Asymptomatic Helicobacter Pylori Infection in Preschool Children and Young Women Does Not Predict Iron Bioavailability from Iron-Fortified Foods

 ,
,
Abstract
1. Introduction
2. Materials and Methods
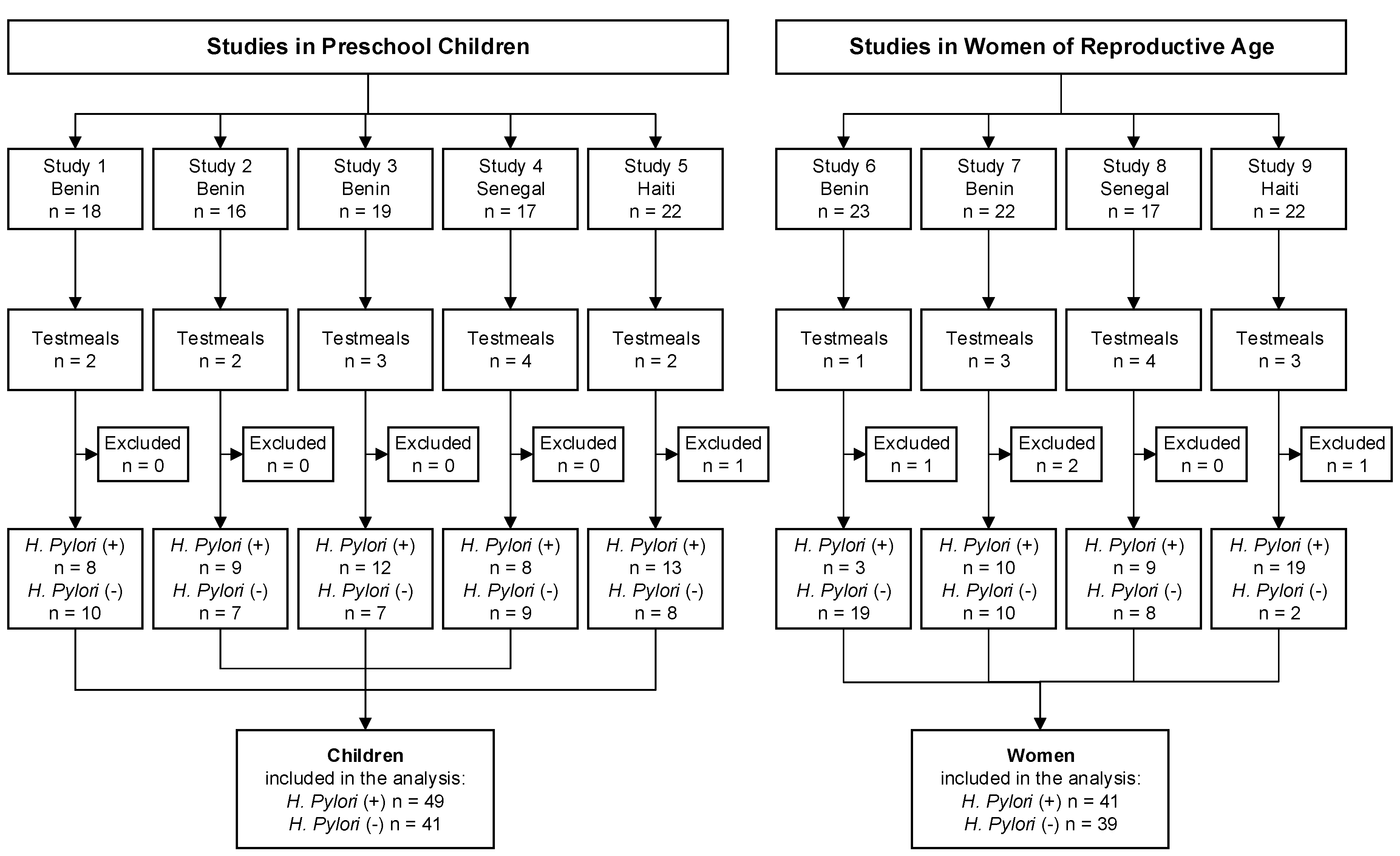
2.1. Subjects and Study Design
2.2. Laboratory Analysis
2.3. Statistical Analysis
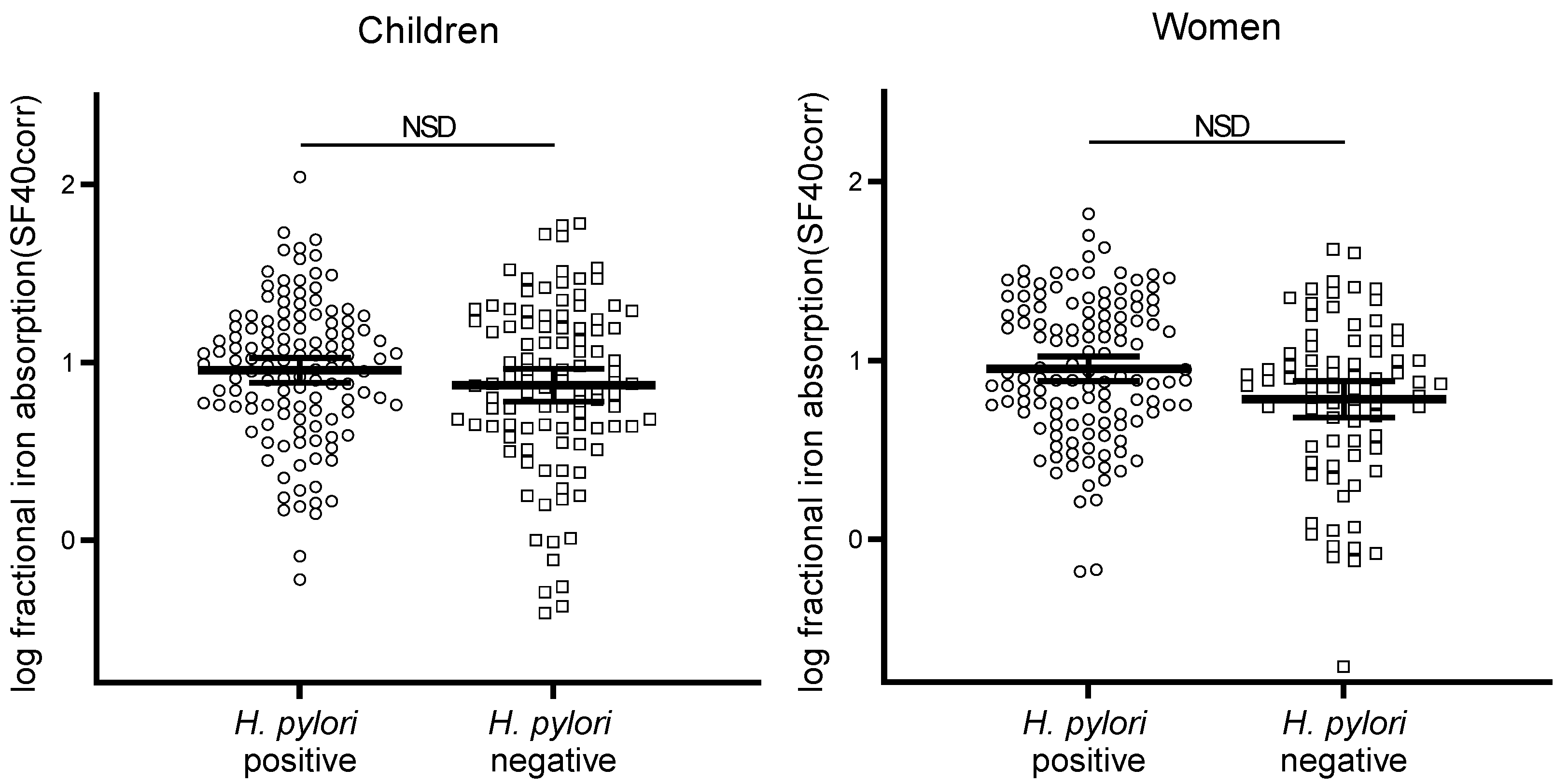
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Blaser, M.J.; Atherton, J.C. Helicobacter pylori persistence: Biology and disease. J. Clin. Investig. 2004, 113, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Atherton, J.C. The pathogenesis of Helicobacter pylori-induced gastro-duodenal diseases. Annu. Rev. Pathol. 2006, 1, 63–96. [Google Scholar] [CrossRef] [PubMed]
- Wongphutorn, P.; Chomvarin, C.; Sripa, B.; Namwat, W.; Faksri, K. Detection and genotyping of Helicobacter pylori in saliva versus stool samples from asymptomatic individuals in Northeastern Thailand reveals intra-host tissue-specific H. pylori subtypes. BMC Microbiol. 2018, 18, 10. [Google Scholar] [CrossRef] [PubMed]
- Mathewos, B.; Moges, B.; Dagnew, M. Seroprevalence and trend of Helicobacter pylori infection in Gondar University Hospital among dyspeptic patients, Gondar, North West Ethiopia. BMC Res. Notes 2013, 6, 346. [Google Scholar] [CrossRef] [PubMed]
- Kienesberger, S.; Perez-Perez, G.I.; Olivares, A.Z.; Bardhan, P.; Sarker, S.A.; Hasan, K.Z.; Sack, R.B.; Blaser, M.J. When is Helicobacter pylori acquired in populations in developing countries? A birth-cohort study in Bangladeshi children. Gut Microbes 2018, 9, 252–263. [Google Scholar] [CrossRef]
- Sarker, S.A.; Mahalanabis, D.; Hildebrand, P.; Rahaman, M.M.; Bardhan, P.K.; Fuchs, G.; Beglinger, C.; Gyr, K. Helicobacter pylori: Prevalence, transmission, and serum pepsinogen II concentrations in children of a poor periurban community in Bangladesh. Clin. Infect. Dis. 1997, 25, 990–995. [Google Scholar] [CrossRef]
- Nahar, S.; Kaderi Kibria, K.M.; Hossain, M.E.; Sarker, S.A.; Bardhan, P.K.; Talukder, K.A.; Rahman, M. Epidemiology of H. pylori and its Relation with Gastrointestinal Disorders, A Community-based Study in Dhaka, Bangladesh. J. Gastroenterol. Hepatol. Res. 2018, 7, 2709–2716. [Google Scholar] [CrossRef]
- Hudak, L.; Jaraisy, A.; Haj, S.; Muhsen, K. An updated systematic review and meta-analysis on the association between Helicobacter pylori infection and iron deficiency anemia. Helicobacter 2017, 22, 12330. [Google Scholar] [CrossRef]
- Xu, M.Y.; Cao, B.; Yuan, B.S.; Yin, J.; Liu, L.; Lu, Q.B. Association of anaemia with Helicobacter pylori infection: A retrospective study. Sci. Rep. 2017, 7, 13434. [Google Scholar] [CrossRef]
- McColl, K.E.; el-Omar, E.; Gillen, D. Interactions between H. pylori infection, gastric acid secretion and anti-secretory therapy. Br. Med. Bull. 1998, 54, 121–138. [Google Scholar] [CrossRef]
- Calam, J.; Gibbons, A.; Healey, Z.V.; Bliss, P.; Arebi, N. How does Helicobacter pylori cause mucosal damage? Its effect on acid and gastrin physiology. Gastroenterology 1997, 113, S43–S49. [Google Scholar] [CrossRef]
- Zhang, Z.W.; Patchett, S.E.; Perrett, D.; Katelaris, P.H.; Domizio, P.; Farthing, M.J. The relation between gastric vitamin C concentrations, mucosal histology, and CagA seropositivity in the human stomach. Gut 1998, 43, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Nahon, S.; Lahmek, P.; Massard, J.; Lesgourgues, B.; de Serre, N.M.; Traissac, L.; Bodiguel, V.; Adotti, F.; Delas, N. Helicobacter pylori-associated chronic gastritis and unexplained iron deficiency anemia: A reliable association? Helicobacter 2003, 8, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Kaye, P.V.; Garsed, K.; Ragunath, K.; Jawhari, A.; Pick, B.; Atherton, J.C. The clinical utility and diagnostic yield of routine gastric biopsies in the investigation of iron deficiency anemia: A case-control study. Am. J. Gastroenterol. 2008, 103, 2883–2889. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Yang, J.H.; Hong, S.N.; Kim, J.H.; Sung, I.K.; Park, H.S.; Shim, C.S. Low Hemoglobin Levels are Related to the Presence of Gastric Atrophy Rather Than the Presence of H. pylori Infection Itself: A Study of 2398 Asymptomatic Adults. Gastroenterology 2012, 142, S474. [Google Scholar] [CrossRef]
- Harris, P.R.; Serrano, C.A.; Villagran, A.; Walker, M.M.; Thomson, M.; Duarte, I.; Windle, H.J.; Crabtree, J.E. Helicobacter pylori-associated hypochlorhydria in children, and development of iron deficiency. J. Clin. Pathol. 2013, 66, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, D.M.; Harris, P.R.; Sanderson, I.R.; Windle, H.J.; Walker, M.M.; Rocha, A.M.; Rocha, G.A.; Carvalho, S.D.; Bittencourt, P.F.; de Castro, L.P.; et al. Iron status and Helicobacter pylori infection in symptomatic children: An international multi-centered study. PLoS ONE 2013, 8, e68833. [Google Scholar] [CrossRef] [PubMed]
- Ciacci, C.; Sabbatini, F.; Cavallaro, R.; Castiglione, F.; di Bella, S.; Iovino, P.; Palumbo, A.; Tortora, R.; Amoruso, D.; Mazzacca, G. Helicobacter pylori impairs iron absorption in infected individuals. Dig. Liver Dis. 2004, 36, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Lopez de Romana, D.; Pizarro, F.; Diazgranados, D.; Barba, A.; Olivares, M.; Brunser, O. Effect of Helicobacter pylori infection on iron absorption in asymptomatic adults consuming wheat flour fortified with iron and zinc. Biol. Trace Elem. Res. 2011, 144, 1318–1326. [Google Scholar] [CrossRef]
- Sarker, S.A.; Davidsson, L.; Mahmud, H.; Walczyk, T.; Hurrell, R.F.; Gyr, N.; Fuchs, G.J. Helicobacter pylori infection, iron absorption, and gastric acid secretion in Bangladeshi children. Am. J. Clin. Nutr. 2004, 80, 149–153. [Google Scholar] [CrossRef]
- Sarker, S.A.; Mahmud, H.; Davidsson, L.; Alam, N.H.; Ahmed, T.; Alam, N.; Salam, M.A.; Beglinger, C.; Gyr, N.; Fuchs, G.J. Causal relationship of Helicobacter pylori with iron-deficiency anemia or failure of iron supplementation in children. Gastroenterology 2008, 135, 1534–1542. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.; Cacoub, P.; Macdougall, I.C.; Peyrin-Biroulet, L. Iron deficiency anaemia. Lancet 2015, 387, 907–916. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines on Food Fortification with Micronutrients. In Bruno De Benoist, Omar Dary, Richard Hurrell; Allen, L., Ed.; World Health Organization: Geneva, Switzerland, 2006; p. 341. [Google Scholar]
- Hurrell, R.F. Flour fortification as a strategy to prevent anaemia. Br. J. Nutr. 2015, 114, 501–502. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Recommendations on Wheat and Maize Flour Fortification Meeting Report: Interim Consensus Statement; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Food Fortification Initiative. Global Progress of Indistrually Milled Cereal Grains. 2018. Available online: http://www.ffinetwork.org/global_progress/index.php (accessed on 9 October 2018).
- Cercamondi, C.I.; Egli, I.M.; Ahouandjinou, E.; Dossa, R.; Zeder, C.; Salami, L.; Tjalsma, H.; Wiegerinck, E.; Tanno, T.; Hurrell, R.F.; et al. Afebrile Plasmodium falciparum parasitemia decreases absorption of fortification iron but does not affect systemic iron utilization: A double stable-isotope study in young Beninese women. Am. J. Clin. Nutr. 2010, 92, 1385–1392. [Google Scholar] [CrossRef] [PubMed]
- Cercamondi, C.I.; Egli, I.M.; Mitchikpe, E.; Tossou, F.; Hessou, J.; Zeder, C.; Hounhouigan, J.D.; Hurrell, R.F. Iron bioavailability from a lipid-based complementary food fortificant mixed with millet porridge can be optimized by adding phytase and ascorbic acid but not by using a mixture of ferrous sulfate and sodium iron EDTA. J. Nutr. 2013, 143, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Cercamondi, C.I.; Egli, I.M.; Mitchikpe, E.; Tossou, F.; Zeder, C.; Hounhouigan, J.D.; Hurrell, R.F. Total iron absorption by young women from iron-biofortified pearl millet composite meals is double that from regular millet meals but less than that from post-harvest iron-fortified millet meals. J. Nutr. 2013, 143, 1376–1382. [Google Scholar] [CrossRef] [PubMed]
- Herter-Aeberli, I.; Eliancy, K.; Rathon, Y.; Loechl, C.U.; Pierre, J.M.; Zimmermann, M.B. In Haitian women and preschool children, iron absorption from wheat flour-based meals fortified with sodium iron EDTA is higher than that from meals fortified with ferrous fumarate, and is not affected by Helicobacter pylori infection in children. Br. J. Nutr. 2017, 118, 273–279. [Google Scholar] [CrossRef]
- World Health Organization. Iron Deficiency Anaemia: Assessment, Prevention and Control: A Guide for Programme Managers; World Health Organization: Geneva, Switzerland, 2001; p. 114. [Google Scholar]
- Rapid Labs. H. pylori Ab Rapid Test, Manufactures Instructions; Rapid Labs Ltd.: Colchester, UK, 2014. [Google Scholar]
- Brown, E.; Bradley, B.; Wennesland, R.; Hodges, J.L.; Hopper, J.; Yamauchi, H. Red Cell, Plasma, and Blood Volume in Healthy Women Measured by Radichromium Cell-Labeling and Hematocrit. J. Clin. Investig. 1962, 41, 2182. [Google Scholar] [CrossRef]
- Walczyk, T.; Davidsson, L.; Zavaleta, N.; Hurrell, R.F. Stable isotope labels as a tool to determine the iron absorption by Peruvian school children from a breakfast meal. Fresenius J. Anal. Chem. 1997, 359, 445–449. [Google Scholar] [CrossRef]
- Turnlund, J.R.; Keyes, W.R.; Peiffer, G.L. Isotope ratios of molybdenum determined by thermal ionization mass spectrometry for stable isotope studies of molybdenum metabolism in humans. Anal. Chem. 1993, 65, 1717–1722. [Google Scholar] [CrossRef]
- International Atomic Energy Agency. Assessment of Iron Bioavailability in Humans Using Stable Iron Isotope Techniques; International Atomic Energy Agency: Vienna, Austria, 2012. [Google Scholar]
- Namaste, S.M.; Rohner, F.; Huang, J.; Bhushan, N.L.; Flores-Ayala, R.; Kupka, R.; Mei, Z.; Rawat, R.; Williams, A.M.; Raiten, D.J.; et al. Adjusting ferritin concentrations for inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 2017, 106, 359S–371S. [Google Scholar] [PubMed]
- Cook, J.D.; Dassenko, S.A.; Lynch, S.R. Assessment of the role of nonheme-iron availability in iron balance. Am. J. Clin. Nutr. 1991, 54, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Duque, X.; Moran, S.; Mera, R.; Medina, M.; Martinez, H.; Mendoza, M.E.; Torres, J.; Correa, P. Effect of eradication of Helicobacter pylori and iron supplementation on the iron status of children with iron deficiency. Arch. Med. Res. 2010, 41, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Otto, B.R.; van Vught Verweij, A.M.; MacLaren, D.M. Transferrins and heme-compounds as iron sources for pathogenic bacteria. Crit. Rev. Microbiol. 1992, 18, 217–233. [Google Scholar] [CrossRef] [PubMed]
- van Vliet, A.H.; Stoof, J.; Vlasblom, R.; Wainwright, S.A.; Hughes, N.J.; Kelly, D.J.; Bereswill, S.; Bijlsma, J.J.; Hoogenboezem, T.; Vandenbroucke-Grauls, C.M.; et al. The role of the Ferric Uptake Regulator (Fur) in regulation of Helicobacter pylori iron uptake. Helicobacter 2002, 7, 237–244. [Google Scholar] [CrossRef]
- Beutler, E. Hepcidin mimetics from microorganisms? A possible explanation for the effect of Helicobacter pylori on iron homeostasis. Blood Cells Mol. Dis. 2007, 38, 54–55. [Google Scholar] [CrossRef][Green Version]
- Sapmaz, F.; Basyigit, S.; Kalkan, I.H.; Kisa, U.; Kavak, E.E.; Guliter, S. The impact of Helicobacter pylori eradication on serum hepcidin-25 level and iron parameters in patients with iron deficiency anemia. Wien. Klin. Wochenschr. 2016, 128, 335–340. [Google Scholar] [CrossRef]
- Lee, S.Y.; Song, E.Y.; Yun, Y.M.; Yoon, S.Y.; Cho, Y.H.; Kim, S.Y.; Lee, M.H. Serum prohepcidin levels in Helicobacter pylori infected patients with iron deficiency anemia. Korean J. Intern. Med. 2010, 25, 195–200. [Google Scholar] [CrossRef]
- Yip, R.; Limburg, P.J.; Ahlquist, D.A.; Carpenter, H.A.; O’Neill, A.; Kruse, D.; Stitham, S.; Gold, B.D.; Gunter, E.W.; Looker, A.C.; et al. Pervasive occult gastrointestinal bleeding in an Alaska native population with prevalent iron deficiency. Role of Helicobacter pylori gastritis. JAMA 1997, 277, 1135–1139. [Google Scholar] [CrossRef]
- World Health Organization. Vitamin and Mineral Requirements in Human Nutrition, 2nd ed.; World Health Organization: Geneva, Switzerland, 2005; p. 341. [Google Scholar]
- Cook, J.D.; Lipschitz, D.A.; Miles, L.E.; Finch, C.A. Serum ferritin as a measure of iron stores in normal subjects. Am. J. Clin. Nutr. 1974, 27, 681–687. [Google Scholar] [CrossRef]
- Urita, Y.; Hike, K.; Torii, N.; Kikuchi, Y.; Kurakata, H.; Kanda, E.; Sasajima, M.; Miki, K. Comparison of serum IgA and IgG antibodies for detecting Helicobacter pylori infection. Intern. Med. 2004, 43, 548–552. [Google Scholar] [CrossRef] [PubMed][Green Version]



{kind=link}
{kind=link}
| Study | Location | Age Group | N | Test Meal Matrix | Fe/Meal (mg) | Study Arms (Fe Compound, Inhibitor or Enhancer) |
|---|---|---|---|---|---|---|
| 1 | Benin | Preschool children | 18 | Pearl millet porridge | 6 | 1. FeSO4 |
| 2. FeSO4 and NaFeEDTA 1 | ||||||
| 2 | Benin | Preschool children | 16 | Pearl millet porridge | 6 | 1. FeSO4 |
| 2. FeSO4 and Ascorbic Acid | ||||||
| 3 | Benin | Preschool children | 18 | Pearl millet porridge | 6 | 1. FeSO4 |
| 2. FeSO4 and phytase | ||||||
| 3. FeSO4 and phytase and Ascorbic Acid | ||||||
| 4 | Senegal | Preschool children | 17 | Wheat bread | 2 | 1. Fe Fumarate |
| 2. FeSO4 | ||||||
| 3. Fe Fumarate and tea infusion | ||||||
| 4. FeSO4 and tea infusion | ||||||
| 5 | Haiti | Preschool children | 21 | Wheat bread | 2 | 1. Fe Fumarate |
| 2. NaFeEDTA | ||||||
| 6 | Benin | Women | 23 | Fermented sorghum porridge | 3 | 1. NaFeEDTA |
| 7 | Benin | Women | 20 | Pearl millet paste | 4 | 1. Regular millet: FeSO4 |
| 2. Biofortified millet: FeSO4 | ||||||
| 3. Post-harvest fortified millet: FeSO4 | ||||||
| 8 | Senegal | Women | 17 | Wheat bread | 4 | 1. Fe Fumarate |
| 2. FeSO4 | ||||||
| 3. Fe Fumarate and tea infusion | ||||||
| 4. FeSO4 and tea infusion | ||||||
| 9 | Haiti | Women | 21 | Wheat bread | 4 | 1. Fe Fumarate |
| 2. NaFeEDTA | ||||||
| 3. NaFeEDTA and Fe fumarate 2 |
| Children | Women | |||||
|---|---|---|---|---|---|---|
| H. pylori Status | Positive | Negative | p | Positive | Negative | p |
| n | 49 | 41 | - | 41 | 39 | - |
| Age y | 2.8 (2.6, 3.1) 2 | 2.9 (2.6, 3.2) | 0.882 | 25.7 (23.4, 28.3) | 21.8 (20.2, 23.6) | 0.007 |
| Weight, kg | 12.3 (11.7, 13.0) | 12.4 (11.7, 13.2) | 0.975 | 55.1 (53.3, 57.0) | 55.0 (52.7, 57.4) | 0.997 |
| Height, cm | 91 (89, 94) | 92 (89, 95) | 0.972 | 160 (158, 162) | 162 (159, 164) | 0.447 |
| WAZ | −0.94 ± 0.78 3 | −0.93 ± 1.08 | 0.759 | n.a. | - | |
| HAZ | −0.88 ± 1.32 | −0.89 ± 1.63 | 0.818 | n.a. | - | |
| WHZ | −0.68 ± 0.87 | −0.67 ± 1.10 | 0.938 | n.a. | - | |
| Hb g/L | 109 (107, 112) | 114 (110, 117) | 0.052 | 126 (121, 132) | 125 (121, 130) | 0.776 |
| SF µg/L | 32.6 (26.7, 39.8) | 31.7 (25.1, 40.0) | 0.855 | 30.1 (22.1, 41.0) | 30.0 (22.9, 39.4) | 0.989 |
| SF adjusted 4 µg/L | 15.8 (12.9, 19.4) | 16.6 (13.3, 20.7) | 0.744 | 18.2 (13.8, 24.1) | 19.1 (14.6, 25.1) | 0.797 |
| CRP mg/L | 1.20 (0.71, 2.03) | 0.82 (0.49, 1.37) | 0.499 | 0.67 (0.43, 1.05) | 0.60 (0.41, 0.88) | 0.696 |
| CRP > 5 mg/L (n) | 12 | 8 | - | 2 | 3 | - |
| Children 2 | Women 3 | |||||
|---|---|---|---|---|---|---|
| Variables | b | SE | p | b | SE | p |
| Intercept | 1.62 | 0.21 | 0.000 | −0.22 | 1.69 | 0.898 |
| H. pylori infection | removed from the model 4 | removed from the model | ||||
| Food Matrix (all pairwise) | ||||||
| wheat bread-millet paste | n.a. | 0.34 | 0.09 | 0.000 | ||
| wheat bread-fermented sorghum | n.a. | −0.21 | 0.09 | 0.016 | ||
| millet paste-fermented sorghum | n.a. | −0.55 | 0.10 | 0.000 | ||
| millet-porridge-wheat bread | 0.41 | 0.11 | 0.000 | n.a. | ||
| Fe compound (all pairwise) | removed from the model | |||||
| Sulfate-Fumarate | 0.17 | 0.05 | 0.001 | |||
| Sulfate-EDTA | 0.05 | 0.08 | 0.557 | |||
| Sulfate-Sulfate and EDTA | 0.15 | 0.06 | 0.024 | |||
| Fumarate-EDTA | −0.13 | 0.07 | 0.055 | |||
| Fumarate-Sulfate and EDTA | −0.02 | 0.08 | 0.762 | |||
| EDTA-Sulfate and EDTA | 0.10 | 0.10 | 0.320 | |||
| Fe absorption enhancer | n.a. | |||||
| Ascorbic Acid-none | 0.19 | 0.07 | 0.005 | |||
| Phytase-none | 0.29 | 0.06 | 0.000 | |||
| Ascorbic Acid and Phytase-none | 0.36 | 0.06 | 0.000 | |||
| Fe absorption inhibitor | ||||||
| Tea-none | −0.42 | 0.05 | 0.000 | −0.33 | 0.05 | 0.000 |
| Gender | removed from the model | n.a. | ||||
| Age | −0.83 | 0.34 | 0.019 | removed from the model | ||
| Hemoglobin | removed | 0.93 | 0.85 | 0.273 | ||
| Serum ferritin adjusted for CRP | removed | −0.52 | 0.13 | 0.000 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buerkli, S.; Fatou Ndiaye, N.; Cercamondi, C.I.; Herter-Aeberli, I.; Moretti, D.; Zimmermann, M.B. Asymptomatic Helicobacter Pylori Infection in Preschool Children and Young Women Does Not Predict Iron Bioavailability from Iron-Fortified Foods. Nutrients 2019, 11, 2093. https://doi.org/10.3390/nu11092093
Buerkli S, Fatou Ndiaye N, Cercamondi CI, Herter-Aeberli I, Moretti D, Zimmermann MB. Asymptomatic Helicobacter Pylori Infection in Preschool Children and Young Women Does Not Predict Iron Bioavailability from Iron-Fortified Foods. Nutrients. 2019; 11(9):2093. https://doi.org/10.3390/nu11092093
Chicago/Turabian StyleBuerkli, Simone, Ndèye Fatou Ndiaye, Colin I. Cercamondi, Isabelle Herter-Aeberli, Diego Moretti, and Michael B. Zimmermann. 2019. "Asymptomatic Helicobacter Pylori Infection in Preschool Children and Young Women Does Not Predict Iron Bioavailability from Iron-Fortified Foods" Nutrients 11, no. 9: 2093. https://doi.org/10.3390/nu11092093
APA StyleBuerkli, S., Fatou Ndiaye, N., Cercamondi, C. I., Herter-Aeberli, I., Moretti, D., & Zimmermann, M. B. (2019). Asymptomatic Helicobacter Pylori Infection in Preschool Children and Young Women Does Not Predict Iron Bioavailability from Iron-Fortified Foods. Nutrients, 11(9), 2093. https://doi.org/10.3390/nu11092093