
Moringa oleifera Leaf Supplementation as a Glycemic Control Strategy in Subjects with Prediabetes

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
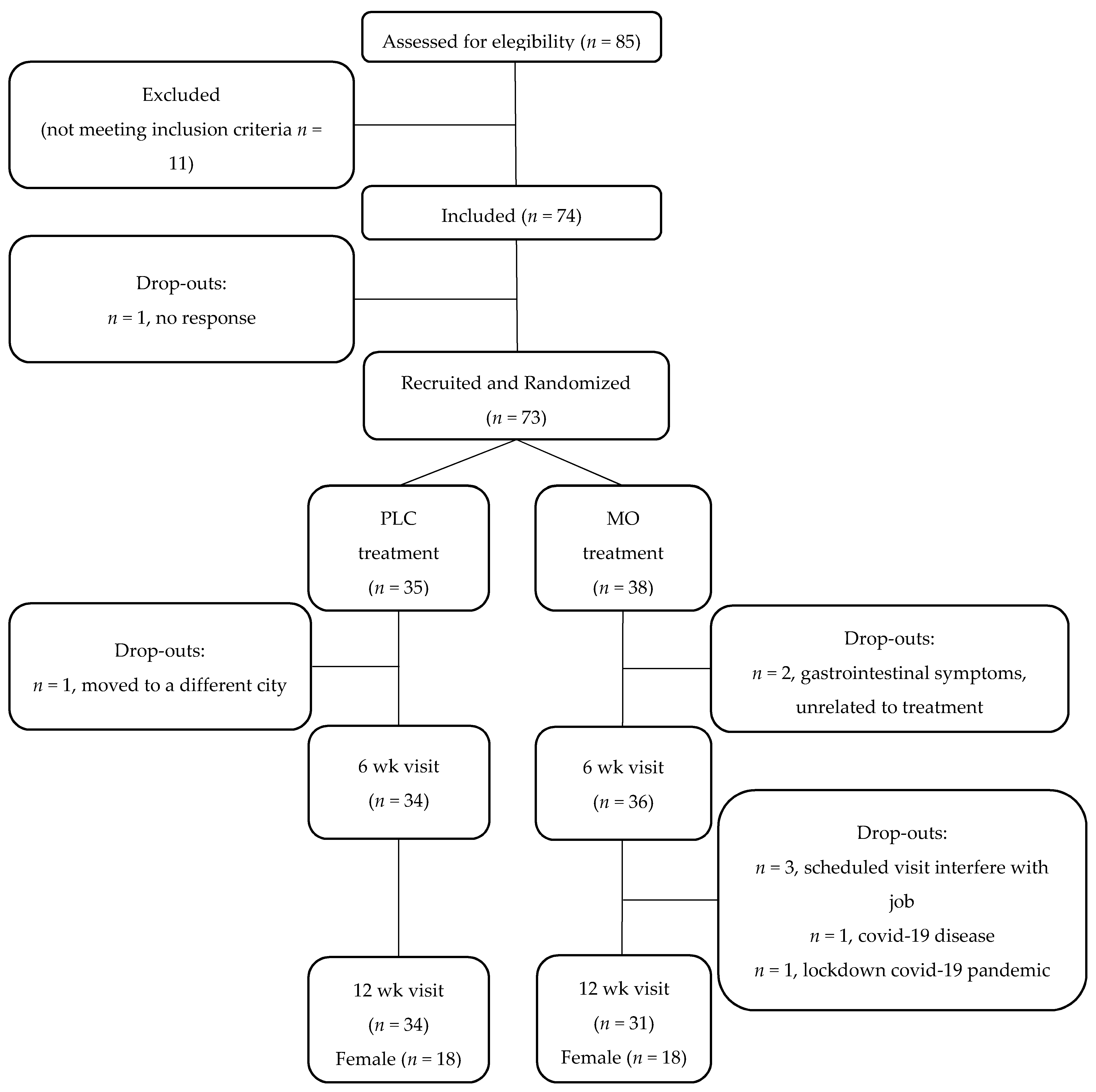
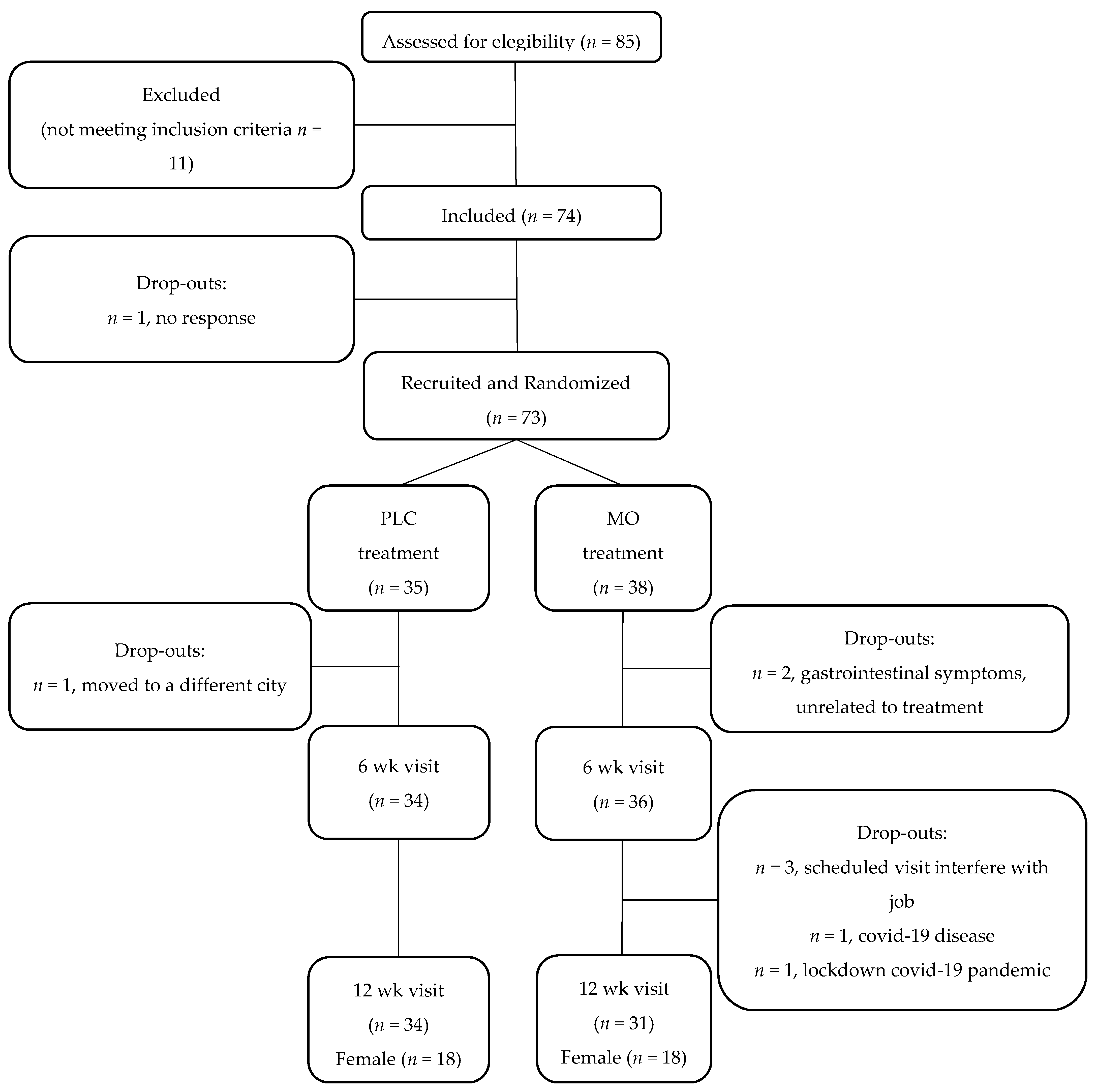
2.1. Study Design
2.2. Study Participants
2.3. Intervention
2.4. Outcomes
2.5. FBG and HbA1c Assessments
2.6. Assessment of Secondary Outcome Measures
2.7. Diet and Anthropometry Assessments
2.8. Sample Size
2.9. Randomization
2.10. Postprandial Study
2.11. Statistical Analysis
3. Results
3.1. Dose Study
3.2. Glycemic Control
3.3. Secondary Outcomes Analyses
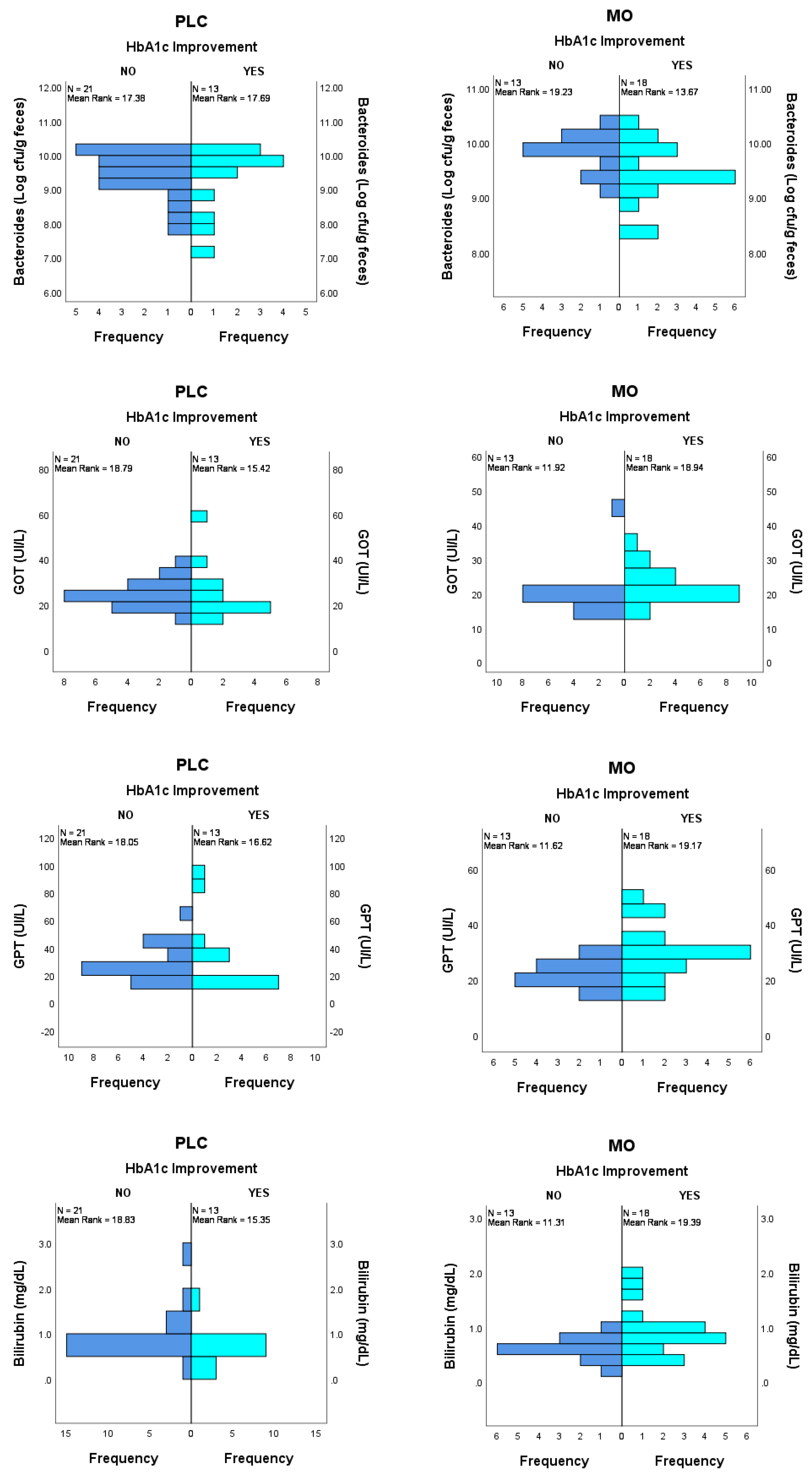
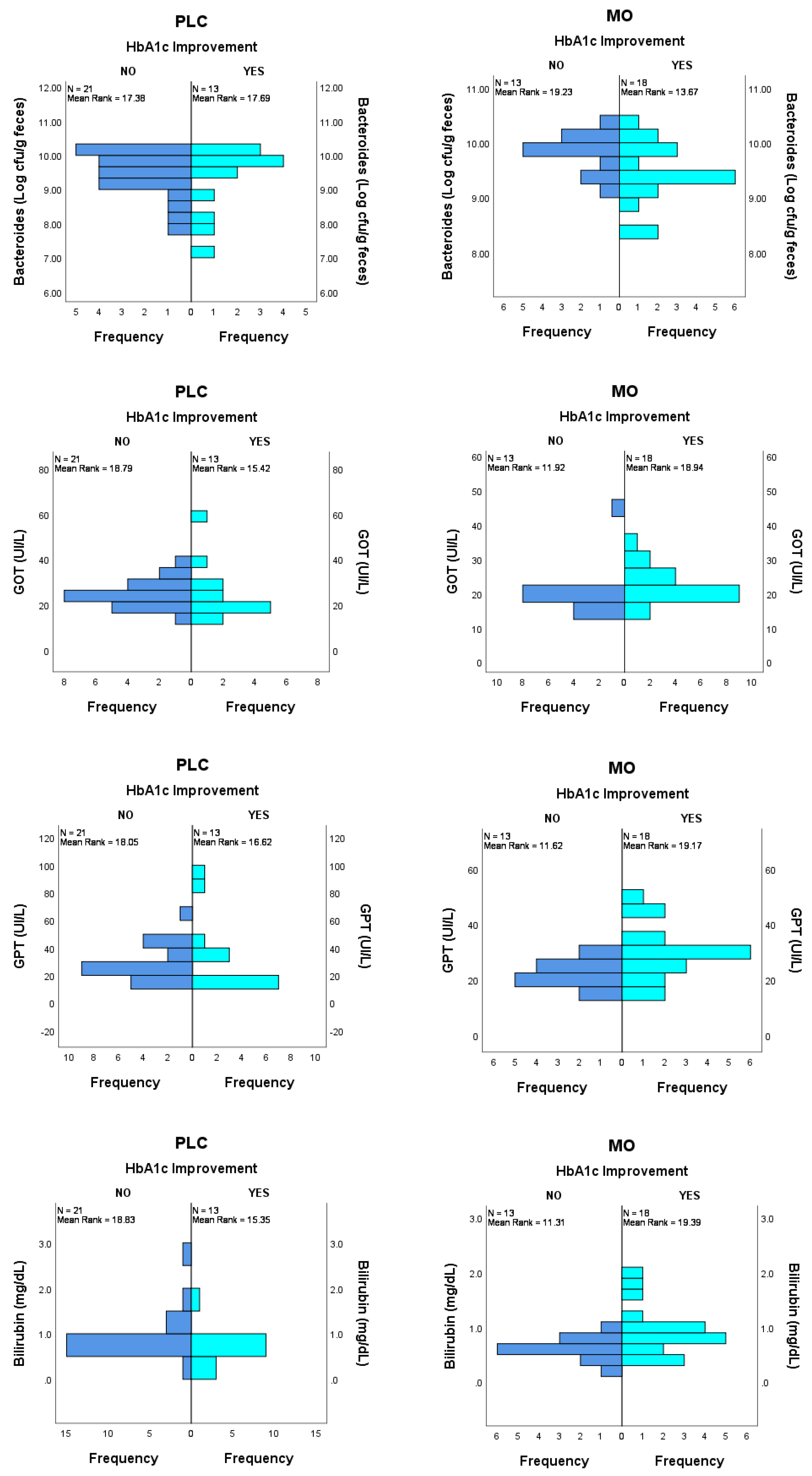
3.4. Prediction of HbA1c Improvement by Basal Biomarker Levels
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leone, A.; Spada, A.; Battezzati, A.; Schiraldi, A.; Aristil, J.; Bertoli, S. Cultivation, Genetic, Ethnopharmacology, Phytochemistry and Pharmacology of Moringa oleifera Leaves: An Overview. Int. J. Mol. Sci. 2015, 16, 12791–12835. [Google Scholar] [CrossRef]
- Taher, M.; Bin Nyeem, M.; Ahammed, M.; Hossain, M.; Nazrul Islam, M. Moringa oleifera (Shajna): The wonderful indigenous medicinal plant. Asian J. Med. Biol. Res. 2017, 3, 20–30. [Google Scholar] [CrossRef] [Green Version]
- Kou, X.; Li, B.; Olayanju, J.B.; Drake, J.M.; Chen, N. Nutraceutical or Pharmacological Potential of Moringa oleifera Lam. Nutrients 2018, 10, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waterman, C.; Rojas-Silva, P.; Tumer, T.B.; Kuhn, P.; Richard, A.J.; Wicks, S.; Stephens, J.M.; Wang, Z.; Mynatt, R.; Cefalu, W.; et al. Isothiocyanate-rich Moringa oleifera extract reduces weight gain, insulin resistance, and hepatic gluconeogenesis in mice. Mol. Nutr. Food Res. 2015, 59, 1013–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vergara-Jimenez, M.; Almatrafi, M.M.; Fernandez, M.L. Bioactive Components in Moringa Oleifera Leaves Protect against Chronic Disease. Antioxidants 2017, 6, 91. [Google Scholar] [CrossRef] [Green Version]
- Dou, Z.; Chen, C.; Fu, X. Bioaccessibility, antioxidant activity and modulation effect on gut microbiota of bioactive compounds from Moringa oleifera Lam. leaves during digestion and fermentation in vitro. Food Funct. 2019, 10, 5070–5079. [Google Scholar] [CrossRef]
- González Garza, N.G.; Chuc Koyoc, J.A.; Torres Castillo, J.A.; García Zambrano, E.A.; Betancur Ancona, D.; Chel Guerrero, L.; Sinagawa García, S.R. Biofunctional properties of bioactive peptide fractions from protein isolates of moringa seed (Moringa oleifera). J. Food Sci. Technol. 2017, 54, 4268–4276. [Google Scholar] [CrossRef]
- Wang, F.; Bao, Y.F.; Si, J.J.; Duan, Y.; Weng, Z.B.; Shen, X.C. The Beneficial Effects of a Polysaccharide from Moringa oleifera Leaf on Gut Microecology in Mice. J. Med. Food 2019, 22, 907–918. [Google Scholar] [CrossRef]
- Tian, H.; Liang, Y.; Liu, G.; Li, Y.; Deng, M.; Liu, D.; Guo, Y.; Sun, B. Moringa oleifera polysaccharides regulates caecal microbiota and small intestinal metabolic profile in C57BL/6 mice. Int. J. Biol. Macromol. 2021, 1, 595–611. [Google Scholar] [CrossRef]
- Jaja-Chimedza, A.; Graf, B.L.; Simmler, C.; Kim, Y.; Kuhn, P.; Pauli, G.F.; Raskin, I. Biochemical characterization and anti-inflammatory properties of an isothiocyanate-enriched moringa (Moringa oleifera) seed extract. PLoS ONE 2017, 12, e0182658. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Li, W.; Wu, R.; Yin, R.; Sargsyan, D.; Raskin, I.; Kong, A.N. Epigenome and transcriptome study of moringa isothiocyanate in mouse kidney mesangial cells induced by high glucose, a potential model for diabetic-induced nephropathy. AAPS J. 2019, 5, 8. [Google Scholar] [CrossRef] [PubMed]
- Sreedharan, N.; Mahadev, R.; Sonal Sekhar, M. Targeting Prediabetes to Preempt Diabetes (Chap 3). In Nutritional and Therapeutic Interventions for Diabetes and Metabolic Syndrome, 2nd ed.; Bagchi, D., Nair, S., Eds.; Elsevier: Amsterdam, The Netherlands; Academic Press: Cambridge, MA, USA, 2018; pp. 33–42. [Google Scholar] [CrossRef]
- Nova, E.; Redondo-Useros, N.; Martínez-García, R.M.; Gómez-Martínez, S.; Díaz-Prieto, L.E.; Marcos, A. Potential of Moringa oleifera to Improve Glucose Control for the Prevention of Diabetes and Related Metabolic Alterations: A Systematic Review of Animal and Human Studies. Nutrients 2020, 10, 2050. [Google Scholar] [CrossRef]
- Vargas-Sánchez, K.; Garay-Jaramillo, E.; González-Reyes, R.E. Effects of Moringa oleifera on Glycemia and Insulin Levels: A Review of Animal and Human Studies. Nutrients 2019, 11, 2907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, J.; Khan, I.; Johnson, S.K.; Alam, I.; Din, Z.U. Effect of Incorporating Stevia and Moringa in Cookies on Postprandial Glycemia, Appetite, Palatability, and Gastrointestinal Well-Being. J. Am. Coll. Nutr. 2018, 37, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Anthanont, P.; Lumlerdkij, N.; Akarasereenont, P.; Vannasaeng, S.; Sriwijitkamol, A. Moringa oleifera Leaf Increases Insulin Secretion after Single Dose Administration: A Preliminary Study in Healthy Subjects. J. Med. Assoc. Thail. 2016, 99, 308–313. [Google Scholar]
- Fombang, E.N.; Saa, W.R. Antihyperglycemic Activity of Moringa oleifera Lam leaf functional tea in rat models and human subjects. Food Nutr. Sci. 2016, 7, 1021–1032. [Google Scholar] [CrossRef] [Green Version]
- Leone, A.; Bertoli, S.; Di Lello, S.; Bassoli, A.; Ravasenghi, S.; Borgonovo, G.; Forlani, F.; Battezzati, A. Effect of Moringa oleifera Leaf Powder on Postprandial Blood Glucose Response: In Vivo Study on Saharawi People Living in Refugee Camps. Nutrients 2018, 10, 1494. [Google Scholar] [CrossRef] [Green Version]
- Kumari, D.J. Hypoglycemic effect of Moringa oleifera and Azadirachta indica in type-2 diabetes. Bioscan 2010, 5, 211–214. [Google Scholar]
- Giridhari, V.A.; Malathi, D.; Geetha, K. Anti diabetic property of drumstick (Moringa oleifera) leaf tablets. Int. J. Health Nutr. 2011, 2, 1–5. [Google Scholar]
- Kushwaha, S.; Chawla, P.; Kochhar, A. Effect of supplementation of drumstick (Moringa oleifera) and amaranth (Amaranthus tricolor) leaves powder on antioxidant profile and oxidative status among postmenopausal women. J. Food Sci. Technol. 2014, 51, 3464–3469. [Google Scholar] [CrossRef] [Green Version]
- Taweerutchana, R.; Lumlerdkij, N.; Vannasaeng, S.; Akarasereenont, P.; Sriwijitkamol, A. Effect of Moringa oleifera Leaf Capsules on Glycemic Control in Therapy-Naïve Type 2 Diabetes Patients: A Randomized Placebo Controlled Study. Evid.-Based Complementary Altern. Med. 2017, 2017, 6581390. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Standards of medical care in diabetes. Diabetes Care 2013, 36, S11–S66. [Google Scholar] [CrossRef] [Green Version]
- González-Zancada, N.; Redondo-Useros, N.; Díaz, L.E.; Gómez-Martínez, S.; Marcos, A.; Nova, E. Association of Moderate Beer Consumption with the Gut Microbiota and SCFA of Healthy Adults. Molecules 2020, 25, 4772. [Google Scholar] [CrossRef]
- Redondo, N.; García-González, N.; Diaz-Prieto, L.E.; Olmedilla-Alonso, B.; Martín-Diana, A.B.; Asensio-Vegas, C.; Nova, E. Effects of ewe’s milk yogurt (whole and semi-skimmed) and cow’s milk yogurt on inflammation markers and gut microbiota of subjects with borderline-high plasma cholesterol levels: A crossover study. Eur. J. Nutr. 2019, 58, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Olayaki, L.A.; Irekpita, J.E.; Yakubu, M.T.; Ojo, O.O. Methanolic extract of Moringa oleifera leaves improves glucose tolerance, glycogen synthesis and lipid metabolism in alloxan-induced diabetic rats. J. Basic Clin. Physiol. Pharmacol. 2015, 26, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Choi, E.J.; Han, W.C.; Oh, M.; Kim, J.; Hwang, J.Y.; Park, P.J.; Moon, S.H.; Kim, Y.S.; Kim, E.K. Moringa oleifera from Cambodia ameliorates oxidative stress, hyperglycemia, and kidney dysfunction in type 2 diabetic mice. J. Med. Food 2017, 20, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Paula, P.C.; Sousa, D.O.; Oliveira, J.T.; Carvalho, A.F.; Alves, B.G.; Pereira, M.L.; Farias, D.F.; Viana, M.P.; Santos, F.A.; Morais, T.C.; et al. A protein isolate from Moringa oleifera leaves has hypoglycemic and antioxidant effects in alloxan-induced diabetic mice. Molecules 2017, 22, 271. [Google Scholar] [CrossRef] [Green Version]
- Egbuna, C.; Awuchi, C.G.; Kushwaha, G.; Rudrapal, M.; Patrick-Iwuanyanwu, K.C.; Singh, O.; Odoh, U.E.; Khan, J.; Jeevanandam, J.; Kumarasamy, S.; et al. Bioactive Compounds Effective Against Type 2 Diabetes Mellitus: A Systematic Review. Curr. Top. Med. Chem. 2021, 21, 1067–1095. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.L.; Xu, Y.B.; Wu, J.L.; Li, N.; Guo, M.Q. Hypoglycemic and hypolipidemic effects of Moringa oleifera leaves and their functional chemical constituents. Food Chem. 2020, 15, 127478. [Google Scholar] [CrossRef] [PubMed]
- Zainab, B.; Ayaz, Z.; Alwahibi, M.S.; Khan, S.; Rizwana, H.; Soliman, D.W.; Alawaad, A.; Mehmood Abbasi, A. In-silico elucidation of Moringa oleifera phytochemicals against diabetes mellitus. Saudi J. Biol. Sci. 2020, 27, 2299–2307. [Google Scholar] [CrossRef]
- Oboh, G.; Oyeleye, S.I.; Akintemi, O.A.; Olasehinde, T.A. Moringa oleifera supplemented diet modulates nootropic-related biomolecules in the brain of STZ-induced diabetic rats treated with acarbose. Metab. Brain Dis. 2018, 33, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Villarruel-López, A.; López-de la Mora, D.A.; Vázquez-Paulino, O.D.; Puebla-Mora, A.G.; Torres-Vitela, M.R.; Guerrero-Quiroz, L.A.; Nuño, K. Effect of Moringa oleifera consumption on diabetic rats. BMC Complementary Altern. Med. 2018, 18, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisanz, J.E.; Enos, M.K.; PrayGod, G.; Seney, S.; Macklaim, J.M.; Chilton, S.; Willner, D.; Knight, R.; Fusch, C.; Fusch, G.; et al. Microbiota at Multiple Body Sites during Pregnancy in a Rural Tanzanian Population and Effects of Moringa-Supplemented Probiotic Yogurt. Appl. Environ. Microbiol. 2015, 81, 4965–4975. [Google Scholar] [CrossRef] [Green Version]
- Colldén, G.; Tschöp, M.H.; Müller, T.D. Therapeutic Potential of Targeting the Ghrelin Pathway. Int. J. Mol. Sci. 2017, 18, 798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajibade, T.O.; Arowolo, R.; Olayemi, F.O. Phytochemical screening and toxicity studies on the methanol extract of the seeds of Moringa oleifera. J. Complementary Integr. Med. 2013, 10, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Stohs, S.J.; Hartman, M.J. Review of the Safety and Efficacy of Moringa oleifera. Phytother. Res. 2015, 29, 796–804. [Google Scholar] [CrossRef]
- Omodanisi, E.I.; Aboua, Y.G.; Chegou, N.N.; Oguntibeju, O.O. Hepatoprotective, Antihyperlipidemic, and Anti-inflammatory Activity of Moringa oleifera in Diabetic-induced Damage in Male Wistar Rats. Pharmacogn. Res. 2017, 9, 182–187. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| PLC (n = 34) | MO (n = 31) | p | |
|---|---|---|---|
| Male:Female # (n, %) | 16/18 (47/53) | 13/18 (42/58) | 0.678 |
| Age (y) | 56.1 ± 10.8 | 56.2 ± 9.2 | 0.967 |
| Weight (kg) | 79.2 ± 13.0 | 79.5 ± 14.1 | 0.928 |
| Height (cm) | 166.5 ± 10.0 | 164.4 ± 10.8 | 0.421 |
| BMI | 28.6 ± 3.8 | 29.4 ± 4.0 | 0.408 |
| 1WC (cm) | |||
| Male | 95.5 ± 11.2 | 101.3 ± 9.7 | 0.161 |
| Female | 92.3 ± 11.0 | 94.1 ± 8.7 | 0.581 |
| 0 wk | 6 wk | 12 wk | p# | Rate of Change 0–12 wk | ||
|---|---|---|---|---|---|---|
| Glucose (mg/dL) | PLC | 104.2 ± 15.7 | 104.5 ± 18.0 | 106.2 ± 18.0 | 0.014 | 2.1 ± 9.9 |
| MO | 103.4 ± 10.8 | 106.9 ± 8.4 | 100.6 ± 8.7 | −2.3 ± 8.6 | ||
| pΦ = 0.049; Power = 0.51 | ||||||
| HbA1c (%) | PLC | 5.83 ± 0.37 | 5.85 ± 0.42 | 5.87 ± 0.47 | 0.030 | 0.7 ± 4.2 |
| MO | 5.88 ± 0.31 | 5.90 ± 0.35 | 5.79 ± 0.37 | −1.5 ± 3.7 | ||
| pΦ = 0.026 Power = 0.61 | ||||||
| Insulin (µUI/mL) | PLC | 8.74 ± 4.25 | 8.65 ± 2.80 | 10.56 ± 5.94 | 0.007 | 27.1 ± 57.7 |
| MO | 11.11 ± 5.21 | 13.46 ± 6.01 | 12.37 ± 5.18 | 17.3 ± 31.5 | ||
| NS | ||||||
| HOMA-IR | PLC | 2.26 ± 1.25 | 2.24 ± 0.82 | 2.83 ± 1.95 | 0.003 | 32.8 ± 78.3 |
| MO | 2.86 ± 1.41 | 3.56 ± 1.58 | 3.10 ± 1.33 | 15.6 ± 34.0 | ||
| NS |
| PLC, n (%) | MO, n (%) | p# | |
|---|---|---|---|
| Prediabetes | 27 (79.4) | 25 (80.6) | 0.901 |
| Normal | 7 (20.6) | 6 (19.4) |
| 0 wk | 6 wk | 12 wk | p# | Rate of Change 0–12 wk (p Φ) | ||
|---|---|---|---|---|---|---|
| Blautia coccoides- Eubacterium rectale | PLC | 11.56 ± 0.29 | 11.61 ± 0.45 | 11.75 ± 0.29 | 0.218 | 1.7 ± 3.3 |
| MO | 11.63 ± 0.32 | 11.72 ± 0.39 | 11.70 ± 0.38 | 0.7 ± 3.6 | ||
| NS | ||||||
| Bacteroides fragilis group. | PLC | 9.38 ± 0.80 | 9.39 ± 0.84 | 9.42 ± 0.67 | 0.482 | 0.6 ± 5.5 |
| MO | 9.59 ± 0.49 | 9.61 ± 0.57 | 9.58 ± 0.58 | −0.1 ± 4.5 | ||
| NS | ||||||
| Clostridium cluster IV | PLC | 8.39 ± 0.36 | 8.38 ± 0.58 | 8.49 ± 0.36 | 0.613 | 1.2 ± 5.2 |
| MO | 8.43 ± 0.33 | 8.47 ± 0.33 | 8.47 ± 0.39 | 0.5 ± 4.8 | ||
| NS | ||||||
| Bifidobacterium spp. | PLC | 7.76 ± 0.40 | 7.85 ± 0.47 | 7.90 ± 0.39 | 0.697 | 1.9 ± 4.8 |
| MO | 7.78 ± 0.39 | 7.85 ± 0.40 | 7.83 ± 0.41 | 0.9 ± 5.8 | ||
| NS | ||||||
| Enterobacteriaceae | PLC | 6.59 ± 1.15 | 6.56 ± 0.96 | 6.64 ± 1.02 | 0.404 | 3.5 ± 22.5 |
| MO | 6.18 ± 0.86 | 6.42 ± 1.07 | 6.57 ± 0.90 | 7.7 ± 17.5 | ||
| NS | ||||||
| Enterococcus spp. | PLC | 4.74 ± 1.02 | 5.14 ± 1.09 | 5.04 ± 1.0 | 0.016 | 9.1 ± 23.1 |
| MO | 4.89 ± 0.97 | 4.62 ± 0.80 | 4.87 ± 0.78 | 2.5 ± 21.9 | ||
| NS | ||||||
| Lactobacillus group | PLC | 4.34 ± 1.15 | 4.49 ± 1.06 | 4.67 ± 0.99 | 0.091 | 11.8 ± 26.9 |
| MO | 4.37 ± 0.80 | 4.05 ± 0.74 | 4.33 ± 0.70 | 1.0 ± 18.6 | ||
| NS | ||||||
| Faecalibacterium prausnitzii | PLC | 9.33 ± 0.36 | 9.38 ± 0.39 | 9.46 ± 0.35 | 0.438 | 1.5 ± 4.4 |
| MO | 9.42 ± 0.30 | 9.49 ± 0.35 | 9.46 ± 0.38 | 0.5 ± 4.0 | ||
| NS | ||||||
| Akkermansia muciniphila | PLC | 7.34 ± 1.25 | 6.99 ± 1.58 | 7.18 ± 1.43 | 0.885 | −1.3 ± 16.7 |
| MO | 7.19 ± 1.26 | 6.69 ± 1.33 | 6.96 ± 1.56 | −0.5 ± 27.0 | ||
| NS |
| 0 wk | 6 wk | 12 wk | GLM p # | Rate of Change 0–12 wk (p Φ) | ||
|---|---|---|---|---|---|---|
| Ghrelin (pg/mL) | PLC | 141.7 ± 91.2 | 128.6 ± 80.4 | 99.1 ± 70.6 | 0.997 | −30.7 ± 25.7 |
| MO | 134.5 ± 92.4 | 121.8 ± 76.6 | 87.5 ± 55.8 | −30.8 ± 26.2 | ||
| NS | ||||||
| PYY (pg/mL) | PLC | 37.4 ± 26.5 | 38.5 ± 26.5 | 30.1 ± 23.7 | 0.161 | −10.3 ± 36.0 |
| MO | 34.0 ± 20.4 | 29.1 ± 22.2 | 28.0 ± 23.2 | −1.8 ± 79.1 | ||
| NS | ||||||
| GLP-1 (pg/mL) | PLC | 6.8 ± 6.6 | 6.6 ± 7.7 | 5.4 ± 5.2 | 0.876 | 18.4 ± 135.8 |
| MO | 7.2 ± 5.6 | 6.2 ± 4.8 | 6.4 ± 6.8 | 6.1 ± 110.9 | ||
| NS |
| 0 wk | 6 wk | 12 wk | p# | Rate of Change 0–12 wk (p Φ) | ||
|---|---|---|---|---|---|---|
| Urea (mg/dL) | PLC | 36.9 ± 7.4 | 35.6 ± 7.9 | 37.2 ± 8.7 | 0.400 | 2.9 ± 20.1 |
| MO | 37.4 ± 6.7 | 38.5 ± 6.7 | 38.9 ± 7.4 | 4.8 ± 20.0 | ||
| NS | ||||||
| BUN (mg/dL) | PLC | 17.2 ± 3.4 | 16.6 ± 3.7 | 17.4 ± 4.1 | 0.402 | 2.9 ± 20.1 |
| MO | 17.5 ± 3.2 | 18.0 ± 3.1 | 18.1 ± 3.5 | 4.8 ± 19.9 | ||
| NS | ||||||
| Uric acid (mg/dL) | PLC | 5.73 ± 1.07 | 5.40 ± 0.93 | 5.67 ± 0.92 | 0.291 | 0.0 ± 10.7 |
| MO | 5.40 ± 1.45 | 5.40 ± 1.34 | 5.58 ± 1.34 | 3.3 ± 16.5 | ||
| NS | ||||||
| Creatinine (mg/dL) | PLC | 0.78 ± 0.17 | 0.72 ± 0.16 | 0.77 ± 0.16 | 0.785 | 0.7 ± 15.7 |
| MO | 0.76 ± 0.13 | 0.77 ± 0.13 | 0.76 ± 0.15 | 0.6 ± 12.2 | ||
| NS | ||||||
| Total Bilirubin (mg/dL) | PLC | 0.78 ± 0.44 | 0.71 ± 0.37 | 0.75 ± 0.39 | 0.880 | −0.1 ± 34.7 |
| MO | 0.76 ± 0.41 | 0.69 ± 0.34 | 0.73 ± 0.42 | −1.2 ± 32.8 | ||
| NS | ||||||
| GOT (UI/L) | PLC | 25.7 ± 8.7 | 22.2 ± 6.0 | 23.4 ± 7.7 | 0.028 | −3.1 ± 20.7 |
| MO | 21.8 ± 6.4 | 23.7 ± 9.5 | 23.5 ± 7.0 | 11.1 ± 31.2 | ||
| NS | ||||||
| GPT (UI/L) | PLC | 30.9 ± 19.1 | 27.0 ± 24.7 | 28.5 ± 14.8 | 0.339 | −0.4 ± 26.4 |
| MO | 26.4 ± 8.3 | 26.0 ± 9.8 | 26.8 ± 8.2 | 5.3 ± 32.4 | ||
| NS | ||||||
| GGT (UI/L) | PLC | 36.9 ± 41.0 | 36.0 ± 50.8 | 35.6 ± 36.6 | 0.549 | 3.6 ± 19.4 |
| MO | 30.4 ± 21.2 | 31.1 ± 20.4 | 29.1 ± 16.5 | 3.9 ± 30.7 | ||
| NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Martínez, S.; Díaz-Prieto, L.E.; Vicente Castro, I.; Jurado, C.; Iturmendi, N.; Martín-Ridaura, M.C.; Calle, N.; Dueñas, M.; Picón, M.J.; Marcos, A.; et al. Moringa oleifera Leaf Supplementation as a Glycemic Control Strategy in Subjects with Prediabetes. Nutrients 2022, 14, 57. https://doi.org/10.3390/nu14010057
Gómez-Martínez S, Díaz-Prieto LE, Vicente Castro I, Jurado C, Iturmendi N, Martín-Ridaura MC, Calle N, Dueñas M, Picón MJ, Marcos A, et al. Moringa oleifera Leaf Supplementation as a Glycemic Control Strategy in Subjects with Prediabetes. Nutrients. 2022; 14(1):57. https://doi.org/10.3390/nu14010057
Chicago/Turabian StyleGómez-Martínez, Sonia, Ligia E. Díaz-Prieto, Iván Vicente Castro, César Jurado, Nerea Iturmendi, Maria Carmen Martín-Ridaura, Nuria Calle, María Dueñas, María J. Picón, Ascensión Marcos, and et al. 2022. "Moringa oleifera Leaf Supplementation as a Glycemic Control Strategy in Subjects with Prediabetes" Nutrients 14, no. 1: 57. https://doi.org/10.3390/nu14010057