Dietary Habits, Fatty Acids and Carotenoid Levels Are Associated with Neovascular Age-Related Macular Degeneration in Chinese

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Calculation of Sample Size
2.3. Measurement of Plasma Fatty Acids and Carotenoids
2.4. Food Frequency Questionnaire
2.5. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Beatty, S.; Koh, H.H.; Phil, M.; Henson, D.; Boulton, M. The Role of Oxidative Stress in the Pathogenesis of Age-Related Macular Degeneration. Surv. Ophthalmol. 2000, 45, 115–134. [Google Scholar] [CrossRef] [Green Version]
- Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch. Ophthalmol. 2001, 119, 1417–1436. [Google Scholar] [CrossRef] [PubMed]
- Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: The Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA 2013, 309, 2005–2015. [Google Scholar] [CrossRef] [PubMed]
- Galano, J.M.; Lee, J.C.Y.; Gladine, C.; Comte, B.; Le Guennec, J.Y.; Oger, C.; Durand, T. Non-enzymatic cyclic oxygenated metabolites of adrenic, docosahexaenoic, eicosapentaenoic and α-linolenic acids; bioactivities and potential use as biomarkers. Biochim. Biophys. Acta (BBA) Mol. Cell Biol. Lipids 2015, 1851, 446–455. [Google Scholar] [CrossRef] [PubMed]
- Rotstein, N.P.; Politi, L.E.; German, O.L.; Girotti, R. Protective Effect of Docosahexaenoic Acid on Oxidative Stress-Induced Apoptosis of Retina Photoreceptors. Investig. Ophthalmol. Vis. Sci. 2003, 44, 2252–2259. [Google Scholar] [CrossRef] [PubMed]
- Hollyfield, J.G.; Bonilha, V.L.; Rayborn, M.E.; Yang, X.; Shadrach, K.G.; Lu, L.; Ufret, R.L.; Salomon, R.G.; Perez, V.L. Oxidative damage–induced inflammation initiates age-related macular degeneration. Nat. Med. 2008, 14, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Souied, E.H.; Delcourt, C.; Querques, G.; Bassols, A.; Merle, B.; Zourdani, A.; Smith, T.; Benlian, P.; Nutritional AMD Treatment study Group. Oral docosahexaenoic acid in the prevention of exudative age-related macular degeneration: The Nutritional AMD Treatment 2 study. Ophthalmology 2013, 120, 1619–1631. [Google Scholar] [CrossRef] [PubMed]
- Chong, E.W.; Kreis, A.J.; Wong, T.Y.; Simpson, J.A.; Guymer, R.H. Dietary omega-3 fatty acid and fish intake in the primary prevention of age-related macular degeneration: A systematic review and meta-analysis. Arch. Ophthalmol. 2008, 126, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Connor, K.M.; SanGiovanni, J.P.; Lofqvist, C.; Aderman, C.M.; Chen, J.; Higuchi, A.; Hong, S.; Pravda, E.A.; Majchrzak, S.; Carper, D.; et al. Increased dietary intake of omega-3-polyunsaturated fatty acids reduces pathological retinal angiogenesis. Nat. Med. 2007, 13, 868–873. [Google Scholar] [CrossRef]
- Wang, X.; Jiang, C.; Zhang, Y.; Gong, Y.; Chen, X.; Zhang, M. Role of Lutein Supplementation in the Management of Age-Related Macular Degeneration: Meta-Analysis of Randomized Controlled Trials. Ophthalmic Res. 2014, 52, 198–205. [Google Scholar] [CrossRef]
- Dawczynski, J.; Jentsch, S.; Schweitzer, D.; Hammer, M.; Lang, G.E.; Strobel, J. Long term effects of lutein, zeaxanthin and omega-3-LCPUFAs supplementation on optical density of macular pigment in AMD patients: The LUTEGA study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2013, 251, 2711–2723. [Google Scholar] [CrossRef] [PubMed]
- Arnold, C.; Winter, L.; Frohlich, K.; Jentsch, S.; Dawczynski, J.; Jahreis, G.; Bohm, V. Macular xanthophylls and omega-3 long-chain polyunsaturated fatty acids in age-related macular degeneration: A randomized trial. JAMA Ophthalmol. 2013, 131, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Merle, B.M.; Benlian, P.; Puche, N.; Bassols, A.; Delcourt, C.; Souied, E.H. Circulating Omega-3 Fatty Acids and Neovascular Age-Related Macular Degeneration. Investig. Ophthalmol. Vis. Sci. 2014, 55, 2010–2019. [Google Scholar] [CrossRef] [Green Version]
- Quehenberger, O.; Armando, A.M.; Dennis, E.A. High Sensitivity Quantitative Lipidomics Analysis of Fatty Acids in Biological Samples by Gas Chromatography-Mass Spectrometry. Biochim. Biophys. Acta (BBA) Mol. Cell Boil. Lipids 2011, 1811, 648–656. [Google Scholar] [CrossRef] [PubMed]
- Karppi, J.; Nurmi, T.; Olmedilla-Alonso, B.; Granado-Lorencio, F.; Nyyssonen, K. Simultaneous measurement of retinol, alpha-tocopherol and six carotenoids in human plasma by using an isocratic reversed-phase HPLC method. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2008, 867, 226–232. [Google Scholar] [CrossRef]
- Woo, J.; Leung, S.; Ho, S.; Lam, T.; Janus, E. A food frequency questionnaire for use in the Chinese population in Hong Kong: Description and examination of validity. Nutr. Res. 1997, 17, 1633–1641. [Google Scholar] [CrossRef]
- Leung, S.; Woo, J.; Ho, S.; Lam, T.; Janus, E. Hong Kong adult dietary survey, 1995. Aust. J. Nutr. Diet. 1998, 55, S11–S13. [Google Scholar]
- Mitchell, P.; Wang, J.J.; Foran, S.; Smith, W. Five-year incidence of age-related maculopathy lesions: The Blue Mountains Eye Study. Ophthalmology 2002, 109, 1092–1097. [Google Scholar] [CrossRef]
- Nirmalan, P.K.; Katz, J.; Robin, A.L.; Tielsch, J.M.; Namperumalsamy, P.; Kim, R.; Narendran, V.; Ramakrishnan, R.; Krishnadas, R.; Thulasiraj, R.D.; et al. Prevalence of vitreoretinal disorders in a rural population of southern India: The Aravind Comprehensive Eye Study. Arch. Ophthalmol. 2004, 122, 581–586. [Google Scholar] [CrossRef]
- Yasuda, M.; Kiyohara, Y.; Hata, Y.; Arakawa, S.; Yonemoto, K.; Doi, Y.; Iida, M.; Ishibashi, T. Nine-Year Incidence and Risk Factors for Age-Related Macular Degeneration in a Defined Japanese Population The Hisayama Study. Ophthalmology 2009, 116, 2135–2140. [Google Scholar] [CrossRef]
- Kawasaki, R.; Yasuda, M.; Song, S.J.; Chen, S.J.; Jonas, J.B.; Wang, J.J.; Mitchell, P.; Wong, T.Y. The prevalence of age-related macular degeneration in Asians: A systematic review and meta-analysis. Ophthalmology 2010, 117, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Knudtson, M.D.; Wong, T.Y.; Cotch, M.F.; Liu, K.; Burke, G.; Saad, M.F.; Jacobs, D.R. Prevalence of Age-Related Macular Degeneration in 4 Racial/Ethnic Groups in the Multi-ethnic Study of Atherosclerosis. Ophthalmology 2006, 113, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Gangwani, R.; Lai, W.W.; Sum, R.; McGhee, S.M.; Chan, C.W.; Hedley, A.J.; Wong, D. The incidental findings of age-related macular degeneration during diabetic retinopathy screening. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 252, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Skrzypski, J.; Bellenger, S.; Bellenger, J.; Sinclair, A.; Poisson, J.P.; Tessier, C.; Rialland, M.; Narce, M. Revisiting delta-6 desaturase regulation by C18 unsaturated fatty acids, depending on the nutritional status. Biochimie 2009, 91, 1443–1449. [Google Scholar] [CrossRef] [PubMed]
- Wood, K.; Mantzioris, E.; Gibson, R.; Ramsden, C.; Muhlhausler, B.; Gibson, R. The effect of modifying dietary LA and ALA intakes on omega-3 long chain polyunsaturated fatty acid (n-3 LCPUFA) status in human adults: A systematic review and commentary. Prostagland. Leukot. Essent. Fatty Acids 2015, 95, 47–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.S.; Huang, W.C.; Li, C.W.; Chuang, L.T. Eicosadienoic acid differentially modulates production of pro-inflammatory modulators in murine macrophages. Mol. Cell Biochem. 2011, 358, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Smith, U.; Kahn, B.B. Adipose tissue regulates insulin sensitivity: Role of adipogenesis, de novo lipogenesis and novel lipids. J. Intern. Med. 2016, 280, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Georgiou, T.; Prokopiou, E. The New Era of Omega-3 Fatty Acids Supplementation: Therapeutic Effects on Dry Age-Related Macular Degeneration. J. Stem Cells 2015, 10, 205–215. [Google Scholar] [PubMed]
- Wu, J.; Cho, E.; Giovannucci, E.L.; Rosner, B.A.; Sastry, S.M.; Willett, W.C.; Schaumberg, D.A. Dietary Intakes of Eicosapentaenoic Acid and Docosahexaenoic Acid and Risk of Age-Related Macular Degeneration. Ophthalmology 2017, 124, 634–643. [Google Scholar] [CrossRef] [Green Version]
- Delyfer, M.N.; Buaud, B.; Korobelnik, J.F.; Rougier, M.B.; Schalch, W.; Etheve, S.; Vaysse, C.; Combe, N.; Le Goff, M.; Wolf-Schnurrbusch, U.E.K.; et al. Association of Macular Pigment Density with Plasma Omega-3 Fatty Acids: The PIMAVOSA Study. Investig. Ophthalmol. Vis. Sci. 2012, 53, 1204–1210. [Google Scholar] [CrossRef]
- Buaud, B.; Korobelnik, J.; Bron, A.; Delyfer, M.; Rougier, M.; Vaysse, C.; Creuzot-Garcher, C.; Merle, B.M.J.; Savel, H.; Delcourt, C. Plasma long-chain omega-3 polyunsaturated fatty acids and macular pigment in subjects with family history of age-related macular degeneration: The Limpia Study. Acta Ophthalmol. 2017, 95, e763–e769. [Google Scholar]
- Korobelnik, J.F.; Rougier, M.B.; Delyfer, M.N.; Bron, A.; Merle, B.M.J.; Savel, H.; Chene, G.; Delcourt, C.; Creuzot-Garcher, C. Effect of Dietary Supplementation with Lutein, Zeaxanthin, and omega-3 on Macular Pigment: A Randomized Clinical Trial. JAMA Ophthalmol. 2017, 135, 1259–1266. [Google Scholar] [CrossRef] [PubMed]
- Lund, E.K. Health benefits of seafood; is it just the fatty acids? Food Chem. 2013, 140, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Gorusupudi, A.; Liu, A.; Hageman, G.S.; Bernstein, P.S. Associations of human retinal very long-chain polyunsaturated fatty acids with dietary lipid biomarkers. J. Lipid Res. 2016, 57, 499–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Mean Difference between Cases & Controls | Standard Error | p-Value | 95% Confidence | Interval | |
|---|---|---|---|---|---|
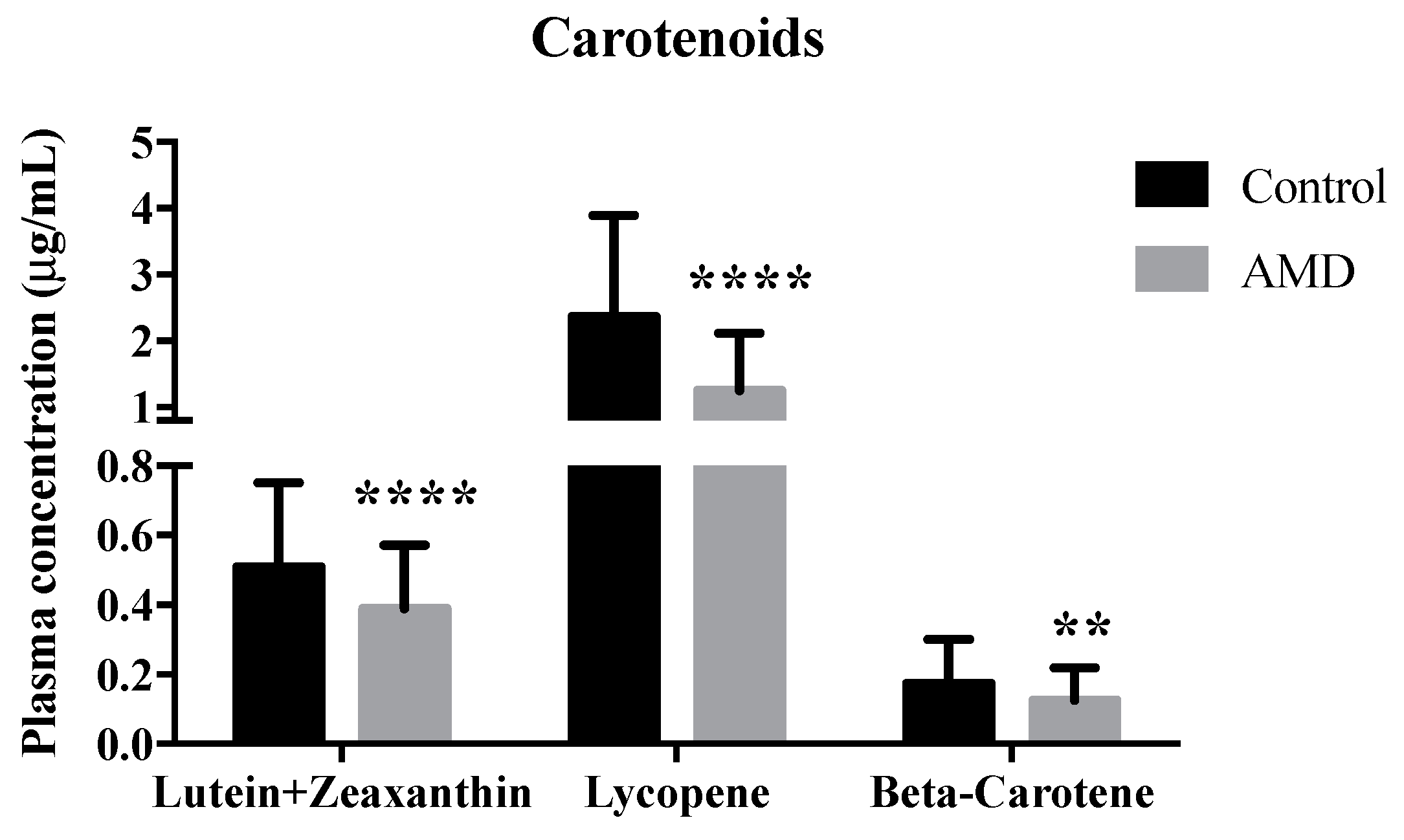
| Carotenoids | |||||
| Beta-carotene | −0.050 | 0.024 | 0.036 | −0.098 | −0.003 |
| Lycopene | −1.197 | 0.358 | 0.001 | −1.903 | −0.492 |
| Lutein + zeaxanthin | −0.097 | 0.039 | 0.013 | −0.173 | −0.021 |
| Saturated Fatty Acids (SFA) | |||||
| C14:0 (Myristic acid) | 2.509 | 0.243 | <0.0005 | 2.031 | 2.988 |
| C15:0 (Pentadecylic acid) | 2.509 | 0.243 | <0.0005 | 2.031 | 2.988 |
| C16:0 (Palmitic acid) | 91.241 | 14.160 | <0.0005 | 63.369 | 119.113 |
| C17:0 (Margaric acid) | 1.954 | 0.340 | <0.0005 | 1.284 | 2.623 |
| C18:0 (Stearic acid) | 16.824 | 10.187 | 0.1 | −3.229 | 36.876 |
| C20:0 (Arachidic acid) | 0.094 | 0.151 | 0.533 | −0.202 | 0.390 |
| Monounsaturated fatty acids (MUFA) | |||||
| C14:1n9 (Myristoleic acid) | 0.112 | 0.397 | 0.778 | −0.669 | 0.893 |
| C15:1n10 (Pentadecenoic acid) | 0.208 | 0.358 | 0.561 | −0.496 | 0.912 |
| C16:1n9 (Palmitoleic acid) | 0.274 | 1.392 | 0.844 | −2.465 | 3.013 |
| C17:1n10 (Heptadecenoic acid) | 1.511 | 0.589 | 0.011 | 0.351 | 2.670 |
| C18:1n9 (Oleic acid) | 101.543 | 14.282 | 0.0005 | 73.431 | 129.655 |
| C20:1n9 (Gondoic acid) | 0.475 | 0.436 | 0.277 | −0.383 | 1.333 |
| C22:1n9 (Erucic acid) | 0.728 | 0.353 | 0.04 | 0.033 | 1.423 |
| Omega-6 Polyunsaturated fatty acids (PUFA) | |||||
| C18:2n6 (Linoleic acid) | 0.843 | 17.843 | 0.962 | −34.279 | 35.964 |
| C18:3n6 (γ-Linolenic acid) | −0.826 | 0.438 | 0.06 | −1.687 | 0.036 |
| C20:2n6 (Eicosadienoic acid) | 1.307 | 0.446 | 0.004 | 0.429 | 2.185 |
| C20:3n6 (Dihomo-γ-linolenic acid) | −3.906 | 1.230 | 0.002 | −6.328 | −1.485 |
| C20:4n6 (Arachidonic acid) | 53.703 | 6.834 | <0.0005 | 40.253 | 67.154 |
| C22:4n6 (Adrenic acid) | −0.226 | 0.350 | 0.519 | −0.914 | 0.462 |
| Omega-3 Polyunsaturated fatty acids (PUFA) | |||||
| C18:3n3 (α-Linolenic acid) | −1.899 | 1.122 | 0.092 | −4.107 | 0.310 |
| C20:3n3 (Eicosatrienoic acid) | 8.307 | 1.449 | <0.0005 | 5.456 | 11.159 |
| C20:5n3 (Eicosapentaenoic acid) | −4.404 | 0.759 | <0.0005 | −5.898 | −2.910 |
| C22:5n3 (Docosapentaenoic acid) | −0.331 | 0.200 | 0.099 | −0.724 | 0.063 |
| C22:6n3 (Docosahexaenoic acid) | −6.651 | 2.134 | 0.002 | −10.851 | −2.450 |
| Concentration (μg/mL) † | Healthy Control (n = 198) | Wet AMD (n = 99) |
|---|---|---|
| Saturated fatty acids | ||
| C14:0 (Myristic acid) | 12.03 ± 5.49 | 13.58 ± 3.24 * |
| C15:0 (Pentadecylic acid) | 2.23 ± 1.40 | 4.67 ± 2.60 **** |
| C16:0 (Palmitic acid) | 267.05 ± 109.79 | 344.98 ± 105.24 **** |
| C17:0 (Margaric acid) | 5.02 ± 2.31 | 6.76 ± 2.60 **** |
| C18:0 (Stearic acid) | 173.50 ± 81.57 | 190.21 ± 64.12 |
| C20:0 (Arachidic acid) | 1.03 ± 0.76 | 1.17 ± 0.56 |
| Mono-unsaturated fatty acids | ||
| C14:1n9 (Myristoleic acid) | 3.20 ± 2.10 | 3.82 ± 1.18 * |
| C15:1n10 (Pentadecenoc acid) | 3.68 ± 2.42 | 4.52 ± 1.15 ** |
| C16:1n9 (Palmitoleic acid) | 23.62 ± 9.68 | 24.10 ± 9.39 |
| C17:1n10 (Heptadecenoic acid) | 8.94 ± 5.14 | 10.40 ± 2.50 * |
| C18:1n9 (Oleic acid) | 280.38 ± 111.20 | 375.69 ± 95.89 **** |
| C20:1n9 (Gondoic acid) | 7.16 ± 3.69 | 7.71 ± 2.13 |
| C22:1n9 (Erucic acid) | 3.57 ± 2.15 | 3.57 ± 1.97 |
| Omega-6 polyunsaturated fatty acids | ||
| C18:2n6 (Linoleic acid) | 417.46 ± 143.05 | 415.25 ± 81.83 |
| C18:3n6 (γ-Linolenic acid) | 3.72 ± 2.09 | 4.31 ± 1.96 |
| C20:2n6 (Eicosadienoic acid) | 5.48 ± 2.92 | 6.95 ± 3.69 *** |
| C20:3n6 (Dihomo−γ-linolenic acid) | 17.77 ± 10.01 | 13.45 ± 7.81 *** |
| C20:4n6 (Arachidonic acid) | 95.57 ± 39.81 | 148.84 ± 68.44 **** |
| C22:4n6 (Adrenic acid) | 3.40 ± 2.04 | 2.85 ± 1.98 |
| Omega-3 polyunsaturated fatty acids | ||
| C18:3n3 (α-Linolenic acid) | 15.02 ± 5.12 | 12.56 ± 3.91 *** |
| C20:3n3 (Eicosatrienoic acid) | 17.77 ± 10.01 | 21.42 ± 11.66 * |
| C20:5n3 (Eicosapentaenoic acid) | 13.10 ± 6.15 | 8.92 ± 4.61 **** |
| C22:5n3 (Docosapentaenoic acid) | 2.14 ± 1.68 | 1.92 ± 0.99 |
| C22:6n3 (Docosahexaenoic acid) | 22.58 ± 14.95 | 12.80 ± 6.52 **** |
| Odds-Ratio | Standard Error | p-Value | 95% Confidence | Interval | |
|---|---|---|---|---|---|
| Carotenoids | |||||
| Beta-carotene | 2.779 | 1.091 | 0.009 | 1.287 | 5.997 |
| Lycopene | 6.017 | 2.478 | <0.0005 | 2.685 | 13.488 |
| Lutein+zeaxanthin | 4.825 | 2.068 | <0.0005 | 2.083 | 11.177 |
| Omega-6 polyunsaturated fatty acids | |||||
| C20:4n6 (Arachidonic acid) | 0.110 | 0.047 | <0.0005 | 0.048 | 0.253 |
| C22:4n6 (Adrenic acid) | 2.594 | 1.025 | 0.016 | 1.196 | 5.630 |
| Omega-3 polyunsaturated fatty acids | |||||
| C18:3n3 (α-Linolenic acid) | 3.107 | 1.184 | 0.003 | 1.472 | 6.558 |
| C20:3n3 (Eicosatrienoic acid) | 0.160 | 0.075 | <0.0005 | 0.064 | 0.399 |
| C22:5n3 (Docosapentaenoic acid) | 7.789 | 3.288 | <0.0005 | 3.406 | 17.813 |
| C22:6n3 (Docosahexaenoic acid) | 6.326 | 2.944 | <0.0005 | 2.541 | 15.750 |
| Odds-Ratio | Standard Error | p-value | 95% Confidence | Interval | |
|---|---|---|---|---|---|
| C20:2n6 (Eicosadienoic acid) | 2.634 | 0.994 | 0.010 | 1.257 | 5.519 |
| C18:1n9 (Oleic acid) | 14.095 | 7.194 | <0.0005 | 5.184 | 38.327 |
| C16:0 (Palmitic acid) | 11.484 | 5.640 | <0.0005 | 4.386 | 30.071 |
| C15:0 (Pentadecylic acid) | 33.754 | 17.897 | <0.0005 | 11.940 | 95.420 |
| Food Item | Frequency of Dietary Intake Per Week * | p-Value | Serving Size Per Meal * | p-Value | ||
|---|---|---|---|---|---|---|
| Control | AMD | Control | AMD | |||
| Source of carotenoids | ||||||
| Green leafy vegetables (e.g., Chinese kale, broccoli, spinach) | 4 (1) | 4 (2) | 0.102 | 5 (1) | 4 (1.5) | <0.001 |
| Tomato | 1 (7) | 2 (7) | 0.287 | 2 (2) | 2 (3) | 0.630 |
| Red carrots | 2 (7) | 8 (7) | 0.129 | 2 (2) | 3 (2) | 0.742 |
| Other vegetables (e.g., turnip, celery cabbage, cabbage and potato) | 2 (7) | 2 (7) | 0.284 | 4 (1) | 3 (2) | <0.001 |
| Source of polyunsaturated fatty acid | ||||||
| Red meat (pork, beef, lamb) | 2 (2) | 3 (3) | 0.012 | 3 (1) | 2 (1) | 0.052 |
| Poultry (chicken, duck, pigeon) | 2 (3) | 2 (7) | 0.031 | 3 (1) | 2 (1) | 0.030 |
| Oily fish (mackerel, eel, woo fish, salmon, sardine) | 8 (2.5) | 8 (4) | 0.912 | 3 (1) | 2 (2) | 0.207 |
| White meat fish (e.g., sea bass, tilapia, cod) | 3 (3) | 2 (2) | 0.361 | 3 (0) | 3 (1.5) | 0.204 |
| Other seafood (e.g., prawn, seafood, crab, mussels, scallop) | 7 (7) | 8 (7) | 0.006 | 2 (2) | 2 (2) | 0.312 |
| Walnuts | 8 (0.5) | 8 (0) | 0.326 | 1 (0) | 1 (0) | 0.784 |
| Peanuts | 8 (4) | 8 (6) | 0.733 | 1 (1) | 1 (1) | 0.671 |
| Other nuts (e.g., almond, pistachio, cashew) | 8 (6) | 8 (6) | 0.151 | 2 (1) | 2 (1) | 0.781 |
| Others † | ||||||
| Milk | 2 (1) | 1 (1) | 0.110 | |||
| Cheese | 2 (1) | 2 (1) | 0.798 | |||
| Preserved vegetables | 2 (1) | 2 (1) | 0.045 | |||
| Preserved meat | 2 (1) | 2 (0) | 0.027 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, A.L.-K.; Leung, H.H.; Kawasaki, R.; Ho, W.-L.; Chow, L.L.-W.; Chow, S.S.-W.; Lee, J.C.-Y.; Wong, I.Y.-H. Dietary Habits, Fatty Acids and Carotenoid Levels Are Associated with Neovascular Age-Related Macular Degeneration in Chinese. Nutrients 2019, 11, 1720. https://doi.org/10.3390/nu11081720
Ng AL-K, Leung HH, Kawasaki R, Ho W-L, Chow LL-W, Chow SS-W, Lee JC-Y, Wong IY-H. Dietary Habits, Fatty Acids and Carotenoid Levels Are Associated with Neovascular Age-Related Macular Degeneration in Chinese. Nutrients. 2019; 11(8):1720. https://doi.org/10.3390/nu11081720
Chicago/Turabian StyleNg, Alex L.-K., Ho Hang Leung, Ryo Kawasaki, Wing-Lau Ho, Loraine L.-W. Chow, Sharon S.-W. Chow, Jetty Chung-Yung Lee, and Ian Y.-H. Wong. 2019. "Dietary Habits, Fatty Acids and Carotenoid Levels Are Associated with Neovascular Age-Related Macular Degeneration in Chinese" Nutrients 11, no. 8: 1720. https://doi.org/10.3390/nu11081720