
Geospatial Analysis of Sodium and Potassium Intake: A Swiss Population-Based Study

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Food Frequency Questionnaire
2.3. Individual-Level Socio-Demographic Characteristics
2.4. Neighborhood Food Environment
2.5. Additional Area-Level Explanatory Variable
2.6. Exclusion Criteria
2.7. Regression Modelling
2.7.1. Ordinary Least Squares Regression Modelling
2.7.2. Geographically Weighted Regression Modelling
2.8. Spatial Analysis
2.8.1. Global Spatial Autocorrelation
2.8.2. Local Spatial Autocorrelation
3. Results
3.1. Descriptive Statistics
3.1.1. Sample Characteristics
3.1.2. Dietary Sources of Sodium and Potassium Intake
3.2. Regression Analyses
3.3. Spatial Analyses
3.3.1. Global Spatial Autocorrelation
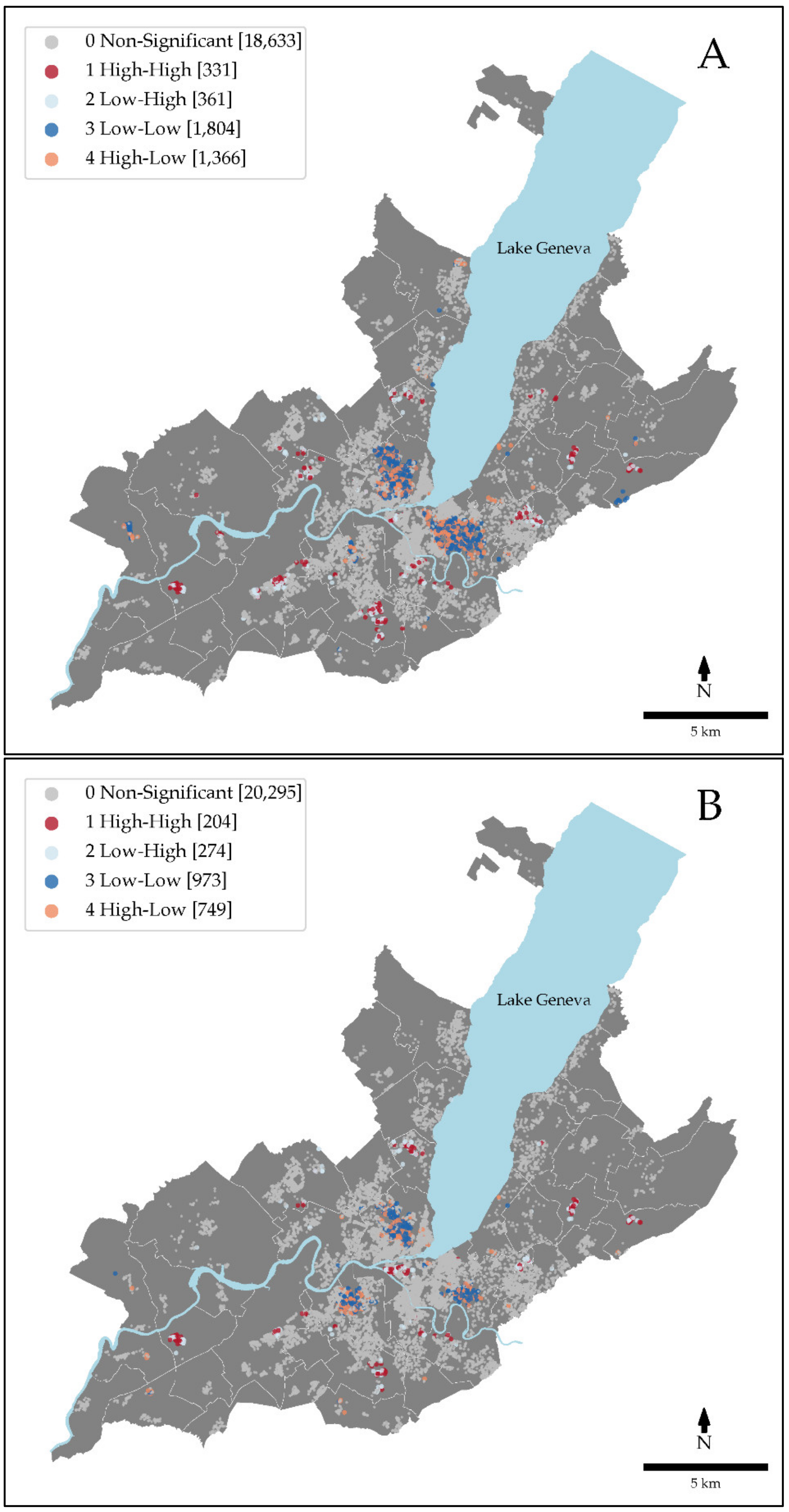
3.3.2. Local Spatial Autocorrelation
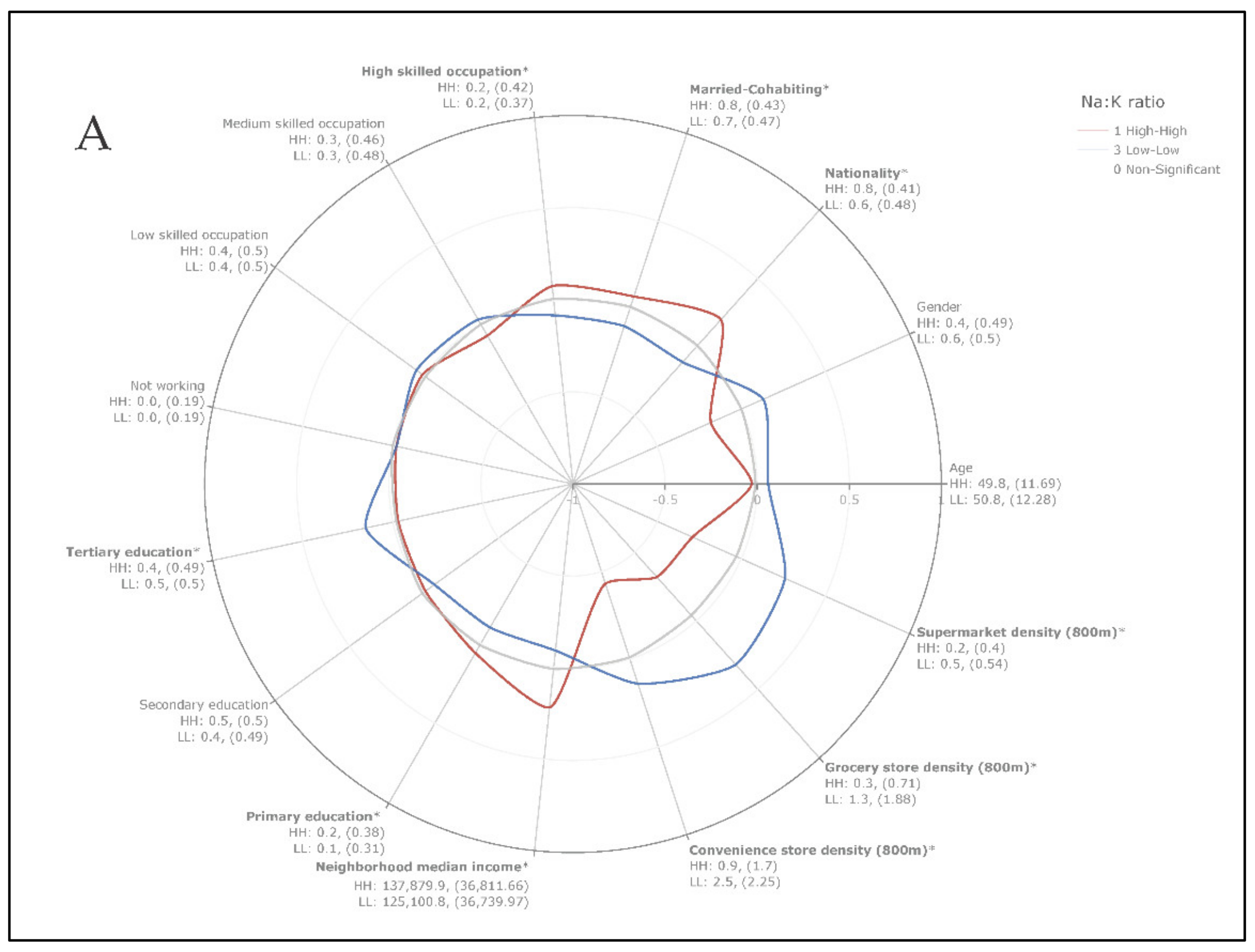
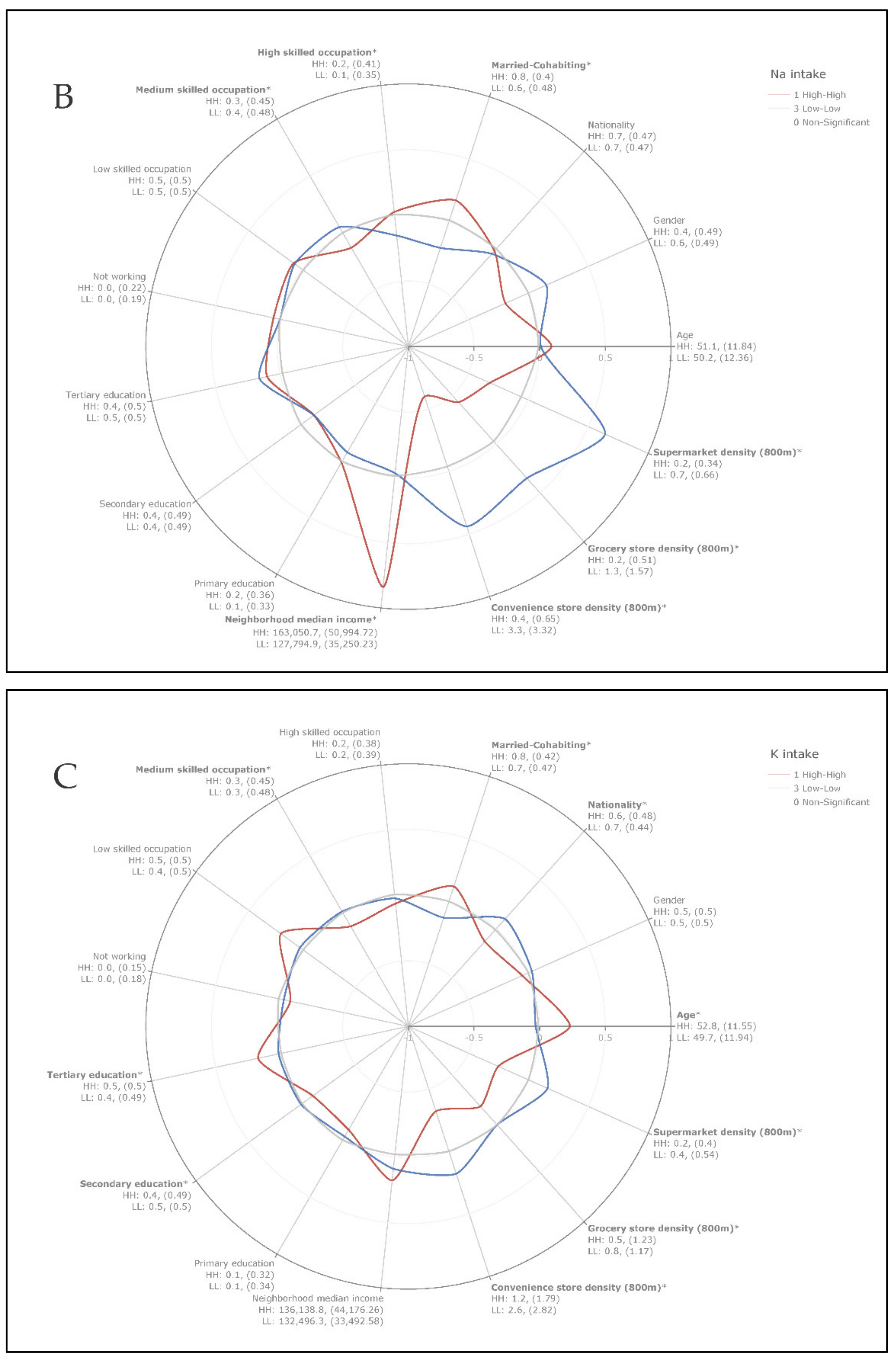
3.3.3. Socio-Demographic and Food Environment Differences between High-High and Low-Low Class Clusters of Unadjusted Na:K Ratio, Na, and K Intakes
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beevers, D.G. The atlas of heart disease and stroke. J. Hum. Hypertens. 2005, 19, 505. [Google Scholar] [CrossRef] [Green Version]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of lower sodium intake on health: Systematic review and meta-analyses. BMJ 2013, 346, f1326. [Google Scholar] [CrossRef] [Green Version]
- Intersalt Cooperative Research Group. Intersalt: An international study of electrolyte excretion and blood pressure. Results for 24 hour urinary sodium and potassium excretion. Intersalt Cooperative Research Group. BMJ 1988, 297, 319–328. [Google Scholar] [CrossRef] [Green Version]
- Yang, Q.; Liu, T.; Kuklina, E.V.; Flanders, W.D.; Hong, Y.; Gillespie, C.; Chang, M.-H.; Gwinn, M.; Dowling, N.; Khoury, M.J.; et al. Sodium and Potassium Intake and Mortality Among US Adults. Arch. Intern. Med. 2011, 171, 1183–1191. [Google Scholar] [CrossRef] [Green Version]
- Cook, N.R.; Cutler, J.A.; Obarzanek, E.; Buring, J.E.; Rexrode, K.M.; Kumanyika, S.K.; Appel, L.J.; Whelton, P.K. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: Observational follow-up of the trials of hypertension prevention (TOHP). BMJ 2007, 334, 885–888. [Google Scholar] [CrossRef] [Green Version]
- Cook, N.R.; Obarzanek, E.; Cutler, J.A.; Buring, J.E.; Rexrode, K.M.; Kumanyika, S.K.; Appel, L.J.; Whelton, P.K. Trials of Hypertension Prevention Collaborative Research Group. Joint Effects of Sodium and Potassium Intake on Subsequent Cardiovascular Disease: The Trials of Hypertension Prevention Follow-up Study. Arch. Intern. Med. 2009, 169, 32–40. [Google Scholar] [CrossRef] [Green Version]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R.; Simons-Morton, D.G.; et al. Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef]
- O’Donnell, M.; Mente, A.; Rangarajan, S.; McQueen, M.J.; Wang, X.; Liu, L.; Yan, H.; Lee, S.F.; Mony, P.; Devanath, A.; et al. Urinary Sodium and Potassium Excretion, Mortality, and Cardiovascular Events. N. Engl. J. Med. 2014, 371, 612–623. [Google Scholar] [CrossRef] [Green Version]
- Geleijnse, J.M.; Witteman, J.C.M.; Stijnen, T.; Kloos, M.W.; Hofman, A.; Grobbee, D.E. Sodium and potassium intake and risk of cardiovascular events and all-cause mortality: The Rotterdam Study. Eur. J. Epidemiol. 2007, 22, 763–770. [Google Scholar] [CrossRef] [Green Version]
- Adrogué, H.J.; Madias, N.E. Sodium and Potassium in the Pathogenesis of Hypertension. N. Engl. J. Med. 2007, 356, 1966–1978. [Google Scholar] [CrossRef] [Green Version]
- WHO. Guideline: Sodium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- WHO. Nutrition and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Consultation; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Beer-Borst, S.; Costanza, M.C.; Pechère-Bertschi, A.; Morabia, A. Twelve-year trends and correlates of dietary salt intakes for the general adult population of Geneva, Switzerland. Eur. J. Clin. Nutr. 2007, 63, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Glatz, N.; Chappuis, A.; Conen, D.; Erne, P.; Péchère-Bertschi, A.; Guessous, I.; Forni, V.; Gabutti, L.; Muggli, F.; Gallino, A.; et al. Associations of sodium, potassium and protein intake with blood pressure and hypertension in Switzerland. Swiss Med. Wkly. 2017, 147, w14411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibbins-Domingo, K.; Chertow, G.M.; Coxson, P.G.; Moran, A.E.; Lightwood, J.M.; Pletcher, M.J.; Goldman, L. Projected Effect of Dietary Salt Reductions on Future Cardiovascular Disease. N. Engl. J. Med. 2010, 362, 590–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appel, L.J.; Anderson, C.A. Compelling Evidence for Public Health Action to Reduce Salt Intake. N. Engl. J. Med. 2010, 362, 650–652. [Google Scholar] [CrossRef] [Green Version]
- Asaria, P.; Chisholm, D.; Mathers, C.; Ezzati, M.; Beaglehole, R. Chronic disease prevention: Health effects and financial costs of strategies to reduce salt intake and control tobacco use. Lancet 2007, 370, 2044–2053. [Google Scholar] [CrossRef]
- World Health Organization. Mapping Salt Reduction Initiatives in the WHO European Region; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Mühlemann, P. Rapport sur le sel; Mühlemann Nutrition: Uitikon, Switzerland, 2019. [Google Scholar]
- Ji, C.; Kandala, N.-B.; Cappuccio, F.P. Spatial variation of salt intake in Britain and association with socioeconomic status. BMJ Open 2013, 3, e002246. [Google Scholar] [CrossRef] [Green Version]
- Cappuccio, F.P.; Ji, C.; Donfrancesco, C.; Palmieri, L.; Ippolito, R.; Vanuzzo, D.; Giampaoli, S.; Strazzullo, P. Geographic and socioeconomic variation of sodium and potassium intake in Italy: Results from the MINISAL-GIRCSI programme. BMJ Open 2015, 5, e007467. [Google Scholar] [CrossRef] [Green Version]
- Ji, C.; Cappuccio, F.P. Socioeconomic inequality in salt intake in Britain 10 years after a national salt reduction programme. BMJ Open 2014, 4, e005683. [Google Scholar] [CrossRef] [Green Version]
- Yenerall, J.; You, W.; Hill, J. Investigating the Spatial Dimension of Food Access. Int. J. Environ. Res. Public Health 2017, 14, 866. [Google Scholar] [CrossRef] [Green Version]
- Rummo, P.E.; Meyer, K.A.; Boone-Heinonen, J.; Jacobs, D.R.; Kiefe, C.I.; Lewis, C.E.; Steffen, L.M.; Gordon-Larsen, P. Neighborhood Availability of Convenience Stores and Diet Quality: Findings From 20 Years of Follow-Up in the Coronary Artery Risk Development in Young Adults Study. Am. J. Public Health 2015, 105, e65–e73. [Google Scholar] [CrossRef]
- Joost, S.; De Ridder, D.; Marques-Vidal, P.; Bacchilega, B.; Theler, J.-M.; Gaspoz, J.-M.; Guessous, I. Overlapping spatial clusters of sugar-sweetened beverage intake and body mass index in Geneva state, Switzerland. Nutr. Diabetes 2019, 9, 1–10. [Google Scholar] [CrossRef]
- Dekker, L.H.; Rijnks, R.H.; Strijker, D.; Navis, G.J. A spatial analysis of dietary patterns in a large representative population in the north of The Netherlands—the Lifelines cohort study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 166. [Google Scholar] [CrossRef] [Green Version]
- Guessous, I.; Bochud, M.; Theler, J.-M.; Gaspoz, J.-M.; Pechère-Bertschi, A. 1999–2009 Trends in Prevalence, Unawareness, Treatment and Control of Hypertension in Geneva, Switzerland. PLoS ONE 2012, 7, e39877. [Google Scholar] [CrossRef] [Green Version]
- Morabia, A.; Bernstein, M.; Héritier, S.; Ylli, A. Community-Based Surveillance of Cardiovascular Risk Factors in Geneva: Methods, Resulting Distributions, and Comparisons with Other Populations. Prev. Med. 1997, 26, 311–319. [Google Scholar] [CrossRef]
- Morabia, A.; Bernstein, M.; Kumanyika, S.; Sorenson, A.; Mabiala, I.; Prodolliet, B.; Luong, B.L. Développement et validation d’un questionnaire alimentaire semi-quantitatif à partir d’une enquête de population. Int. J. Public Health 1994, 39, 345–369. [Google Scholar] [CrossRef]
- Belle, F.N.; Schindera, C.; Guessous, I.; Popovic, M.B.; Ansari, M.; Kuehni, C.E.; Bochud, M. Sodium and Potassium Intakes and Cardiovascular Risk Profiles in Childhood Cancer Survivors: The SCCSS-Nutrition Study. Nutrition 2019, 12, 57. [Google Scholar] [CrossRef] [Green Version]
- Home—The Swiss Food Composition Database. Published 2019. Available online: https://naehrwertdaten.ch/de/ (accessed on 7 January 2021).
- Ciqual: Table de Composition Nutritionnelle des Aliments. Available online: https://ciqual.anses.fr/ (accessed on 23 October 2020).
- Sandoval, J.L.; Leao, T.; Theler, J.-M.; Favrod-Coune, T.; Broers, B.; Gaspoz, J.-M.; Marques-Vidal, P.; Guessous, I. Alcohol control policies and socioeconomic inequalities in hazardous alcohol consumption: A 22-year cross-sectional study in a Swiss urban population. BMJ Open 2019, 9, e028971. [Google Scholar] [CrossRef] [Green Version]
- REG. Available online: https://www.ge.ch/utiliser-repertoire-entreprises-reg/consulter-reg (accessed on 7 January 2021).
- Historiques|SITG. Available online: https://ge.ch/sitg/donnees/historiques (accessed on 25 March 2020).
- Larsen, J.; El-Geneidy, A.; Yasmin, F. Beyond the Quarter Mile. Can. J. Urban Res. 2010, 19, 70–88. [Google Scholar] [CrossRef]
- Buehler, R.; Pucher, J.; Merom, D.; Bauman, A. Active Travel in Germany and the U.S.: Contributions of Daily Walking and Cycling to Physical Activity. Am. J. Prev. Med. 2011, 41, 241–250. [Google Scholar] [CrossRef]
- Boeing, G. OSMnx: New methods for acquiring, constructing, analyzing, and visualizing complex street networks. Comput. Environ. Urban Syst. 2017, 65, 126–139. [Google Scholar] [CrossRef] [Green Version]
- Foti, F.; Waddell, P.; Luxen, D. A Generalized Computational Framework for Accessibility: From the Pedestrian to the Metropolitan Scale. In Proceedings of the 4th Transportation Research Board Conference on Innovations in Travel Modeling, Tampa, FL, USA, 29 April–2 May 2012; Transportation Research Board: Washington, DC, USA, 2012; pp. 1–14. [Google Scholar]
- Agrawal, A.W.; Schlossberg, M.; Irvin, K. How Far, by Which Route and Why? A Spatial Analysis of Pedestrian Preference. J. Urban Des. 2008, 13, 81–98. [Google Scholar] [CrossRef]
- Duncan, D.T.; Castro, M.C.; Gortmaker, S.L.; Aldstadt, J.; Melly, S.J.; Bennett, G.G. Racial differences in the built environment—Body mass index relationship? A geospatial analysis of adolescents in urban neighborhoods. Int. J. Health Geogr. 2012, 11, 11. [Google Scholar] [CrossRef] [Green Version]
- Marques-Vidal, P.; Vollenweider, P.; Grange, M.; Guessous, I.; Waeber, G. Dietary intake of subjects with diabetes is inadequate in Switzerland: The CoLaus study. Eur. J. Nutr. 2016, 56, 981–989. [Google Scholar] [CrossRef]
- Ferro-Luzzi, G.; Schaerer, C. Analyse Des Inégalités Dans Le Canton de Genève; CATI-GE: Geneva, Switzerland, 2020. [Google Scholar]
- Chaix, B.; Merlo, J.; Chauvin, P. Comparison of a spatial approach with the multilevel approach for investigating place effects on health: The example of healthcare utilisation in France. J. Epidemiol. Commun. Health 2005, 59, 517–526. [Google Scholar] [CrossRef] [Green Version]
- Clary, C.; Lewis, D.J.; Flint, E.; Smith, N.R.; Kestens, Y.; Cummins, S. The Local Food Environment and Fruit and Vegetable Intake: A Geographically Weighted Regression Approach in the ORiEL Study. Am. J. Epidemiol. 2016, 184, 837–846. [Google Scholar] [CrossRef]
- Oshan, T.M.; Li, Z.; Kang, W.; Wolf, L.J.; Fotheringham, A.S. mgwr: A Python Implementation of Multiscale Geographically Weighted Regression for Investigating Process Spatial Heterogeneity and Scale. ISPRS Int. J. Geo-Inf. 2019, 8, 269. [Google Scholar] [CrossRef] [Green Version]
- O’Sullivan, D. Geographically Weighted Regression: The Analysis of Spatially Varying Relationships (review). Geogr. Anal. 2003, 35, 272–275. [Google Scholar] [CrossRef]
- Rey, S.J.; Anselin, L. PySAL: A Python Library of Spatial Analytical Methods. In Handbook of Applied Spatial Analysis; Springer: Berlin, Germany, 2009; Volume 37, pp. 175–193. [Google Scholar] [CrossRef]
- Ullah, A. Spatial Dependence in linear Regression Models with an Introduction to Spatial Econometrics. In Handbook of Applied Economic Statistics; Marcel Dekker: New York, NY, USA, 1998; pp. 257–259. [Google Scholar]
- Zhang, C.; Luo, L.; Xu, W.; Ledwith, V. Use of local Moran’s I and GIS to identify pollution hotspots of Pb in urban soils of Galway, Ireland. Sci. Total Environ. 2008, 398, 212–221. [Google Scholar] [CrossRef]
- Anselin, L. Local Indicators of Spatial Association-LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Stopka, T.J.; Krawczyk, C.; Gradziel, P.; Geraghty, E.M. Use of Spatial Epidemiology and Hot Spot Analysis to Target Women Eligible for Prenatal Women, Infants, and Children Services. Am. J. Public Health 2014, 104, S183–S189. [Google Scholar] [CrossRef]
- ArcGIS. Incremental Spatial Autocorrelation (Spatial Statistics)—ArcGIS Pro|Documentation. Available online: https://pro.arcgis.com/en/pro-app/latest/tool-reference/spatial-statistics/incremental-spatial-autocorrelation.htm (accessed on 19 March 2021).
- Openshaw, S. The Modifiable Areal Unit Problem; Geo Books: Norwich, UK, 1983; Volume 38. [Google Scholar]
- Chen, D.-R.; Truong, K. Using multilevel modeling and geographically weighted regression to identify spatial variations in the relationship between place-level disadvantages and obesity in Taiwan. Appl. Geogr. 2012, 32, 737–745. [Google Scholar] [CrossRef]
- Chi, S.-H.; Grigsby-Toussaint, D.S.; Bradford, N.; Choi, J. Can Geographically Weighted Regression improve our contextual understanding of obesity in the US? Findings from the USDA Food Atlas. Appl. Geogr. 2013, 44, 134–142. [Google Scholar] [CrossRef]
- Mennis, J. Mapping the Results of Geographically Weighted Regression. Cartogr. J. 2006, 43, 171–179. [Google Scholar] [CrossRef] [Green Version]
- Kauhl, B.; Maier, W.; Schweikart, J.; Keste, A.; Moskwyn, M. Exploring the small-scale spatial distribution of hypertension and its association to area deprivation based on health insurance claims in Northeastern Germany. BMC Public Health 2018, 18, 121. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, D.; Painho, M.; Roquette, R. A geographically weighted regression approach to investigate air pollution effect on lung cancer: A case study in Portugal. Geospat. Health 2019, 14, 35–45. [Google Scholar] [CrossRef]
- Comber, A.J.; Brunsdon, C.; Radburn, R. A spatial analysis of variations in health access: Linking geography, socio-economic status and access perceptions. Int. J. Health Geogr. 2011, 10, 44. [Google Scholar] [CrossRef] [Green Version]
- Galobardes, B.; Morabia, A.; Bernstein, M.S. Diet and socioeconomic position: Does the use of different indicators matter? Int. J. Epidemiol. 2001, 30, 334–340. [Google Scholar] [CrossRef] [Green Version]
- De Mestral, C.; Mayén, A.-L.; Petrovic, D.; Marques-Vidal, P.; Bochud, M.; Stringhini, S. Socioeconomic Determinants of Sodium Intake in Adult Populations of High-Income Countries: A Systematic Review and Meta-Analysis. Am. J. Public Health 2017, 107, e1–e12. [Google Scholar] [CrossRef]
- Suarez, J.J.; Isakova, T.; Anderson, C.A.; Boulware, L.E.; Wolf, M.; Scialla, J.J. Food Access, Chronic Kidney Disease, and Hypertension in the U.S. Am. J. Prev. Med. 2015, 49, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Mackenbach, J.D.; Burgoine, T.; Lakerveld, J.; Forouhi, N.G.; Griffin, S.J.; Wareham, N.J.; Monsivais, P. Accessibility and Affordability of Supermarkets: Associations With the DASH Diet. Am. J. Prev. Med. 2017, 53, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Drewnowski, A.; Rehm, C.D.; Maillot, M.; Monsivais, P. The relation of potassium and sodium intakes to diet cost among US adults. J. Hum. Hypertens. 2014, 29, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Hyseni, L.; Elliot-Green, A.; Lloyd-Williams, F.; Kypridemos, C.; O’Flaherty, M.; McGill, R.; Orton, L.; Bromley, H.; Cappuccio, F.P.; Capewell, S. Systematic review of dietary salt reduction policies: Evidence for an effectiveness hierarchy? PLoS ONE 2017, 12, e0177535. [Google Scholar] [CrossRef] [Green Version]
- Morrissey, E.; Giltinan, M.; Kehoe, L.; Nugent, A.P.; McNulty, B.A.; Flynn, A.; Walton, J. Sodium and Potassium Intakes and Their Ratio in Adults (18–90 y): Findings from the Irish National Adult Nutrition Survey. Nutrition 2020, 12, 938. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Value | ||
|---|---|---|
| Age, mean (SD) | 50.1 (12) | |
| Gender, n (%) | ||
| Woman | 11,237 (50) | |
| Man | 11,258 (50) | |
| Civil status, n (%) | ||
| Married/Cohabiting | 16,192 (72) | |
| Not married/cohabiting | 6303 (28) | |
| Occupation, n (%) | ||
| Low | 9530 (42) | |
| Medium | 7587 (34) | |
| High | 4478 (20) | |
| Not working | 900 (4) | |
| Education, n (%) | ||
| Primary | 3296 (15) | |
| Secondary | 10,252 (45) | |
| Tertiary | 8947 (40) | |
| Nationality, n (%) | ||
| Switzerland | 15,624 (70) | |
| Other | 6871 (30) | |
| Neighborhood median household income (CHF), mean (SD) | 128,831.4 (40,884.1) | |
| Sodium and Potassium intake, mean (SD) | ||
| Na Intake (g/day) | 3.7 (1.6) | |
| K Intake (g/day) | 2.7 (1.0) | |
| Na:K Ratio | 1.4 (0.5) | |
| Food environment, mean (SD) | ||
| Convenience store density (800 m) | 2.1 (2.8) | |
| Grocery store density (800 m) | 0.8 (1.4) | |
| Supermarket density (800 m) | 0.3 (0.5) | |
| SD, standard deviation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Ridder, D.; Belle, F.N.; Marques-Vidal, P.; Ponte, B.; Bochud, M.; Stringhini, S.; Joost, S.; Guessous, I. Geospatial Analysis of Sodium and Potassium Intake: A Swiss Population-Based Study. Nutrients 2021, 13, 1798. https://doi.org/10.3390/nu13061798
De Ridder D, Belle FN, Marques-Vidal P, Ponte B, Bochud M, Stringhini S, Joost S, Guessous I. Geospatial Analysis of Sodium and Potassium Intake: A Swiss Population-Based Study. Nutrients. 2021; 13(6):1798. https://doi.org/10.3390/nu13061798
Chicago/Turabian StyleDe Ridder, David, Fabiën N. Belle, Pedro Marques-Vidal, Belén Ponte, Murielle Bochud, Silvia Stringhini, Stéphane Joost, and Idris Guessous. 2021. "Geospatial Analysis of Sodium and Potassium Intake: A Swiss Population-Based Study" Nutrients 13, no. 6: 1798. https://doi.org/10.3390/nu13061798