Anthropometric, Familial- and Lifestyle-Related Characteristics of School Children Skipping Breakfast in Jeddah, Saudi Arabia


Abstract
:1. Introduction
2. Materials and Methods
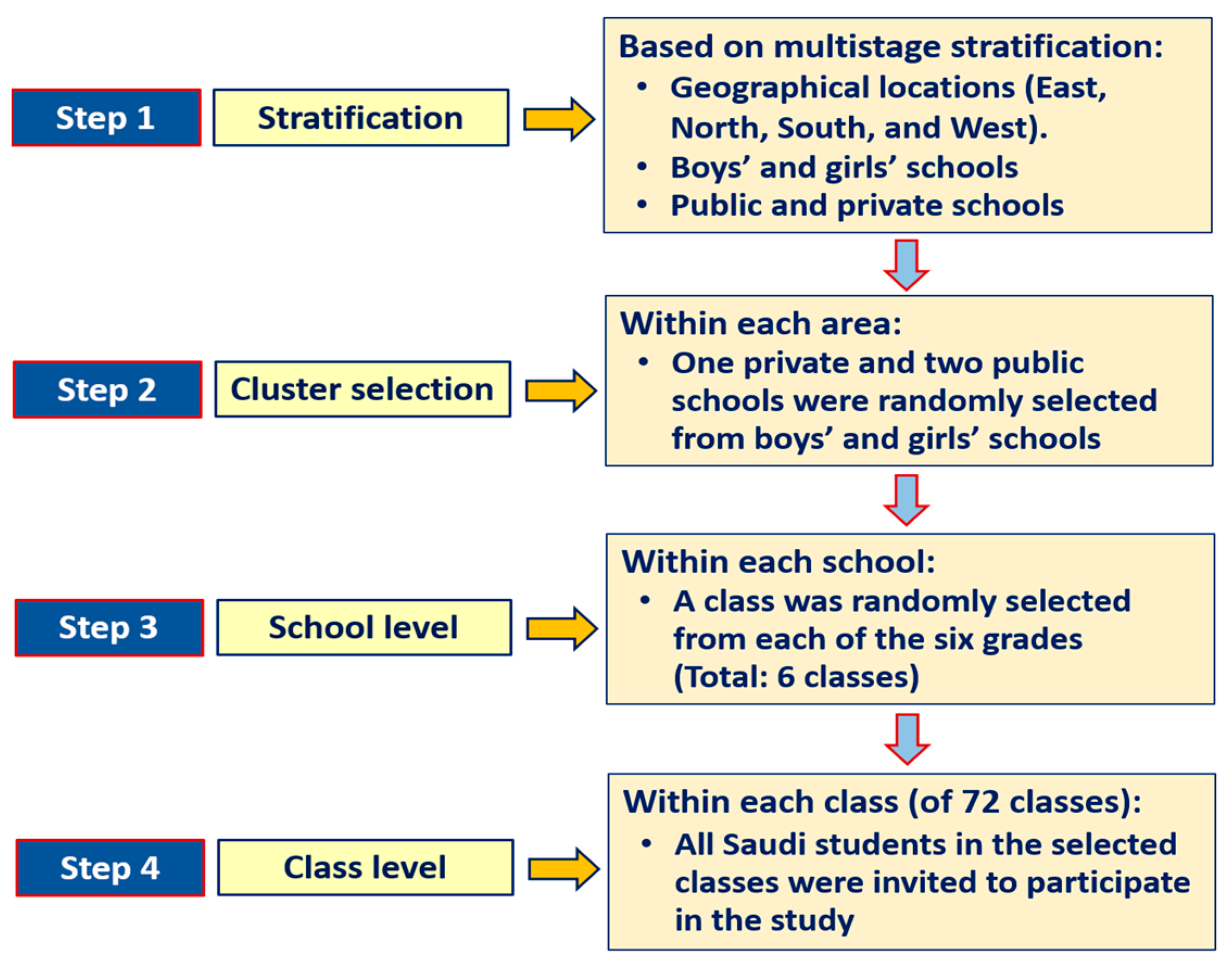
2.1. Study Design and Sample Selection
2.2. Anthropometric Measurement
2.3. Assessment of Breakfast Eating Habits
2.4. Assessment of Screen Time, Sleep, and Physical Activity
2.5. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Caprio, S.; Santoro, N.; Weiss, R. Childhood obesity and the associated rise in cardiometabolic complications. Nat. Metab. 2020, 2, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, M.; Llewellyn, A.; Owen, C.; Woolacott, N. Predicting adult obesity from childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2015, 17, 95–107. [Google Scholar]
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar]
- Al-Hussaini, A.A.; Bashir, M.S.; Khormi, M.; Alturaiki, M.; Alkhamis, W.; Alrajhi, M.; Halal, T. Overweight and obesity among Saudi children and adolescents: Where do we stand today? Saudi J. Gastroenterol. 2019, 25, 229–235. [Google Scholar] [PubMed]
- Wen, L.M.; Rissel, C.; He, G. The effect of early life factors and early interventions on childhood overweight and obesity 2016. J. Obes. 2017, 2017, 3642818. [Google Scholar] [CrossRef]
- Fang, J.; Gong, C.; Wan, Y.; Xu, Y.; Tao, F.; Sun, Y. Polygenic risk, adherence to a healthy lifestyle, and childhood obesity. Pediatr. Obes. 2019, 14, e12489. [Google Scholar] [CrossRef]
- Blondin, S.; Anzman-Frasca, S.; Djang, H.; Economos, C. Breakfast consumption and adiposity among children and adolescents: An updated review of the literature. Pediatr. Obes. 2016, 11, 333–348. [Google Scholar]
- Affenito, S.G.; Thompson, D.R.; Barton, B.A.; Franko, D.L.; Daniels, S.R.; Obarzanek, E.; Schreiber, G.B.; Striegel-Moore, R.H. Breakfast consumption by African-American and white adolescent girls correlates positively with calcium and fiber intake and negatively with body mass index. J. Am. Diet. Assoc. 2005, 105, 938–945. [Google Scholar]
- Dubois, L.; Girard, M.; Potvin, K.M. Breakfast eating and overweight in a preschool population: Is there a link? Public Health Nutr. 2006, 9, 436–442. [Google Scholar]
- Horikawa, C.; Kodama, S.; Yachi, Y.; Heianza, Y.; Hirasawa, R.; Ibe, Y.; Saito, K.; Shimano, H.; Yamada, N.; Sone, H.; et al. Skipping breakfast and prevalence of overweight and obesity in Asian and Pacific regions: A meta-analysis. Prev. Med. 2011, 53, 260–267. [Google Scholar] [PubMed]
- Kyriazis, I.; Rekleiti, M.; Saridi, M.; Beliotis, E.; Toska, A.; Souliotis, K.; Wozniak, G. Prevalence of obesity in children aged 6–12 years in Greece: Nutritional behaviour and physical activity. Arch. Med. Sci. 2012, 8, 859–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timlin, M.T.; Pereira, M.A.; Story, M.; Neumark-Sztainer, D. Breakfast eating and weight change in a 5-year prospective analysis of adolescents: Project EAT (Eating Among Teens). Pediatrics 2008, 121, e638–e645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaguchi-Tanaka, Y.; Tabuchi, T. Skipping breakfast and subsequent overweight/obesity in children: A nationwide prospective study of 2.5 to 13-year olds in Japan. J. Epidemiol. 2020. ahead of print. [Google Scholar] [CrossRef]
- Sila, S.; Ilić, A.; Mišigoj-Duraković, M.; Sorić, M.; Radman, I.; Šatalić, Z. Obesity in adolescents who skip breakfast is not associated with physical activity. Nutrients 2019, 11, 2511. [Google Scholar] [CrossRef] [Green Version]
- Al Turki, M.; Al Shloi, S.; Al Harbi, A.; Al Agil, A.; Philip, W.; Qureshi, S. Breakfast consumption habits among schoolchildren: A cross-sectional study in Riyadh, Saudi Arabia. Int. Res. J. Med. Med. Sci. 2018, 6, 50–55. [Google Scholar]
- Al-Hazzaa, H.M.; Alhowikan, A.M.; Alhussain, M.H.; Obeid, O.A. Breakfast consumption among Saudi primary-school children relative to sex and socio-demographic factors. BMC Public Health 2020, 20, 448. [Google Scholar] [CrossRef] [Green Version]
- Monzani, A.; Ricotti, R.; Caputo, M.; Solito, A.; Archero, F.; Bellone, S.; Prodam, F. A systematic review of the association of skipping breakfast with weight and cardiometabolic risk factors in children and adolescents. What should we better investigate in the future? Nutrients 2019, 11, 387. [Google Scholar] [CrossRef] [Green Version]
- Adolphus, K.; Lawton, C.L.; Dye, L. The effects of breakfast on behavior and academic performance in children and adolescents. Front. Hum. Neurosci. 2013, 7, 425. [Google Scholar]
- Rampersaud, G.C.; Pereira, M.A.; Girard, B.L.; Adams, J.; Metzl, J.D. Breakfast habits, nutritional status, body weight, and academic performance in children and adolescents. J. Am. Diet. Assoc. 2005, 105, 743–760. [Google Scholar] [PubMed]
- Widenhorn-Müller, K.; Hille, K.; Klenk, J.; Weiland, U. Influence of having breakfast on cognitive performance and mood in 13-to 20-year-old high school students: Results of a crossover trial. Pediatrics 2008, 122, 279–284. [Google Scholar]
- Mielgo-Ayuso, J.; Valtueña, J.; Cuenca-García, M.; Gottrand, F.; Breidenassel, C.; Ferrari, M.; Manios, Y.; De Henauw, S.; Widhalm, K.; Kafatos, A.; et al. Regular breakfast consumption is associated with higher blood vitamin status in adolescents: The HELENA (healthy lifestyle in Europe by nutrition in adolescence) study. Public Health Nutr. 2017, 20, 1393–1404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramsay, S.A.; Bloch, T.D.; Marriage, B.; Shriver, L.H.; Spees, C.K.; Taylor, C.A. Skipping breakfast is associated with lower diet quality in young US children. Eur. J. Clin. Nutr. 2018, 72, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Mounayar, R.; Jreij, R.; Hachem, J.; Abboud, F.; Tueni, M. Breakfast intake and factors associated with adherence to the Mediterranean diet among Lebanese high school adolescents. J. Nutr. Metab. 2019, 2019, 2714286. [Google Scholar] [CrossRef] [PubMed]
- Al-Hazzaa, H.M.; Alhussain, M.H.; Alhowikan, A.M.; Obeid, O.A. Insufficient sleep duration and its association with breakfast intake, overweight/obesity, socio-demographics and selected lifestyle behaviors among Saudi school children. Nat. Sci. Sleep 2019, 11, 253–263. [Google Scholar] [CrossRef] [Green Version]
- Vereecken, C.; The HBSC Eating & Dieting Focus Group; Dupuy, M.; Rasmussen, M.; Kelly, C.; Nansel, T.R.; Al Sabbah, H.; Baldassari, D.; Jordan, M.D.; Maes, L.; et al. Breakfast consumption and its socio-demographic and lifestyle correlates in schoolchildren in 41 countries participating in the HBSC study. Int. J. Public Health 2009, 54 (Suppl. 2), 180–190. [Google Scholar] [CrossRef] [Green Version]
- Al-Othaimeen, A.; Osman, A.K.; Al Orf, S. Prevalence of nutritional anaemia among primary school girls in Riyadh City, Saudi Arabia. Int. J. Food Sci. Nutr. 1999, 50, 237–243. [Google Scholar] [CrossRef]
- Abalkhail, B.; Shawky, S. Prevalence of daily breakfast intake, iron deficiency anaemia and awareness of being anaemic among Saudi school students. Int. J. Food Sci. Nutr. 2002, 53, 519–528. [Google Scholar] [CrossRef]
- AL-Oboudi, L.M. Impact of breakfast eating pattern on nutritional status, glucose level, iron status in blood and test grades among upper primary school girls in Riyadh city, Saudi Arabia. Pakistan J. Nutr. 2010, 9, 106–111. Available online: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.624.9904&rep=rep1&type=pdf (accessed on 25 May 2020). [CrossRef] [Green Version]
- Cole, T.J.; Lobstein, T. Extended International (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. Committee on Public Education. American academy of pediatrics: Children, adolescents, and television. Pediatrics 2001, 107, 423–426. [Google Scholar] [CrossRef] [Green Version]
- Canadian Society for Exercise Physiology. Canadian 24-Hour Movement Guidelines for Children and Youth (Ages 5–17 Years). 2020. Available online: https://csepguidelines.ca/children-and-youth-5-17/ (accessed on 15 October 2020).
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Warburton, D.E.; Janssen, I.; Paterson, D.H.; Latimer, A.E.; Rhodes, R.E.; Kho, M.E.; Hicks, A.; Leblanc, A.G.; Zehr, L.; et al. New Canadian physical activity guidelines. Appl. Physiol. Nutr. Metab. 2011, 36, 47–58. [Google Scholar] [CrossRef]
- Farghaly, N.F.; Ghazali, B.M.; Al-Wabel, H.M.; Sadek, A.A.; Abbag, F.I. Life style and nutrition and their impact on health of Saudi school students in Abha, Southwestern region of Saudi Arabia. Saudi Med. J. 2007, 28, 415–421. [Google Scholar] [PubMed]
- Alenazi, S.A.; Ali, H.W.; Alshammary, O.M.; Alenazi, M.S.; Wazir, F. Effect of breakfast on body mass index (BMI) in male children in northern border region Saudi Arabia. Khyber Med. Univ. J. 2014, 6, 106–109. [Google Scholar]
- Smith, K.J.; Breslin, M.C.; McNaughton, S.A.; Gall, S.L.; Blizzard, L.; Venn, A.J. Skipping breakfast among Australian children and adolescents; findings from the 2011–2012 National Nutrition and Physical Activity Survey. Aust. N. Z. J. Public Health 2017, 41, 572–578. [Google Scholar] [CrossRef]
- Manios, Y.; Moschonis, G.; Androutsos, O.; Filippou, C.; Van Lippevelde, W.; Vik, F.N.; Velde, S.J.T.; Jan, N.; Dössegger, A.; Bere, E.; et al. Family sociodemographic characteristics as correlates of children’s breakfast habits and weight status in eight European countries. The ENERGY (EuropeaN Energy balance research to prevent excessive weight gain among youth) project. Public Health Nutr. 2015, 18, 774–783. [Google Scholar] [CrossRef] [Green Version]
- Tambalis, K.D.; Panagiotakos, D.B.; Psarra, G.; Sidossis, L.S. Breakfast skipping in Greek schoolchildren connected to an unhealthy lifestyle profile. Results from the National Action for Children’s Health program. Nutr. Diet 2019, 76, 328–335. [Google Scholar] [CrossRef]
- Sirichakwal, P.P.; Janesiripanich, N.; Kunapun, P.; Senaprom, S.; Purttipornthanee, S. Breakfast consumption behaviors of elementary school children in Bangkok metropolitan region. Southeast Asian J. Trop. Med. Public Health 2015, 46, 939–948. [Google Scholar]
- Al-Hazzaa, H.M.; Abahussain, N.; Al-Sobayel, H.; Qahwaji, D.; Musaiger, A.O. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 140. [Google Scholar] [CrossRef] [Green Version]
- Albataineh, S.R.; Badran, E.F.; Tayyem, R.F. Dietary factors and their association with childhood obesity in the Middle East: A systematic review. Nutr. Health 2019, 25, 53–60. [Google Scholar] [CrossRef]
- Champilomati, G.; Notara, V.; Prapas, C.; Konstantinou, E.; Kordoni, M.; Velentza, A.; Mesimeri, M.; Antonogeorgos, G.; Rojas-Gil, A.P.; Kornilaki, E.N.; et al. Breakfast consumption and obesity among preadolescents: An epidemiological study. Pediatr. Int. 2020, 62, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardeshirlarijani, E.; Namazi, N.; Jabbari, M.; Zeinali, M.; Gerami, H.; Jalili, R.B.; Larijani, B.; Azadbakht, L. The link between breakfast skipping and overweigh/obesity in children and adolescents: A meta-analysis of observational studies. J. Diabetes Metab. Disord. 2019, 18, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.W.; Brown, M.M.; Allison, D.B. Belief beyond the evidence: Using the proposed effect of breakfast on obesity to show 2 practices that distort scientific evidence. Am. J. Clin. Nutr. 2013, 98, 1298–1308. [Google Scholar] [CrossRef] [PubMed]
- Albertson, A.M.; Affenito, S.G.; Bauserman, R.; Holschuh, N.M.; Eldridge, A.L.; Barton, B.A. The relationship of ready-to-eat cereal consumption to nutrient intake, blood lipids, and body mass index of children as they age through adolescence. J. Am. Diet. Assoc. 2009, 109, 1557–1565. [Google Scholar] [CrossRef]
- Van den Boom, A.; Serra-Majem, L.; Ribas, L.; Ngo, J.; Pérez-Rodrigo, C.; Aranceta, J.; Fletcher, R. The contribution of ready-to-eat cereals to daily nutrient intake and breakfast quality in a Mediterranean setting. J. Am. Coll. Nutr. 2006, 25, 135–143. [Google Scholar] [CrossRef]
- Williams, P.G. The benefits of breakfast cereal consumption: A systematic review of the evidence base. Adv. Nutr. 2014, 5, 636S–673S. [Google Scholar] [CrossRef]
- Vatanparast, H.; Islam, N.; Patil, R.P.; Shamloo, A.; Keshavarz, P.; Smith, J.; Chu, L.M.; Whiting, S. Consumption of Ready-to-Eat Cereal in Canada and its contribution to nutrient intake and nutrient density among Canadians. Nutrients 2019, 11, 1009. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, T.P.; Meilstrup, C.; Holstein, B.E.; Rasmussen, M. Fruit and vegetable intake is associated with frequency of breakfast, lunch and evening meal: Cross-sectional study of 11-, 13-, and 15-year-olds. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 9. [Google Scholar] [CrossRef] [Green Version]
- Pourrostami, K.; Heshmat, R.; Hemati, Z.; Heidari-Beni, M.; Qorbani, M.; Motlagh, M.E.; Raeisi, A.; Shafiee, G.; Ziaodini, H.; Beshtar, S.; et al. Association of fruit and vegetable intake with meal skipping in children and adolescents: The CASPIAN-V study. Eat. Weight Disord. 2019, 25, 903–910. [Google Scholar] [CrossRef]
- Levin, K.; Kirby, J.; Currie, C. Family structure and breakfast consumption of 11–15 year old boys and girls in Scotland, 1994–2010: A repeated cross-sectional study. BMC Public Health 2012, 12, 228. [Google Scholar] [CrossRef] [Green Version]
- Johansen, A.; Rasmussen, S.; Madsen, M. Health behaviour among adolescents in Denmark: Influence of school class and individual risk factors. Scand. J. Public Health 2006, 34, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Keski-Rahkonen, A.; Kaprio, J.; Rissanen, A.; Virkkunen, M.; Rose, R.J. Breakfast skipping and health-compromising behaviors in adolescents and adults. Eur. J. Clin. Nutr. 2003, 57, 842–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearson, N.; Biddle, S.J.; Gorely, T. Family correlates of breakfast consumption among children and adolescents. A systematic review. Appetite 2009, 52, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Utter, J.; Scragg, R.; Mhurchu, C.N.; Schaaf, D. At-home breakfast consumption among New Zealand children: Associations with body mass index and related nutrition behaviors. J. Am. Diet. Assoc. 2007, 107, 570–576. [Google Scholar] [CrossRef]
- Zakrzewski-Fruer, J.K.; Gillison, F.B.; Katzmarzyk, P.T.; Mire, E.F.; Broyles, S.T.; Champagne, C.M.; Chaput, J.-P.; Denstel, K.D.; Fogelholm, M.; Gang, H.; et al. Association between breakfast frequency and physical activity and sedentary time: A cross-sectional study in children from 12 countries. BMC Public Health 2019, 19, 222. [Google Scholar] [CrossRef] [Green Version]
- Al-Hazzaa, H.M.; Al-Sobayel, H.I.; Abahussain, N.A.; Qahwaji, D.M.; Alahmadi, M.A.; Musaiger, A.O. Association of dietary habits with levels of physical activity and screen time among adolescents living in Saudi Arabia. J. Hum. Nutr. Diet. 2014, 27 (Suppl. 2), 204–213. [Google Scholar] [CrossRef]
- Chen, M.-Y.; Wang, E.K.; Jeng, Y.-J. Adequate sleep among adolescents is positively associated with health status and health-related behaviors. BMC Public Health 2006, 6, 59. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Musaiger, A.O.; Abahussain, N.A.; Al-Sobayel, H.I.; Qahwaji, D.M. Lifestyle correlates of self-reported sleep duration among Saudi adolescents: A multicentre school-based cross-sectional study. Child. Care Health Dev. 2014, 40, 533–542. [Google Scholar] [CrossRef]
- Agostini, A.; Lushington, K.; Kohler, M.; Dorrian, J. Associations between self-reported sleep measures and dietary behaviours in a large sample of Australian school students (n = 28,010). J. Sleep Res. 2018, 27, e12682. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, H.; Taira, K.; Arakawa, M.; Masuda, A.; Yamamoto, Y.; Komoda, Y.; Kadegaru, H.; Shirakawa, S. An examination of sleep health, lifestyle and mental health in junior high school students. Psychiatry Clin. Neurosci. 2002, 56, 235–236. [Google Scholar] [CrossRef]
- Adolphus, K.; Bellissimo, N.; Lawton, C.L.; Ford, N.A.; Rains, T.M.; de Zepetnek, J.T.; Dye, L. Methodological challenges in studies examining the effects of breakfast on cognitive performance and appetite in children and adolescents. Adv. Nutr. 2017, 8, 184S–196S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Neil, C.E.; Byrd-Bredbenner, C.; Hayes, D.; Jana, L.; Klinger, S.E.; Stephenson-Martin, S. The role of breakfast in health: Definition and criteria for a quality breakfast. J. Acad. Nutr. Diet. 2014, 114 (Suppl. 12), S8–S26. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | All (N = 1149) | Boys (N = 523) | Girls (N = 626) | p-Value * |
|---|---|---|---|---|
| Age (year) | 9.3 ± 1.7 | 9.3 ± 1.6 | 9.4 ± 1.7 | 0.365 |
| Body weight (kg) | 32.8 ± 11.3 | 32.4 ± 11.1 | 33.2 ± 11.5 | 0.246 |
| Body height (cm) | 133.2 ± 11.4 | 133.3 ± 10.5 | 133.0 ± 12.1 | 0.608 |
| Body mass index (kg/m2) | 18.1 ± 3.9 | 17.8 ± 4.0 | 18.3 ± 3.9 | 0.055 |
| Breakfast intake (days/week) | 3.76 ± 2.3 | 3.75 ± 2.3 | 3.76 ± 2.2 | 0.778 |
| BMI category (%) | 0.093 | |||
| Underweight | 15.4 | 17.9 | 13.3 | |
| Normal weight | 55.9 | 54.7 | 56.9 | |
| Overweight | 19.4 | 17.5 | 21.1 | |
| Obesity | 9.3 | 10.0 | 8.8 | |
| Overweight + obesity | 28.7 | 27.5 | 29.8 |
| Variable | Criterion * | Proportion (%) | p-Value ** | ||
|---|---|---|---|---|---|
| All (N =1149) | Boys (N = 523) | Girls (N = 626) | |||
| Breakfast intake at home | Non-daily intake | 79.6 | 78.8 | 80.4 | 0.509 |
| Overweight or obesity | BMI > cut-offs | 28.7 | 27.5 | 29.8 | 0.378 |
| Screen time | >2 h/day | 69.5 | 77.8 | 62.6 | <0.001 |
| Nocturnal sleep duration | <9 h | 65.8 | 67.5 | 64.4 | 0.267 |
| Physical activity | <420 min/week | 84.8 | 74.8 | 93.1 | <0.001 |
| Walking to school | Not walking to school | 95.7 | 95.0 | 96.3 | 00.005 |
| Variable | <5 Days/Week (N = 685) | 5 + Days/Week (N = 464) | p-Value * |
|---|---|---|---|
| Breakfast intake (day per week) | 2.1 ± 1.1 | 6.3 ± 0.83 | |
| Gender (%) | 0.923 | ||
| Boys | 45.4 | 45.7 | |
| Girls | 54.6 | 54.3 | |
| School type (%) | 0.490 | ||
| Public | 76.4 | 74.6 | |
| Private | 23.6 | 25.4 | |
| Parent answering the questionnaire (%) | 0.099 | ||
| Father | 38.5 | 33.4 | |
| Mother | 58.1 | 64.2 | |
| Someone else | 3.4 | 2.4 | |
| Number of children in the family (%) | 0.019 | ||
| 1–2 | 14.2 | 18.3 | |
| 3–4 | 49.9 | 53.0 | |
| 5+ | 35.9 | 28.7 | |
| Number of family members in the house (%) | 0.272 | ||
| 1–3 | 45.7 | 50.0 | |
| 4–5 | 50.9 | 47.6 | |
| 6+ | 3.4 | 2.4 | |
| Paternal age (%) | 0.019 | ||
| <30 years | 0.7 | 0.4 | |
| 30-39 years | 28.8 | 32.5 | |
| 40–49 years | 47.2 | 51.3 | |
| 50–59 years | 19.0 | 13.4 | |
| 60+ years | 3.4 | 2.4 | |
| Maternal age (%) | 0.057 | ||
| <30 years | 8.2 | 9.1 | |
| 30–39 years | 60.3 | 64.4 | |
| 40–49 years | 27.2 | 24.8 | |
| 50–59 years | 4.4 | 1.7 | |
| 60+ years | 0.00 | 0.00 | |
| Paternal education (%) | 0.001 | ||
| Intermediate or less | 15.2 | 9.3 | |
| High school | 30.8 | 25.4 | |
| University degree | 46.1 | 54.3 | |
| Post graduate degree | 7.9 | 11.0 | |
| Maternal education (%) | <0.001 | ||
| Intermediate or less | 14.0 | 6.9 | |
| High school | 30.2 | 28.2 | |
| University degree | 52.3 | 59.5 | |
| Post graduate degree | 3.5 | 5.4 | |
| Family income (%) ** | 0.146 | ||
| 10,000 SR or less | 45.8 | 42.5 | |
| 10,001–20,000 SR | 37.8 | 41.2 | |
| 20,001–30,000 SR | 11.2 | 13.4 | |
| 30,001 + SR | 5.1 | 3.0 | |
| Screen time | 0.728 | ||
| ≤2 h/day | 30.1 | 31.0 | |
| >2 h/day | 69.9 | 69.0 | |
| Sleep duration | 0.001 | ||
| <9 h/night | 69.5 | 60.3 | |
| ≥9 h/night | 30.5 | 39.7 | |
| Physical activity (%) | 0.840 | ||
| No physical activity | 53.1 | 50.9 | |
| Less than 30 min/day | 20.6 | 21.6 | |
| 30 min to less than 60 min/day | 11.8 | 11.2 | |
| 60 min/day | 8.3 | 10.6 | |
| More than 60 min/day | 3.5 | 3.4 | |
| Physical activity/inactivity (%) | 0.372 | ||
| Low active | 85.5 | 83.6 | |
| High active | 14.5 | 16.4 | |
| Means of travelling to school (%) | 0.291 | ||
| Walking | 4.8 | 3.4 | |
| Family or private car | 86.9 | 89.9 | |
| School bus | 8.3 | 6.7 | |
| BMI category | 0.057 | ||
| <25 kg/m2 | 69.1 | 74.3 | |
| 25 + kg/m2 | 30.9 | 25.7 |
| Variable | Breakfast Intake | p-Value * | ||
|---|---|---|---|---|
| All (N = 1149) | <5 Days/Week (N = 685) | 5 + Days/Week (N = 464) | ||
| Fried egg sandwich | 48.1 | 46.1 | 51.1 | 0.100 |
| Breakfast cereals | 45.9 | 39.0 | 56.0 | <0.001 |
| Spread cheese sandwich | 41.3 | 39.3 | 44.4 | 0.083 |
| Boiled egg sandwich | 27.7 | 25.5 | 30.8 | 0.050 |
| Tuna sandwich | 25.8 | 23.9 | 28.4 | 0.087 |
| Nutella sandwich | 25.0 | 23.4 | 27.4 | 0.123 |
| Croissant | 20.3 | 21.3 | 18.8 | 0.289 |
| Labneh sandwich ** | 16.5 | 14.2 | 20.0 | 0.008 |
| Cheese pie (Fataer Jubin) | 14.2 | 15.2 | 12.7 | 0.240 |
| Pancake | 13.3 | 13.9 | 12.5 | 0.503 |
| Fava beans (Foul) | 12.7 | 13.0 | 12.3 | 0.724 |
| Peanut butter sandwich | 8.3 | 6.7 | 10.6 | 0.020 |
| Thyme sandwich | 7.8 | 7.3 | 8.6 | 0.413 |
| Cake or cookies | 7.6 | 7.4 | 7.8 | 0.844 |
| Pizza | 7.6 | 7.3 | 8.0 | 0.671 |
| Mortadella sandwich | 7.4 | 8.5 | 5.8 | 0.092 |
| Solid cheese sandwich | 7.4 | 5.5 | 10.1 | 0.004 |
| Oreo biscuit/other types of biscuit | 7.2 | 6.7 | 8.0 | 0.419 |
| Falafel sandwich | 6.9 | 7.4 | 6.0 | 0.354 |
| Jam sandwich | 6.6 | 5.7 | 8.0 | 0.127 |
| Thyme pie (Fataer Zatar) | 6.4 | 6.6 | 6.0 | 0.715 |
| Labneh pie (Fataer Labneh) | 6.4 | 6.0 | 6.9 | 0.534 |
| Hot dog | 5.5 | 6.7 | 3.7 | 0.026 |
| Yogurt-with or without fruits | 4.6 | 4.4 | 5.0 | 0.647 |
| Chickpeas (Hummus) sandwich | 4.2 | 3.9 | 4.5 | 0.627 |
| Other kinds of breakfast *** | 12.4 | 9.9 | 16.2 | 00.002 |
| Variable | All (N = (1149) | Boys (N = (523) | Girls (N = (626) | p-Value * |
|---|---|---|---|---|
| Preference for cereal with/without added sugar (%) | 0.194 | |||
| With sugar | 66.9 | 65.3 | 68.1 | |
| Without sugar | 33.1 | 34.7 | 31.9 | |
| Preference for cereal with or without fruit (%) | 0.700 | |||
| With fruit | 15.6 | 14.6 | 16.5 | |
| Without fruit | 84.4 | 85.4 | 83.5 | |
| Percentage of fresh fruit eaten with breakfast (%) | 53.1 | 60.6 | 46.8 | <0.001 |
| Types of fruits consumed most with breakfast (%): | ||||
| Apple | 31.8 | 26.8 | 35.9 | 0.001 |
| Banana | 24.6 | 26.0 | 22.9 | 0.237 |
| Grape | 16.6 | 12.4 | 20.1 | <0.001 |
| Orange | 15.9 | 14.5 | 17.1 | 0.237 |
| Strawberries | 8.6 | 3.8 | 12.6 | <0.001 |
| Pear | 5.3 | 6.4 | 4.0 | 0.074 |
| Mango | 1.8 | 1.7 | 1.9 | 0.805 |
| Kiwi | 1.5 | 1.5 | 1.4 | 0.898 |
| Watermelon | 1.0 | 1.0 | 1.0 | 0.997 |
| All others (less than 1% each and include dates, pineapple, figs and raisins) | 1.1 | 0.3 | 2.0 | <0.001 |
| Drinks consumed with breakfast (%) | 90.5 | 95.0 | 86.7 | <0.001 |
| Types of Drinks consumed with breakfast (%): | ||||
| Full fat milk | 44.6 | 44.0 | 45.2 | 0.676 |
| Water | 42.2 | 39.2 | 44.7 | 0.095 |
| Chocolate milk | 31.6 | 27.2 | 35.3 | 0.003 |
| Fruit juice | 29.4 | 27.3 | 31.2 | 0.158 |
| Tea with milk | 27.2 | 28.7 | 25.9 | 0.279 |
| Tea | 11.6 | 13.8 | 9.7 | 0.034 |
| Strawberry milk | 9.7 | 6.7 | 12.3 | 0.001 |
| Fruit drink | 9.4 | 8.8 | 9.9 | 0.521 |
| Low fat milk | 8.2 | 9.4 | 7.2 | 0.179 |
| Soft drink (soft beverage) | 2.0 | 3.3 | 1.0 | 0.006 |
| Butter milk | 1.0 | 1.3 | 0.8 | 0.370 |
| Coffee with milk | 0.7 | 1.0 | 0.5 | 0.333 |
| Other drinks | 1.0 | 0.0 | 1.9 | 0.333 |
| Variable | Frequency of Breakfast Intake | p-Value * | ||
|---|---|---|---|---|
| All (N = 1149) | <5 Days/Week (N = 685) | 5 + Days/Week (N = 464) | ||
| Who prepare the breakfast the most for the child? (%) | 0.019 | |||
| Mother | 77.9 | 76.8 | 79.5 | |
| Domestic helper | 7.3 | 7.0 | 7.8 | |
| The child himself/herself | 4.4 | 5.8 | 2.4 | |
| Father | 3.6 | 3.5 | 3.7 | |
| Nothing is prepared at home | 3.0 | 3.8 | 1.9 | |
| Sister/brother | 2.2 | 1.5 | 3.2 | |
| Brought ready from the market | 1.6 | 1.6 | 1.5 | |
| Does your child have lactose intolerance? (%) | 0.266 | |||
| Yes | 1.8 | 2.2 | 1.3 | |
| No | 98.2 | 97.8 | 98.7 | |
| Are you satisfied with the breakfast consumed by your child at home? (%) | 0.001 | |||
| Yes, satisfied | 45.7 | 43.4 | 49.1 | |
| Somewhat satisfied | 46.7 | 46.7 | 46.8 | |
| Not satisfied | 7.6 | 9.9 | 4.1 | |
| As a meal, how important for you is your child’s breakfast? (%) | 0.069 | |||
| Very important | 93.0 | 91.5 | 95.0 | |
| Somewhat important | 6.6 | 7.9 | 4.7 | |
| Not important | 0.4 | 0.6 | 0.2 | |
| In your opinion, which is the most important meal of the day for your child? (%) | 0.009 | |||
| Breakfast | 80.6 | 77.7 | 84.9 | |
| Lunch | 17.6 | 20.1 | 13.8 | |
| Dinner | 1.8 | 2.2 | 1.3 | |
| Variable | Gender | Breakfast Intakes | p-Value * | |
|---|---|---|---|---|
| <5 Days/Week (N = 685) | 5 + Days/Week (N = 464) | |||
| Body weight (kg) | Boys | 33.5 ± 11.8 | 30.9 ± 9.6 | Breakfast intake: 0.004 |
| Gender: 0.287 | ||||
| Girls | 33.8 ± 11.7 | 32.4 ± 11.3 | Breakfast intake by gender interaction: 0.127 | |
| All | 33.7 ± 11.8 | 31.7 ± 10.5 | ||
| BMI (kg/m2) | Boys | 18.2 ± 4.2 | 17.3 ± 3.6 | Breakfast intake: 0.009 |
| Girls | 18.4 ± 3.9 | 18.0 ± 3.9 | Gender: 0.054 | |
| All | 18.3 ± 4.0 | 17.7 ± 3.8 | Breakfast intake by gender interaction: 0.213 | |
| Screen time (h/night) | Boys | 3.55 ± 1.8 | 3.04 ± 1.5 | Breakfast intake: 0.081 |
| Gender: =<0.001= | ||||
| Girls | 2.78 ± 1.5 | 2.81 ± 1.8 | Breakfast intake by gender interaction: 0.005 | |
| All | 3.13 ± 1.7 | 2.91 ± 1.7 | Breakfast intake: <0.001 | |
| Sleep duration (h/night) | Boys | 8.18 ± 1.2 | 8.51 ± 1.1 | Gender: 0.025 |
| Girls | 8.30 ± 1.3 | 8.63 ± 1.0 | Breakfast intake by gender interaction: 0.886 | |
| All | 8.25 ± 1.2 | 8.57 ± 1.1 | ||
| Physical activity (min/week) | Boys | 196.0 ± 232.5 | 213.3 ± 225.5 | Breakfast intake: 0.526 |
| Girls | 95.2 ± 158.4 | 92.4 ± 157.8 | Gender: <0.001 | |
| All | 141.2 ± 202.0 | 148.2 ± 201.1 | Breakfast intake by gender interaction: 0.268 | |
| Variable | Breakfast Intake (<5 Days/Week Versus 5 + Days/Week) * | |||
|---|---|---|---|---|
| aOR | (95% CI) | SEE | p-Value | |
| Age | 1.008 | 0.934–1.088 | 0.039 | 0.837 |
| Gender (girls = ref) | 1.00 | |||
| Boys | 1.026 | 0.79401.326 | 0.131 | 0.843 |
| No. of family member in the house (high = ref) | 1.00 | |||
| Low number | 1.053 | 0.797–1.392 | 0.142 | 0.715 |
| Paternal age (older age = ref) | 1.00 | |||
| Younger age | 0.937 | 0.774–1.135 | 0.098 | 0.507 |
| Maternal age (older age = ref) | 1.00 | |||
| younger age | 0.953 | 0.755–1.202 | 0.119 | 0.684 |
| Paternal education (high = ref) | 1.00 | |||
| Low education | 1.212 | 1.020–1.440 | 0.088 | 0.029 |
| Maternal education (high = ref) | 1.00 | |||
| Low education | 1.212 | 1.003–1.464 | 0.096 | 0.046 |
| Family income (> low = ref) | 1.00 | |||
| High income | 0.964 | 0.808–1.151 | 0.090 | 0.688 |
| No. of children in the family (high = ref) | 1.00 | |||
| Low number of children | 0.848 | 0.673–1.069 | 0.118 | 0.163 |
| Screen time (high = ref) | 1.00 | |||
| Low screen time | 1.026 | 0.784–1.344 | 0.138 | 0.849 |
| Sleep duration (sufficient = ref) | 1.00 | |||
| Insufficient sleep | 0.735 | 0.567–0.951 | 0.132 | 0.019 |
| Physical activity (active = ref) | 1.00 | |||
| Inactive | 0.899 | 0.636–1.271 | 0.177 | 0.548 |
| Overweight or obesity (BMI ≥ 25 kg/m2 = ref) | 1.00 | |||
| BMI < 25 kg/m 2 | 1.333 | 1.015–1.752 | 0.139 | 00.039 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Hazzaa, H.M.; Al-Rasheedi, A.A.; Alsulaimani, R.A.; Jabri, L. Anthropometric, Familial- and Lifestyle-Related Characteristics of School Children Skipping Breakfast in Jeddah, Saudi Arabia. Nutrients 2020, 12, 3668. https://doi.org/10.3390/nu12123668
Al-Hazzaa HM, Al-Rasheedi AA, Alsulaimani RA, Jabri L. Anthropometric, Familial- and Lifestyle-Related Characteristics of School Children Skipping Breakfast in Jeddah, Saudi Arabia. Nutrients. 2020; 12(12):3668. https://doi.org/10.3390/nu12123668
Chicago/Turabian StyleAl-Hazzaa, Hazzaa M., Amani A. Al-Rasheedi, Rayan A. Alsulaimani, and Laura Jabri. 2020. "Anthropometric, Familial- and Lifestyle-Related Characteristics of School Children Skipping Breakfast in Jeddah, Saudi Arabia" Nutrients 12, no. 12: 3668. https://doi.org/10.3390/nu12123668