Association between Sociodemographic Factors and Dietary Patterns in Children Under 24 Months of Age: A Systematic Review

 ,
,
Abstract
1. Introduction
2. Material and Methods
2.1. Types of Studies
2.2. Types of Participants
2.3. Data Collection and Analysis
2.3.1. Search Strategy
2.3.2. Selection of Studies
2.3.3. Data Extraction and Management
2.3.4. Assessment of Potential Bias in Included Studies
2.3.5. Data Synthesis
3. Results
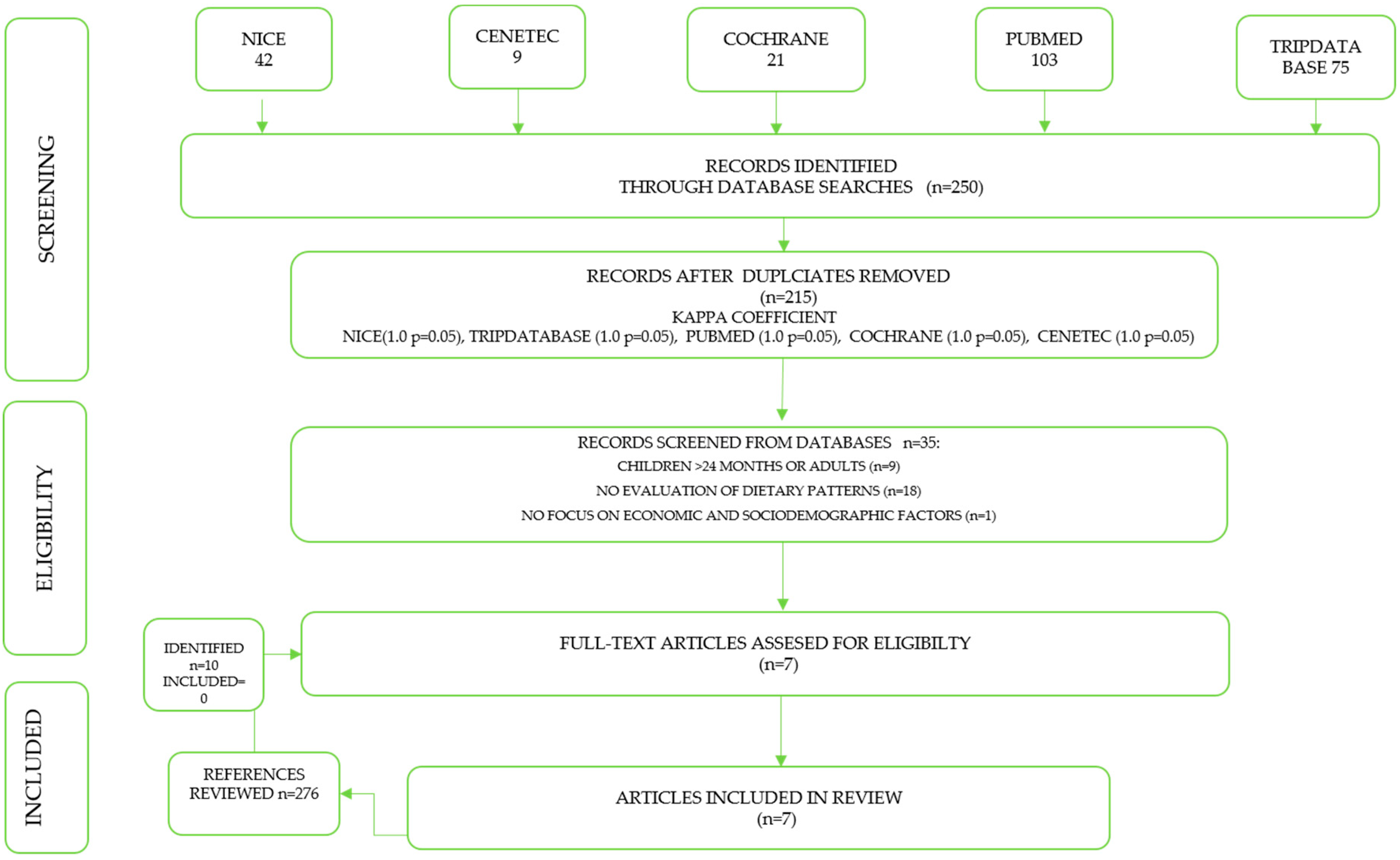
3.1. Results of the Search and Study Selection
3.2. Included Studies
3.3. Dietary Patterns Analysis
3.4. Associations between Sociodemographic Factors and Dietary Patterns
3.5. Risk of Bias in the Studies Included
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Panamerican Health Organization. Guiding Principles for Complementary Feeding of the Breastfed Child; PAHO/WHO: Washington, DC, USA, 2001. [Google Scholar]
- Panamerican Health Organization; WHO. Principios de Orientación Para la Alimentación de Niños no Amamantados Entre Los 6 y los 24 Meses de Edad; OPS: Washington, DC, USA, 2007; ISBN 978-92-7-532795-1. [Google Scholar]
- WHO. Infant and young child feeding. In Model Chapter for Textbooks for Medical Students and Allied Health Professionals; World Health Organization: Geneva, Switzerland, 2009; ISBN 9789241597494. [Google Scholar]
- Pantoja-Mendoza, I.Y.; Meléndez, G.; Guevara, C.M.; Serralde, Z.A.E. Review of complementary feeding practices in Mexican children. Nutr. Hosp. 2015, 31, 552–558. [Google Scholar]
- Dewey, K.G.; Adu-Afarwuah, S. Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Matern. Child Nutr. 2008, 4, 24–85. [Google Scholar] [CrossRef] [PubMed]
- Aggett, P.J.; Agostoni, C.; Axelsson, I.; Bresson, J.L.; Goulet, O.; Hernell, O.; Koletzko, B.; Lafeber, H.L.; Michaelsen, K.F.; Micheli, J.L.; et al. Iron Metabolism and Requirements in Early Childhood: Do We Know Enough?: A Commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2002, 34, 337–345. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Assessing and managing children at primary health-care facilities to prevent overweight and obesity in the context of the double burden of malnutrition. In Updates for the Integrated Management of Childhood Illness (IMCI); World Health Organization: Geneva, Switzerland, 2017; ISBN 978-92-4-155012-3. [Google Scholar]
- Qu, P.; Zhang, Y.; Li, J.; Zhang, R.; Yang, J.; Lei, F.; Li, S.; Liu, D.; Dang, S.; Yan, H. Complementary feeding patterns among ethnic groups in rural Western China. J. Zheijiang (Biomed. Biotech.) 2018, 19, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Emmett, P.M. Dietary patterns during complementary feeding and later outcomes. Nestle Nutr. Inst. Workshop Ser. 2016, 85, 145–154. [Google Scholar]
- Rocha, N.P.; Milagres, L.C.; Longo, G.Z.; Ribeiro, A.Q.; Novaes, J.F. Association between dietary pattern and cardiometabolic risk in children and adolescents: A systematic review. J. Pediatr. (Rio J). 2017, 93, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Nwaru, B.I.; Onyeka, I.N.; Ndiokwelu, C.H.; Esangbedo, D.O.; Ngwu, E.K.; Okolo, S.N. Maternal and child dietary patterns and their determinants in Nigeria. Matern. Child Nutr. 2015, 11, 283–296. [Google Scholar] [CrossRef]
- Kant, A.K. Dietary patterns and health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef]
- Smithers, L.G.; Golley, R.K.; Brazionis, L.; Lynch, J.W. Characterizing whole diets of young children from developed countries and the association between diet and health: A systematic review. Nutr. Rev. 2011, 69, 449–467. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Sonnenberg, L.; Pencina, M.; Kimokoti, R.; Quatromoni, P.; Nam, B.H.; D’Angostino, R.; Meigs, J.B.; Ordovas, J.; Cobain, M.; Millen, B. Dietary patterns and the metabolic syndrome in obese and non-obese Framingham women. Obes. Res. 2005, 13, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Cao, X.; Harris, R.; Hennis, A.J.; Wu, S.Y.; Leske, M.C.; Barbados National Cancer Study Group. Assessing dietary patterns in Barbados highlights the need for nutritional intervention to reduce the risk of chronic disease. J. Hum. Nutr. Diet. 2008, 21, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Schwedhelm, C.; Iqbal, K.; Knüppel, S.; Schwingshack, L.; Boeing, H. Contribution to the understanding of how principal component analysis–derived dietary patterns emerge from habitual data on food consumption. Am. J. Clin. Nutr. 2018, 107, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Monroy, C.L.; Vidal, R.S.; Saade, H.A. Cap II. Análisis de clases latentes. In Análisis de Clases Latentes. Una Técnica Para Detectar Heterogeneidad en Poblaciones; Cuaderno Técnico 2, 1st ed.; Centro Nacional de Evaluación para la Educación Superior, A.C. (Ceneval): México, México, 2010; Volume 2, pp. 19–27. [Google Scholar]
- Zwick, W.R.; Velicer, W.F. Factors Influencing Four Rules for Determining the Number of Components To Retain. Multivar. Behav. Res. 1982, 17, 253–269. [Google Scholar] [CrossRef] [PubMed]
- Denova, G.E.; Méndez, S.L.; Muñoz, A.P.; Tucker, K.L.; Clark, P. Dietary Patterns, Bone Mineral Density, and Risk of Fractures: A Systematic Review and Meta-Analysis. Nutrients. 2018, 10, 1922. [Google Scholar] [CrossRef]
- Bradley, R.H.; Robert, F.; Corwyn, R.F. Socioeconomic Status and Child Development. Annu. Rev. Psychol. 2002, 53, 371–399. [Google Scholar] [CrossRef] [PubMed]
- Manyanga, T.; Tremblay, M.S.; Chaput, J.P.; Katzmarzyk, P.T.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; Maher, C.; et al. Socioeconomic status and dietary patterns in children from around the world: Different associations by levels of country human development? BMC Public Health 2017, 17, 457. [Google Scholar] [CrossRef]
- Northstone, K.; Smith, A.D.A.C.; Newby, P.K.; Emmett, P.M. Longitudinal comparisons of dietary patterns derived by cluster analysis in 7- to 13-year-old children. Br. J. Nutr. 2013, 109, 2050–2058. [Google Scholar] [CrossRef]
- Lioret, S.; Betoko, A.; Forhan, A.; Charles, M.A.; Heu, B.; de Guillain, B.L.; The EDEN Mother–Child Cohort Study Group. Dietary Patterns Track from Infancy to Preschool Age: Cross-Sectional and Longitudinal Perspective. J. Nutr. 2015, 145, 775–782. [Google Scholar]
- Mayen, A.L.; Vidal, M.P.; Paccaud, F.; Bovet, P.; Stringhini, S. Socioeconomic determinants of dietary patterns in low- and middle income countries: A systematic review. Am. J. Clin. Nutr. 2014, 100, 1520–1523. [Google Scholar] [CrossRef]
- Robinson, S.; Marriot, L.; Poole, J.; Crozier, S.; Borland, S.; Lawrence, W.; Law, C.; Godfrey, K.; Cooper, C.; Inskip, H.; et al. Dietary patterns in infancy: The importance of maternal and family influences on feeding practice. Br. J. Nutr. 2007, 98, 1029–1037. [Google Scholar] [CrossRef] [PubMed]
- García, C.C.G.; Rodríguez, R.S.; Rivera, J.A.; Monterrubio, F.E.; Tucker, K.L. Sociodemographic factors are associated with dietary patterns in Mexican schoolchildren. Public Health Nutr. 2017, 21, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Wall, C.R.; Gammon, C.S.; Bandara, D.K.; Grant, C.C.; Atatoa Carr, P.E.; Morton, S. Dietary patterns in pregnancy in New Zealand—Influence of maternal socio-demographic, health and lifestyle factors. Nutrients 2016, 8, 300. [Google Scholar] [CrossRef] [PubMed]
- Procter, S.B.; Campbell, C.G. Position of the Academy of Nutrition and Dietetics: Nutrition and Lifestyle for a Healthy Pregnancy Outcome. J. Acad. Nutr. Diet. 2014, 114, 1099–1103. [Google Scholar] [CrossRef] [PubMed]
- Dourado Villa, J.K.; Souza, S.T.S.; Ribeiro, A.Q.; e Silva, A.R.; da Rocha Sant’Ana, L.F.; Pessoa, M.C. Dietary patterns of children and socioeconomical, behavioral and maternal determinants. Rev. Paul. Pediatr. 2015, 33, 302–309. [Google Scholar]
- Durao, C.; Severo, M.; Olveira, A.; Moreira, P.; Guerra, A.; Barros, H.; Lopes, C. Association of maternal characteristics and behaivours with 4 year old children’s dietary patterns. Matern. Child Nutr. 2016, 13, 1–16. [Google Scholar]
- Nobre, L.N.; Lamounier, J.A.; Franceshini, S.C. Preschool children dietary patterns and associated factors. J. Pediatr. (Rio J.). 2012, 88, 129–136. [Google Scholar] [CrossRef][Green Version]
- Santos, L.P.; Assuncao, M.C.; Matijasevich, A.; Santos, I.S.; Barros, A.J. Dietary intake patterns of children aged 6 years and their association with socioeconomic and demographic characteristics, early feeding practices and body mass index. BMC Public Health 2016, 16, 1055. [Google Scholar] [CrossRef]
- Galvan, P.M.; Sánchez, E.; Cárdenas, C.M.; Karam, R.; Claudio, L.; Cruz, M.; Burguete, G.A. Dietary patterns in Mexican children and adolescents: Characterization and relation with socioeconomic and home environment factors. Appetite 2018, 121, 275–284. [Google Scholar] [CrossRef]
- Zarnowiecki, D.M.; Parletta, N.; Dollman, J. The role of socio-economic position as a moderator of children’s healthy food intake. Br. J. Nutr. 2014, 112, 830–840. [Google Scholar] [CrossRef]
- Affret, A.; Severi, G.; Dow, C.; Rey, G.; Delpierre, C.; Boutron-Ruault, M.C.; Clavel, C.F.; Fagherazzi, G. Socio-economic factors associated with healthy diet: Results from the E3N study. Public Health Nutr. 2017, 20, 1574–1583. [Google Scholar] [CrossRef] [PubMed]
- Mais, L.A.; Warkentin, S.; Vega, J.B.; Latorre, M.D.R.D.O.; Carnell, S.; Taddei, J.A.A.C. Sociodemographic, anthropometric and behavioural risk factors for ultra-processed food consumption in a sample of 2–9 year olds in Brazil. Public Health Nutr. 2018, 21, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, A.E.M.; Conde, W.L. Secular trends in dietary patterns of young children in Brazil from 1996 to 2006. Public Heakth Nutr. 2017, 20, 2937–2945. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Birch, L.L.; Fisher, J.O. Development of eating behaviors among children and adolescents. Pediatrics 1998, 101, 539–549. [Google Scholar] [PubMed]
- Zhen, S.; Ma, Y.; Zhao, Z.; Yang, X.; Wen, D. Dietary pattern is associated with obesity in Chinese children and adolescents: Data from China Health and Nutrition Survey (CHNS). Nutr. J. 2018, 17. [Google Scholar] [CrossRef] [PubMed]
- Ong, H.; Meng, M.; Wei, L.; Xiawei, Z.; Wan, M.C. Chinese Children at a Crossroads: Influence of Family Socioeconomic Factors on Diet Patterns. Ecol. Food Nutr. 2010, 49, 247–261. [Google Scholar] [CrossRef]
- Emmett, P.M.; Jones, L.R.; Northstone, K. Dietary patterns in the Avon Longitudinal Study of Parents and Children. Nutr. Rev. 2015, 73, 207–230. [Google Scholar] [CrossRef]
- Wall, C.R.; Thompson, J.M.D.; Robinson, E.; Mitchell, E.A. Dietary patterns of children at 3.5 and 7 years of age: A New Zealand birth cohort study. Acta Paediatr. 2013, 102, 137–142. [Google Scholar] [CrossRef]
- Davison, B.; Saeedi, P.; Black, K.; Harrex, H.; Haszard, J.; Meredith, J.K.; Quigg, R.; Skeaff, S.; Stoner, L.; Wong, J.E.; et al. The association between parent diet quality and child dietary patterns in nine to eleven year old children from Dunedin, New Zeland. Nutrients 2017, 11, 483. [Google Scholar] [CrossRef]
- Peltner, J.; Thiele, S. Convenience-based food purchase patterns: Identification an associations with dietary quality, sociodemographic factors and attitudes. Public Health Nutr. 2018, 21, 558–570. [Google Scholar] [CrossRef]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Fidler, M.N.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. JPGN 2017, 64, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Hohman, E.E.; Pau, I.M.; Birch, L.L.; Savage, J.S. INSIGHT responsive parenting intervention is associated with healthier patterns of dietary exposures in infants. Obesity 2017, 25, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Smithers, L.G.; Brazionis, L.; Golley, R.K.; Mittinty, M.N.; Northstone, K.; Emmett, P.; Mc Naughton, S.A.; Campbell, K.J.; Lynch, J.W. Associations between dietary patterns at 6 and 15 months of age and sociodemographic factors. Eur. J. Clin. Nutr. 2012, 66, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Bell, L.K.; Golley, R.K.; Daniels, L.; Magarey, A.M. Dietary patterns of Australian children aged 14 and 24 months and associations with socio-demographic factors and adiposity. Eur. J. Clin. Nutr. 2013, 67, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Chelsea, M.R.; Savage, J.S.; Birch, L.L. Patterns of early dietary exposures have implications for maternal and child weight outcomes. Obesity 2016, 24, 430–438. [Google Scholar] [CrossRef]
- Kiefte de Jong, J.C.; de Vries, J.H.; Bleeker, S.E.; Jaddoe, V.W.V.; Hofman, A.; Raat, H.; Moll, H.A. Socio-demographic and lifestyle determinants of Western-like and “Health conscious” dietary patterns in toddlers. Br. J. Nutr. 2013, 109, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Miyake, Y.; Sasaki, S.; Tanaka, K.; Murakami, K.; Hirota, Y.; Osaka maternal and Child Health Study Group. Dietary patterns in infancy and their associations with maternal socio-economic and lifestyle factors among 758 Japanese mother–child pairs: The Osaka Maternal and Child Health Study. Matern. Child Nutr. 2012, 10, 1–13. [Google Scholar] [CrossRef]
- Wen, X.; Kong, K.L.; Eiden, R.D.; Sharma, N.N.; Xie, C. Sociodemographic differences and Infant Dietary Patterns. Pediatrics 2014, 134, e1387. [Google Scholar] [CrossRef]
- Arikpo, D.; Edet, E.S.; Chibuzo, M.T.; Odey, F.; Caldewell, D.M. Educational interventions for improving primary caregiver complementary feeding practices for children aged 24 months and under. Cochrane Database Syst. Rev. 2018, 18, CD011768. [Google Scholar] [CrossRef]
- Miller, L.C.; Neena, J.; Lohani, M.; Rogers, B.; Mahato, S.; Ghosh, S.; Webb, P. Women’s education level amplifies the effects of a livelihoods-based intervention on household wealth, child diet, and child growth in rural Nepal. Int. J. Equity Health 2017, 16, 183. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Darmstadt, G.L.; Hasan, B.S.; Haws, R.A. Community-based interventions for improving perinatal and neonatal health outcomes in developing countries: A review of the evidence. Pediatrics 2005, 115, 519–617. [Google Scholar] [CrossRef] [PubMed]
- Wamani, H.; Tylleskar, T.; Astrom, A.N.; Tumwine, J.K.; Peterson, S. Mothers’ education but not fathers’ education, household assets or land ownership is the best predictor of child health inequalities in rural Uganda. Int. J. Equity Health 2004, 3, 9. [Google Scholar] [CrossRef] [PubMed]
- Showell, N.N.; Jennings, J.M.; Johnson, K.A.; Perin, J.; Thornton, R.L.J. Where Children Live: Examining Whether Neighborhood Crime and Poverty Is Associated with Overweight and Obesity Among Low-Income Preschool-Aged Primary Care Patients. Front. Pediatr. 2019, 6, 433. [Google Scholar] [CrossRef] [PubMed]
- Hidaka, B.H.; Kerling, E.H.; Thodosoff, J.M.; Sullivan, D.K.; Colombo, J.; Carlson, S. Dietary patterns of early childhood and maternal socioeconomic status in a unique prospective sample from a randomized controlled trial of Prenatal DHA Supplementation. BMC Pediatr. 2016, 16, 191. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, A.N.; Kaji, A.; Felker-Kantor, E.; Bazzano, L.A.; Potts, K.S. Qualitative Studies of Infant and Young Child Feeding in Lower-Income Countries: A Systematic Review and Synthesis of Dietary Patterns. Nutrients 2017, 9, 1140. [Google Scholar] [CrossRef] [PubMed]
- An, R.; Yang, Y.; Hoschke, A.; Xue, H.; Wang, Y. Influence of neighborhood safety on childhood obesity: A systematic review and meta-analysis of longitudinal studies. Obes. Rev. 2017, 18, 1289–1309. [Google Scholar] [CrossRef] [PubMed]
- De Fragas, H.P.; Santos, M.J.; Altenburg de Assis, M.A.; Bertazzi, L.R.; Peres, M.A.; Perazi, M. Dietary Patterns of Children and Adolescents from High, Medium and Low Human Development Countries and Associated Socioeconomic Factors: A Systematic Review. Nutrients 2018, 10, 436. [Google Scholar] [CrossRef]
- Dowle, K.M.; Kilner, K.; Burley, V.; Soltani, H. Differences in dietary pattern by maternal age in the Born in Bradford cohort: A comparative analysis. PLoS ONE 2018, 13, e0208879. [Google Scholar] [CrossRef]
- Cárdenas, V.V.M.; Ortiz, F.R.E.; Cortés-Castell, E.; Miranda, F.P.E.; Guevara, V.M.C.; Rizo-Baez, M.M. Características maternas e infantiles asociadas a obesidad en lactantes menores de un año de edad del norte de México. Nutr. Hosp. 2018, 35, 1024–1032. [Google Scholar]
- Kracht, C.H.L.; Swyden, K.J.; Weedn, A.E.; Salvatore, A.L.; Terry, R.A.; Sisson, S.B. A Structural Equation Modelling Approach to Understanding Influences of Maternal and Family Characteristics on Feeding Practices in Young Children. Curr. Dev. Nutr. 2018, 2, 1–8. [Google Scholar] [CrossRef]
- Tripicchio, G.L.; Keller, K.L.; Johnson, C.; Pietrobelli, A.; Heo, M.; Faith, M.S. Differential maternal feeding practices, eating self-regulation, and adiposity in young twins. Pediatrics 2014, 134, 1399–1404. [Google Scholar] [CrossRef]
- Novakovic, R.; Cavelaars, A.; Geelen, A.; Nikolic, M.; Altaba, I.I.; Viñas, B.R. Socio-economic determinants of micronutrient intake and status in Europe: A systematic review. Public Health Nutr. 2013, 17, 1031–1045. [Google Scholar] [CrossRef]
- Alvisi, P.; Brusa, S.; Alboresi, S.; Amarri, S.; Bottau, P.; Cavagni, G.; Corradini, B.; Landi, L.; Loroni, L.; Marani, M.; et al. Recommendations on complementary feeding for healthy, full-term infants. Ital. J. Pediatr. 2015, 41, 36. [Google Scholar] [CrossRef]
- Vilela, S.; Severo, M.; Moreira, T.; Ramos, E.; Lopes, C. Evaluation of a short food frequency questionnaire for dietary intake assessment among children. Eur. J. Clin. Nutr. 2018, 73, 679–691. [Google Scholar] [CrossRef]
- Pitt, E.; Cameron, C.M.; Thornto, L.; Gallegos, D.; Filus, A.; Ng, S.K.; Comans, T. Dietary patterns of Australian children at three and five years of age and their changes over time: A latent class and latent transition analysis. Appetite 2018, 129, 207–216. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Country | Sample Size | Age | Dietary Pattern Name and Food Contents |
|---|---|---|---|---|
| Bell LK et al., 2013 [49] | Australia | Infants 14 months: 552 Infants 24 months: 493 | 14 and 24 months | 14 months Core foods: fruit, grains, no white bread, vegetables, cheese, eggs, nuts and seeds. Basic combination: white bread, milk and (non-core) spreads, juices, ice cream, food and beverages with no fruit or vegetables. 24 months Core foods: fruit, grains, non-white bread vegetables, cheese, eggs, walnuts, seeds, and water. Non-core food: (energy-dense, low-nutrient, sugars); sweetened beverages, spreads, high-fat fried/processed potatoes, snacks, chocolate, processed meat. |
| Chelsea MR et al., 2016 [50] | United States | Infants 1071 | Infants 9 months | Breastfeeding (BF) Breastfeeding, fruits and vegetables (BFFV). Characterized by high probability of breastfeeding, fruits and vegetables, and low probability of high energy density. Breastfeeding low variety (BFLV). Represented by high probability of breastfeeding, low probability of fruits and vegetables and low variety. Formula Feeding (FF) Milk formula feeding, fruits and vegetables (FFFV). Characterized by high probability of fruits and vegetables, and low probability of energy-dense food. Milk formula feeding low variety (FFLV). Represented by high probability of formula, low probability of fruit and vegetable, and low food variety. Mixed: FF, low in fruits and vegetables and high probability of energy-dense food. |
| Smithers LG et al., 2012 [48] | England | Infants 6 months: 5129 Infants of 15 months: 3998 | Infants 6 and 15 months | 6 months Meat, vegetables, and desserts (vegetables cooked at home, potatoes, meat, fish, fruit or milk pudding, eggs). Biscuits, sweets, crisps: biscuits, chocolate, tea, sweets, bread, cola, fizzy drinks. Pre-made baby foods (commercial products, canned/jarred meat, processed meat), fruit puddings, vegetables or milk pudding, fish. Breastfeeding: breastfeeding, raw fruits and vegetables. 15 months Herbs, raw fruit and vegetables: legumes, raw vegetables, fruit, cheese, spices. Biscuits, sweets and crisps: fizzy drinks, sweets, crisps, biscuits, ketchup. Pre-made baby foods: rice cereal, rusks, baby meat, baby vegetables, baby milk and fruit pudding. Dorsal meat, vegetables and desserts. high consumption of meat products, home-cooked potatoes, milk puddings and vegetables. |
| Hohman EE et al., 2017 [47] | United States | 279 | Children 9 months | (BFV) Breastfeeding, fruits and vegetables. (BLV) Breastfeeding, low variety. (FFV) Milk formula, fruits and vegetables. (FLV) Milk formula, low variety. (FHED) Energy-dense food, juice, milk formula, sweetened drinks, French fries and sweetened food. |
| Kiefte de JJC et al., 2012 [51] | The Netherlands | 2420 | Children 14 months | Health conscious: fruits, vegetables, legumes, fish. Western-like: savory snacks, animal fats, confectionery, sweetened drinks. |
| Okubo H. et al., 2012 [52] | Japan | 758 | Infants from 16 to 24 months | Fruits, vegetables and high-protein foods: basic food, meat, fish, eggs, vegetables, fruits, yoghurt, green tea, Oolong tea. Confectionaries and sweetened beverages: fresh fruit juice, sweetened fruit juice, puddings, jellies, chocolate, rice crackers. |
| Xiaozhong W. et al., 2014 [53] | United States | 1378 | Infants from 6 to 12 months | High, sugar, fat, and protein pattern: sweetened drinks, sweetened food, French fries, fish/shellfish, nut products, eggs. Infant guideline solids: baby cereals, fruit, vegetables, meat/chicken. Formula. High dairy/regular cereal: cow’s milk, dairy products, fruit and vegetable juice, non-baby cereals/starches. |
| Reference | Country | Study Location | Sample Size | Age Range | Diet Assessment Method/Dietary Pattern Method | Dietary Pattern Identified | Economic and Sociodemographic Factors Assessed | Association of Economic and Sociodemographic Factors and Dietary Patterns. |
|---|---|---|---|---|---|---|---|---|
| Bell LK et al., 2013 [49] | Australia | Brisbane, Adelaide, South of Australia | Infants 14 months: 552 Infants 24 months: 493 | 14 and 24 months | Multiple-pass 24-h recall/Principal Component Analysis (PCA)-factor analysis (varimax rotation). | 14 months: “core food”, “basic combination” 24 months: “core food”, “non-core food” | Maternal: education level, age (during delivery), smoking during pregnancy, breastfeeding duration, marital status, weight, parity, economic status (decile), Australian nationality. | 14 months Higher education levels (university) were associated with high consumption of “core food”. Younger mothers at time of delivery and smokers were conversely associated with the “basic combination pattern”. 24 months Australian nationality and younger mothers were associated with “non-core food”. |
| Chelsea MR et al., 2016 [50] | Unites States | Atlanta, Georgia | 1071 | 9 months | Food Frequency Questionnaire (FFQ)/Class latent analysis | “Breastfeeding, fruit and vegetables” (BFFV), “Breastfeeding low variety” (BFLV) “Milk formula feeding, fruits and vegetables” (FFFV), “Milk formula feeding low variety” (FFLV) Mixed: “high energetic density” | Maternal: parity, age, excessive weight-gain, body mass index before pregnancy, ethnic group, education level, household income, postpartum depression, marital status. | Hispanic vs. non-Hispanic white race/ethnicity mothers were associated with “fruits and vegetables “and “formula feeding and low variety”. Multiparity was associated with “formula feeding and low variety patterns”. High school education or less was associated with both “formula feeding and low variety” and “mixed patterns”. Low household income was associated with the “formula feeding and fruit and vegetables pattern”. |
| Smithers LG et al., 2012 [48] | England | Avon (South-West of England) | Infants 6 months: 5129 Infants 15 months: 3998 | Infants 6 and 15 months | Questionnaire not validated/PCA-factor analysis | 6 months: 1. ”Meat, vegetables, desserts”; 2. “Biscuits, sweets, crisps”; 3. “Pre-made baby food”; 4. “Breastfeeding”. 15 months: 1. “Herbs, raw fruit and vegetables”; 2. “Biscuits, sweets and crisps”; 3. “Pre-made baby food”; 4. “Dorsal meat, vegetables and desserts”. | Maternal: education, age, social class, smoking, number of children, marital status, and body mass index. | 6 months Infants from mothers with higher education levels were positively associated with dietary pattern 1. Younger mothers, with lower levels of education who smoked during pregnancy had higher body mass index and a larger number of children were positively associated with dietary pattern 2. Younger mothers, lower education and smoking during pregnancy were positively associated with dietary pattern 3. At 15 months Older mothers with higher education levels were positively associated with dietary pattern 1, however, older, unmarried mothers who only had one child scored highly for dietary pattern 3. Maternal body mass index ≥ 30 kg/m2 was associated with high dietary pattern 2 scores. Being married was associated with low pattern 4 scores. |
| Hohman EE et al., 2017 [47] | United States | Pennsylvania | 279 | 9 months | FFQ/class latent analysis | “Breastfeeding, fruit and vegetables (BFV)” “Breastfeeding, low variety (BLV)” “Milk formula, fruits and vegetables (FFV)” “Milk formula, low variety (FLV)” “Milk formula, high energetic density food” (FHED). | Mother’s education level, age, household income, marital status, gestational weight gain, prenatal body mass index, return to work after 3 months. | Older, high-income, married, and high education-level mothers were less associated with milk formula, low variety and milk formula, high energetic density food. High pre-pregnancy body mass index was associated with milk formula, low variety and milk formula, and high energetic density food. Milk formula, low variety was associated with mothers who returned to work at 3 months. No differences were found between weight gain during pregnancy, child sex, body weight at birth (Z score), and use of childcare. |
| Kiefte de JJC et al., 2012 [51] | Holland | Rotterdam | 2420 | Children 14 months | FFQ/PCA-factor analysis (varimax rotation). | “Health conscious”, “Western-like” | Mother’s education, household income, marital status, smoking during pregnancy, alcoholism during pregnancy, prenatal body mass index, energy intake before pregnancy, number of children, arterial hypertension, hypercholesterolemia, paternal education, paternal body mass index, paternal diabetes, arterial hypertension, paternal age, smoking. | Low paternal education, low household income, parental smoking, high maternal body mass index during pregnancy, high intake of carbohydrates, and multiparity were associated with the “Western-like pattern”. High fiber intake during pregnancy and older parents were conversely associated with the “Western-like pattern”. Folic acid intake during pregnancy, high fiber maternal diet, and single parenthood were positively associated with the “healthy pattern”. Mothers who consumed alcohol during pregnancy and had a history of comorbidity, and those with daughters, were less associated to the “health conscious” pattern. |
| Okubo H. et al., 2012 [52] | Japan | Neyagawa Osaka | 758 | Infants from 16 to 24 months | Self-administered questionnaire/PCA-factor analysis (varimax rotation). Cluster analysis. | “Fruit, vegetables and high-protein foods” “Confectionaries and sweetened beverages” | Maternal age, pre-pregnancy body mass index, education (years), employment status, household income, family structure, married (yes/no), number of infants’ older siblings, cigarette smoking during pregnancy, physical activity, maternal dietary pattern. | Unemployed mothers, daily smokers during pregnancy, lower education levels, lower household income, higher number of children, were associated with “confectionary and sweetened beverages”. Non-smokers during pregnancy, high education levels, longer duration of breastfeeding, full-time employment, and higher household income with a rice, fish and vegetable intake pattern were less associated with “confectionary and sweetened beverages”. Mothers with more than 13 years of education and a rice, fish, and vegetable dietary pattern, were less associated with “confectionary and sweetened beverages”. |
| Xiaozhong W. et al., 2014 [53] | United States | Buffalo, New York | 1378 1275 | Infants from 6 to 12 months | Surveys/PCA-factor analysis (varimax rotation). | “High sugar, fat and protein pattern”, “infant guideline solids”, “formula milk”, “high dairy and regular cereal”. | Maternal: age, ethnicity, education level, married (yes/no), employment (yes/no), parity, gestational diabetes, gestational weight gain, pre-gestational body mass index, household income. | Low household income, maternal non-Hispanic Afro-American ethnicity, low education level, high body mass index were associated with the “high sugar, fat and protein dietary pattern. High household income, maternal non-Hispanic, white ethnicity, and high education were associated with “Infant guideline solids”. Emergency cesarean-section, higher maternal age, Asian-pacific ethnicity, and low gestational weight gain were associated with the “formula, baby cereal dietary pattern”. Vaginal non-induced, maternal non-Hispanic, white race/ethnicity, low education, being employed, and obesity were associated with “high dairy and regular cereal dietary pattern”. |
| Author, Year, and Country of Study | Title | Source Type | Objective | Study Design, Analysis Method (AM) | Setting and Sample Size | Assessment of Methodological Limitations of Study (STROBE)/Quality of the Evidence using the Nomenclature of the GRADE Manual Valued at: High ⨁⨁⨁⨁; Moderate ⨁⨁⨁ ◯; Low ⨁⨁ ◯◯; and Very Low ⨁ ◯◯◯. |
|---|---|---|---|---|---|---|
| Bell LK et al., 2013, Australia [49] | Dietary patterns of Australian children aged 14 and 24 months, and associations with socio-demographic factors and adiposity | Journal: European Journal of Clinical Nutrition | To describe dietary patterns of Australian children aged 14 and 24 months; identify socio-demographic factors behind dietary patterns; examine associations between dietary patterns and child adiposity. | Secondary analysis, longitudinal study. Dietary patterns were extracted using Principal component analysis (PCA). | Purposive sampling, subjects were recruited in a two-stage process; mothers delivering healthy infants (37-week gestation, 2500 g) were approached for permission to be re-contacted approximately 3 months later for full enrolment in the study, 1 045 subjects. | No explanation regarding sample size calculation, interactions, missing data treatment. No information on loss of participants, and no flow chart/diagram shown. Moderate ⨁⨁⨁ ◯ |
| Chelsea MR et al., 2016, United States, [50] | Patterns of Early Dietary Exposures Have Implications for Maternal and Child Weight Outcomes | Journal: Obesity | To identify distinct classes of infant dietary patterns at 9 months using latent class analysis; identify maternal and infant characteristics associated with infant dietary patterns; test whether infant dietary class membership is associated with child and maternal weight. | Cohort study, latent class analysis was used to identify discrete, mutually exclusive latent classes, based on 9-month Food Frequency Questionnaire (FFQ) data. | Convenience sampling, women were recruited late in pregnancy to participate in the IFPS II project, conducted in 2005. All data were self-reported by mothers on mailed surveys, 1 807 continued participation through 1 year. | No explanation of possible bias in sources, interactions, and missing data treatment. No information on sampling methods, on loss of participants, and no flow chart/diagram or information on approval from the ethics committee shown. Moderate ⨁⨁⨁ ◯ |
| Smithers LG et al., 2012, England, [48] | Associations between dietary patterns at 6 and 15 months of age and sociodemographic factors | Journal: Journal of Clinical Nutrition | To describe dietary patterns in early life and their associations with maternal and infant sociodemographic characteristics. | Cohort study, PCA was used to explore latent diet patterns on a continuous scale. | Convenience sampling, all pregnant women residing in Avon, southwest England, were invited to participate. The core ALSPAC sample consists of 14,541 pregnancies with 13,988 infants alive at 1 year. | No explanation regarding sample size calculation, interactions, missing data treatment. No information on loss of participants. Moderate ⨁⨁⨁ ◯ |
| Hohman EE et al., 2017, United States, [47] | INSIGHT Responsive Parenting Intervention is Associated with Healthier Patterns of Dietary Exposures in Infants | Journal: Pediatric Obesity | INSIGHT study: Latent class analysis (LCA) approach to identify patterns of milk and complementary feeding in 9-month-old infants., Explored the relationship between the BMI and the effect of maternal and infant characteristics on dietary pattern class membership, determine whether dietary pattern class membership differed between RP and control groups. | Cohort study. LCA was used and based on the infant FFQ data. | Primiparous mothers-newborns dyads (n = 291) were randomized to the intervention INSIGHT, RP or control. Latent class analysis identified patterns of dietary exposure at 9 months (cohort). | No explanation of interactions, missing data treatment. No explanation of source bias. Moderate ⨁⨁⨁ ◯ |
| Kiefte de JJC et al., 2012, Holland, [51] | Socio-demographic and lifestyle determinants of ‘Western-like’ and ‘Health conscious’ dietary patterns in toddlers | Journal: British Journal of Nutrition | To identify common dietary pattern in toddlers and to explore parental and child indicators of these dietary patterns. | Cohort prospective study, principal component analysis and varimax method by maximizing the sum of the variance of the loading components was used. | Convenience sampling the study was embedded in a population-based prospective cohort study in Rotterdam, the Netherlands. In total, 9778 mothers with a delivery date between April 2002 and January 2006 were enrolled but only 3643 (72%) were eligible for analysis. | No explanation of interactions, missing data treatment, loss of participants or confusion factors. No explanation of source bias. Moderate ⨁⨁⨁ ◯ |
| Okubo H. et al., 2012, Japan, [52] | Dietary patterns in infancy and their associations with maternal socio-economic and lifestyle factors among 758 Japanese mother–child pairs: the Osaka Maternal and Child Health Study | Journal: Maternal and Child Nutrition | To identify dietary patterns in US infants at ages of 6 and 12 months, sociodemographic differences in these patterns, and their associations with infant growth from ages of 6 to 12 months. | Prospective cohort study. First, they adopted an a posteriori approach, using principal component analysis. Second, they conducted several runs with the number of clusters varied from two to six. | Purposive sampling all pregnant women in the Osaka Prefecture, were recruited between 2001 and 2003. Of 3639 eligible women, 627 (17.2%) agreed to participate in the survey. An additional 375 pregnant women living in other municipalities were also enrolled between 2001 and 2003. The final analysis consisted of 758 mother–child pairs. | No explanation about statistical methods used to control confusion factors, subjects were not randomly sampled, no explanation about missing data treatment, and they assumed high bias risks sources, and lack of precision on some study variables (socio-economic status). Very low ⨁ ◯◯◯. |
| Xiaozhong W. et al., 2014, United States, [53] | Sociodemographic Differences and Infant Dietary Patterns | Journal: Pediatrics | To identify dietary patterns among infants aged 16–24 months, and the influence of maternal socio-economic and lifestyle characteristics on identified dietary patterns. | Secondary analysis—longitudinal study. Principal component analysis and Orthogonal transformation (varimax) to rotate the original derived components were used. | Purposive sampling, this longitudinal study followed pregnant women from late pregnancy through their infant’s first year of life. The original study sample consisted of 4902 pregnant women and 3033 full-term newborns. The final growth analysis only included the 530 infants who had complete data. | No explanation of statistical methods used to control confusion factors. No explanation of missing data treatment. Moderate ⨁⨁⨁ ◯ |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez-Camacho, C.; Méndez-Sánchez, L.; Klünder-Klünder, M.; Clark, P.; Denova-Gutiérrez, E. Association between Sociodemographic Factors and Dietary Patterns in Children Under 24 Months of Age: A Systematic Review. Nutrients 2019, 11, 2006. https://doi.org/10.3390/nu11092006
Gutiérrez-Camacho C, Méndez-Sánchez L, Klünder-Klünder M, Clark P, Denova-Gutiérrez E. Association between Sociodemographic Factors and Dietary Patterns in Children Under 24 Months of Age: A Systematic Review. Nutrients. 2019; 11(9):2006. https://doi.org/10.3390/nu11092006
Chicago/Turabian StyleGutiérrez-Camacho, Claudia, Lucia Méndez-Sánchez, Miguel Klünder-Klünder, Patricia Clark, and Edgar Denova-Gutiérrez. 2019. "Association between Sociodemographic Factors and Dietary Patterns in Children Under 24 Months of Age: A Systematic Review" Nutrients 11, no. 9: 2006. https://doi.org/10.3390/nu11092006
APA StyleGutiérrez-Camacho, C., Méndez-Sánchez, L., Klünder-Klünder, M., Clark, P., & Denova-Gutiérrez, E. (2019). Association between Sociodemographic Factors and Dietary Patterns in Children Under 24 Months of Age: A Systematic Review. Nutrients, 11(9), 2006. https://doi.org/10.3390/nu11092006