Association of Adherence to The Mediterranean Diet with Urinary Factors Favoring Renal Lithiasis: Cross-Sectional Study of Overweight Individuals with Metabolic Syndrome

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Overview and Sample
2.2. Dietary Assessment and Mediterranean Diet Score
2.3. Urine Collection and Analysis
2.4. Covariates Assessment
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Urinary Parameters
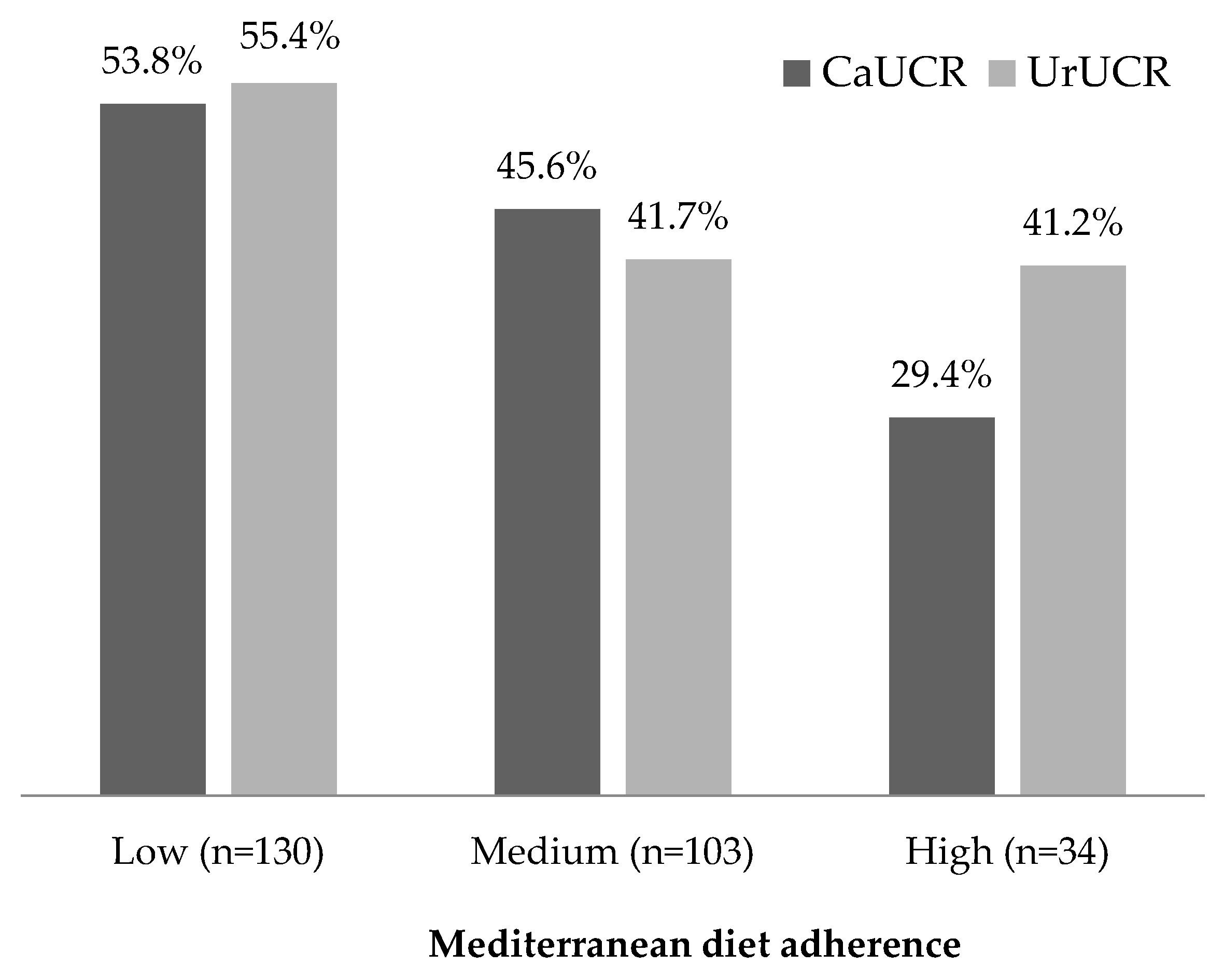
3.2. Calcium and Uric Acid Urinary Crystallization Risk
3.3. Association between MedDiet Adherence and Urinary Crystallization Risk
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Grases, F.; Costa-Bauzá, A.; Ramis, M.; Montesinos, V.; Conte, A. Simple classification of renal calculi closely related to their micromorphology and etiology. Clin. Chim. Acta 2002, 322, 29–36. [Google Scholar] [CrossRef]
- Sohgaura, A.; Bigoniya, P. A Review on Epidemiology and Etiology of Renal Stone. Am. J. Drug Discov. Dev. 2017, 7, 54–62. [Google Scholar] [CrossRef]
- Romero, V.; Akpinar, H.; Assimos, D.G. Kidney stones: A global picture of prevalence, incidence, and associated risk factors. Rev. Urol. 2010, 12, e86. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, J.A.; Maalouf, N.M.; Pearle, M.S.; Lotan, Y. Use of the National Health and Nutrition Examination Survey to calculate the impact of obesity and diabetes on cost and prevalence of urolithiasis in 2030. Eur. Urol. 2014, 66, 724–729. [Google Scholar] [CrossRef] [PubMed]
- Sakhaee, K.; Maalouf, N.M. Metabolic syndrome and uric acid nephrolithiasis. Semin. Nephrol. 2008, 28, 174–180. [Google Scholar] [CrossRef]
- Parivar, F.; Low, R.K.; Stoller, M.L. The influence of diet on urinary stone disease. J. Urol. 1996, 155, 432–440. [Google Scholar] [CrossRef]
- Grases, F.; Costa-Bauza, A.; Prieto, R.M. Renal lithiasis and nutrition. Nutr. J. 2006, 5, 23. [Google Scholar] [CrossRef]
- Prezioso, D.; Strazzullo, P.; Lotti, T.; Bianchi, G.; Borghi, L.; Caione, P.; Carini, M.; Caudarella, R.; Ferraro, M.; Gambaro, G.; et al. Dietary treatment of urinary risk factors for renal stone formation. A review of CLU Working Group. Arch. Ital. Urol. Androl. 2015, 87, 105–120. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Buil-Cosiales, P.; Corella, D.; Bulló, M.; Fitó, M.; Vioque, J.; Romaguera, D.; Martínez, J.A.; Wärnberg, J.; López-Miranda, J.; et al. Cohort Profile: Design and methods of the PREDIMED-Plus randomized trial. Int. J. Epidemiol. 2019, 48, 387–388o. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef]
- De la Fuente-Arrillaga, C.; Vazquez Ruiz, Z.; Bes-Rastrollo, M.; Sampson, L.; Martinez-González, M.A. Reproducibility of an FFQ validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef]
- Mataix, J.; Manas, M.; Llopis, J.; Martínez de Victoria, E.; Juan, J.; Borregón, A. Tabla de Composición de Alimentos Españoles (Spanish Food Composition Tables), 4th ed.; Universidad de Granada: Granada, Spain, 2003. (In Spanish) [Google Scholar]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos (Spanish Food Composition Tables), 16th ed.; Pirámide: Madrid, Spain, 2013. (In Spanish) [Google Scholar]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Grases, F.; Costa-Bauzá, A.; Prieto, R.M.; Arrabal, M.; De Haro, T.; Lancina, J.A.; Barbuzano, C.; Colom, S.; Riera, J.; Perelló, J.; et al. Urinary lithogenesis risk tests: Comparison of a commercial kit and a laboratory prototype test. Scand. J. Urol. Nephrol. 2011, 45, 312–318. [Google Scholar] [CrossRef]
- Grases, F.; García-Ferragut, L.; Costa-Bauzá, A.; Conte, A.; García-Raja, A. Simple test to evaluate the risk of urinary calcium stone formation. Clin. Chim. Acta 1997, 263, 43–55. [Google Scholar] [CrossRef]
- Galán, J.A.; Conte, A.; Llobera, A.; Costa-Bauzá, A.; Grases, F. A comparative study between etiological factors of calcium oxalate monohydrate and calcium oxalate dihydrate urolithiasis. Urol. Int. 1996, 56, 79–85. [Google Scholar] [CrossRef]
- Kenny, J.E.S.; Goldfarb, D.S. Update on the pathophysiology and management of uric acid renal stones. Curr. Rheumatol. Rep. 2010, 12, 125–129. [Google Scholar] [CrossRef]
- Zhang, J.; Kai, F.Y. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA 1998, 280, 1690–1691. [Google Scholar] [CrossRef]
- Leone, A.; Fernández-Montero, A.; de la Fuente-Arrillaga, C.; Martínez-González, M.A.; Bertoli, S.; Battezzati, A.; Bes-Rastrollo, M. Adherence to the Mediterranean Dietary Pattern and Incidence of Nephrolithiasis in the Seguimiento Universidad de Navarra Follow-up (SUN) Cohort. Am. J. Kidney Dis. 2017, 70, 778–786. [Google Scholar] [CrossRef]
- Gentle, D.L.; Stoller, M.L.; Bruce, J.E.; Leslie, S.W. Geriatric urolithiasis. J. Urol. 1997, 158, 2221–2224. [Google Scholar] [CrossRef]
- Sorensen, M.D.; Hsi, R.S.; Chi, T.; Shara, N.; Wactawski-Wende, J.; Kahn, A.J.; Wang, H.; Hou, L.; Stoller, M.L.; Women’s Health Initiative Writing Group. Dietary intake of fiber, fruit and vegetables decreases the risk of incident kidney stones in women: A Women’s Health Initiative report. J. Urol. 2014, 192, 1694–1699. [Google Scholar] [CrossRef]
- Meschi, T.; Maggiore, U.; Fiaccadori, E.; Schianchi, T.; Bosi, S.; Adorni, G.; Ridolo, E.; Guerra, A.; Allegri, F.; Novarini, A.; et al. The effect of fruits and vegetables on urinary stone risk factors. Kidney Int. 2004, 66, 2402–2410. [Google Scholar] [CrossRef] [Green Version]
- Remer, T.; Manz, F. Potential renal acid load of foods and its influence on urine pH. J. Am. Diet. Assoc. 1995, 95, 791–797. [Google Scholar] [CrossRef]
- Taylor, E.N.; Fung, T.T.; Curhan, G.C. DASH-style diet associates with reduced risk for kidney stones. J. Am. Soc. Nephrol. 2009, 20, 2253–2259. [Google Scholar] [CrossRef]
- Taylor, E.N.; Stampfer, M.J.; Mount, D.B.; Curhan, G.C. DASH-style diet and 24-hour urine composition. Clin. J. Am. Soc. Nephrol. 2010, 5, 2315–2322. [Google Scholar] [CrossRef]
- Rendina, D.; De Filippo, G.; D’Elia, L.; Strazzullo, P. Metabolic syndrome and nephrolithiasis: A systematic review and meta-analysis of the scientific evidence. J. Nephrol. 2014, 27, 371–376. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| CaUCR: at least one of four conditions must be present | |
| Calcium | >20 mg/dL |
| Oxalate | >4 mg/dL |
| Ca/Cit ratio | >0.33 |
| Three or more of these alterations | |
| pH | <5.5 |
| pH | >6.0 |
| Calcium | >17 mg/dL |
| Phosphorous | >100 mg/dL |
| Urate | >60 mg/dL |
| Citrate | <23 mg/dL |
| Oxalate | >3 mg/dL |
| Magnesium | <5 mg/dL |
| UrUCR: at least one of two conditions must be present | |
| pH | <5.5 |
| Uric acid | >100 mg/dL |
| Mediterranean Diet Adherence a | ||||
|---|---|---|---|---|
| Low (n = 130) | Medium (n = 103) | High (n = 34) | p-value b | |
| Age (years) | 64 ± 5 | 66 ± 5 | 65 ± 5 | 0.023 |
| Sex (% female) | 67 (51.5) | 48 (46.6) | 17 (50) | 0.750 |
| DM (%) | 37 (28.5) | 26 (25.2) | 10 (29.4) | 0.830 |
| HTA (%) | 116 (89.2) | 91 (88.3) | 29 (85.3) | 0.816 |
| BMI (kg/m2) | 33 ± 3 | 32 ± 3 | 32 ± 4 | 0.093 |
| Energy (kcal/day) | 2202 ± 665 | 2275 ± 609 | 2287 ±4 36 | 0.603 |
| pH | 5.7 ± 0.7 | 5.8 ± 0.7 | 5.8 ± 0.7 | 0.395 |
| Ur (mg/dL) | 55 ± 25 | 47 ± 23 | 49 ± 26 | 0.025 |
| P (mg/dL) | 74 ± 40 | 70 ± 37 | 59 ± 22 | 0.131 |
| Cit (mg/L) | 639 ± 392 | 568 ± 347 | 599 ± 367 | 0.354 |
| Ox (mg/L) | 21 ± 9 | 21 ± 12 | 21 ± 9 | 0.976 |
| Ca (mg/dL) | 12 ± 9 | 11 ± 10 | 9 ± 5 | 0.297 |
| Mg (mg/dL) | 7 ± 5 | 7 ± 5 | 7 ± 3 | 0.446 |
| Ca/Cit ratio | 0.23 ± 0.23 0.20 (0.11–0.29) * | 0.26 ± 0.26 0.24 (0.12–0.45) * | 0.17 ± 0.12 0.19 (0.07–0.22) * | 0.148 |
| Mediterranean Diet Adherence a | |||||
|---|---|---|---|---|---|
| Low (n = 130) | Medium (n = 103) | High (n = 34) | p for trend | ||
| CaUCR | Model 1 b | ref. | 0.85 (0.62, 1.09) | 0.55 (0.29, 0.90) | 0.012 |
| Model 2 c | ref. | 0.87 (0.63, 1.12) | 0.51 (0.26, 0.87) | 0.012 | |
| UrUCR | Model 1 b | ref. | 0.75 (0.54, 0.99) | 0.74 (0.44, 1.08) | 0.042 |
| Model 2 c | ref. | 0.76 (0.54, 1.00) | 0.77 (0.46, 1.12) | 0.069 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prieto, R.M.; Rodriguez, A.; Sanchis, P.; Morey, M.; Fiol, M.; Grases, F.; Castañer, O.; Martínez-González, M.A.; Salas-Salvadó, J.; Romaguera, D. Association of Adherence to The Mediterranean Diet with Urinary Factors Favoring Renal Lithiasis: Cross-Sectional Study of Overweight Individuals with Metabolic Syndrome. Nutrients 2019, 11, 1708. https://doi.org/10.3390/nu11081708
Prieto RM, Rodriguez A, Sanchis P, Morey M, Fiol M, Grases F, Castañer O, Martínez-González MA, Salas-Salvadó J, Romaguera D. Association of Adherence to The Mediterranean Diet with Urinary Factors Favoring Renal Lithiasis: Cross-Sectional Study of Overweight Individuals with Metabolic Syndrome. Nutrients. 2019; 11(8):1708. https://doi.org/10.3390/nu11081708
Chicago/Turabian StylePrieto, Rafael M., Adrian Rodriguez, Pilar Sanchis, Margalida Morey, Miquel Fiol, Felix Grases, Olga Castañer, Miguel A. Martínez-González, Jordi Salas-Salvadó, and Dora Romaguera. 2019. "Association of Adherence to The Mediterranean Diet with Urinary Factors Favoring Renal Lithiasis: Cross-Sectional Study of Overweight Individuals with Metabolic Syndrome" Nutrients 11, no. 8: 1708. https://doi.org/10.3390/nu11081708