Significant Decrease in Childhood Obesity and Waist Circumference over 15 Years in Switzerland: A Repeated Cross-Sectional Study


Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Design
2.2. Enrollment and Participation
2.3. Anthropometric Measures
2.4. Assessment of Predictors for Obesity
2.5. Data Analysis
3. Results
3.1. Recruitment Statistics of the Obesity Survey 2017/18
3.2. Inter- and Intra-Observer Variability in the Obesity Survey 2017/18
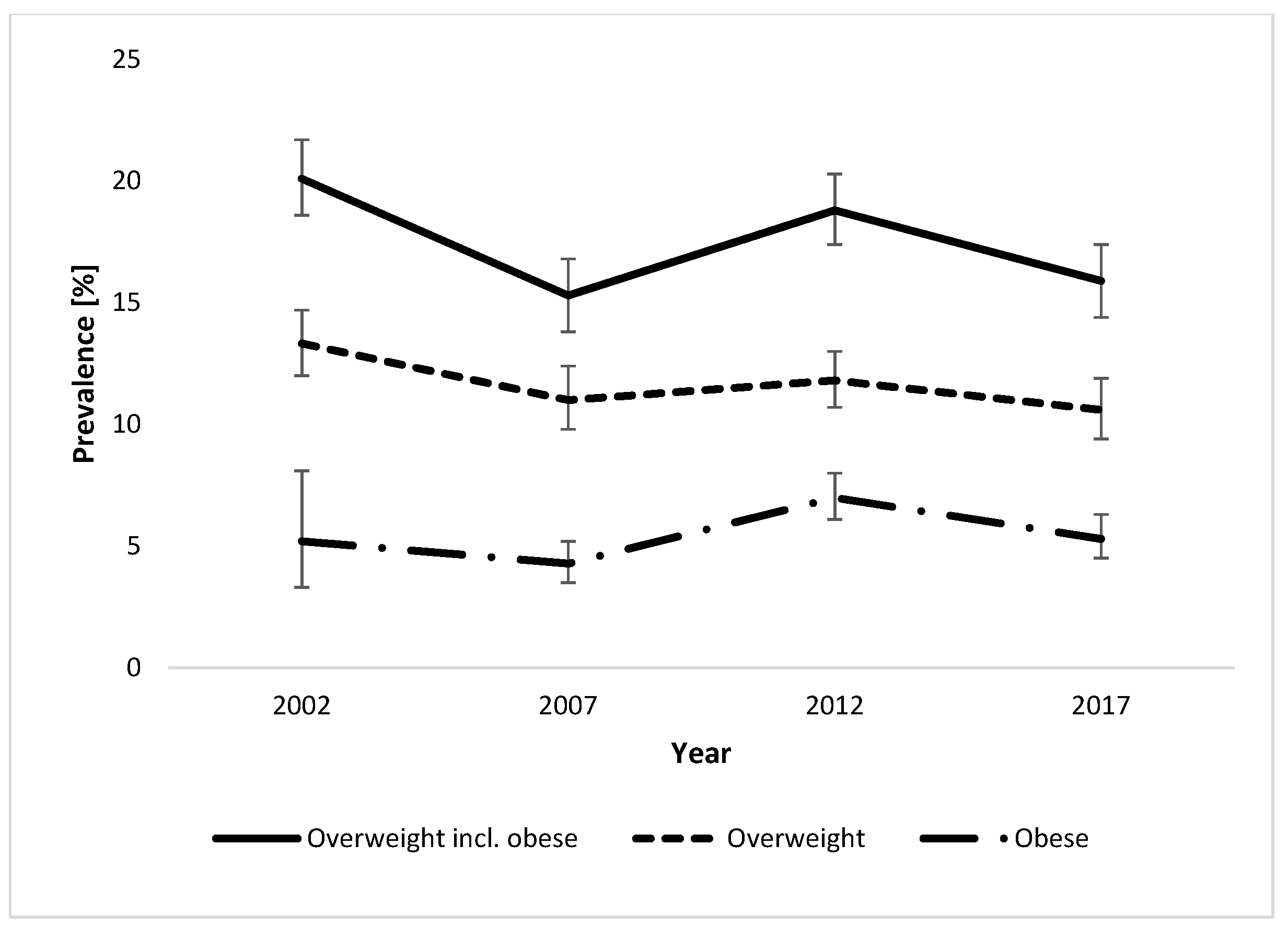
3.3. Trends in Overweight and Obesity Prevalence between 2002 and 2017/18
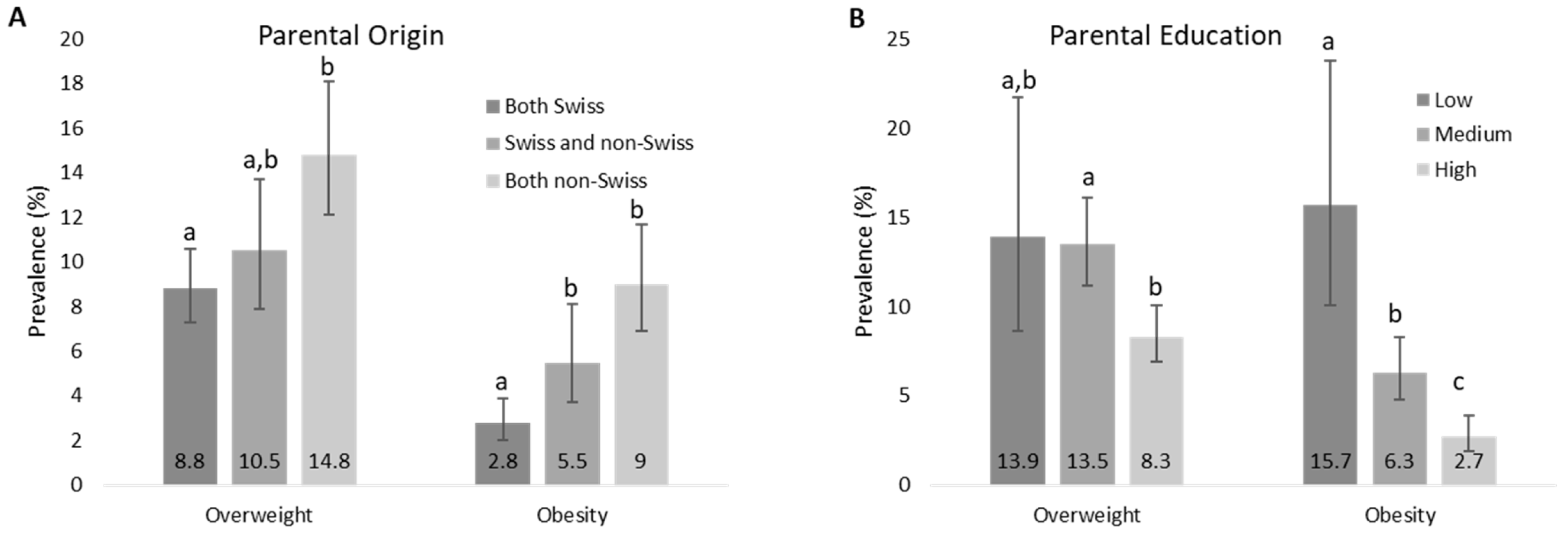
3.4. Predictors for the Development of Overweight and Obesity in 2017/18
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Habib, S.H.; Saha, S. Burden of non-communicable disease: Global overview. Diabetes Metab. Syndr. Clin. Res. Rev. 2010, 4, 41–47. [Google Scholar] [CrossRef]
- Park, M.H.; Falconer, C.; Viner, R.M.; Kinra, S. The impact of childhood obesity on morbidity and mortality in adulthood: A systematic review. Obes. Rev. 2012, 13, 985–1000. [Google Scholar] [CrossRef]
- Singhal, A. The role of infant nutrition in the global epidemic of non-communicable disease. Proc. Nutr. Soc. 2016, 75, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef]
- Singh, A.; Bassi, S.; Nazar, G.P.; Saluja, K.; Park, M.; Kinra, S.; Arora, M. Impact of school policies on non-communicable disease risk factors—A systematic review. BMC Public Health 2017, 17, 292. [Google Scholar]
- Hedley, A.A.; Ogden, C.L.; Johnson, C.L.; Carroll, M.D.; Curtin, L.R.; Flegal, K.M. Prevalence of Overweight and Obesity Among US Children, Adolescents, and Adults, 1999–2002. JAMA 2004, 291, 2847. [Google Scholar] [CrossRef]
- Seidell, J.C. Obesity in Europe: Scaling an epidemic. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 1995, 19, 1–4. [Google Scholar]
- Flegal, K.M.; Ogden, C.L.; Wei, R.; Kuczmarski, R.L.; Johnson, C.L. Prevalence of overweight in US children: Comparison of US growth charts from the Centers for Disease Control and Prevention with other reference values for body mass index. Am. J. Clin. Nutr. 2001, 73, 1086–1093. [Google Scholar] [CrossRef]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity among Adults and Youth: United States, 2015–2016. In NCHS Data Brief no 288; National Center for Health Statistics: Hyattswille, MD, USA, 2017. [Google Scholar]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Dong, Y.; Jan, C.; Ma, Y.; Dong, B.; Zou, Z.; Yang, Y.; Xu, R.; Song, Y.; Ma, J.; Sawyer, S.M.; et al. Economic development and the nutritional status of Chinese school-aged children and adolescents from 1995 to 2014: An analysis of five successive national surveys. Lancet Diabetes Endocrinol. 2019, 7, 288–299. [Google Scholar] [CrossRef]
- Bann, D.; Johnson, W.; Li, L.; Kuh, D.; Hardy, R. Socioeconomic inequalities in childhood and adolescent body-mass index, weight, and height from 1953 to 2015: An analysis of four longitudinal, observational, British birth cohort studies. Lancet Public Health 2018, 3, e194–e203. [Google Scholar] [CrossRef]
- Organisation for Economic Co-operation and Development. OECD(2017) Obesity Update; Organisation for Economic Co-operation and Development: Paris, France, 2017. [Google Scholar]
- Olds, T.; Maher, C.; Zumin, S.; Péneau, S.; Lioret, S.; Castetbon, K.; Bellisle; De Wilde, J.; Hohepa, M.; Maddison, R.; et al. Evidence that the prevalence of childhood overweight is plateauing: Data from nine countries. Pediatr. Obes. 2011, 6, 342–360. [Google Scholar] [CrossRef]
- Murer, S.B.; Saarsalu, S.; Zimmermann, M.B.; Aeberli, I. Pediatric adiposity stabilized in Switzerland between 1999 and 2012. Eur. J. Nutr. 2013, 53, 865–875. [Google Scholar] [CrossRef]
- Boesch, S.; Lobstein, T.; Brinsden, H.; Ralston, J.; Bull, F.; Willumsen, J.; Brance, F.; Engesveen, K.; Grummer-Strawn, L.M.; Nishida, C.; et al. Taking Action on Childhood Obesity; World Health Organization: Geneva, Switzerland; World Obesity: London, UK, 2018. [Google Scholar]
- Reinehr, T. Lifestyle intervention in childhood obesity: Changes and challenges. Nat. Rev. Endocrinol. 2013, 9, 607–614. [Google Scholar] [CrossRef]
- Kirschenbaum, D.S.; Gierut, K.J. Five Recent Expert Recommendations on the Treatment of Childhood and Adolescent Obesity: Toward an Emerging Consensus—A Stepped Care Approach. Child. Obes. 2013, 9, 376–385. [Google Scholar] [CrossRef]
- Bourke, M.; Whittaker, P.J.; Verma, A. Are dietary interventions effective at increasing fruit and vegetable consumption among overweight children? A systematic review. J. Epidemiol. Community Health 2014, 68, 485–490. [Google Scholar] [CrossRef]
- Vos, M.B.; Welsh, J. Childhood Obesity: Update on Predisposing Factors and Prevention Strategies. Curr. Gastroenterol. Rep. 2010, 12, 280–287. [Google Scholar] [CrossRef] [Green Version]
- Murer, S.B.; Saarsalu, S.; Zimmermann, J.; Herter-Aeberli, I. Risk factors for overweight and obesity in Swiss primary school children: Results from a representative national survey. Eur. J. Nutr. 2015, 55, 621–629. [Google Scholar] [CrossRef]
- Knai, C.; Lobstein, T.; Darmon, N.; Rutter, H.; McKee, M. Socioeconomic Patterning of Childhood Overweight Status in Europe. Int. J. Environ. Res. Public Health 2012, 9, 1472–1489. [Google Scholar] [CrossRef] [Green Version]
- Keane, E.; Layte, R.; Harrington, J.; Kearney, P.M.; Perry, I.J. Measured Parental Weight Status and Familial Socio-Economic Status Correlates with Childhood Overweight and Obesity at Age 9. PLoS ONE 2012, 7, e43503. [Google Scholar] [CrossRef]
- Aeberli, I.; Ammann, R.S.; Knabenhans, M.; Molinari, L.; Zimmermann, M.B. Decrease in the prevalence of paediatric adiposity in Switzerland from 2002 to 2007. Public Health Nutr. 2010, 13, 806–811. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Aeberli, I.; Torresani, T.; Bürgi, H. Increasing the iodine concentration in the Swiss iodized salt program markedly improved iodine status in pregnant women and children: A 5-y prospective national study. Am. J. Clin. Nutr. 2005, 82, 388–392. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Gübeli, C.; Püntener, C.; Molinari, L. Overweight and obesity in 6–12 year old children in Switzerland. Swiss Med. Wkly. 2004, 134, 523–528. [Google Scholar]
- Zimmermann, M.B.; Gübeli, C.; Püntener, C.; Molinari, L. Detection of overweight and obesity in a national sample of 6–12-y-old Swiss children: Accuracy and validity of reference values for body mass index from the US Centers for Disease Control and Prevention and the International Obesity Task Force. Am. J. Clin. Nutr. 2004, 79, 838–843. [Google Scholar] [CrossRef]
- Gibson, R.S. Nutritional Assessment: A Laboratory Manual; Oxford University Press: Oxford, UK, 1993; pp. 79–100. [Google Scholar]
- Ulijaszek, S.J.; Kerr, D.A. Anthropometric measurement error and the assessment of nutritional status. Br. J. Nutr. 1999, 82, 165–177. [Google Scholar] [CrossRef] [Green Version]
- Ogden, C.L.; Kuczmarski, R.J.; Flegal, K.M.; Mei, Z.; Guo, S.; Wei, R.; Grummer-Strawn, L.M.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. Centers for Disease Control and Prevention 2000 Growth Charts for the United States: Improvements to the 1977 National Center for Health Statistics Version. Pediatrics 2002, 109, 45–60. [Google Scholar] [CrossRef] [Green Version]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240. [Google Scholar] [CrossRef]
- World Health Organization. WHO Child Growth Standards and the Identification of Severe Acute Malnutrition in Infants and Children; World Health Organization/UNICEF: Geneva, Switzerland, 2009. [Google Scholar]
- Aeberli, I.; Gut-Knabenhans, M.; Kusche-Ammann, R.S.; Molinari, L.; Zimmermann, M.B. Waist circumference and waist-to-height ratio percentiles in a nationally representative sample of 6–13 year old children in Switzerland. Swiss Med. Wkly. 2011, 141, 13227. [Google Scholar] [CrossRef]
- Deurenberg, P.; Pieters, J.J.L.; Hautvast, J.G.A.J. The assessment of the body fat percentage by skinfold thickness measurements in childhood and young adolescence. Br. J. Nutr. 1990, 63, 293–303. [Google Scholar] [CrossRef] [Green Version]
- Wilson, E.B. Probable Inference, the Law of Succession, and Statistical Inference. J. Am. Stat. Assoc. 1927, 22, 209–212. [Google Scholar] [CrossRef]
- Newcombe, R.G. Two-sided confidence intervals for the single proportion: Comparison of seven methods. Stat. Med. 1998, 17, 857–872. [Google Scholar] [CrossRef]
- Bancej, C.; Jayabalasingham, B.; Wall, R.W.; Rao, D.P.; Do, M.T.; De Groh, M.; Jayaraman, G.C. Trends and projections of obesity among Canadians. Health Promot. Chronic Dis. Prev. Can. 2015, 35, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Keß, A.; Spielau, U.; Beger, C.; Gausche, R.; Vogel, M.; Lipek, T.; Körner, A.; Pfäffle, R.; Kiess, W. Further stabilization and even decrease in the prevalence rates of overweight and obesity in German children and adolescents from 2005 to 2015: A cross-sectional and trend analysis. Public Health Nutr. 2017, 20, 3075–3083. [Google Scholar] [CrossRef] [PubMed]
- Wijnhoven, T.M.; Van Raaij, J.M.; Spinelli, A.; Starc, G.; Hassapidou, M.; Spiroski, I.; Rutter, H.; Martos, E.; Rito, A.I.; Hovengen, R.; et al. WHO European Childhood Obesity Surveillance Initiative: Body mass index and level of overweight among 6–9-year-old children from school year 2007/2008 to school year 2009/2010. BMC Public Health 2014, 14, 806. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Switzerland (Gesundheitsförderung Schweiz). Monitoring of Weight Data from School Physicians in the Towns of Basel, Bern and Zurich (Monitoring der Gewichtsdaten der schulärztlichen Dienste der Städte Basel, Bern und Zürich); Factsheet 20; Health Promotion Switzerland: Bern, Switzerland, 2017. (In German) [Google Scholar]
- FOPH. Looking Back, Looking Ahead: The National Programme on Diet and Physical Activity. Spectra-Prevention and Health Promotion 2017. Available online: http://www.spectra-online.ch/spectra/themen/rueckblick-n-ausblick-das-nationale-programm-fuer-ernaehrung-und-bewegung-596-10.html (accessed on 8 February 2019).
- Crosbie, A.; Eichner, J.; Moore, W. Body Mass Index Screening and Volunteer Bias. Ann. Epidemiol. 2008, 18, 602–604. [Google Scholar] [CrossRef]
- Ebenegger, V.; Marques-Vidal, P.M.; Nydegger, A.; Laimbacher, J.; Niederer, I.; Bürgi, F.; Giusti, V.; Bodenmann, P.; Kriemler, S.; Puder, J.J. Independent contribution of parental migrant status and educational level to adiposity and eating habits in preschool children. Eur. J. Clin. Nutr. 2011, 65, 210–218. [Google Scholar] [CrossRef]
- Lasserre, A.M.; Chiolero, A.; Cachat, F.; Paccaud, F.; Bovet, P. Overweight in Swiss Children and Associations With Children’s and Parents’ Characteristics. Obesity 2007, 15, 2912–2919. [Google Scholar] [CrossRef]
- Will, B.; Zeeb, H.; Baune, B.T. Overweight and obesity at school entry among migrant and German children: A cross-sectional study. BMC Public Health 2005, 5, 45. [Google Scholar] [CrossRef]
- De Wilde, J.A.; Van Dommelen, P.; Middelkoop, B.J.; Verkerk, P.H. Trends in overweight and obesity prevalence in Dutch, Turkish, Moroccan and Surinamese South Asian children in the Netherlands. Arch. Dis. Child. 2009, 94, 795–800. [Google Scholar] [CrossRef]
- Furthner, D.; Ehrenmüller, M.; Biebl, A.; Lanzersdorfer, R.; Halmerbauer, G.; Auer-Hackenberg, L.; Schmitt, K. Gender differences and the role of parental education, school types and migration on the body mass index of 2930 Austrian school children. Wien. Klin. Wochenschr. 2017, 129, 786–792. [Google Scholar] [CrossRef]
- Conolly, A.; Davies, B. Health Survey for England 2017—Adult and Child Overweight and Obesity; NHS Digital, NHS: Leeds, UK, 2018. [Google Scholar]
- Sundblom, E.; Petzold, M.; Rasmussen, F.; Callmer, E.; Lissner, L. Childhood overweight and obesity prevalences levelling off in Stockholm but socioeconomic differences persist. Int. J. Obes. 2008, 32, 1525–1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lioret, S.; Touvier, M.; Dubuisson, C.; Dufour, A.; Lafay, L.; Volatier, J.-L.; Maire, B.; Calamassi-Tran, G.; Calamassi-Tran, G. Trends in Child Overweight Rates and Energy Intake in France From 1999 to 2007: Relationships With Socioeconomic Status. Obesity 2009, 17, 1092–1100. [Google Scholar] [CrossRef] [PubMed]
- Groth, M.V.; Fagt, S.; Brøndsted, L. Social determinants of dietary habits in Denmark. Eur. J. Clin. Nutr. 2001, 55, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Johansson, L.; Thelle, D.S.; Solvoll, K.; Bjørneboe, G.-E.A.; Drevon, C.A. Healthy dietary habits in relation to social determinants and lifestyle factors. Br. J. Nutr. 1999, 81, 211–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubois, L.; Farmer, A.; Girard, M.; Peterson, K. Social factors and television use during meals and snacks is associated with higher BMI among pre-school children. Public Health Nutr. 2008, 11, 1267–1279. [Google Scholar] [CrossRef] [Green Version]
- Janssen, I.; Katzmarzyk, P.T.; Boyce, W.F.; Vereecken, C.; Mulvihill, C.; Roberts, C.; Currie, C.; Pickett, W.; The Health Behaviour in School-Aged Children Obesity Working Group. Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obes. Rev. 2005, 6, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Kosti, R.I.; Panagiotakos, D.B.; Mihas, C.C.; Alevizos, A.; Zampelas, A.; Mariolis, A.; Tountas, Y. Dietary habits, physical activity and prevalence of overweight/obesity among adolescents in Greece: The Vyronas study. Med. Sci. Monit. 2007, 13, 437–444. [Google Scholar]
- Hills, A.; Andersen, L.B.; Byrne, N.M. Physical activity and obesity in children. Br. J. Sports Med. 2011, 45, 866–870. [Google Scholar] [CrossRef] [Green Version]
- Rito, A.; Wijnhoven, T.M.A.; Rutter, H.; Carvalho, M.A.; Paixao, E.; Ramos, C.; Claudio, D.; Espanca, R.; Sancho, T.; Cerqueira, Z.; et al. Prevalence of obesity among Portuguese children (6–8 years old) using three definition criteria: COSI Portugal, 2008. Pediatr. Obes. 2012, 7, 413–422. [Google Scholar] [CrossRef]
- Binkin, N.; Fontana, G.; Lamberti, A.; Cattaneo, C.; Baglio, G.; Perra, A.; Spinelli, A. A national survey of the prevalence of childhood overweight and obesity in Italy. Obes. Rev. 2010, 11, 2–10. [Google Scholar] [CrossRef]
- Meigen, C.; Keller, A.; Gausche, R.; Kromeyer-Hauschild, K.; Blüher, S.; Kiess, W.; Keller, E. Secular trends in body mass index in German children and adolescents: A cross-sectional data analysis via CrescNet between 1999 and 2006. Metabolism 2008, 57, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Sjöberg, A.; Lissner, L.; Mårild, S.; Albertsson-Wikland, K.; Albertsson-Wikland, K. Recent anthropometric trends among Swedish school children: Evidence for decreasing prevalence of overweight in girls. Acta Paediatr. 2008, 97, 118–123. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 2002 | 2007 | 2012 | 2017/18 | |
|---|---|---|---|---|
| N | 2493 | 2218 | 2963 | 2279 |
| Sex (n (%)) | ||||
| Boys | 1231 (49.4) | 1082 (48.8) | 1499 (50.6) | 1144 (50.2) |
| Girls | 1262 (50.6) | 1136 (51.2) | 1464 (49.4) | 1135 (49.8) |
| Age (y) | 9.9 (6.2–13.0) a | 10.1 (6.3–13.0) | 9.9 (6.3–13.0) | 9.5 (6.0–12.9) |
| Weight (kg) | 32.7 (17.7–94.4) | 33.2 (15.9–83.3) | 32.7 (16.7–132.3) | 33.1 (16.7–106.2) |
| Height (m) | 1.39 ± 0.120 b | 1.40 ± 0.116 | 1.39 ± 0.117 | 1.38 ± 0.111 |
| BMI (kg/m2) | 17.1 (12.5–35.0) | 16.9 (12.3–34.7) | 16.9 (12.4–42.7) | 17.2 (11.9–42.5) |
| Body fat (%) | 18.2 ± 9.0 | - | 19.3 ± 9.5 | 17.1 ± 8.0 |
| Waist circumference (cm) | - | 64.0 ± 8.0 | 63.2 ± 9.0 | 59.7 ± 7.1 |
| Nr of schools | 57 | 60 | 58 | 60 |
| Response rate (%) | 76 | 73 | 95 | 55 |
| 2002 (n = 2493) | 2007 (n = 2218) | 2012 (n = 2963) | 2017/18 (n = 2279) | |
|---|---|---|---|---|
| Overweight including obesity | ||||
| Total | 20.1 (18.6–21.7) a | 15.3 (13.8–16.8) b | 18.8 (17.4–20.3) a | 15.9 (14.4–17.4) b |
| Boys | 21.0 (18.8–23.4) a | 17.2 (15.1–19.6) b,c | 20.0 (18.1–22.1) a,c | 17.1 (15.1–19.4) b |
| Girls | 19.3 (17.2–21.5) a | 13.5 (11.6–15.6) b,* | 17.5 (15.6–19.5) a,c | 14.7 (12.8–16.9) b,c |
| Overweight | ||||
| Total | 13.3 (12.0–14.7) a | 11.0 (9.8–12.4) b | 11.8 (10.7–13.0) a,b | 10.6 (9.4–11.9) b |
| Boys | 13.4 (11.6–15.4) a | 11.8 (10.0–13.9) a | 12.1 (10.6–13.9) a | 10.8 (9.1–12.7) a |
| Girls | 13.3 (11.5–15.3) a | 10.2 (8.6–12.1) b | 11.5 (10.0–13.2) a,b | 10.4 (8.8–12.3) b |
| Obesity | ||||
| Total | 6.8 (5.9–7.9) a | 4.3 (3.5–5.2) b | 7.0 (6.1–8.0) a | 5.3 (4.5–6.3) b |
| Boys | 7.6 (6.2–9.3) a | 5.4 (4.2–6.9) b | 7.9 (6.7–9.4) a | 6.3 (5.0–7.9) a,b |
| Girls | 6. (4.8–7.5) a | 3.3 (2.4–4.5) b,* | 6.0 (4.9–7.4) a,* | 4.3 (3.3–5.7) a,b,* |
| Central adiposity | ||||
| Total | - | 12.0 (10.7–13.4)a | 18.4 (17.0–19.8)b | 6.3 (5.4–7.4) c |
| Boys | - | 11.5 (9.7–13.5)a | 18.3 (16.5–20.4)b | 7.3 (5.9–8.9)c |
| Girls | - | 12.5 (10.7–14.6)a | 18.4 (16.5–20.5)b | 5.3 (4.1–6.8)c |
| Healthy Weight | Overweight | Obese | |||||
|---|---|---|---|---|---|---|---|
| % | % | OR (95% CI) | p | % | OR (95% CI) | p | |
| Parental origin | |||||||
| Both non-Swiss | 23.3 | 35.8 | 1.695 (1.161–2.474) | 0.006 | 47.1 | 2.037 (1.152–3.602) | 0.014 |
| Swiss and non-Swiss | 19.8 | 19.5 | 1.236 (0.819–1.864) | 0.313 | 22.1 | 1.754 (0.952–3.231) | 0.072 |
| Both Swiss | 56.9 | 44.7 | 0 | 30.8 | 0 | ||
| Parental education | |||||||
| Low | 4.4 | 7.0 | 1.319 (0.662–2.630) | 0.431 | 17.7 | 3.118 (1.458–6.666) | 0.003 |
| Medium | 35.3 | 47.7 | 1.721 (1.245–2.377) | 0.001 | 50.0 | 1.945 (1.181–3.204) | 0.009 |
| High | 60.2 | 45.3 | 0 | 32.3 | 0 | ||
| Physical activity | |||||||
| ≤1 day | 3.6 | 7.0 | 2.203 (1.058–4.588) | 0.035 | 12.5 | 5.073 (2.083–12.355) | <0.001 |
| 2–3 days | 23.2 | 36.7 | 2.238 (1.476–3.392) | <0.001 | 43.3 | 3.307 (1.755–6.231) | <0.001 |
| 4–5 days | 39.5 | 34.5 | 1.387 (0.927–2.078) | 0.112 | 28.8 | 1.393 (0.714–2.717) | 0.331 |
| ≥6 days | 33.6 | 21.8 | 15.4 | ||||
| Sex | |||||||
| Girls | 50.5 | 49.0 | 0.824 (0.604–1.124) | 0.222 | 40.5 | 0.554 (0.350–0.879) | 0.012 |
| Boys | 49.5 | 51.0 | 59.5 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herter-Aeberli, I.; Osuna, E.; Sarnovská, Z.; Zimmermann, M.B. Significant Decrease in Childhood Obesity and Waist Circumference over 15 Years in Switzerland: A Repeated Cross-Sectional Study. Nutrients 2019, 11, 1922. https://doi.org/10.3390/nu11081922
Herter-Aeberli I, Osuna E, Sarnovská Z, Zimmermann MB. Significant Decrease in Childhood Obesity and Waist Circumference over 15 Years in Switzerland: A Repeated Cross-Sectional Study. Nutrients. 2019; 11(8):1922. https://doi.org/10.3390/nu11081922
Chicago/Turabian StyleHerter-Aeberli, Isabelle, Ester Osuna, Zuzana Sarnovská, and Michael B. Zimmermann. 2019. "Significant Decrease in Childhood Obesity and Waist Circumference over 15 Years in Switzerland: A Repeated Cross-Sectional Study" Nutrients 11, no. 8: 1922. https://doi.org/10.3390/nu11081922