Impact of Caffeine Intake on 800-m Running Performance and Sleep Quality in Trained Runners

 ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Design
2.2. Participants
2.3. Procedures
2.4. Testing Session
2.5. Actigraphic Quality of Sleep, Subjective Quality of Sleep, and Autonomous Nocturnal Cardiac Activity
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ramos-Campo, D.J.; Rubio-Arias, J.; Freitas, T.T.; Camacho, A.; Jiménez-Diaz, J.F.; Alcaraz, P.E. Acute Physiological and Performance Responses to High-Intensity Resistance Circuit Training in Hypoxic and Normoxic Conditions. J. Strength Cond. Res. 2017, 31, 1040–1047. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Sánchez, A.; Ramos-Campo, D.J.; Fernández-Lobato, B.; Rubio-Arias, J.A.; Alacid, F.; Aguayo, E. Biochemical, physiological, and performance response of a functional watermelon juice enriched in l-citrulline during a half-marathon race. Food Nutr. Res. 2017, 61, 1330098. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; O’Donnell, J.M.; Starck, C.; Rutherfurd-Markwick, K.J. The effect of caffeine ingestion during evening exercise on subsequent sleep quality in females. Int. J. Sports Med. 2015, 36, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Del Coso, J.; Muñoz, G.; Muñoz-Guerra, J. Prevalence of caffeine use in elite athletes following its removal from the World Anti-Doping Agency list of banned substances. Appl. Physiol. Nutr. Metab. 2011, 36, 555–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mark Davis, J.; Zhao, Z.; Stock, H.S.; Mehl, K.A.; Buggy, J.; Hand, G.A.; Mark, J.; Mehl, K.A. Central nervous system effects of caffeine and adenosine on fatigue. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2003, 284, R399–R404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bazzucchi, I.; Felici, F.; Montini, M.; Figura, F.; Sacchetti, M. Caffeine improves neuromuscular function during maximal dynamic exercise. Muscle Nerve 2011, 43, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Mohr, M.; Nielsen, J.J.; Bangsbo, J. Caffeine intake improves intense intermittent exercise performance and reduces muscle interstitial potassium accumulation. J. Appl. Physiol. 2011, 111, 1372–1379. [Google Scholar] [CrossRef]
- Weber, A.; Herz, R. The relationship between caffeine contracture of intact muscle and the effect of caffeine on reticulum. J. Gen. Physiol. 1968, 52, 750–759. [Google Scholar] [CrossRef]
- Van Soeren, M.H.; Graham, T.E. Effect of caffeine on metabolism, exercise endurance, and catecholamine responses after withdrawal. J. Appl. Physiol. 2017, 85, 1493–1501. [Google Scholar] [CrossRef]
- Graham, T.E.; Hibbert, E.; Sathasivam, P. Metabolic and exercise endurance effects of coffee and caffeine ingestion. J. Appl. Physiol. 2017, 85, 883–889. [Google Scholar] [CrossRef]
- Gonlach, A.R.; Ade, C.J.; Bemben, M.G.; Larson, R.D.; Black, C.D. Muscle Pain as a Regulator of Cycling Intensity. Med. Sci. Sport. Exerc. 2016, 48, 287–296. [Google Scholar] [CrossRef] [PubMed]
- O’Rourke, M.P.; O’Brien, B.J.; Knez, W.L.; Paton, C.D. Caffeine has a small effect on 5-km running performance of well-trained and recreational runners. J. Sci. Med. Sport 2008, 11, 231–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiles, J.D.; Bird, S.R.; Hopkins, J.; Riley, M. Effect of caffeinated coffee on running speed, respiratory factors, blood lactate and perceived exertion during 1500-m treadmill running. Br. J. Sports Med. 1992, 26, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Clarke, N.D.; Richardson, D.L.; Thie, J.; Taylor, R. Coffee Ingestion Enhances One-Mile Running Race performance. Int. J. Sport. Physiol. Perform. 2018, 13, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.C.; Jesus, A.A.; Giglio, B.M.; Marini, A.C.; Lobo, P.C.B.; Mota, J.F.; Pimentel, G.D. Acute caffeinated coffee consumption does not improve time trial performance in an 800-m run: A randomized, double-blind, crossover, placebo-controlled study. Nutrients 2018, 10, 657. [Google Scholar] [CrossRef] [PubMed]
- Clark, I.; Landolt, H.P. Coffee, caffeine, and sleep: A systematic review of epidemiological studies and randomized controlled trials. Sleep Med. Rev. 2017, 31, 70–78. [Google Scholar] [CrossRef] [Green Version]
- Myllymäki, T.; Kyröläinen, H.; Savolainen, K.; Hokka, L.; Jakonen, R.; Juuti, T.; Martinmäki, K.; Kaartinen, J.; Kinnunen, M.L.; Rusko, H. Effects of vigorous late-night exercise on sleep quality and cardiac autonomic activity. J. Sleep Res. 2011, 20, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Nédélec, M.; Halson, S.; Abaidia, A.E.; Ahmaidi, S.; Dupont, G. Stress, Sleep and Recovery in Elite Soccer: A Critical Review of the Literature. Sport. Med. 2015, 45, 1387–1400. [Google Scholar] [CrossRef]
- Ramos-Campo, D.J.; Ávila-Gandía, V.; Luque, A.J.; Rubio-Arias, J. Effects of hour of training and exercise intensity on nocturnal autonomic modulation and sleep quality of amateur ultra-endurance runners. Physiol. Behav. 2019, 198, 134–139. [Google Scholar] [CrossRef]
- Shohet, K.L.; Landrum, R.E. Caffeine Consumption Questionnaire: A Standardized Measure for Caffeine Consumption in Undergraduate Students. Psychol. Rep. 2011, 89, 521–526. [Google Scholar] [CrossRef]
- Fitt, E.; Pell, D.; Cole, D. Assessing caffeine intake in the United Kingdom diet. Food Chem. 2013, 140, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Campo, D.J.; Sánchez, F.M.; García, P.E.; Arias, J.A.R.; Cerezal, A.B.; Clemente-Suarez, V.J.; Díaz, J.F.J. Body composition features in different playing position of professional team indoor players: Basketball, handball and futsal. Int. J. Morphol. 2014, 32, 1316–1324. [Google Scholar] [CrossRef]
- Borg, G.; Hassmén, P.; Lagerström, M. Perceived exertion related to heart rate and blood lactate during arm and leg exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1987, 56, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Åkerstedt, T.; Hume, K.; Minors, D.; Waterhouse, J. The Subjective Meaning of Good Sleep, An Intraindividual Approach Using the Karolinska Sleep Diary. Percept. Mot. Skills 2011, 79, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J.; Burke, L.M.; Dvorak, J.; Larson-Meyer, D.E.; Peeling, P.; Phillips, S.M.; Rawson, E.S.; Walsh, N.P.; Garthe, I.; Geyer, H.; et al. IOC consensus statement: Dietary supplements and the high-performance athlete. Br. J. Sports Med. 2018, 52, 439–455. [Google Scholar] [CrossRef]
- Silveira, R.; Andrade-Souza, V.A.; Arcoverde, L.; Tomazini, F.; Sansonio, A.; Bishop, D.J.; Bertuzzi, R.; Lima-Silva, A.E. Caffeine Increases Work Done above Critical Power, but Not Anaerobic Work. Med. Sci. Sports Exerc. 2018, 50, 131–140. [Google Scholar] [CrossRef]
- Wiles, J.D.; Coleman, D.; Tegerdine, M.; Swaine, I.L. The effects of caffeine ingestion on performance time, speed and power during a laboratory-based 1 km cycling time-trial. J. Sports Sci. 2006, 24, 1165–1171. [Google Scholar] [CrossRef]
- Beaumont, R.; Cordery, P.; Funnell, M.; Mears, S.; James, L.; Watson, P. Chronic ingestion of a low dose of caffeine induces tolerance to the performance benefits of caffeine. J. Sports Sci. 2017, 35, 1920–1927. [Google Scholar] [CrossRef]
- Bell, D.G.; McLellan, T.M. Exercise endurance 1, 3, and 6 h after caffeine ingestion in caffeine users and nonusers. J. Appl. Physiol. 2002, 93, 1227–1234. [Google Scholar] [CrossRef] [Green Version]
- Mora-Rodríguez, R.; Pallarés, J.G.; López-Gullón, J.M.; López-Samanes, Á.; Fernández-Elías, V.E.; Ortega, J.F. Improvements on neuromuscular performance with caffeine ingestion depend on the time-of-day. J. Sci. Med. Sport 2015, 18, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Souissi, M.; Abedelmalek, S.; Chtourou, H.; Boussita, A.; Hakim, A.; Sahnoun, Z. Effects of time-of-day and caffeine ingestion on mood states, simple reaction time, and short-term maximal performance in elite judoists. Biol. Rhythm Res. 2013, 44, 897–907. [Google Scholar] [CrossRef]
- Pickering, C.; Kiely, J. Are the Current Guidelines on Caffeine Use in Sport Optimal for Everyone? Inter-individual Variation in Caffeine Ergogenicity, and a Move Towards Personalised Sports Nutrition. Sports Med. 2018, 48, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Doherty, M.; Smith, P.M. Effects of caffeine ingestion on rating of perceived exertion during and after exercise: A meta-analysis. Scand. J. Med. Sci. Sport. 2005, 15, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Driver, H.S.; Taylor, S.R. Exercise and sleep. Sleep Med. Rev. 2000, 4, 387–402. [Google Scholar] [CrossRef]
- Erlacher, D.; Ehrlenspiel, F.; Adegbesan, O.A.; El-Din, H.G. Sleep habits in German athletes before important competitions or games. J. Sports Sci. 2011, 29, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Fullagar, H.H.K.; Skorski, S.; Duffield, R.; Hammes, D.; Coutts, A.J.; Meyer, T. Sleep and Athletic Performance: The Effects of Sleep Loss on Exercise Performance, and Physiological and Cognitive Responses to Exercise. Sports Med. 2015, 45, 161–186. [Google Scholar] [CrossRef]
- Nehlig, A.; Daval, J.L.; Debry, G. Caffeine and the central nervous system: Mechanisms of action, biochemical, metabolic and psychostimulant effects. Brain Res. Rev. 1992, 17, 139–170. [Google Scholar] [CrossRef]
- Shilo, L.; Sabbah, H.; Hadari, R.; Kovatz, S.; Weinberg, U.; Dolev, S.; Dagan, Y.; Shenkman, L. The effects of coffee consumption on sleep and melatonin secretion. Sleep Med. 2002, 3, 271–273. [Google Scholar] [CrossRef]
- Lastella, M.; Lovell, G.P.; Sargent, C. Athletes’ precompetitive sleep behaviour and its relationship with subsequent precompetitive mood and performance. Eur. J. Sport Sci. 2014, 14, 123–130. [Google Scholar] [CrossRef]
- Sondermeijer, H.P.; Van Marle, A.G.J.; Kamen, P.; Krum, H. Acute effects of caffeine on heart rate variability. Am. J. Cardiol. 2002, 90, 906–907. [Google Scholar] [CrossRef]
- Koenig, J.; Jarczok, M.N.; Kuhn, W.; Morsch, K.; Schäfer, A.; Hillecke, T.K.; Thayer, J.F. Impact of Caffeine on Heart Rate Variability: A Systematic Review. J. Caffeine Res. 2013, 3, 22–37. [Google Scholar] [CrossRef]
- Waring, W.S.; Goudsmit, J.; Marwick, J.; Webb, D.J.; Maxwell, S.R.J. Acute Caffeine Intake Influences Central More Than Peripheral Blood Pressure in Young Adults. Am. J. Hypertens. 2003, 16, 919–924. [Google Scholar] [CrossRef]
- Notarius, C.F.; Floras, J.S. Caffeine Enhances Heart Rate Variability in Middle-Aged Healthy, But Not Heart Failure Subjects. J. Caffeine Res. 2012, 2, 77–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnet, M.; Tancer, M.; Uhde, T.; Yeragani, V.K. Effects of caffeine on heart rate and QT variability during sleep. Depress. Anxiety 2005, 22, 150–155. [Google Scholar] [CrossRef]
- Nishijima, Y.; Ikeda, T.; Takamatsu, M.; Kiso, Y.; Shibata, H.; Fushiki, T.; Moritani, T. Influence of caffeine ingestion on autonomic nervous activity during endurance exercise in humans. Eur. J. Appl. Physiol. 2002, 87, 475–480. [Google Scholar] [CrossRef]
- Rauh, R.; Burkert, M.; Siepmann, M.; Mueck-Weymann, M. Acute effects of caffeine on heart rate variability in habitual caffeine consumers. Clin. Physiol. Funct. Imaging 2006, 26, 163–166. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Placebo | Caffeine | ANOVA | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Test 1 | Test 2 | Test 1 | Test 2 | ||||||||
| mean | SD | mean | SD | mean | SD | mean | SD | F | p | η2p | |
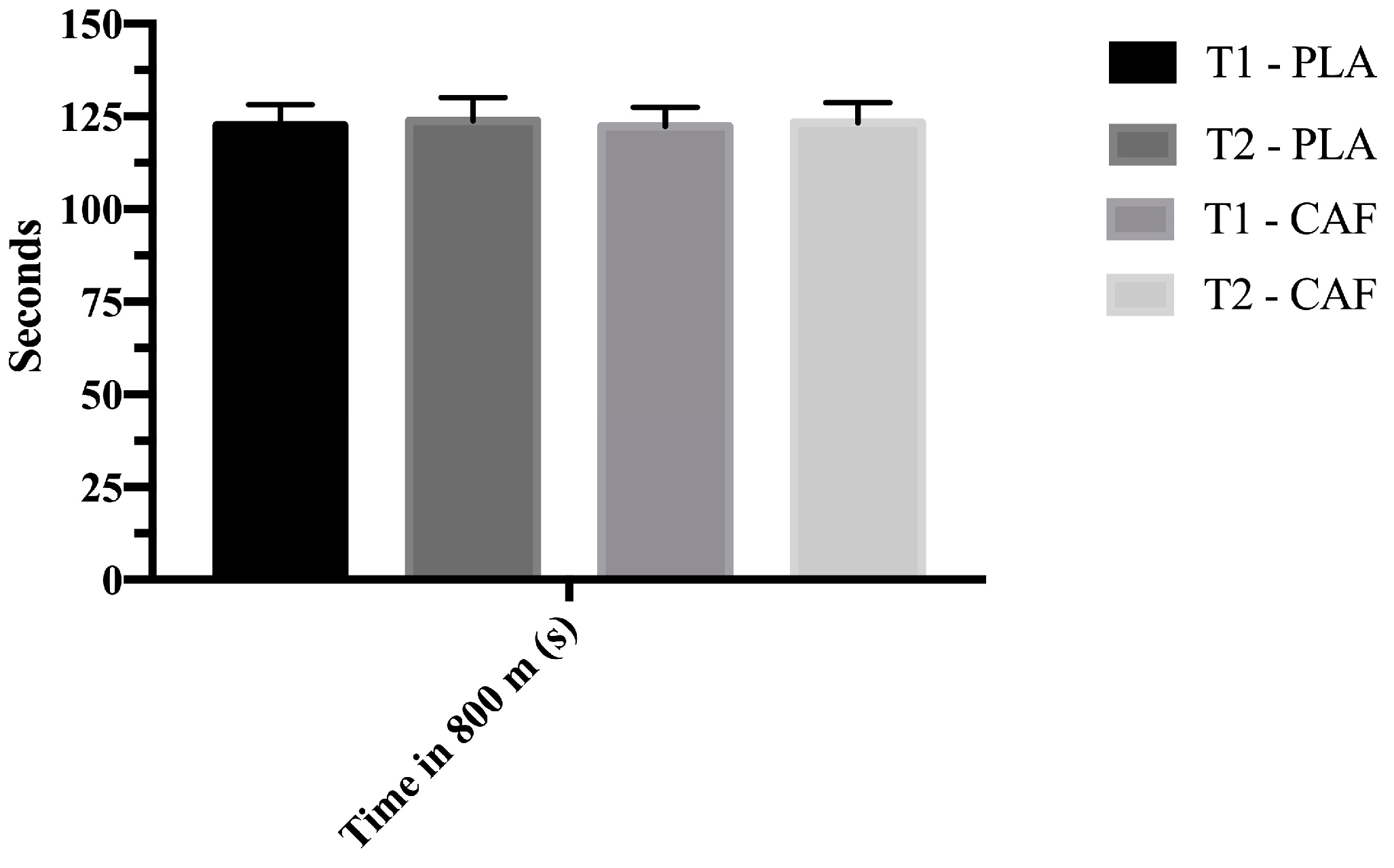
| Time in 800 m (s) | 122.6 | 5.6 | 123.8 | 6.2 | 122.3 | 5.1 | 123.3 | 5.4 | 2.317 | 0.12 | 0.15 |
| RPE (A.U) | 8.4 | 1.1 | 8.2 | 1.0 | 8.3 | 0.9 | 8.1 | 0.9 | 0.142 | 0.934 | 0.01 |
| mean HR in 800 m (bpm) | 170.4 | 9.8 | 171.4 | 10.1 | 172.7 | 10.6 | 173.2 | 9.2 | 0.625 | 0.525 | 0.06 |
| peak HR in 800 m (bpm) | 185.8 | 9.1 | 184.5 | 10.1 | 188.3 | 8.2 | 185.5 | 10.5 | 0.889 | 0.395 | 0.08 |
| CMJ (Δ cm) | −10.2 | 8.8 | −6.8 | 4.8 | −13.3 | 8.7 | −6.8 | 5.9 | 4.564 | 0.008 | 0.28 |
| Lactate (mmoL/L) | 19.1 | 4.7 | 19.0 | 4.2 | 20.1 | 4.6 | 17.8 | 4.4 | 0.979 | 0.413 | 0.07 |
| Placebo | Caffeine | Effect Size (ES) | 95% CI for ES | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p | Lower | Upper | ||
| Actigraphic sleep quality | ||||||||
| Latency (min) | 6.15 | 2.79 | 6.77 | 2.32 | 0.290 | −0.31 | −0.86 | 0.25 |
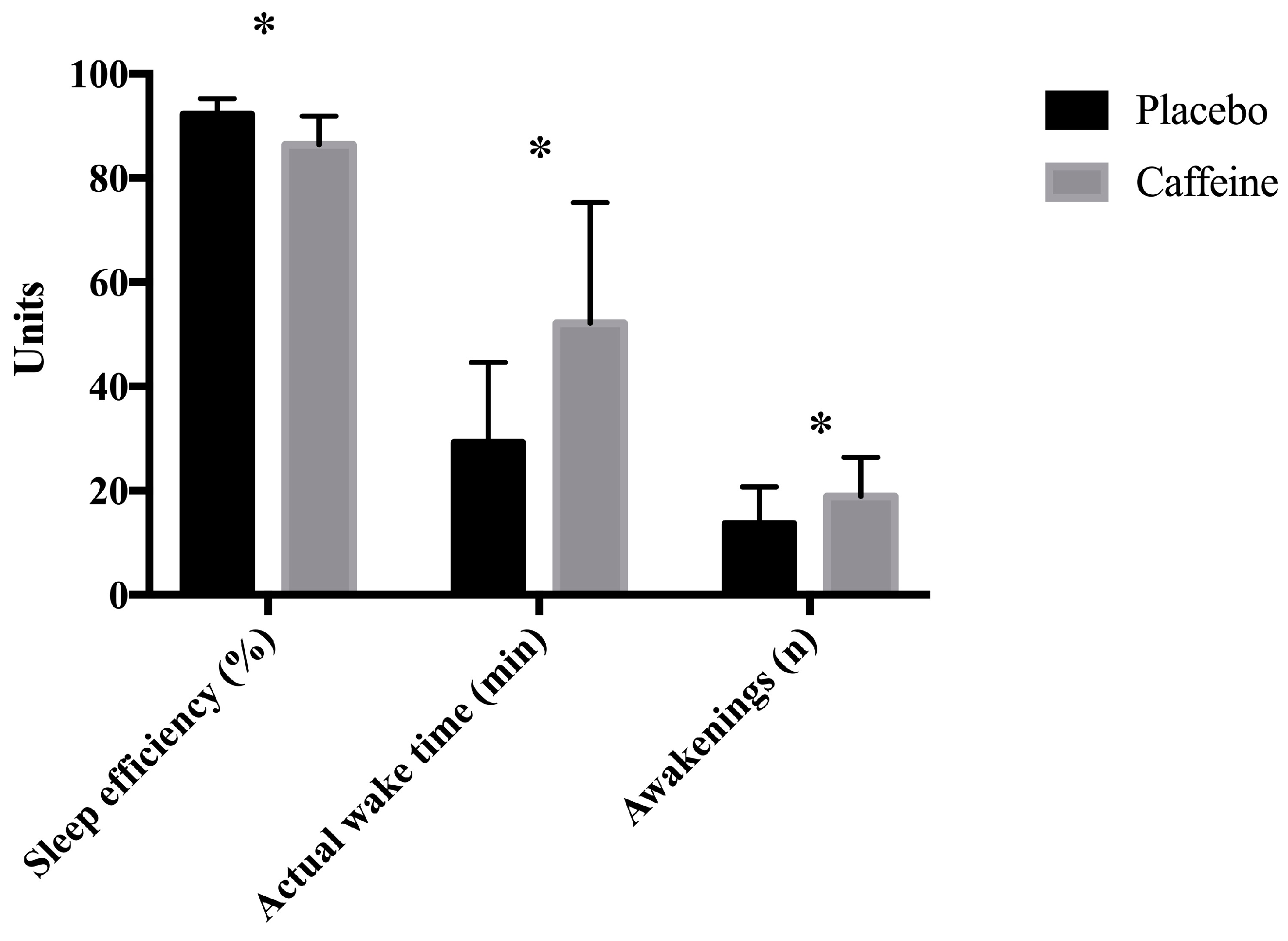
| Sleep efficiency (%) | 92.2 | 3.0 | 86.4 | 5.5 | 0.003 | 0.71 | 0.27 | 0.91 |
| Time in bed (min) | 470.2 | 118.3 | 461.2 | 128.2 | 0.641 | 0.13 | −0.42 | 0.68 |
| Actual sleep time (min) | 434.8 | 119.7 | 402.3 | 136.3 | 0.091 | 0.51 | −0.08 | 1.08 |
| Actual wake time (min) | 29.2 | 15.4 | 52.1 | 23.2 | 0.001 | −1.18 | −1.89 | −0.45 |
| Awakenings (n) | 13.62 | 7.05 | 18.85 | 7.50 | 0.005 | −0.96 | −1.61 | −0.28 |
| Average time of each awakening (min) | 2.79 | 1.90 | 3.18 | 1.72 | 0.402 | −0.24 | −0.79 | 0.32 |
| Karolinska Sleep Questionnaire | ||||||||
| Sleep quality | 3.36 | 0.75 | 2.21 | 0.98 | 0.005 | 1.11 | 0.43 | 1.77 |
| Calm sleep | 3.50 | 1.09 | 2.36 | 1.15 | 0.005 | 1.11 | 0.43 | 1.77 |
| Ease of falling asleep | 3.43 | 1.22 | 1.57 | 0.85 | 0.003 | 1.38 | 0.62 | 2.10 |
| Amount of dreaming | 1.43 | 0.76 | 1.07 | 0.48 | 0.120 | 0.48 | −0.08 | 1.03 |
| Ease of waking up | 3.43 | 0.76 | 3.14 | 0.86 | 0.395 | 0.24 | −0.30 | 0.76 |
| Feeling refreshed after awakening | 2.07 | 0.73 | 1.50 | 0.65 | 0.006 | 1.11 | 0.43 | 1.77 |
| Slept throughout the time allotted | 3.14 | 0.86 | 2.79 | 1.89 | 0.389 | 0.24 | −0.30 | 0.77 |
| Placebo | Caffeine | Effect Size (ES) | 95% CI for ES | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p | Lower | Upper | ||
| Mean R-R (ms) | 1151.5 | 114.4 | 1184.7 | 131.1 | 1.000 | −0.21 | −0.80 | 0.39 |
| SDNN (ms) | 40.4 | 7.2 | 36.5 | 6.7 | 0.102 | 0.56 | −0.58 | 0.58 |
| HR (bpm) | 52.4 | 5.7 | 51.2 | 6.1 | 1.000 | 0.58 | −0.01 | 0.87 |
| RMSSD (ms) | 27.1 | 4.1 | 26.9 | 4.0 | 0.715 | 0.11 | −0.48 | 0.70 |
| pNN50 (%) | 7.1 | 3.3 | 7.2 | 3.1 | 0.956 | −0.02 | −0.61 | 0.58 |
| LF (ms2) | 986.3 | 617.3 | 814.0 | 377.4 | 0.205 | 0.41 | −0.22 | 1.02 |
| HF (ms2) | 192.4 | 111.1 | 190.7 | 77.8 | 0.953 | 0.02 | −0.57 | 0.61 |
| TP (ms) | 1689.1 | 1094.3 | 1371.7 | 639.8 | 0.214 | 0.40 | −0.23 | 1.08 |
| LF/HF | 5.6 | 2.5 | 4.6 | 2.0 | 0.182 | 0.43 | −0.20 | 1.04 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos-Campo, D.J.; Pérez, A.; Ávila-Gandía, V.; Pérez-Piñero, S.; Rubio-Arias, J.Á. Impact of Caffeine Intake on 800-m Running Performance and Sleep Quality in Trained Runners. Nutrients 2019, 11, 2040. https://doi.org/10.3390/nu11092040
Ramos-Campo DJ, Pérez A, Ávila-Gandía V, Pérez-Piñero S, Rubio-Arias JÁ. Impact of Caffeine Intake on 800-m Running Performance and Sleep Quality in Trained Runners. Nutrients. 2019; 11(9):2040. https://doi.org/10.3390/nu11092040
Chicago/Turabian StyleRamos-Campo, Domingo Jesús, Andrés Pérez, Vicente Ávila-Gandía, Silvia Pérez-Piñero, and Jacobo Ángel Rubio-Arias. 2019. "Impact of Caffeine Intake on 800-m Running Performance and Sleep Quality in Trained Runners" Nutrients 11, no. 9: 2040. https://doi.org/10.3390/nu11092040
APA StyleRamos-Campo, D. J., Pérez, A., Ávila-Gandía, V., Pérez-Piñero, S., & Rubio-Arias, J. Á. (2019). Impact of Caffeine Intake on 800-m Running Performance and Sleep Quality in Trained Runners. Nutrients, 11(9), 2040. https://doi.org/10.3390/nu11092040