Systematic Review: Effect of Health Education Intervention on Improving Knowledge, Attitudes and Practices of Adolescents on Malnutrition

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Method
2.2. Eligibility Criteria
- Population:
- Adolescents age 10 to 19 years old with a minimum study population of 50. Study population below the age of 10 years and above 19 years were excluded from the study.
- Intervention:
- Interventions on nutrition, healthy eating/diet, dietary intake, anemia, fruits and vegetables were included in the study.
- Comparison:
- A comparison group with no intervention or given other trial interventions were included. Studies with no direct comparison group, such as quasi experimental studies, were excluded from the study.
- Outcome:
- Studies with knowledge or attitude or practice as the study outcome were included.
- Study design:
- Randomized controlled trials/clustered randomized control trials were included in the study. Studies with quasi experimental studies, non-randomized controlled trials, or the study design not mentioned were excluded.
2.3. Data Extraction
2.4. Quality Assessment of the Study
2.4.1. Risk of Bias
2.4.2. GRADE Quality Assessment
2.5. Intervention Intensity
- The duration of the intervention. This shows the length of the intervention (1 = ≤6 weeks, 2 = 6 to 11 weeks, 3 = 12 weeks to 5 months, 4 = 6 to 12 months, 5 = ≥12 months).
- The frequency of contact with the intervention. This assessed the frequency of contact between the intervention and the participants. In cases where the intervention used more than one contact, the average score of contact was calculated. The score on frequency of contact ranges from (1 = annually, 2 = bimonthly to quarterly, 3 = monthly, 4 = weekly, 5 = daily).
- Type of contact (level of personalization). This assessed the type and the level of contact with the intervention. 1 = environmental, 2 = adolescent only, 3 = group (adolescents and teachers), 4 = group (adolescents and parents), 5 = group (adolescents and parents and teachers and community).
- The reach of the intervention strategies. This assessed the different settings used where 1 = one setting, 3 = two settings and 5 = three or more settings. The larger the number of settings in the intervention, the greater the intensity of the intervention.
3. Results
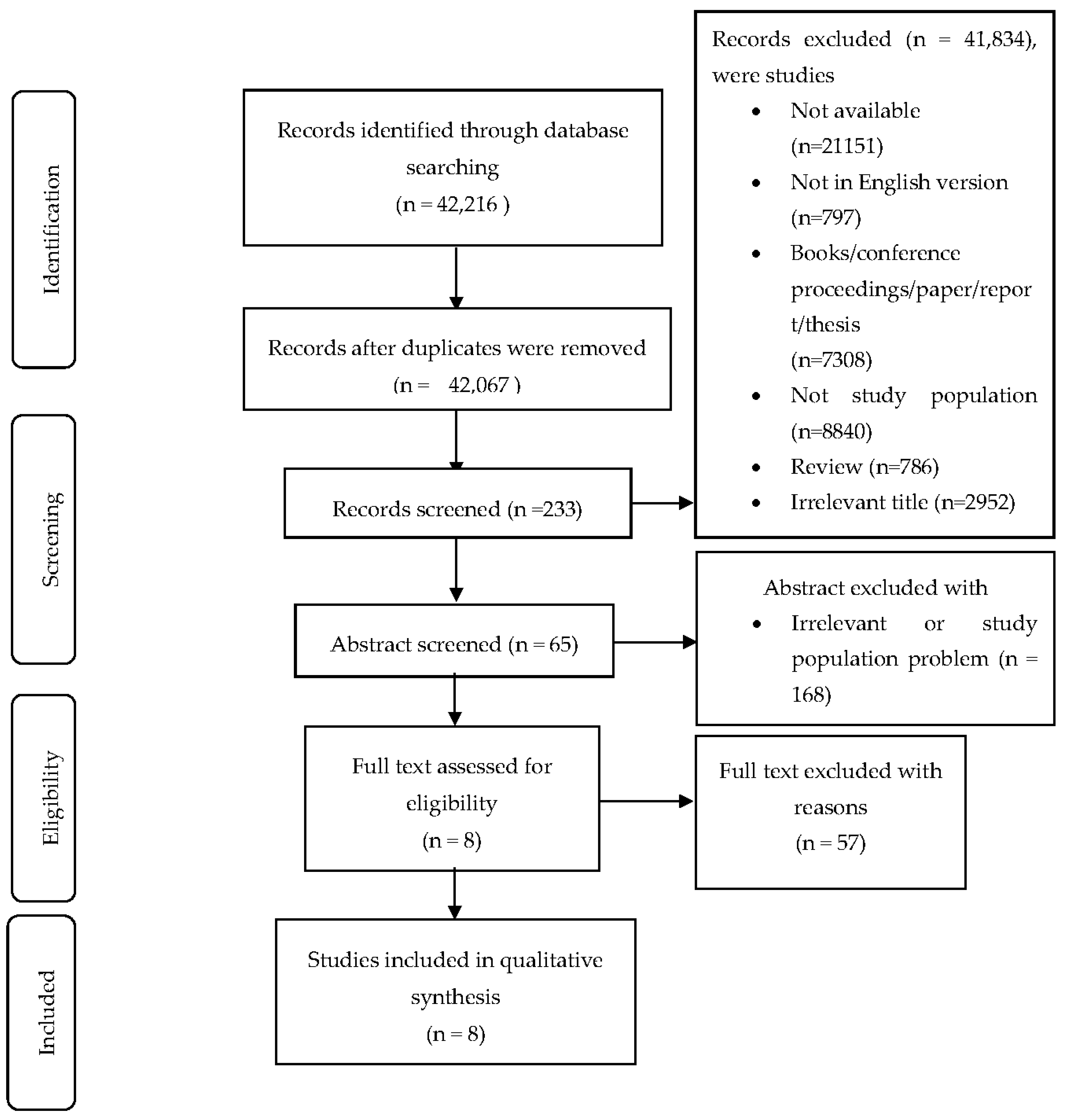
3.1. Search Findings
3.1.1. Study Characteristics
3.1.2. Country and Study Design
3.1.3. Setting and Target Population
3.1.4. Duration, Approaches and Contents of Intervention
3.1.5. Sample Size, Control Group, Effect Size, Attrition Rate
3.1.6. The Use of Theory
3.1.7. Intervention Intensity
3.2. Quality of Reporting
3.2.1. Risk of Bias
3.2.2. Grades of Recommendation, Assessment, Development and Evaluation (GRADE)
3.3. Effect of the Intervention
3.3.1. Knowledge
3.3.2. Attitude
3.3.3. Practice
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UNICEF. The State of the World’s Children 2011-Executive Summary: Adolescence an Age of Opportunity; UNICEF: New York, NY, USA, 2011; ISBN 9789280645552.
- WHO. The Global Strategy for Women’s and Children’s and Adolescents’ Health (2016–2030): Survive, Thrive, Transform; United Nations: New York, NY, USA, 2015; Volume 1, pp. 1–108.
- World Health Organization. The Optimal Duration of Exclusive Breastfeeding: Report of an Expert Consultation: Geneva, Switzerland 28–30 March 2001; World Health Organization: Geneva, Switzerland, 2002; pp. 1–10. Available online: https://www.who.int/nutrition/publications/infantfeeding/WHO_NHD_01.09/en/ (accessed on 17 May 2018).
- Bakrania, S.; Ghimire, A.; Balvin, N. Bridging the Gap to Understand Effective Interventions for Adolescent Well-Being: An Evidence Gap Map on Protection, Participation, and Financial and Material Well-Being in Low-And Middle-Income Countries; UNICEF Office of Research-Innocenti: New York, NY, USA, 2018; pp. 1–63. [Google Scholar]
- Christian, P.; Smith, E.R. Adolescent Undernutrition: Global Burden, Physiology, and Nutritional Risks. Ann. Nutr. Metab. 2018, 72, 316–328. [Google Scholar] [CrossRef] [PubMed]
- UNFPA & UNICEF. Fact Sheet: Girls and Young Women. In United Nations Adolescent Girls Task Force; United Nations: New York, NY, USA, 2012; pp. 1–6. [Google Scholar]
- Ward, S.; Hisley, S. Maternal-Child Nursing Care Optimizing Outcomes for Mothers, Children, and Families; F.A. Davis Company: Philadelphia, PA, USA, 2015; ISBN 9780803614864. [Google Scholar]
- World Health Organization. Guideline: Implementing Effective Actions for Improving Adolescent Nutrition; World Health Organization: Geneva, Switzerland, 2018; ISBN 9789241513708.
- Mokhtari, F.; Kazemi, A.; Soheila, E. Effect of educational intervention program for parents on adolescents’nutritional behaviors in Isfahan in 2016. J. Educ. Health Promot. 2017, 6. [Google Scholar] [CrossRef]
- Blum, R.W.; Gates, W.H. Girlhood, not Motherhood Preventing Adolescent Pregnancy; United Nations Population Fund UNFPA: New York, NY, USA, 2015; pp. 1–62. ISBN 9780897149860. [Google Scholar]
- WHO. Nutrition in Adolescence—Issues and Challenges for the Health Sector; World Health Organization: Geneva, Switzerland, 2005; pp. 1–123.
- Sireesha, G.; Rajani, N.; Bindu, V. Teenage girls ’ knowledge attitude and practices on nutrition. Int. J. Home Sci. 2017, 3, 491–494. [Google Scholar]
- World Health organization(WHO). Adolescents: Agents of Change for a Well-Nourished World: An Expert Consultation on Nutrition Programming for the Next Generation. 19–20 June 2018. Available online: https://www.who.int/nutrition/events/2018-consultation-adolescents-19to29jun/en/ (accessed on 17 September 2019).
- World Health Organization. Adolescent Pregnancy: Issues in Adolescent Health and Development; World Health Organization: Geneva, Switzerland, 2004; pp. 1–92.
- World Health Organization. Adolescent Nutrition: A Review of the Situation in Selected South-East Asian Countries (No. SEA-NUT-163); Available online: https://apps.who.int/iris/handle/10665/204764 (accessed on 1 June 2018).
- Branca, F.; Piwoz, E.; Schultink, W.; Sullivan, L.M. Nutrition and health in women, children, and adolescent girls. Br. Med. J. 2015, 351, h4173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; De Onis, M.; Ezzati, M.; Grantham-Mcgregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Akseer, N.; Al-gashm, S.; Mehta, S.; Mokdad, A.; Bhutta, Z.A. Global and regional trends in the nutritional status of young people: A critical and neglected age group. Ann. N. Y. Acad. Sci. 2017, 1393, 3–20. [Google Scholar] [CrossRef] [Green Version]
- NCD Risk Factor Collaboration (NCD-RisC) Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [CrossRef] [Green Version]
- Gupta, A.; Noronha, J.A.; Garg, M. Dietary intake of macronutrients and micronutrients among adolescent girls: A cross sectional study. Clin. Epidemiol. Glob. Health 2018, 6, 192–197. [Google Scholar] [CrossRef] [Green Version]
- Mangiaterra, V.; Pendse, R.; Mcclure, K.; Rosen, J.; Mouli, V.; Camacho, V.; Mathai, M.; Portela, A.; Zupan, J.; Olukoya, P. Adolescent Pregnancy. WHO MPS Notes 2008, 1, 1–4. [Google Scholar]
- Nelima, D. Prevalence and Determinants of Anaemia among Adolescent Girls in Secondary Schools in Yala Division Siaya District, Kenya. Univers. J. Food Nutr. Sci. 2015, 3, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Rosen, J.E.; Adolescent Health and Development (AHD); The World Bank. 2004 Apr:281627-1095698140167. Available online: https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.630.384&rep=rep1&type=pdf (accessed on 6 March 2018).
- Promoting Girls’ Nutrition in Early Adolescence. Available online: http://documents1.worldbank.org/curated/pt/505211566452421860/pdf/Promoting-Girl-s-Nutrition-in-Early-Adolescence-a-last-window-of-opportunity.pdf (accessed on 23 December 2019).
- Arora, G.; Kochar, G.K. Impact of Nutrition Education on Knowledge, Attitude, Practices and Beliefs of Adolescent Girls Belonging to Rural and Urban Area of District Kurukshetra. Int. J. Nutr. Food Sci. 2016, 5, 278–283. [Google Scholar] [CrossRef] [Green Version]
- Camacho-Miñano, M.J.; LaVoi, N.M.; Barr-Anderson, D.J. Interventions to promote physical activity among young and adolescent girls: A systematic review. Health Educ. Res. 2011, 26, 1025–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steiner, G.Z.; Mathersul, D.C.; Macmillan, F.; Camfield, D.A.; Klupp, N.L.; Seto, S.W.; Huang, Y.; Hohenberg, M.I.; Chang, D.H. A Systematic Review of Intervention Studies Examining Nutritional and Herbal Therapies for Mild Cognitive Impairment and Dementia Using Neuroimaging Methods: Study Characteristics and Intervention Efficacy. Evid.-Based Complementary Altern. Med. 2017, 2017, 21. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Altman, D.; Sterne, J. Assessing risk of bias in included studies: Cochrane review. Cochrane Collab. 2011, 5, 1–46. [Google Scholar]
- Reviews, I. The Cochrane Public Health Group Guide for developing a Cochrane protocol. Cochrane Consum. Commun. Gr 2011. [Google Scholar]
- Ryan, R.; Hill, S. How to GRADE the quality of the evidence. Cochrane Consum. Commun. Gr. 2016, 3, 1–24. [Google Scholar]
- Rafiq, M.; Boccia, S. Application of the GRADE Approach in the Development of Guidelines and Recommendations in Genomic Medicine. Cochrane Consum. Commun. Gr 2018. [Google Scholar] [CrossRef] [Green Version]
- Hendrie, G.A.; Brindal, E.; Baird, D.; Gardner, C. Improving children’s dairy food and calcium intake: Can intervention work? A systematic review of the literature. Public Health Nutr. 2013, 16, 365–376. [Google Scholar] [CrossRef] [Green Version]
- Srbely, V.; Janjua, I.; Buchholz, A.C.; Newton, G. Interventions Aimed at Increasing Dairy and/or Calcium Consumption of Preschool-Aged Children: A Systematic Literature Review. Nutrients 2019, 11, 714. [Google Scholar] [CrossRef] [Green Version]
- Abdur Razzak, M.; Mahfuz Al Hasan, S.; Shahinur Rahman, S.; Asaduzzaman, M.; Matin Juliana, F.; Sabir Hossain, M. Role of nutrition education in improving the nutritional status of adolescent girls in North West areas of Bangladesh. Int. J. Sci. Eng. Res. 2016, 7, 1340–1346. [Google Scholar]
- LaChausse, R.G. A clustered randomized controlled trial to determine impacts of the Harvest of the Month program. Health Educ. Res. 2017, 32, 375–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogart, L.M.; Cowgill, B.O.; Elliott, M.N.; Klein, D.J.; Hawes-Dawson, J.; Uyeda, K.; Elijah, J.; Binkle, D.G.; Schuster, M.A. A Randomized Controlled Trial of Students for Nutrition and eXercise: A Community-Based Participatory Research Study. J. Adolesc. Heal. 2014, 55, 415–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Stewart, D.; Chang, C.; Shi, Y. Effect of a school-based nutrition education program on adolescents’ nutrition-related knowledge, attitudes and behaviour in rural areas of China. Environ. Health Prev. Med. 2015, 20, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saraf, D.S.; Gupta, S.K.; Pandav, C.S. Effectiveness of a School Based Intervention for Prevention of Non-communicable Diseases in Middle School Children of Rural North India: A Randomized Controlled Trial. Indian J. Pediatrics 2014, 82, 354–362. [Google Scholar] [CrossRef]
- Laram, C.; Drapeau, V.; Valois, P.; Goulet, C. Evaluation of a Theory-Based Intervention Aimed at Reducing Intention to Use Restrictive Dietary Behaviors Among Adolescent Female Athletes. J. Nutr. Educ. Behav. 2017, 49. [Google Scholar] [CrossRef]
- Shin, A.; Surkan, P.J.; Coutinho, A.J.; Suratkar, S.R.; Campbell, R.K.; Rowan, M.; Sharma, S.; Dennisuk, L.A.; Karlsen, M.; Gass, A.; et al. Impact of Baltimore Healthy Eating Zones: An Environmental Intervention to Improve Diet Among African American Youth. Heal. Educ. Behav. 2015, 42, 97S–105S. [Google Scholar] [CrossRef]
- Jalambo, M.O.; Sharif, R.; Naser, I.A.; Karim, N.A. Improvement in Knowledge, Attitude and Practice of Iron Deficiency Anaemia among Iron-Deficient Female Adolescents after Nutritional Educational Intervention. Glob. J. Health Sci. 2017, 9, 15. [Google Scholar] [CrossRef] [Green Version]
- Jacob, R.; Lamarche, B.; Provencher, V.; Laramée, C.; Valois, P.; Goulet, C.; Drapeau, V. Evaluation of a Theory-Based Intervention Aimed at Improving Coaches’ Recommendations on Sports Nutrition to Their Athletes. J. Acad. Nutr. Diet. 2016, 116, 1308–1315. [Google Scholar] [CrossRef]
- Wang, D.; Stewart, D.; Chang, C. Original Article Is an ecological school-based nutrition intervention effective to improve adolescents’ nutrition-related knowledge, attitudes and behaviour in rural areas of China? Global Health Promot. 2016, 24, 81–89. [Google Scholar] [CrossRef]
- Zhou, W.; Xu, X.; Li, G.; Sharma, M.; Qie, Y.; Zhao, Y. Effectiveness of a school-based nutrition and food safety education program among primary and junior high school students in Chongqing, China. Glob. Health Promot. 2016, 23, 37–49. [Google Scholar] [CrossRef] [Green Version]
- Naghashpour, M.; Shakerinejad, G.; Lourizadeh, M.R. Nutrition Education Based on Health Belief Model Improves Dietary Calcium Intake among Female Students of Junior High Schools. J. Health Popul. Nutr. 2014, 32, 420–429. [Google Scholar] [PubMed]
- Gallotta, M.C.; Iazzoni, S.; Emerenziani, G.P.; Meucci, M.; Migliaccio, S.; Guidetti, L.; Baldari, C. Effects of combined physical education and nutritional programs on schoolchildren’s healthy habits. PeerJ 2016, 11, e1880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kesten, J.M.; Griffiths, P.L.; Cameron, N. A systematic review to determine the effectiveness of interventions designed to prevent overweight and obesity in pre-adolescent girls. Obes. Rev. 2011, 12, 997–1021. [Google Scholar] [CrossRef] [PubMed]
- Salam, R.A.; Hooda, M.; Das, J.K.; Arshad, A.; Lassi, Z.S.; Middleton, P.; Bhutta, Z.A. Interventions to Improve Adolescent Nutrition: A Systematic Review and Meta-Analysis. J. Adolesc. Health 2016, 59, S29–S39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keshani, P.; Kaveh, M.H.; Faghih, S.; Salehi, M. Improving diet quality among adolescents, using health belief model in a collaborative learning context: A randomized field trial study. Health Educ. Res. 2019, 34, 279–288. [Google Scholar] [CrossRef] [Green Version]
- Kropski, J.A.; Keckley, P.H.; Jensen, G.L. School-based Obesity Prevention Programs: An Evidence-based Review. Behav. Psychol. 2008, 16, 1–11. [Google Scholar] [CrossRef]
- Łuszczki, E.; Sobek, G.; Bartosiewicz, A.; Baran, J.; Weres, A.; Dereń, K.; Mazur, A. Analysis of Fruit and Vegetable Consumption by Children in School Canteens Depending on Selected Sociodemographic Factors. Medicina 2019, 55, 397. [Google Scholar] [CrossRef] [Green Version]
- Kupolati, M.D.; Macintyre, U.E.; Gericke, G.J. A Theory-Based Contextual Nutrition Education Manual Enhanced Nutrition Teaching Skill. Front. Public Health 2018, 6, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Wan, T.T.H.; Rav-Marathe, K.; Marathe, S. A Systematic Review on the KAP-O Framework for Diabetes Education and Research. Med. Res. Arch. 2016, 4, 1–21. [Google Scholar]
- Rabiu, A.; Simbak, N.B.; Haque, M.A. Systematic Review of Knowledge, Attitude and Practice on Adverse Drug Reactions and Pharmacovigilance among Doctors. J. Appl. Pharm. Sci. 2014, 4, 117–127. [Google Scholar]
- Barzkar, F.; Baradaran, H.R.; Koohpayehzadeh, J. Knowledge, Attitude, And Practice Of Evidence-Based Medicine Among Physicians: A Systematic Review. Biomed. J. 2017, 7, 32–33. [Google Scholar]
- Xu, T.; Tomokawa, S.; Gregorio, E.R., Jr.; Mannava, P.; Nagai, M.; Sobel, H. School-based interventions to promote adolescent health: A systematic review in low- and middle-income countries of WHO Western Pacific Region. PLoS ONE 2020, 15, e0230046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaushal, P.; Singh, T.; Padda, A.S.; Deepti, S.S. Effectiveness of a health education intervention on the knowledge, attitude and practices of teachers regarding physical and psychosocial health of adolescents in Amritsar, Punjab. Int. J. Community Med. Public Health 2018, 5, 4921–4926. [Google Scholar] [CrossRef]
- Elsayed, E.; Elsabagh, M. Effect of Health Education Intervention on Knowledge and Practice about reproductive health among Adolescent Female Students. J. Med. Sci. Clin. Res. 2017, 05, 21663–21678. [Google Scholar]
- Midzi, N.; Mtapuri, S.; Mutsaka, M.J.; Ruhanya, V.; Magwenzi, M.; Chin, N.; Nyandoro, G.; Marume, A.; Kumar, N.; Mduluza, T. Impact of School Based Health Education on Knowledge, Attitude and Practice of Grade Three Primary School Children in Zimbabwe. J. Community Med. Health Educ. 2014, 4, 1–8. [Google Scholar] [CrossRef]
- Adolescent Nutrition: Policy and programming in SUN+ countries. Available online: https://resourcecentre.savethechildren.net/node/8970/pdf/adolescent_nutrition.pdf (accessed on 29 September 2018).
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Lassi, Z.S.; Moin, A.; Das, J.K.; Salam, R.A.; Bhutta, Z.A. Systematic review on evidence-based adolescent nutrition interventions. Ann. N. Y. Acad. Sci. 2017, 1393, 34–50. [Google Scholar] [CrossRef] [Green Version]
- Maaloul, J.; Harrabi, I.; Delpierre, C.; Gaha, R.; Ghannem, H. Predictors of food and physical activity patterns among schoolchildren in the region of Sousse, Tunisia. Obes. Res. Clin. Pract. 2013, 7, e407–e413. [Google Scholar]
- Brito, K.; Fiaccone, R.L.; Couto, R.D.; Ribeiro-silva, R.D.C. Evaluation of the effects of a programme promoting adequate and healthy eating on adolescent health markers: An interventional study. Nutr. Hosp. 2015, 32, 1582–1590. [Google Scholar]
- Zota, D.; Dalma, A.; Petralias, A.; Lykou, A.; Kastorini, C.M.; Yannakoulia, M.; Karnaki, P.; Belogianni, K.; Veloudaki, A.; Riza, E.; et al. Promotion of healthy nutrition among students participating in a school food aid program: A randomized trial. Int. J. Public Health. 2016, 61, 583–592. [Google Scholar] [CrossRef]
- Mccabe, B.E.; Plotnikoff, R.C.; Dewar, D.L.; Collins, C.E.; Lubans, D.R. Social Cognitive Mediators of Dietary Behavior Change in Adolescent Girls. Am. J. Health Behav. 2015, 39, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Alaimo, K.; Oleksyk, S.C.; Drzal, N.B.; Golzynski, D.L.; Lucarelli, J.F.; Wen, Y.; Velie, E.M. Effects of Changes in Lunch-Time Competitive Foods, Nutrition Practices, and Nutrition Policies on Low-Income Middle-School Children’s Diets. Child. Obes. 2013, 9, 509–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth-Cline, M.; Nelson, R.M. Parental permission and child assent in research on children. Yale J. Biol. Med. 2013, 86, 291–301. [Google Scholar] [PubMed]


{kind=link}
| Author, Year, Country, Study Design | Settings/Duration/Frequency of Intervention | Target Population/Theory | Description of the Intervention (I: Intervention, C: Control) | Outcome Assessed, Significance | Effect Size 2 | Effective (Y/N) 1 |
|---|---|---|---|---|---|---|
| Abdur Razzak et al., 2016 [34] Bangladesh, RCT 3. | Community-based/ 2 years/NM | 10 to 19 years old girls (n = 250) No theory | I: Nutrition education was communicated through group or personal discussion (malnutrition, dietary diversity, food taboos, hygiene and sanitation) to adolescent girls using charts, leaflets, posters. | Knowledge (p < 0.001) Attitude (p < 0.05) Practice (p < 0.05) Anthropometric (p < 0.05) Reported pre and post-test intervention changes in nutritional status. | ND | Y |
| C: No action was provided to control group | ||||||
| Lachausse, 2017 [35] USA, CRCT 4 | School-based (after school program)/ 3 months/Monthly | Grade 4 to 6 boys and girls, (n = 275) No theory | I: Harvest of the month (HOTM) nutrition education program on fruits and vegetables consumption, and physical activities including fruits and vegetable tasting, students work book, nutritional information presentations, story books, farm to school presentation, HOTM newsletter for parents, menu slicks, and cafeteria posters | Knowledge (p > 0.05) Self-efficacy (p > 0.05) Reported pre and post-test on fruit and vegetable consumption, knowledge, and self-efficacy on fruit and vegetable consumption | ND | N |
| C: Normal after school activity (homework tutorial, arts and crafts) as assigned by their after school teacher. | ||||||
| Bogart et al., 2014 [36], USA, RCT 3 | School-based/ 5 weeks/daily | Grade 7 boys and girls, (n = 4022) Diffusion of innovation theory | I: Students for Nutrition and eXercise intervention (SNaX), including school food environment changes, peer leader club and social marketing (cafeteria food taste test, nutritional messages, and educational book marks) | Knowledge (p < 0.01) Attitude (p < 0.05) Intention (p < 0.05) Reported pre-test and post-test on cafeteria food tasting, knowledge on healthy eating/physical activity, and intention | ND | Y |
| C: No action was provided to control group | ||||||
| Wang et al., 2015 [37], China, CRCT 4 | School-based/ 6 months/weekly | Grade 7 to 9 boys and girls, (n = 130) No theory | I: Nutrition education intervention including in-class nutrition curriculum, peer support activities and the distribution of brochures using mass media, television (TV) messages, information leaflets. | Knowledge (p < 0.05) Attitude (p < 0.05) Healthy eating behaviour (p < 0.05) Reported pre-test and post-test on knowledge, attitude and healthy eating behaviour | ND | Y |
| C: No action was provided to control group | ||||||
| Saraf et al., 2014 [38], India, CRCT 4 | School-based/ 8 months/NM | Grade 6 and 7 girls (n = 2279) No theory | I: Health education on diet, physical activities and tobacco through school component, class room component and family/community component using health education lectures, flash films, peer group discussion, flip charts, physical training (PT) classes | Knowledge (p < 0.01) Behavioural practice on physical activity, diet and tobacco (p < 0.01) Reported pre-test and post-test for knowledge and behavioural practices | 39% | Y |
| C: No action was provided to control group | ||||||
| Laram et al., 2017 [39], Canada, CRCT 4 | Community-based/ 3 weeks/Weekly | 12 to 17 years old girls, (n = 89) Theory of planned behaviour (TPB) | I: Nutrition education on healthy eating and sport nutrition through persuasive communication, active learning, observational modelling, using lectures, brainstorming, and discussion | Knowledge (p < 0.001) Attitude (p < 0.001) Subjective norm (p < 0.01) Intention (p > 0.05) Perceived behavioural control (P > 0.05) | ND | Y |
| C: No action was provided to control group | ||||||
| Shin et al., 2015 [40], USA, CRCT 4 | Recreation centre/ 8 months/daily | 10 to 14 years’ boys and girls, (n = 152) No theory | I: Nutrition education: The Baltimore Healthy Eating Zones (BHEZ) intervention in recreation centres (corner stores/carryout restaurants and food outlets), with a focus on healthy eating, beverages, breakfast, snacks, and cooking at home through activities such as lectures, taste tests, cooking demonstrations, shelf labels, point of purchase, posters and flyers | Knowledge (p < 0.001) Behavioural intention (healthy food purchase, beverages, snacks, and food preparation) (p = 0.01) Outcome expectancy (p = 0.02) Self-efficacy (p = 0.54) BMI (p < 0.04) | ND | Y |
| C: No action was provided to control group | ||||||
| Jalambo et al., 2017 [41], Palestine, RCT 3 | School-based/ 3 months/weekly | 15 to 19 years old girls, (n = 89) No theory | I: Nutrition education on food groups, food pyramid, balanced food, iron absorption enhancers and inhibitors, sources of iron, anaemia and iron deficiency using lectures, wall writing, videos, booklets and brochures | Knowledge (p < 0.001) Attitude (p < 0.001) Nutrition practice (p < = 0.002) | ND | Y |
| C: No action was provided to control group |
| Study (n = 9) | 1 Duration | 2 Frequency of Contact | 3 Level of Personalization | 4 Reach of the Intervention | Overall Intensity Score | 5 Overall Intensity Rating | 6 Effective |
|---|---|---|---|---|---|---|---|
| Abdur Razzak et al., 2016 [34] Bangladesh. | 5 | 7 NM | 2 | 1 | 8 | Low | Y |
| Lachausse, 2017 [35] USA. | 3 | 3 | 2 | 1 | 9 | Low | N |
| Bogart et al., 2014 [36] USA. | 1 | 5 | 3 | 3 | 12 | Medium | Y |
| Wang et al., 2015 [37] China. | 4 | 4 | 3 | 1 | 12 | Medium | Y |
| Saraf et al., 2014 [38] India. | 4 | NM | 5 | 5 | 14 | High | Y |
| Laram et al., 2017 [39] Canada. | 1 | 4 | 2 | 1 | 8 | Low | Y |
| Shin et al., 2015 [40] USA. | 4 | 5 | 4 | 3 | 16 | High | Y |
| Jalambo et al., 2017 [41] Palestine. | 3 | 4 | 2 | 1 | 10 | Low | Y |
| Study | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Item 10 | Item 11 | Item 12 | Total n (%) | Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abdur Razzak et al. (2016) [34] | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 4 (33%) | High |
| Lachausse (2017) [35] | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 7 (58%) | Low |
| Bogart et al. (2014) [36] | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 5 (42%) | High |
| Wang et al. (2015) [37] | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 4 (33%) | High |
| Saraf et al. (2014) [38] | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 7 (58%) | Low |
| Laram et al. (2017) [39] | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 8 (67%) | Low |
| Shin et al. (2015) [40] | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 4 (33%) | High |
| Jalambo et al. (2017) [41] | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 5 (42%) | High |
| Study | Type of Evidence | Quality Point | Consistency | Directness | Effect Size | Quality of Evidence |
|---|---|---|---|---|---|---|
| Abdur Razzak et al. (2016) [34] | 4 | 2 | 3 | 3 | 0 | Low |
| Lachausse (2017) [35] | 4 | 3 | 3 | 3 | 0 | Moderate |
| Bogart et al. (2014) [36] | 4 | 3 | 3 | 4 | 0 | Moderate |
| Wang et al. (2015) [37] | 4 | 1 | 3 | 3 | 0 | Low |
| Saraf et al. (2014) [38] | 4 | 3 | 4 | 4 | 3 | High |
| Laram et al. (2017) [39] | 4 | 3 | 3 | 3 | 0 | Moderate |
| Shin et al. (2015) [40] | 4 | 2 | 3 | 3 | 0 | Low |
| Jalambo et al. (2017) [41] | 4 | 1 | 3 | 3 | 0 | Low |
| Overall Quality | High | Low | Moderate | Moderate | Very low | Moderate |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charles Shapu, R.; Ismail, S.; Ahmad, N.; Lim, P.Y.; Abubakar Njodi, I. Systematic Review: Effect of Health Education Intervention on Improving Knowledge, Attitudes and Practices of Adolescents on Malnutrition. Nutrients 2020, 12, 2426. https://doi.org/10.3390/nu12082426
Charles Shapu R, Ismail S, Ahmad N, Lim PY, Abubakar Njodi I. Systematic Review: Effect of Health Education Intervention on Improving Knowledge, Attitudes and Practices of Adolescents on Malnutrition. Nutrients. 2020; 12(8):2426. https://doi.org/10.3390/nu12082426
Chicago/Turabian StyleCharles Shapu, Ruth, Suriani Ismail, Norliza Ahmad, Poh Ying Lim, and Ibrahim Abubakar Njodi. 2020. "Systematic Review: Effect of Health Education Intervention on Improving Knowledge, Attitudes and Practices of Adolescents on Malnutrition" Nutrients 12, no. 8: 2426. https://doi.org/10.3390/nu12082426