Alcohol Consumption and Risk of Chronic Kidney Disease: A Nationwide Observational Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Ethical Statement
2.3. Alcohol Consumption
2.4. Determination of CKD
2.5. Potential Confounders
2.6. Study Design
2.7. Statistical Analysis
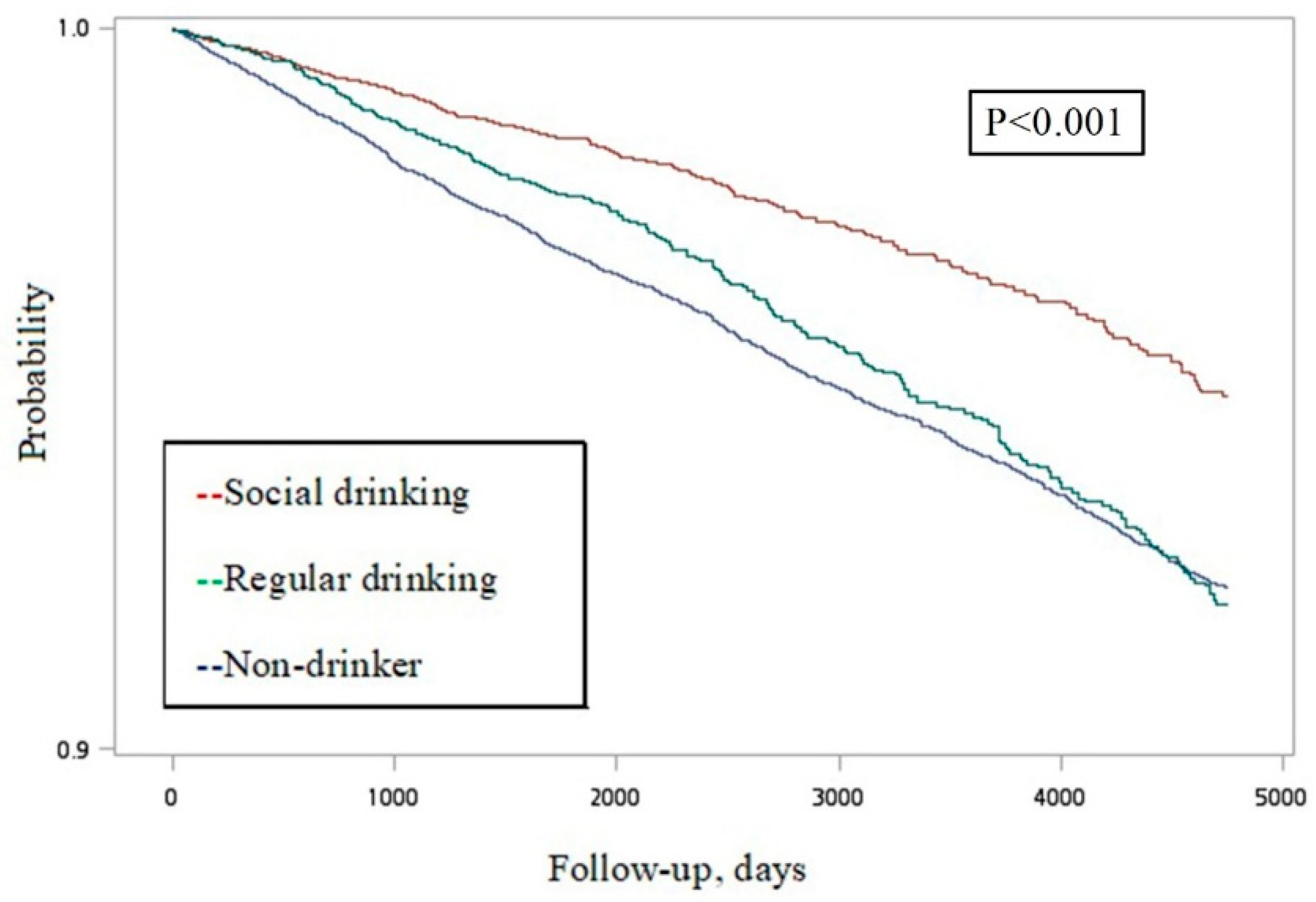
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ronksley, P.E.; Brien, S.E.; Turner, B.J.; Mukamal, K.J.; Ghali, W.A. Association of alcohol consumption with selected cardiovascular disease outcomes: A systematic review and meta-analysis. BMJ (Clin. Res. Ed.) 2011, 342, d671. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, L.; Gronbaek, M.; Becker, U.; Tolstrup, J.S. Risk of pancreatitis according to alcohol drinking habits: A population-based cohort study. Am. J. Epidemiol. 2008, 168, 932–937. [Google Scholar] [CrossRef] [PubMed]
- Varela-Rey, M.; Woodhoo, A.; Martinez-Chantar, M.L.; Mato, J.M.; Lu, S.C. Alcohol, DNA methylation, and cancer. Alcohol Res. Curr. Rev. 2013, 35, 25–35. [Google Scholar]
- Dinu, D.; Nechifor, M.T.; Movileanu, L. Ethanol-induced alterations of the antioxidant defense system in rat kidney. J. Biochem. Mol. Toxicol. 2005, 19, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, R.; Miranda, A.; Vergara, L. Modulation of endogenous antioxidant system by wine polyphenols in human disease. Clin. Chim. Acta 2011, 412, 410–424. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, R.; Rivera, G.; Orellana, M.; Araya, J.; Bosco, C. Rat kidney antioxidant response to long-term exposure to flavonol rich red wine. Life Sci. 2002, 71, 2881–2895. [Google Scholar] [CrossRef]
- Rodrigo, R.; Castillo, R.; Carrasco, R.; Huerta, P.; Moreno, M. Diminution of tissue lipid peroxidation in rats is related to the in vitro antioxidant capacity of wine. Life Sci. 2005, 76, 889–900. [Google Scholar] [CrossRef]
- Leal, S.; Ricardo Jorge, D.O.; Joana, B.; Maria, S.S.; Isabel, S.S. Heavy Alcohol Consumption Effects on Blood Pressure and on Kidney Structure Persist After Long-Term Withdrawal. Kidney Blood Press. Res. 2017, 42, 664–675. [Google Scholar] [CrossRef]
- Hsu, Y.H.; Pai, H.C.; Chang, Y.M.; Liu, W.H.; Hsu, C.C. Alcohol consumption is inversely associated with stage 3 chronic kidney disease in middle-aged Taiwanese men. BMC Nephrol. 2013, 14, 254. [Google Scholar] [CrossRef]
- Kim, H.N.; Kim, S.H.; Song, S.W. Is alcohol drinking associated with renal impairment in the general population of South Korea? Kidney Blood Press. Res. 2014, 39, 40–49. [Google Scholar] [CrossRef]
- Matsumoto, A.; Nagasawa, Y.; Yamamoto, R.; Shinzawa, M.; Hasuike, Y.; Kuragano, T.; Isaka, Y.; Nakanishi, T.; Iseki, K.; Yamagata, K.; et al. The association of alcohol and smoking with CKD in a Japanese nationwide cross-sectional survey. Hypertens. Res. 2017, 40, 771–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, S.L.; Polkinghorne, K.R.; Cass, A.; Shaw, J.E.; Atkins, R.C.; Chadban, S.J. Alcohol consumption and 5-year onset of chronic kidney disease: The AusDiab study. Nephrol. Dial. Transplant. 2009, 24, 2464–2472. [Google Scholar] [CrossRef] [PubMed]
- Menon, V.; Katz, R.; Mukamal, K.; Kestenbaum, B.; de Boer, I.H.; Siscovick, D.S.; Sarnak, M.J.; Shlipak, M.G. Alcohol consumption and kidney function decline in the elderly: Alcohol and kidney disease. Nephrol. Dial. Transplant. 2010, 25, 3301–3307. [Google Scholar] [CrossRef] [PubMed]
- Koning, S.H.; Gansevoort, R.T.; Mukamal, K.J.; Rimm, E.B.; Bakker, S.J.; Joosten, M.M. Alcohol consumption is inversely associated with the risk of developing chronic kidney disease. Kidney Int. 2015, 87, 1009–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, H.H.; Chang, H.Y.; Chiang, Y.T.; Wu, M.S.; Lin, J.T.; Liao, W.C. Smoking, drinking, and pancreatitis: A population-based cohort study in Taiwan. Pancreas 2014, 43, 1117–1122. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.J.; Hu, H.Y.; Lee, Y.L.; Ko, M.C.; Ku, P.W.; Yen, Y.F.; Chu, D. Frequency of alcohol consumption and risk of type 2 diabetes mellitus: A nationwide cohort study. Clin. Nutr. (Edinb. Scotl.) 2018. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.J.; Hu, H.Y.; Lin, C.H.; Lee, S.T.; Kuo, S.C.; Chou, P. Incidence and risk factors of lower extremity amputations in people with type 2 diabetes in Taiwan, 2001–2010. J. Diabetes 2015, 7, 260–267. [Google Scholar] [CrossRef]
- Pan, W.H.; Lee, M.S.; Chuang, S.Y.; Lin, Y.C.; Fu, M.L. Obesity pandemic, correlated factors and guidelines to define, screen and manage obesity in Taiwan. Obes. Rev. 2008, 9, 22–31. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef]
- Chiva-Blanch, G.; Urpi-Sarda, M.; Llorach, R.; Rotches-Ribalta, M.; Guillen, M.; Casas, R.; Arranz, S.; Valderas-Martinez, P.; Portoles, O.; Corella, D.; et al. Differential effects of polyphenols and alcohol of red wine on the expression of adhesion molecules and inflammatory cytokines related to atherosclerosis: A randomized clinical trial. Am. J. Clin. Nutr. 2012, 95, 326–334. [Google Scholar] [CrossRef]
- Wakabayashi, I.; Daimon, T. Alcohol-independent beneficial cardiometabolic profile of individuals with hyper-HDL cholesterolemia in Japanese men and women. J. Clin. Lipidol. 2015, 9, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Li, J.; Shearer, G.C.; Lichtenstein, A.H.; Zheng, X.; Wu, Y.; Jin, C.; Wu, S.; Gao, X. Longitudinal study of alcohol consumption and HDL concentrations: A community-based study. Am. J. Clin. Nutr. 2017, 105, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Crandall, J.P.; Polsky, S.; Howard, A.A.; Perreault, L.; Bray, G.A.; Barrett-Connor, E.; Brown-Friday, J.; Whittington, T.; Foo, S.; Ma, Y.; et al. Alcohol consumption and diabetes risk in the Diabetes Prevention Program. Am. J. Clin. Nutr. 2009, 90, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Abbasi, F.; Lamendola, C.; Reaven, G.M. Effect of moderate alcoholic beverage consumption on insulin sensitivity in insulin-resistant, nondiabetic individuals. Metab. Clin. Exp. 2009, 58, 387–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napoli, R.; Cozzolino, D.; Guardasole, V.; Angelini, V.; Zarra, E.; Matarazzo, M.; Cittadini, A.; Sacca, L.; Torella, R. Red wine consumption improves insulin resistance but not endothelial function in type 2 diabetic patients. Metab. Clin. Exp. 2005, 54, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Baliunas, D.O.; Taylor, B.J.; Irving, H.; Roerecke, M.; Patra, J.; Mohapatra, S.; Rehm, J. Alcohol as a risk factor for type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2009, 32, 2123–2132. [Google Scholar] [CrossRef] [PubMed]
- Tsubono, Y.; Yamada, S.; Nishino, Y.; Tsuji, I.; Hisamichi, S. Choice of comparison group in assessing the health effects of moderate alcohol consumption. JAMA 2001, 286, 1177–1178. [Google Scholar] [CrossRef] [PubMed]
- Conigrave, K.M.; Hu, B.F.; Camargo, C.A., Jr.; Stampfer, M.J.; Willett, W.C.; Rimm, E.B. A prospective study of drinking patterns in relation to risk of type 2 diabetes among men. Diabetes 2001, 50, 2390–2395. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographics | Mean ± SD/Numbers (% In Column) | Number of CKD Cases (% In Row) | Hazard Ratio | (95% CI) |
|---|---|---|---|---|
| Alcohol | ||||
| Non-drinker | 27,781 (61.5) | 1535 (5.5) | Ref | |
| Social | 10,997 (24.3) | 292 (2.7) | 0.57 | (0.50–0.65) |
| Regular | 6422 (14.2) | 317 (4.9) | 0.93 | (0.82–1.05) |
| Age in years, mean (SD) | 42.73 (16.64) | 50.08 (15.78) | 1.07 | (1.06–1.07) |
| Gender | ||||
| Female | 22,971 (50.8) | 960 (4.2) | Ref | |
| Male | 22,229 (49.2) | 1184 (5.3) | 1.27 | (1.16–1.38) |
| Marriage status | ||||
| Married/cohabiting | 27,295 (60.4) | 1523 (5.6) | Ref | |
| Never married | 13,152 (29.1) | 177 (1.4) | 0.24 | (0.20–0.28) |
| Widowed/divorced/separated | 4743 (10.5) | 444 (9.4) | 1.96 | (1.77–2.18) |
| Education | ||||
| Low (elementary or below) | 11,108 (24.6) | 1244 (11.2) | Ref | |
| Moderate (junior/senior high) | 20,009 (44.3) | 638 (3.2) | 0.26 | (0.24–0.29) |
| High (college or above) | 14,046 (31.1) | 256 (1.8) | 0.16 | (0.14–0.18) |
| Household income | ||||
| <US $952/month | 9796 (23.2) | 763 (7.8) | Ref | |
| US $952–2222/month | 18,353 (43.4) | 774 (4.2) | 0.49 | (0.44–0.54) |
| >US$ 2222/month | 14,118 (33.4) | 480 (3.4) | 0.39 | (0.34–0.43) |
| Obesity | ||||
| No | 36,270 (84.3) | 1367 (3.8) | Ref | |
| Yes | 6771 (15.7) | 474 (7.0) | 1.97 | (1.78–2.19) |
| Smoking status | ||||
| Never | 31,082 (68.8) | 1393 (4.5) | Ref | |
| Current | 11,456 (25.4) | 544 (4.8) | 1.05 | (0.95–1.16) |
| Former | 2639 (5.8) | 207 (7.8) | 2.23 | (1.92–2.58) |
| Vegetables | ||||
| <5 days/week | 6358 (14.1) | 330 (5.2) | Ref | |
| 5–7 days/week | 38,790 (85.9) | 1808 (4.7) | 0.97 | (0.86–1.09) |
| Fruit | ||||
| <5 days/week | 16,782 (37.2) | 876 (5.2) | Ref | |
| 5–7 days/week | 28,365 (62.8) | 1263 (4.5) | 0.94 | (0.86–1.02) |
| Physical activity | ||||
| 0 kcal/week | 20,963 (47.5) | 976 (4.7) | Ref | |
| 0–800 kcal/week | 12,253 (27.8) | 465 (3.8) | 0.84 | (0.75–0.94) |
| >800 kcal/week | 10,931 (24.8) | 606 (5.5) | 1.24 | (1.12–1.37) |
| Diabetes | ||||
| No | 38,864 (86.0) | 1292 (3.3) | Ref | |
| Yes | 6336 (14.0) | 852 (13.5) | 4.15 | (3.80–4.52) |
| Hypertension | ||||
| No | 32,260 (71.4) | 671 (2.1) | Ref | |
| Yes | 12,940 (28.6) | 1473 (11.4) | 5.53 | (5.06–6.06) |
| Hyperlipidemia | ||||
| No | 35,395 (78.3) | 1222 (3.5) | Ref | |
| Yes | 9805 (21.7) | 922 (9.4) | 2.64 | (2.43–2.88) |
| Urolithiasis | ||||
| No | 42,440 (93.9) | 1917 (4.5) | Ref | |
| Yes | 2760 (6.1) | 227 (8.2) | 1.79 | (1.56–2.05) |
| Gouty arthritis | ||||
| No | 40,402 (89.4) | 1504 (3.7) | Ref | |
| Yes | 4798 (10.6) | 640 (13.3) | 3.55 | (3.23–3.89) |
| Demographics | Adjusted Hazard Ratio | (95% CI) | p-Value |
|---|---|---|---|
| Alcohol * | |||
| Non-drinker | Ref | ||
| Social | 0.85 | (0.74–0.97) | 0.018 |
| Regular | 0.85 | (0.74–0.98) | 0.024 |
| Age in years | 1.05 | (1.05–1.05) | <0.001 * |
| Gender | |||
| Female | Ref | ||
| Male | 1.28 | (1.14–1.44) | <0.001 |
| Education | |||
| Low (elementary or below) | Ref | ||
| Moderate (junior/senior high) | 0.86 | (0.76–0.97) | 0.013 |
| High (college or above) | 0.72 | (0.61–0.84) | <0.001 |
| Vegetable | |||
| <5 days/week | Ref | ||
| 5–7 days/week | 0.82 | (0.71–0.95) | 0.007 |
| Fruit | |||
| <5 days/week | Ref | ||
| 5–7 days/week | 0.98 | (0.88–1.09) | 0.73 |
| Physical activity | |||
| 0 kcal/week | Ref | ||
| 0–800 kcal/week | 0.89 | (0.79–1.01) | 0.07 |
| >800 kcal/week | 0.92 | (0.82–1.03) | 0.16 |
| Obesity (BMI ≥ 27 kg/m2) | |||
| No | Ref | ||
| Yes | 1.31 | (1.17–1.47) | <0.001 |
| Smoking status | |||
| Never | Ref | ||
| Current | 1.11 | (0.97–1.26) | 0.13 |
| Former | 1.3 | (1.09–1.54) | 0.005 |
| Diabetes | |||
| No | Ref | ||
| Yes | 1.65 | (1.48–1.83) | <0.001 |
| Hypertension | |||
| No | Ref | ||
| Yes | 1.54 | (1.36–1.74) | <0.001 |
| Urolithiasis | |||
| No | Ref | ||
| Yes | 1.19 | (1.02–1.39) | 0.027 |
| Gouty arthritis | |||
| No | Ref | ||
| Yes | 1.76 | (1.58–1.96) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.-J.; Chen, Y.-Y.; Lin, Y.-K.; Chen, C.-C.; Yen, Y.-F.; Deng, C.-Y. Alcohol Consumption and Risk of Chronic Kidney Disease: A Nationwide Observational Cohort Study. Nutrients 2019, 11, 2121. https://doi.org/10.3390/nu11092121
Lai Y-J, Chen Y-Y, Lin Y-K, Chen C-C, Yen Y-F, Deng C-Y. Alcohol Consumption and Risk of Chronic Kidney Disease: A Nationwide Observational Cohort Study. Nutrients. 2019; 11(9):2121. https://doi.org/10.3390/nu11092121
Chicago/Turabian StyleLai, Yun-Ju, Yu-Yen Chen, Yu-Kai Lin, Chu-Chieh Chen, Yung-Feng Yen, and Chung-Yeh Deng. 2019. "Alcohol Consumption and Risk of Chronic Kidney Disease: A Nationwide Observational Cohort Study" Nutrients 11, no. 9: 2121. https://doi.org/10.3390/nu11092121
APA StyleLai, Y.-J., Chen, Y.-Y., Lin, Y.-K., Chen, C.-C., Yen, Y.-F., & Deng, C.-Y. (2019). Alcohol Consumption and Risk of Chronic Kidney Disease: A Nationwide Observational Cohort Study. Nutrients, 11(9), 2121. https://doi.org/10.3390/nu11092121