CI | Confidence Interval |
| CG | Control Group |
| CVD | Cardiovascular Disease |
| D-A-CH | Association of nutritional societies of Germany (D), Austria (A) and Switzerland (CH) |
| DBP | 24 h Diastolic Blood Pressure |
| DGE | Society for Nutrition in Germany (Deutsche Gesellschaft für Ernährung) |
| DRI | Daily Recommended Intake |
| HbA1c | Hemoglobin A1c |
| HDL | High Density Lipoprotein |
| HOMA | Homeostasis Model Assessment |
| LDL | Low Density Lipoprotein |
| MUFA | Monounsaturated Fatty Acids |
| ÖGE | Society for Nutrition in Austria |
| PAL | Physical Activity Level |
| PBD | Plant-Based Diet |
| PBG | Plant-Based Group |
| PUFA | Polyunsaturated atty Acids |
| SBP | 24 h Systolic Blood Pressure |
| SD | Standard Deviation |
| SFA | Saturated Fatty Acids |
| SGE | Society for Nutrition in Switzerland |
References
- Jardine, M.A.; Kahleova, H.; Levin, S.M.; Ali, Z.; Trapp, C.B.; Barnard, N.D. Perspective: Plant-Based Eating Pattern for Type 2 Diabetes Prevention and Treatment: Efficacy, Mechanisms, and Practical Considerations. Adv. Nutr. 2021, 12, 2045–2055. [Google Scholar] [CrossRef] [PubMed]
- Qian, F.; Liu, G.; Hu, F.B.; Bhupathiraju, S.N.; Sun, Q. Association Between Plant-Based Dietary Patterns and Risk of Type 2 Diabetes: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2019, 179, 1335–1344. [Google Scholar] [CrossRef] [PubMed]
- Storz, M.A. The Role of Vegan Diets in Lipotoxicity-induced Beta-cell Dysfunction in Type-2-Diabetes: A Narrative Review. J. Popul. Ther. Clin. Pharmacol. 2020, 27 Pt 2, e22–e38. [Google Scholar] [CrossRef]
- Kaiser, J.; van Daalen, K.R.; Thayyil, A.; Cocco, M.; Caputo, D.; Oliver-Williams, C. A Systematic Review of the Association Between Vegan Diets and Risk of Cardiovascular Disease. J. Nutr. 2021, 151, 1539–1552. [Google Scholar] [CrossRef] [PubMed]
- Jabri, A.; Kumar, A.; Verghese, E.; Alameh, A.; Kumar, A.; Khan, M.S.; Khan, S.U.; Michos, E.D.; Kapadia, S.R.; Reed, G.W.; et al. Meta-analysis of effect of vegetarian diet on ischemic heart disease and all-cause mortality. Am. J. Prev. Cardiol. 2021, 7, 100182. [Google Scholar] [CrossRef] [PubMed]
- Tong, T.Y.N.; Appleby, P.N.; Bradbury, K.E.; Perez-Cornago, A.; Travis, R.C.; Clarke, R.; Key, T.J. Risks of ischaemic heart disease and stroke in meat eaters, fish eaters, and vegetarians over 18 years of follow-up: Results from the prospective EPIC-Oxford study. BMJ 2019, 366, 14897. [Google Scholar] [CrossRef] [Green Version]
- Ornish, D.; Brown, S.E.; Scherwitz, L.W.; Billings, J.H.; Armstrong, W.T.; Ports, T.A.; McLanahan, S.M.; Kirkeeide, R.L.; Brand, R.J.; Gould, K.L. Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial. Lancet 1990, 336, 129–133. [Google Scholar] [CrossRef]
- Storz, M.A.; Helle, P. Atrial fibrillation risk factor management with a plant-based diet: A review. J. Arrhythm. 2019, 35, 781–788. [Google Scholar] [CrossRef] [Green Version]
- Müller, A.; Zimmermann-Klemd, A.M.; Lederer, A.K.; Hannibal, L.; Kowarschik, S.; Huber, R.; Storz, M.A. A Vegan Diet Is Associated with a Significant Reduction in Dietary Acid Load: Post Hoc Analysis of a Randomized Controlled Trial in Healthy Individuals. Int. J. Environ. Res. Public Health 2021, 18, 9998. [Google Scholar] [CrossRef]
- Storz, M.A. What makes a plant-based diet? A review of current concepts and proposal for a standardized plant-based dietary intervention checklist. Eur. J. Clin. Nutr. 2022, 76, 789–800. [Google Scholar] [CrossRef]
- Tuso, P.J.; Ismail, M.H.; Ha, B.P.; Bartolotto, C. Nutritional update for physicians: Plant-based diets. Perm J. 2013, 17, 61–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boeing, H.; Bechthold, A.; Bub, A.; Ellinger, S.; Haller, D.; Kroke, A.; Leschik-Bonnet, E.; Müller, M.J.; Oberritter, H.; Schulze, M.; et al. Critical review: Vegetables and fruit in the prevention of chronic diseases. Eur. J. Nutr. 2012, 51, 637–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujioka, N.; Fritz, V.; Upadhyaya, P.; Kassie, F.; Hecht, S.S. Research on cruciferous vegetables, indole-3-carbinol, and cancer prevention: A tribute to Lee W. Wattenberg. Mol. Nutr. Food Res. 2016, 60, 1228–1238. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Beaubernard, L.; Lamothe, V.; Bennetau-Pelissero, C. New Evaluation of Isoflavone Exposure in the French Population. Nutrients 2019, 11, 2308. [Google Scholar] [CrossRef] [Green Version]
- Rajaram, S.; Jones, J.; Lee, G.J. Plant-Based Dietary Patterns, Plant Foods, and Age-Related Cognitive Decline. Adv. Nutr. 2019, 10 (Suppl. S4), S422–S436. [Google Scholar] [CrossRef] [Green Version]
- Verneau, F.; La Barbera, F.; Furno, M. The Role of Health Information in Consumers’ Willingness to Pay for Canned Crushed Tomatoes Enriched with Lycopene. Nutrients 2019, 11, 2173. [Google Scholar] [CrossRef] [Green Version]
- Viguiliouk, E.; Glenn, A.J.; Nishi, S.K.; Chiavaroli, L.; Seider, M.; Khan, T.; Bonaccio, M.; Iacoviello, L.; Mejia, S.B.; Jenkins, D.J.A.; et al. Associations between Dietary Pulses Alone or with Other Legumes and Cardiometabolic Disease Outcomes: An Umbrella Review and Updated Systematic Review and Meta-analysis of Prospective Cohort Studies. Adv. Nutr. 2019, 10 (Suppl. S4), S308–S319. [Google Scholar] [CrossRef] [Green Version]
- Veronese, N.; Solmi, M.; Caruso, M.G.; Giannelli, G.; Osella, A.R.; Evangelou, E.; Maggi, S.; Fontana, L.; Stubbs, B.; Tzoulaki, I. Dietary fiber and health outcomes: An umbrella review of systematic reviews and meta-analyses. Am. J. Clin. Nutr. 2018, 107, 436–444. [Google Scholar] [CrossRef] [Green Version]
- Mayhew, A.J.; de Souza, R.J.; Meyre, D.; Anand, S.S.; Mente, A. A systematic review and meta-analysis of nut consumption and incident risk of CVD and all-cause mortality. Br. J. Nutr. 2016, 115, 212–225. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Monounsaturated fatty acids, olive oil and health status: A systematic review and meta-analysis of cohort studies. Lipids Health Dis. 2014, 13, 154. [Google Scholar] [CrossRef]
- Zeraatkar, D.; Han, M.A.; Guyatt, G.H.; Vernooij, R.W.M.; El Dib, R.; Cheung, K.; Milio, K.; Zworth, M.; Bartoszko, J.J.; Valli, C.; et al. Red and Processed Meat Consumption and Risk for All-Cause Mortality and Cardiometabolic Outcomes: A Systematic Review and Meta-analysis of Cohort Studies. Ann. Intern. Med. 2019, 171, 703–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, L.T.; Sabaté, J. Beyond meatless, the health effects of vegan diets: Findings from the Adventist cohorts. Nutrients 2014, 6, 2131–2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.-L.; Wang, J.-H.; Chang, C.-C.; Chiu, T.H.T.; Lin, M.-N. Vegetarian Diets and Medical Expenditure in Taiwan—A Matched Cohort Study. Nutrients 2019, 11, 2688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcorta, A.; Porta, A.; Tárrega, A.; Alvarez, M.D.; Vaquero, M.P. Foods for Plant-Based Diets: Challenges and Innovations. Foods 2021, 10, 293. [Google Scholar] [CrossRef] [PubMed]
- Hemler, E.C.; Hu, F.B. Plant-Based Diets for Personal, Population, and Planetary Health. Adv. Nutr. 2019, 10 (Suppl. S4), S275–S283. [Google Scholar] [CrossRef] [Green Version]
- Richter, M.; Boeing, H.; Grünewald-Funk, D.; Heseker, H.; Kroke, A.; Leschik-Bonnet, E.; Oberritter, H.; Strohm, D.; Watzl, B. Vegan diet. Position of the German Nutrition Society (DGE). Ernahr. Umsch. 2016, 63, 92–102, Erratum in Ernahr. Umsch. 2016, 63, M262. [Google Scholar]
- Deutsche Gesellschaft für Ernährung (DGE); Österreichische Gesellschaft für Ernährung (ÖGE); Schweizerische Gesellschaft für Ernährung (SGE). D-A-CH-Referenzwerte für die Nährstoffzufuhr; Neuer Umschau Buchverlag: Bonn, Germany, 2018. [Google Scholar]
- Clarys, P.; Deliens, T.; Huybrechts, I.; Deriemaeker, P.; Vanaelst, B.; De Keyzer, W.; Hebbelinck, M.; Mullie, P. Comparison of nutritional quality of the vegan, vegetarian, semi-vegetarian, pesco-vegetarian and omnivorous diet. Nutrients 2014, 6, 1318–1332. [Google Scholar] [CrossRef]
- Lemale, J.; Mas, E.; Jung, C.; Bellaiche, M.; Tounian, P. Vegan diet in children and adolescents. Recommendations from the French-speaking Pediatric Hepatology, Gastroenterology and Nutrition Group (GFHGNP). Arch. Pediatr. 2019, 26, 442–450. [Google Scholar] [CrossRef]
- Vergeer, L.; Vanderlee, L.; White, C.M.; Rynard, V.L.; Hammond, D. Vegetarianism and other eating practices among youth and young adults in major Canadian cities. Public Health Nutr. 2020, 23, 609–619. [Google Scholar] [CrossRef]
- Lally, P.; van Jaarsveld, C.H.M.; Potts, H.W.W.; Wardle, J. How are habits formed: Modelling habit formation in the real world. Eur. J. Soc. Psychol. 2010, 40, 998–1009. [Google Scholar] [CrossRef] [Green Version]
- Alexy, U.; Fischer, M.; Weder, S.; Längler, A.; Michalsen, A.; Sputtek, A.; Keller, M. Nutrient Intake and Status of German Children and Adolescents Consuming Vegetarian, Vegan or Omnivore Diets: Results of the VeChi Youth Study. Nutrients 2021, 13, 1707. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.S.; Ning, H.; Wilkins, J.T.; Allen, N.; Carnethon, M.; Berry, J.D.; Sweis, R.N.; Lloyd-Jones, D.M. Association of Body Mass Index With Lifetime Risk of Cardiovascular Disease and Compression of Morbidity. JAMA Cardiol. 2018, 3, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Rolls, B.J. The relationship between dietary energy density and energy intake. Physiol. Behav. 2009, 97, 609–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Muniz, F.J. Dietary fibre and cardiovascular health. Nutr. Hosp. 2012, 27, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J. Fiber and prebiotics: Mechanisms and health benefits. Nutrients 2013, 5, 1417–1435. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Lietz, G.; Bal, W.; Watson, A.; Morfey, B.; Seal, C. Effects of Quinoa (Chenopodium quinoa Willd.) Consumption on Markers of CVD Risk. Nutrients 2018, 10, 777. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Harding, S.V.; Thandapilly, S.J.; Tosh, S.M.; Jones, P.J.H.; Ames, N.P. Barley β-glucan reduces blood cholesterol levels via interrupting bile acid metabolism. Br. J. Nutr. 2017, 118, 822–829. [Google Scholar] [CrossRef] [Green Version]
- Gulati, S.; Misra, A.; Pandey, R.M. Effects of 3 g of soluble fiber from oats on lipid levels of Asian Indians—A randomized controlled, parallel arm study. Lipids Health Dis. 2017, 16, 71. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, D.J.; Kendall, C.W.; Nguyen, T.H.; Marchie, A.; Faulkner, D.A.; Ireland, C.; Josse, A.R.; Vidgen, E.; Trautwein, E.A.; Lapsley, K.G.; et al. Effect of plant sterols in combination with other cholesterol-lowering foods. Metabolism 2008, 57, 130–139. [Google Scholar] [CrossRef]
- Bradbury, K.E.; Crowe, F.L.; Appleby, P.N.; Schmidt, J.A.; Travis, R.C.; Key, T.J. Serum concentrations of cholesterol, apolipoprotein A-I and apolipoprotein B in a total of 1694 meat-eaters, fish-eaters, vegetarians and vegans. Eur. J. Clin. Nutr. 2014, 68, 178–183. [Google Scholar] [CrossRef] [Green Version]
- Kahleova, H.; Hlozkova, A.; Fleeman, R.; Fletcher, K.; Holubkov, R.; Barnard, N.D. Fat Quantity and Quality, as Part of a Low-Fat, Vegan Diet, Are Associated with Changes in Body Composition, Insulin Resistance, and Insulin Secretion. A 16-Week Randomized Controlled Trial. Nutrients 2019, 11, 615. [Google Scholar] [CrossRef] [PubMed]
- Desmond, M.A.; Sobiecki, J.; Fewtrell, M.; Wells, J.C.K. Plant-based diets for children as a means of improving adult cardiometabolic health. Nutr. Rev. 2018, 76, 260–273. [Google Scholar] [CrossRef] [PubMed]
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 1970–1980. [Google Scholar] [CrossRef] [PubMed]
- Satija, A.; Bhupathiraju, S.N.; Spiegelman, D.; Chiuve, S.E.; Manson, J.E.; Willett, W.; Rexrode, K.M.; Rimm, E.B.; Hu, F.B. Healthful and Unhealthful Plant-Based Diets and the Risk of Coronary Heart Disease in U.S. Adults. J. Am. Coll. Cardiol. 2017, 70, 411–422. [Google Scholar] [CrossRef]
- Russo, G.L. Dietary n−6 and n−3 polyunsaturated fatty acids: From biochemistry to clinical implications in cardiovascular prevention. Biochem. Pharmacol. 2009, 77, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Thumann, T.A.; Pferschy-Wenzig, E.-M.; Moissl-Eichinger, C.; Bauer, R. The role of gut microbiota for the activity of medicinal plants traditionally used in the European Union for gastrointestinal disorders. J. Ethnopharmacol. 2019, 245, 112153. [Google Scholar] [CrossRef]
- NCEP. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Hegsted, D.M. Serum-cholesterol response to dietary cholesterol: A re-evaluation. Am. J. Clin. Nutr. 1986, 44, 299–305. [Google Scholar] [CrossRef]
- Weggemans, R.M.; Zock, P.L.; Katan, M.B. Dietary cholesterol from eggs increases the ratio of total cholesterol to high-density lipoprotein cholesterol in humans: A meta-analysis. Am. J. Clin. Nutr. 2001, 73, 885–891. [Google Scholar] [CrossRef] [Green Version]
- Kotchen, T.A. Contributions of sodium and chloride to NaCl-induced hypertension. Hypertension 2005, 45, 849–850. [Google Scholar] [CrossRef] [Green Version]
- He, F.J.; Li, J.; MacGregor, G.A. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ Br. Med. J. 2013, 346, f1325. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Trieu, K.; Yoshimura, S.; Neal, B.; Woodward, M.; Campbell, N.R.C.; Li, Q.; Lackland, D.T.; Leung, A.A.; Anderson, C.A.M.; et al. Effect of dose and duration of reduction in dietary sodium on blood pressure levels: Systematic review and meta-analysis of randomised trials. BMJ 2020, 368, m315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, J.W.; Rucker, R.B. Pantothenic acid. In Present Knowledge in Nutrition, 10th ed.; Wiley-Blackwell: New York, NY, USA, 2012; pp. 375–390. [Google Scholar]
- Zmijewski, M.A. Vitamin D and Human Health. Int. J. Mol. Sci. 2019, 20, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurberg, P. Iodine. In Modern Nutrition in Health and Disease, 11th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014; pp. 217–224. [Google Scholar]
- Weaver, C.M. Calcium. In Present Knowledge in Nutrition, 10th ed.; Sons, J.W., Ed.; John Wiley & Sons: Hoboken, NJ, USA, 2012; pp. 434–446. [Google Scholar]
- Maifeld, A.; Bartolomaeus, H.; Löber, U.; Avery, E.G.; Steckhan, N.; Markó, L.; Wilck, N.; Hamad, I.; Šušnjar, U.; Mähler, A.; et al. Fasting alters the gut microbiome reducing blood pressure and body weight in metabolic syndrome patients. Nat. Commun. 2021, 12, 1970. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
Men and women aged 25 to 75 and diagnosed with:
|
|
| Plant-Based Group (n = 18) | Control Group (n = 19) | ||||||
|---|---|---|---|---|---|---|---|
| Baseline | Week 8 | Δ [95% CI] | Baseline | Week 8 | Δ [95% CI] | p-Value * | |
| Anthropometrics | |||||||
| Weight [kg] | 93.0 ± 16.6 | 89.5 ± 15.5 | −3.5 [−5.3–−1.7] | 80.7 ± 11.9 | 80.4 ± 12.1 | −0.3 [−1.1–0.5] | 0.002 |
| Body mass index [kg/m2] | 31.7 ± 4.6 | 30.5 ± 4.1 | −1.2 [−1.8–−0.6] | 29.5 ± 4.5 | 29.4 ± 4.8 | −0.1 [−0.4–0.3] | 0.002 |
| Waist circumference [cm] | 109.9 ± 11.1 | 106.7 ± 9.4 | −3.2 [−5.1–−1.3] | 101.2 ± 7.0 | 101.5 ± 7.1 | 0.2 [−0.9–1.4] | 0.004 |
| Laboratory data | |||||||
| Fasting blood glucose [mg/dl] | 99.7 ± 15.5 | 93.9 ± 12.9 | −5.8 [−9.1–−2.6] | 93.1 ± 16.2 | 92.5 ± 15.1 | −0.6 [−3.9–2.8] | 0.042 |
| HbA1c [mmol/mol] | 40.1 ± 6.5 | 38.4 ± 5.4 | −1.7 [−2.8–−0.6] | 36.5 ± 3.1 | 36.8 ± 3.8 | 0.3 [−0.5–1.2] | 0.009 |
| HOMA Index | 3.7 ± 2.7 | 2.9 ± 1.8 | −0.8 [−1.4–−0.1] | 2.6 ± 1.9 | 2.4 ± 1.7 | −0.2 [−0.6–0.3] | 0.170 |
| Triglycerides [mg/dl] | 112.1 ± 36.5 | 126.6 ± 48.5 | 14.6 [−2.5–31.6] | 120.1 ± 58.1 | 135.6 ± 76.7 | 15.6 [−1.0–32.2] | 0.936 |
| Cholesterol [mg/dl] | 214.1 ± 26.8 | 198.7 ± 28.1 | −15.4 [−27.4–−3.5] | 227.4 ± 46.1 | 223.9 ± 53.7 | −3.5 [−15.5–8.4] | 0.191 |
| LDL [mg/dl] | 137.3 ± 26.0 | 125.0 ± 27.6 | −12.3 [−23.9–−0.7] | 147.4 ± 44.8 | 147.0 ± 52.7 | −0.4 [−11.6–10.8] | 0.171 |
| HDL [mg/dl] | 63.6 ± 15.9 | 56.3 ± 13.4 | −7.4 [−10.1–−4.7] | 66.3 ± 21.1 | 62.4 ± 20.2 | −3.9 [−6.9–−0.9] | 0.117 |
| Ambulatory blood pressure monitoring | |||||||
| ABPM SBP [mm Hg] | 135.9 ± 11.0 | 130.3 ± 14.7 | −5.6 [−10.6–−0.5] | 130.6 ± 13.3 | 131.9 ± 13.1 | 1.3 [−3.5–6.1] | 0.088 |
| ABPM DBP [mm Hg] | 83.3 ± 8.8 | 80.1 ± 9.3 | −3.2 [−6.2–−0.3] | 76.9 ± 5.8 | 78.0 ± 6.8 | 1.1 [−1.8–3.9] | 0.069 |
| Plant-Based Group (n = 18) | Control Group (n = 19) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Week 8 | Baseline | Week 8 | p-Value b | |||||
| Intake a | % of DRI c | Intake | % of DRI | Intake | % of DRI | Intake | % of DRI | ||
| Macronutrients | |||||||||
| Energy [kcal] | 2392.2 ± 382.6 | 111 [101;121] | 1798.1 ± 315.1 | 84 [78;90] | 1955.4 ± 452.0 | 95 [85;106] | 1955.1 ± 477.1 | 101 [88;113] | <0.001 |
| Total carbohydrates [g] | 217.2 ± 58.9 | 74 [65;82] | 189.7 ± 41.6 | 69 [62;75] | 178.8 ± 52.7 | 64 [54;73] | 187.9 ± 47.2 | 74 [60;89] | 0.078 |
| Total dietary fiber [g] | 24.2 ± 8.7 | 98 [84;111] | 31.3 ± 8.6 | 114 [98;130] | 24.9 ± 8.3 | 81 [68;94] | 24.5 ± 8.1 | 91 [74;108] | 0.002 |
| Total Protein [g] | 90.3 ± 15.0 | 121 [108;134] | 56.2 ± 10.1 | 89 [80;98] | 74.4 ± 15.5 | 123 [110;136] | 75.8 ± 18.4 | 123 [110;136] | <0.001 |
| Total Fat [g] | 112.6 ± 22.3 | 144 ± 41 [125;163] | 78.1 ± 18.3 | 110 [98;122] | 91.3 ± 29.5 | 138 [119;158] | 87.5 ± 30.8 | 135 [114;157] | 0.005 |
| SFA [g] | 45.3 ± 12.7 | 149 [121;178] | 21.3 ± 9.0 | 84 [70;98] | 35.6 ± 12.8 | 162 [136;187] | 34.7 ± 14.7 | 161 [130;191] | <0.001 |
| MUFA [g] | 41.1 ± 9.1 | 157 [134;180] | 28.3 ± 8.2 | 123 [105;141] | 31.2 ± 10.5 | 143 [122;164] | 29.5 ± 10.6 | 136 [113;158] | 0.001 |
| PUFA [g] | 18.3 ± 5.3 | 101 [88;113] | 23.7 ± 8.4 | 107 [92;122] | 18.4 ± 12.1 | 83 [58;108] | 17.6 ± 8.4 | 85 [66;103] | 0.129 |
| LA [g] | 14.4 ± 5.2 | 290 [246;333] | 19.1 ± 7.4 | 300 [244;357] | 14.0 ± 9.4 | 253 [177;330] | 14.1 ± 7.6 | 250 [181;318] | 0.191 |
| ALA [g] | 2.5 ± 1.8 | 351 [280;421] | 4.1 ± 3.3 | 375 [231;519] | 3.2 ± 3.8 | 293 [133;453] | 2.3 ± 2.1 | 224 [139;309] | 0.013 |
| Cholesterol [mg] | 383.7 ± 133.1 | 79 [58;99] | 76.7 ± 58.8 | 24 [16;33] | 301.9 ± 142.6 | 99 [78;120] | 294.7 ± 163.8 | 96 [72;120] | <0.001 |
| Salt [g] | 6.5 ± 2.0 | 102 [84;120] | 3.7 ± 2.1 | 75 [56;94] | 4.3 ± 2.0 | 83 [64;102] | 5.0 ± 1.8 | 110 [79;142] | <0.001 |
| Vitamins | |||||||||
| Retinol equivalent [µg] | 1660.6 ± 865.3 | 169 [119;219] | 1230.4 ± 771.3 | 140 [95;184] | 1575.9 ± 8401 | 173 [141;206] | 1578.3 ± 632.6 | 193 [155;230] | 0.202 |
| Vitamine B1 [mg] | 1.4 ± 0.3 | 133 [118;148] | 1.4 ± 0.4 | 128 [110;145] | 1.2 ± 0.3 | 111 [98;125] | 1.3 ± 0.4 | 130 [110;150] | 0.136 |
| Vitamine B2 [mg] | 1.7 ± 0.4 | 136 [119;154] | 1.1 ± 0.3 | 106 [92;121] | 1.4 ± 0.4 | 127 [108;147] | 1.5 ± 0.5 | 151 [126;175] | 0.242 |
| Vitamine B3, Niacin equivalent [mg] | 38.3 ± 8.1 | 268 [229;307] | 24.7 ± 5.5 | 195 [166;224] | 31.1 ± 7.8 | 269 [235;304] | 30.1 ± 8.2 | 258 [224;292] | <0.001 |
| Vitamine B5 [mg] | 5.0 ± 1.2 | 80 [71;90] | 4.0 ± 1.6 | 69 [56;81] | 4.5 ± 1.2 | 71 [62;81] | 4.7 ± 1.7 | 85 [67;103] | 0.068 |
| Vitamine B6 [mg] | 1.8 ± 0.4 | 132 [117;146] | 1.5 ± 0.4 | 117 [102;132] | 1.6 ± 0.3 | 127 [113;141] | 1.6 ± 0.4 | 131 [116;145] | 0.005 |
| Vitamine B7, Biotin [µg] | 52.3 ± 16.3 | 118 [102;135] | 48.5 ± 14.8 | 109 [93;125] | 46.3 ± 11.7 | 97 [84;110] | 49.5 ± 15.2 | 116 [98;134] | 0.288 |
| Vitamine B9, Folate [µg] | 350.9 ± 109.1 | 115 [98;131] | 310.9 ± 70.6 | 109 [99;118] | 291.6 ± 94.3 | 94 [79;109] | 292.1 ± 75.9 | 103 [88;118] | 0.236 |
| Vitamine B12 [µg] | 5.7 ± 2.4 | 112 [75;148] | 1.0 ± 1.2 | 28 [11;45] | 3.9 ± 1.7 | 130 [105;155] | 4.0 ± 2.0 | 129 [99;159] | <0.001 |
| Vitamine C [mg] | 125.5 ± 54.3 | 144 [120;167] | 144.1 ± 84.6 | 160 [121;200] | 157.1 ± 80.1 | 175 [135;214] | 126.4 ± 47.3 | 127 [104;150] | 0.121 |
| Vitamine D [µg] | 3.8 ± 3.2 | 17 [10;24] | 1.7 ± 1.5 | 15 [2;29] | 3.9 ± 6.3 | 12 [8;15] | 2.7 ± 1.5 | 28 [−1;58] | 0.136 |
| Vitamine E [mg] | 16.8 ± 6.0 | 155 [134;177] | 19.8 ± 5.4 | 163 [141;184] | 16.1 ± 7.7 | 142 [111;172] | 18.0 ± 8.0 | 152 [119;185] | 0.574 |
| Vitamine K [µg] | 195.6 ± 193.3 | 254 [143;366] | 152.2 ± 131.3 | 214 [117;310] | 161.4 ± 108.5 | 246 [172;320] | 190.2 ± 152.7 | 269 [162;376] | 0.316 |
| Minerals | |||||||||
| Sodium [mg] | 2753.5 ± 822.2 | 109 [90;128] | 1620.7 ± 870.7 | 81 [60;101] | 1861.1 ± 863.5 | 90 [69;110] | 2147.6 ± 820.4 | 119 [88;149] | <0.001 |
| Chloride [mg] | 4170.7 ± 1222.8 | 113 [94;132] | 2563.5 ± 1298.8 | 86 [66;106] | 2814.6 ± 1189.6 | 91 [72;110] | 3291.0 ± 1150.5 | 117 [93;141] | <0.001 |
| Potassium [mg] | 3402.8 ± 651.3 | 160 [145;175] | 2970.9 ± 655.5 | 144 [126;162] | 3001.4 ± 627.3 | 144 [126;161] | 3046.4 ± 581.7 | 149 [134;164] | 0.021 |
| Magnesium [mg] | 498.1 ± 401.7 | 145 [83;208] | 428.3 ± 107.4 | 131 [111;152] | 348.4 ± 117.6 | 110 [91;129] | 362.4 ± 99.6 | 127 [108;145] | 0.715 |
| Zinc [mg] | 11.9 ± 2.6 | 137 [114;160] | 8.9 ± 2.2 | 117 [102;131] | 9.6 ± 2.5 | 132 [116;148] | 10.6 ± 3.6 | 143 [123;164] | 0.001 |
| Copper [µg] | 2260.1 ± 720.2 | 181 [154;207] | 2372.7 ± 603.8 | 180 [152;208] | 1896.4 ± 658.7 | 146 [119;173] | 1931.5 ± 613.2 | 163 [136;189] | 0.738 |
| Phosphorus [mg] | 1453.4 ± 258.4 | 187 [170;204] | 1127.2 ± 303.5 | 156 [133;179] | 1210.0 ± 246.9 | 165 [146;185] | 1289.6 ± 331.4 | 187 [166;209] | <0.001 |
| Fluoride [µg] | 2004.3 ± 4179.9 | 45 [−17;108] | 953.0 ± 501.6 | 31 [22;41] | 789.0 ± 377.2 | 24 [18;30] | 872.4 ± 435.6 | 58 [−1;116] | 0.136 |
| Calcium [µg] | 1174.5 ± 1412.9 | 89 [24;154] | 551.4 ± 188.7 | 56 [44;68] | 708.4 ± 203.7 | 67 [56;78] | 849.8 ± 260.5 | 101 [68;135] | <0.001 |
| Iron [mg] | 14.3 ± 3.8 | 138 [119;157] | 13.8 ± 3.7 | 132 [113;151] | 13.5 ± 4.0 | 124 [103;144] | 13.6 ± 4.1 | 141 [118;163] | 0.727 |
| Iodine [µg] | 121.9 ± 77.2 | 51 [31;71] | 54.7 ± 25.5 | 32 [23;40] | 91.9 ± 55.1 | 43 [34;52] | 92.3 ± 28.0 | 66 [33;100] | <0.001 |
| Manganese [µg] | 5402.7 ± 2411.8 | 194 [162;226] | 8038.3 ± 3563.5 | 243 [200;287] | 5630.7 ± 2979.4 | 155 [114;196] | 6324.4 ± 3642.3 | 218 [142;293] | 0.019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dressler, J.; Storz, M.A.; Müller, C.; Kandil, F.I.; Kessler, C.S.; Michalsen, A.; Jeitler, M. Does a Plant-Based Diet Stand Out for Its Favorable Composition for Heart Health? Dietary Intake Data from a Randomized Controlled Trial. Nutrients 2022, 14, 4597. https://doi.org/10.3390/nu14214597
Dressler J, Storz MA, Müller C, Kandil FI, Kessler CS, Michalsen A, Jeitler M. Does a Plant-Based Diet Stand Out for Its Favorable Composition for Heart Health? Dietary Intake Data from a Randomized Controlled Trial. Nutrients. 2022; 14(21):4597. https://doi.org/10.3390/nu14214597
Chicago/Turabian StyleDressler, Justina, Maximilian Andreas Storz, Carolin Müller, Farid I. Kandil, Christian S. Kessler, Andreas Michalsen, and Michael Jeitler. 2022. "Does a Plant-Based Diet Stand Out for Its Favorable Composition for Heart Health? Dietary Intake Data from a Randomized Controlled Trial" Nutrients 14, no. 21: 4597. https://doi.org/10.3390/nu14214597