Role of Calcium and Low-Fat Dairy Foods in Weight-Loss Outcomes Revisited: Results from the Randomized Trial of Effects on Bone and Body Composition in Overweight/Obese Postmenopausal Women

 , ,
, ,
Abstract
:1. Introduction
2. Methods
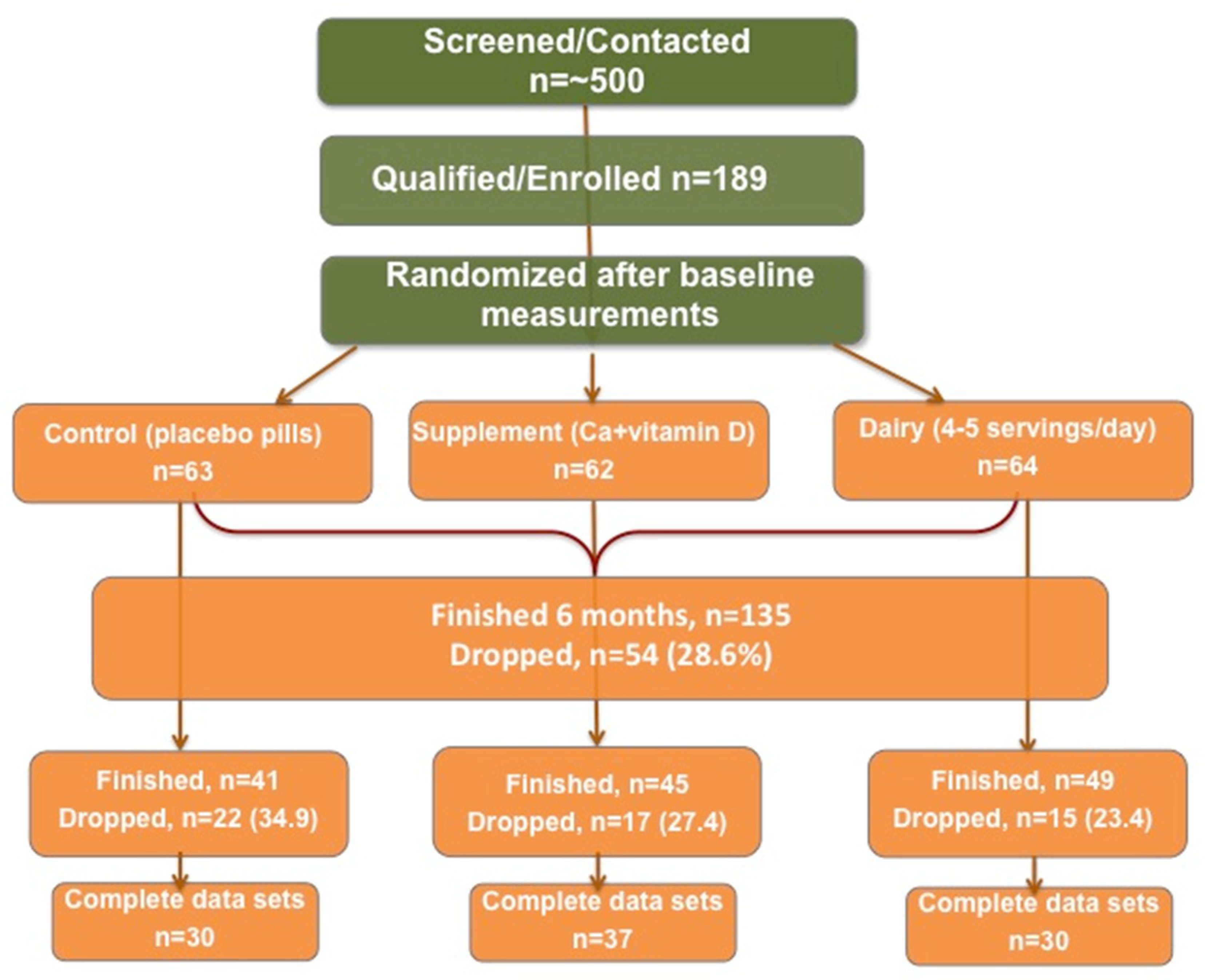
2.1. Overview of Design
2.1.1. Weight Reduction/Management and Lifestyle Change Intervention
2.1.2. Dietary Plan
2.2. Participants and Inclusion/Exclusion Criteria
2.3. Physical Measurements
Anthropometry and Body Composition
2.4. Clinical Chemistry
2.4.1. Blood
2.4.2. Urine
2.5. Dietary and Physical Activity (PA) Assessment
2.6. Questionnaires
2.7. Statistical Analyses
3. Results
4. Discussion
5. Conclusion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferrara, C.M.; Lynch, N.A.; Nicklas, B.J.; Ryan, A.S.; Berman, D.M. Differences in adipose tissue metabolism between postmenopausal and perimenopausal women. J. Clin. Endocrinol. Metab. 2002, 87, 4166–4170. [Google Scholar] [CrossRef]
- JafariNasabian, P.; Inglis, J.E.; Reilly, W.; Kelly, O.J.; Ilich, J.Z. Aging human body: Changes in bone, muscle and body fat with consequent changes in nutrient intake. J. Endocrinol. 2017, 234, R37–R51. [Google Scholar] [CrossRef] [PubMed]
- Iwaniec, U.T.; Turner, R.T. Influence of body weight on bone mass, architecture and turnover. J. Endocrinol. 2016, 230, R115–130. [Google Scholar] [CrossRef] [PubMed]
- Von Thun, N.L.; Sukumar, D.; Heymsfield, S.B.; Shapses, S.A. Does bone loss begin after weight loss ends? Results 2 years after weight loss or regain in postmenopausal women. Menopause 2014, 21, 501–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bleicher, K.; Cumming, R.G.; Naganathan, V.; Travison, T.G.; Sambrook, P.N.; Blyth, F.M.; Handelsman, D.J.; Le Couteur, D.G.; Waite, L.M.; Creasey, H.M.; et al. The role of fat and lean mass in bone loss in older men: Findings from the Champ study. Bone 2011, 49, 1299–1305. [Google Scholar] [CrossRef]
- Chao, D.; Espeland, M.A.; Farmer, D.; Register, T.C.; Lenchik, L.; Applegate, W.B.; Ettinger, W.H., Jr. Effect of voluntary weight loss on bone mineral density in older overweight women. J. Am. Geriatr. Soc. 2000, 48, 753–759. [Google Scholar] [CrossRef]
- Compston, J.E.; Wyman, A.; FitzGerald, G.; Adachi, J.D.; Chapurlat, R.D.; Cooper, C.; Diez-Perez, A.; Gehlbach, S.H.; Greenspan, S.L.; Hooven, F.H.; et al. Increase in fracture risk following unintentional weight loss in postmenopausal women: The global longitudinal study of osteoporosis in women. J. Bone Miner. Res. 2016, 31, 1466–1472. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Ewing, S.K.; Stone, K.L.; Cauley, J.A.; Bowman, P.J.; Cummings, S.R. Study of Osteoporotic Fractures Research Group. Intentional and unintentional weight loss increase bone loss and hip fracture risk in older women. J. Am. Geriatr. Soc. 2003, 51, 1740–1747. [Google Scholar] [CrossRef]
- Villareal, D.T.; Fontana, L.; Weiss, E.P.; Racette, S.B.; Steger-May, K.; Schechtman, K.B.; Klein, S.; Holloszy, J.O. Bone mineral density response to caloric restriction-induced weight loss or exercise-induced weight loss: A randomized controlled trial. Arch. Intern. Med. 2006, 166, 2502–2510. [Google Scholar] [CrossRef]
- Cava, E.; Yeat, N.C.; Mittendorfer, B. Preserving healthy muscle during weight loss. Adv. Nutr. 2017, 8, 511–519. [Google Scholar] [CrossRef]
- Hunter, G.R.; Bryan, D.R.; Borges, J.H.; David Diggs, M.; Carter, S.J. Racial differences in relative skeletal muscle mass loss during diet-induced weight loss in women. Obesity 2018, 26, 1255–1260. [Google Scholar] [CrossRef] [PubMed]
- Marsh, A.P.; Shea, M.K.; Vance Locke, R.M.; Miller, M.E.; Isom, S.; Miller, G.D.; Nicklas, B.J.; Lyles, M.F.; Carr, J.J.; Kritchevsky, S.B. Resistance training and pioglitazone lead to improvements in muscle power during voluntary weight loss in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 828–836. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Gonzalez, M.C.; Shen, W.; Redman, L.; Thomas, D. Weight loss composition is one-fourth fat-free mass: A critical review and critique of this widely cited rule. Obes. Rev. 2014, 15, 310–321. [Google Scholar] [CrossRef]
- Jensen, L.B.; Kollerup, G.; Quaade, F.; Sorensen, O.H. Bone minerals changes in obese women during a moderate weight loss with and without calcium supplementation. J. Bone Miner. Res. 2001, 16, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Weiss, E.P.; Jordan, R.C.; Frese, E.M.; Albert, S.G.; Villareal, D.T. Effects of weight loss on lean mass, strength, bone, and aerobic capacity. Med. Sci. Sports Exerc. 2017, 49, 206–217. [Google Scholar] [CrossRef]
- Ilich, J.Z.; Kelly, O.J.; Inglis, J.E. Osteosarcopenic obesity syndrome: What is it and how can it be identified and diagnosed? Curr. Gerontol. Geriatr. Res. 2016, 2016, 7325973. [Google Scholar] [CrossRef]
- Ilich, J.Z.; Kelly, O.J.; Inglis, J.E.; Panton, L.B.; Duque, G.; Ormsbee, M.J. Interrelationship among muscle, fat, and bone: Connecting the dots on cellular, hormonal, and whole body levels. Ageing Res. Rev. 2014, 15, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Kelly, O.J.; Gilman, J.C.; Boschiero, D.; Ilich, J.Z. Osteosarcopenic obesity: Current knowledge, revised identification criteria and treatment principles. Nutrients 2019, 11, 747. [Google Scholar] [CrossRef]
- Ilich, J.Z.; Kelly, O.J.; Kim, Y.; Spicer, M.T. Low-grade chronic inflammation perpetuated by modern diet as a promoter of obesity and osteoporosis. Arch. Ind. Hyg. Toxicol. 2014, 65, 139–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, P.Y.; Ilich, J.Z.; Brummel-Smith, K.; Ghosh, S. New insight into fat, muscle and bone relationship in women: Determining the threshold at which body fat assumes negative relationship with bone mineral density. Int. J. Prev. Med. 2014, 5, 1452–1463. [Google Scholar]
- Shin, H.; Liu, P.Y.; Panton, L.B.; Ilich, J.Z. Physical performance in relation to body composition and bone mineral density in healthy, overweight, and obese postmenopausal women. J. Geriatr. Phys. Ther. 2014, 37, 7–16. [Google Scholar] [CrossRef]
- Davies, K.M.; Heaney, R.P.; Recker, R.R.; Lappe, J.M.; Barger-Lux, M.J.; Rafferty, K.; Hinders, S. Calcium intake and body weight. J. Clin. Endocrinol. Metab. 2000, 85, 4635–4638. [Google Scholar] [CrossRef]
- Major, G.C.; Alarie, F.P.; Doré, J.; Tremblay, A. Calcium plus vitamin d supplementation and fat mass loss in female very low-calcium consumers: Potential link with a calcium-specific appetite control. Br. J. Nutr. 2008, 101, 659–663. [Google Scholar] [CrossRef]
- Rodriguez-Rodriguez, E.; Perea, J.M.; Lopez-Sobaler, A.M.; Ortega, R.M.; Research, G. An adequate calcium intake could help achieve weight loss in overweight/obese women following hypocaloric diets. Ann. Nutr. Metab. 2010, 57, 95–102. [Google Scholar] [CrossRef]
- Subih, H.S.; Zueter, Z.; Obeidat, B.M.; Al-Qudah, M.A.; Janakat, S.; Hammoh, F.; Sharkas, G.; Bawadi, H.A. A high weekly dose of cholecalciferol and calcium supplement enhances weight loss and improves health biomarkers in obese women. Nutr. Res. 2018, 59, 53–64. [Google Scholar] [CrossRef]
- Zemel, M.B. Regulation of adiposity and obesity risk by dietary calcium: Mechanisms and implications. J. Am. Coll. Nutr. 2002, 21, 146S–151S. [Google Scholar] [CrossRef]
- Zhu, W.; Cai, D.; Wang, Y.; Lin, N.; Hu, Q.; Qi, Y.; Ma, S.; Amarasekara, S. Calcium plus vitamin d3 supplementation facilitated fat loss in overweight and obese college students with very-low calcium consumption: A randomized controlled trial. Nutr. J. 2013, 12, 8. [Google Scholar] [CrossRef]
- Pereira, M.A.; Jacobs, J.; David, R.; Van Horn, L.; Slattery, M.L.; Kartashov, A.I.; Ludwig, D.S. Dairy consumption, obesity, and the insulin resistance syndrome in young adultsthe cardia study. JAMA 2002, 287, 2081–2089. [Google Scholar] [CrossRef]
- Faghih, S.; Abadi, A.R.; Hedayati, M.; Kimiagar, S.M. Comparison of the effects of cows’ milk, fortified soy milk, and calcium supplement on weight and fat loss in premenopausal overweight and obese women. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 499–503. [Google Scholar] [CrossRef]
- Rosado, J.L.; Garcia, O.P.; Ronquillo, D.; Hervert-Hernandez, D.; Caamano Mdel, C.; Martinez, G.; Gutierrez, J.; Garcia, S. Intake of milk with added micronutrients increases the effectiveness of an energy-restricted diet to reduce body weight: A randomized controlled clinical trial in mexican women. J. Am. Diet Assoc. 2011, 111, 1507–1516. [Google Scholar] [CrossRef]
- Shahar, D.R.; Schwarzfuchs, D.; Fraser, D.; Vardi, H.; Thiery, J.; Fiedler, G.M.; Bluher, M.; Stumvoll, M.; Stampfer, M.J.; Shai, I.; et al. Dairy calcium intake, serum vitamin d, and successful weight loss. Am. J. Clin. Nutr. 2010, 92, 1017–1022. [Google Scholar] [PubMed]
- Wyatt, H.R.; Jortberg, B.T.; Babbel, C.; Garner, S.; Dong, F.; Grunwald, G.K.; Hill, J.O. Weight loss in a community initiative that promotes decreased energy intake and increased physical activity and dairy consumption: Calcium weighs-in. J. Phys. Act. Health 2008, 5, 28–44. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-C.; Lyle, R.M.; McCabe, L.D.; McCabe, G.P.; Weaver, C.M.; Teegarden, D. Dairy calcium is related to changes in body composition during a two-year exercise intervention in young women. J. Am. Coll. Nutr. 2000, 19, 754–760. [Google Scholar] [CrossRef]
- Poddar, K.H.; Hosig, K.W.; Nickols-Richardson, S.M.; Anderson, E.S.; Herbert, W.G.; Duncan, S.E. Low-fat dairy intake and body weight and composition changes in college students. J. Am. Diet Assoc. 2009, 109, 1433–1438. [Google Scholar] [CrossRef]
- Dicker, D.; Belnic, Y.; Goldsmith, R.; Kaluski, D.N. Relationship between dietary calcium intake, body mass index, and waist circumference in mabat—The israeli national health and nutrition study. Israel Med. Assoc. J. 2008, 10, 512–515. [Google Scholar]
- Tidwell, D.K.; Valliant, M.W. Higher amounts of body fat are associated with inadequate intakes of calcium and vitamin d in african american women. Nutr. Res. 2011, 31, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Zemel, M.B.; Teegarden, D.; Loan, M.V.; Schoeller, D.A.; Matkovic, V.; Lyle, R.M.; Craig, B.A. Dairy-rich diets augment fat loss on an energy-restricted diet: A multicenter trial. Nutrients 2009, 1, 83–100. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Pan, A.; Malik, V.S.; Hu, F.B. Effects of dairy intake on body weight and fat: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2012, 96, 735–747. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.W.; Eller, L.K.; Parnell, J.A.; Doyle-Baker, P.K.; Edwards, A.L.; Reimer, R.A. Effect of a dairy- and calcium-rich diet on weight loss and appetite during energy restriction in overweight and obese adults: A randomized trial. Eur. J. Clin. Nutr. 2013, 67, 371–376. [Google Scholar] [CrossRef]
- Smilowitz, J.T.; Wiest, M.M.; Teegarden, D.; Zemel, M.B.; German, J.B.; Van Loan, M.D. Dietary fat and not calcium supplementation or dairy product consumption is associated with changes in anthropometrics during a randomized, placebo-controlled energy-restriction trial. Nutr. Metab. 2011, 8, 67. [Google Scholar] [CrossRef] [PubMed]
- Shapses, S.A.; Heshka, S.; Heymsfield, S.B. Effect of calcium supplementation on weight and fat loss in women. J. Clin. Endocrinol. Metab. 2004, 89, 632–637. [Google Scholar] [CrossRef]
- Wagner, G.; Kindrick, S.; Hertzler, S.; DiSilvestro, R.A. Effects of various forms of calcium on body weight and bone turnover markers in women participating in a weight loss program. J. Am. Coll. Nutr. 2007, 26, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Lappe, J.M.; McMahon, D.J.; Laughlin, A.; Hanson, C.; Desmangles, J.C.; Begley, M.; Schwartz, M. The effect of increasing dairy calcium intake of adolescent girls on changes in body fat and weight. Am. J. Clin. Nutr. 2017, 105, 1046–1053. [Google Scholar] [CrossRef] [Green Version]
- Lukaszuk, J.M.; Luebbers, P.; Gordon, B.A. Preliminary study: Soy milk as effective as skim milk in promoting weight loss. J. Am. Diet Assoc. 2007, 107, 1811–1814. [Google Scholar] [CrossRef]
- Lanou, A.J.; Barnard, N.D. Dairy and weight loss hypothesis: An evaluation of the clinical trials. Nutr. Rev. 2008, 66, 272–279. [Google Scholar] [CrossRef]
- Shin, H.; Shin, J.; Liu, P.Y.; Dutton, G.R.; Abood, D.A.; Ilich, J.Z. Self-efficacy improves weight loss in overweight/obese postmenopausal women during a 6-month weight loss intervention. Nutr. Res. 2011, 31, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M.A.; Brownell, K.D. A comprehensive treatment manual for the management of obesity. In Sourcebook of Psychological Treatment Manuals for Adult Disorders; Van Hasselt, V.B., Hersen, M., Eds.; Springer US: Boston, MA, USA, 1996; pp. 375–422. [Google Scholar]
- Perri, M.G.; Nezu, A.M.; McKelvey, W.F.; Shermer, R.L.; Renjilian, D.A.; Viegener, B.J. Relapse prevention training and problem-solving therapy in the long-term management of obesity. J. Consult. Clin. Psychol. 2001, 69, 722–726. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2010, 7th ed.; U.S. Government Printing Office: Washington, DC, USA, 2010. [Google Scholar]
- Mifflin, M.D.; St Jeor, S.T.; Hill, L.A.; Scott, B.J.; Daugherty, S.A.; Koh, Y.O. A new predictive equation for resting energy expenditure in healthy individuals. Am. J. Clin. Nutr. 1990, 51, 241–247. [Google Scholar] [CrossRef]
- Brownbill, R.A.; Ilich, J.Z. Measuring body composition in overweight individuals by dual energy X-ray absorptiometry. BMC Med. Imaging 2005, 5, 1. [Google Scholar] [CrossRef]
- Carter, A.N.; Ralston, P.A.; Young-Clark, I.; Ilich, J.Z. Diabetic indicators are the strongest predictors for cardiovascular disease risk in african american adults. Am. J. Cardiovasc. Dis. 2016, 6, 129–137. [Google Scholar]
- Ilich, J.Z.; Blanusa, M.; Orlic, Z.C.; Orct, T.; Kostial, K. Comparison of calcium, magnesium, sodium, potassium, zinc, and creatinine concentration in 24-h and spot urine samples in women. Clin. Chem. Lab. Med. 2009, 47, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Ilich, J.Z.; Brownbill, R.A.; Coster, D.C. Higher habitual sodium intake is not detrimental for bones in older women with adequate calcium intake. Eur. J. Appl. Physiol. 2010, 109, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Lemacks, J.L.; Ilich, J.Z.; Liu, P.-Y.; Shin, H.; Ralston, P.A.; Cui, M.; Wickrama, K.A.S. Dietary influence on calcitropic hormones and adiposity in caucasian and african american postmenopausal women assessed by structural equation modeling (sem). J. Nutr. Health Aging 2016, 20, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Brownbill, R.A.; Lindsey, C.; Crncevic-Orlic, Z.; Ilich, J.Z. Dual hip bone mineral density in postmenopausal women: Geometry and effect of physical activity. Calcif. Tissue Int. 2003, 73, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Ilich, J.Z.; Brownbill, R.A. Habitual and low-impact activities are associated with better bone outcomes and lower body fat in older women. Calcif. Tissue Int. 2008, 83, 260–271. [Google Scholar] [CrossRef]
- Bouchard, C.; Tremblay, A.; Leblanc, C.; Lortie, G.; Savard, R.; Theriault, G. A method to assess energy expenditure in children and adults. Am. J. Clin. Nutr. 1983, 37, 461–467. [Google Scholar] [CrossRef]
- Li, P.; Stuart, E.A. Best (but oft-forgotten) practices: Missing data methods in randomized controlled nutrition trials. Am. J. Clin. Nutr. 2019, 109, 504–508. [Google Scholar] [CrossRef]
- Sinharay, S.; Stern, H.S.; Russell, D. The use of multiple imputation for the analysis of missing data. Psychol. Methods 2001, 6, 317–329. [Google Scholar] [CrossRef]
- Zemel, M.B.; Thompson, W.; Milstead, A.; Morris, K.; Campbell, P. Calcium and dairy acceleration of weight and fat loss during energy restriction in obese adults. Obes. Res. 2004, 12, 582–590. [Google Scholar] [CrossRef]
- Compston, J.E.; Laskey, M.A.; Croucher, P.I.; Coxon, A.; Kreitzman, S. Effect of diet-induced weight loss on total body bone mass. Clin. Sci. 1992, 82, 429–432. [Google Scholar] [CrossRef] [Green Version]
- Pritchard, J.E.; Nowson, C.; Wark, J.D. Bone loss accompanying diet-induced or exercise-induced weight loss: A randomised controlled study. Int. J. Obes. 1996, 20, 513–520. [Google Scholar]
- Ilich, J.Z. A lighter side of calcium: Role of calcium and dairy foods in body weight. Arhiv Higijenu Rada Toksikologiju 2005, 56, 33–38. [Google Scholar]
- Radak, T.L. Caloric restriction and calcium’s effect on bone metabolism and body composition in overweight and obese premenopausal women. Nutr. Rev. 2004, 62, 468–481. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin d from the institute of medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, 9th ed.; American Society for Bone and Mineral Research: Hoboken, NJ, USA, 2018.
- Schousboe, J.T.; Bauer, D.C. Clinical use of bone turnover markers to monitor pharmacologic fracture prevention therapy. Curr. Osteoporos. Rep. 2012, 10, 56–63. [Google Scholar] [CrossRef]
- Wheater, G.; Elshahaly, M.; Tuck, S.P.; Datta, H.K.; van Laar, J.M. The clinical utility of bone marker measurements in osteoporosis. J. Transl. Med. 2013, 11, 201. [Google Scholar] [CrossRef] [PubMed]
- Shea, K.L.; Barry, D.W.; Sherk, V.D.; Hansen, K.C.; Wolfe, P.; Kohrt, W.M. Calcium supplementation and parathyroid hormone response to vigorous walking in postmenopausal women. Med. Sci. Sports Exerc. 2014, 46, 2007–2013. [Google Scholar] [CrossRef]
- Zikan, V.; Haas, T.; Stepan, J.J. Acute effects in healthy women of oral calcium on the calcium-parathyroid axis and bone resorption as assessed by serum beta-crosslaps. Calcif. Tissue Int. 2001, 68, 352–357. [Google Scholar] [CrossRef]
- McCarty, M.F. Elevated sympathetic activity may promote insulin resistance syndrome by activating alpha-1 adrenergic receptors on adipocytes. Med. Hypotheses 2004, 62, 830–838. [Google Scholar] [CrossRef] [PubMed]
- McCarty, M.F.; Thomas, C.A. Pth excess may promote weight gain by impeding catecholamine-induced lipolysis-implications for the impact of calcium, vitamin d, and alcohol on body weight. Med. Hypotheses 2003, 61, 535–542. [Google Scholar] [CrossRef]
- Pfeifer, M.; Begerow, B.; Minne, H.W.; Nachtigall, D.; Hansen, C. Effects of a short-term vitamin d(3) and calcium supplementation on blood pressure and parathyroid hormone levels in elderly women. J. Clin. Endocrinol. Metab. 2001, 86, 1633–1637. [Google Scholar] [PubMed]
- Ricci, T.A.; Chowdhury, H.A.; Heymsfield, S.B.; Stahl, T.; Pierson, R.N., Jr.; Shapses, S.A. Calcium supplementation suppresses bone turnover during weight reduction in postmenopausal women. J. Bone Miner. Res. 1998, 13, 1045–1050. [Google Scholar] [CrossRef] [PubMed]
- Riggs, B.L.; O’Fallon, W.M.; Muhs, J.; O’Connor, M.K.; Kumar, R.; Melton, L.J. Long-term effects of calcium supplementation on serum parathyroid hormone level, bone turnover, and bone loss in elderly women. J. Bone Miner. Res. 1998, 13, 168–174. [Google Scholar] [CrossRef]
- Gunther, C.W.; McCabe, G.P.; Eagan, M.S.; Peacock, M.; Legowski, P.A.; Lyle, R.M.; Teegarden, D. Dairy products do not lead to alterations in body weight or fat mass in young women in a 1-y intervention. Am. J. Clin. Nutr. 2005, 81, 751–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Josse, A.R.; Atkinson, S.A.; Tarnopolsky, M.A.; Phillips, S.M. Diets higher in dairy foods and dietary protein support bone health during diet- and exercise-induced weight loss in overweight and obese premenopausal women. J. Clin. Endocrinol. Metab. 2012, 97, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Bowen, J.; Noakes, M.; Clifton, P.M. A high dairy protein, high-calcium diet minimizes bone turnover in overweight adults during weight loss. J. Nutr. 2004, 134, 568–573. [Google Scholar] [CrossRef]
- Karsenty, G.; Ferron, M. The contribution of bone to whole-organism physiology. Nature 2012, 481, 314–320. [Google Scholar] [CrossRef]
- Mantzoros, C.S.; Magkos, F.; Brinkoetter, M.; Sienkiewicz, E.; Dardeno, T.A.; Kim, S.Y.; Hamnvik, O.P.; Koniaris, A. Leptin in human physiology and pathophysiology. Am. J. Physiol. Endocrinol. Metab. 2011, 301, E567–584. [Google Scholar] [CrossRef] [PubMed]
- Castro, J.P.; Joseph, L.A.; Shin, J.J.; Arora, S.K.; Nicasio, J.; Shatzkes, J.; Raklyar, I.; Erlikh, I.; Pantone, V.; Bahtiyar, G.; et al. Differential effect of obesity on bone mineral density in white, hispanic and african american women: A cross sectional study. Nutr. Metab. 2005, 2, 9. [Google Scholar] [CrossRef]
- Douchi, T.; Yamamoto, S.; Oki, T.; Maruta, K.; Kuwahata, R.; Yamasaki, H.; Nagata, Y. Difference in the effect of adiposity on bone density between pre- and postmenopausal women. Maturitas 2000, 34, 261–266. [Google Scholar] [CrossRef]
- Rico, H.; Arribas, I.; Casanova, F.J.; Duce, A.M.; Herna’ndez, E.R.; Cortes-Prieto, J.J.O.I. Bone mass, bone metabolism, gonadal status and body mass index. Osteoporos. Int. 2002, 13, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Travison, T.G.; Araujo, A.B.; Esche, G.R.; McKinlay, J.B. The relationship between body composition and bone mineral content: Threshold effects in a racially and ethnically diverse group of men. Osteoporos. Int. 2008, 19, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Waning, D.L.; Mohammad, K.S.; Reiken, S.; Xie, W.; Andersson, D.C.; John, S.; Chiechi, A.; Wright, L.E.; Umanskaya, A.; Niewolna, M.; et al. Excess tgf-beta mediates muscle weakness associated with bone metastases in mice. Nat. Med. 2015, 21, 1262–1271. [Google Scholar] [CrossRef] [PubMed]
- van Dronkelaar, C.; van Velzen, A.; Abdelrazek, M.; van der Steen, A.; Weijs, P.J.M.; Tieland, M. Minerals and sarcopenia; the role of calcium, iron, magnesium, phosphorus, potassium, selenium, sodium, and zinc on muscle mass, muscle strength, and physical performance in older adults: A systematic review. J. Am. Med. Dir. Assoc. 2018, 19, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Klein, G.L. The role of bone secreted factors in burn-induced muscle cachexia. Curr. Osteoporos. Rep. 2018, 16, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Stonehouse, W.; Wycherley, T.; Luscombe-Marsh, N.; Taylor, P.; Brinkworth, G.; Riley, M. Dairy intake enhances body weight and composition changes during energy restriction in 18-50-year-old adults-a meta-analysis of randomized controlled trials. Nutrients 2016, 8, 349. [Google Scholar] [CrossRef]
- Geng, T.; Qi, L.; Huang, T. Effects of dairy products consumption on body weight and body composition among adults: An updated meta-analysis of 37 randomized control trials. Mol. Nutr. Food Res. 2018, 62, 1700410. [Google Scholar] [CrossRef]
- Abargouei, A.S.; Janghorbani, M.; Salehi-Marzijarani, M.; Esmaillzadeh, A. Effect of dairy consumption on weight and body composition in adults: A systematic review and meta-analysis of randomized controlled clinical trials. Int. J. Obes. 2012, 36, 1485–1493. [Google Scholar] [CrossRef]
- Zemel, M.B. Mechanisms of dairy modulation of adiposity. J. Nutr. 2003, 133, 252S–256S. [Google Scholar] [CrossRef]
- Zemel, M.B.; Shi, H.; Greer, B.; Dirienzo, D.; Zemel, P.C. Regulation of adiposity by dietary calcium. FASEB J. 2000, 14, 1132–1138. [Google Scholar] [CrossRef]
- Fujita, T.; Palmieri, G.M.A.J.J.O.B.; Metabolism, M. Calcium paradox disease: Calcium deficiency prompting secondary hyperparathyroidism and cellular calcium overload. J. Bone Miner. Metab. 2000, 18, 109–125. [Google Scholar] [CrossRef]
- Frestedt, J.L.; Zenk, J.L.; Kuskowski, M.A.; Ward, L.S.; Bastian, E.D. A whey-protein supplement increases fat loss and spares lean muscle in obese subjects: A randomized human clinical study. Nutr. Metab. 2008, 5, 8. [Google Scholar] [CrossRef]
- Egras, A.M.; Hamilton, W.R.; Lenz, T.L.; Monaghan, M.S. An evidence-based review of fat modifying supplemental weight loss products. J. Obes. 2011, 2011. [Google Scholar] [CrossRef]
- Layman, D.K. The role of leucine in weight loss diets and glucose homeostasis. J. Nutr. 2003, 133, 261S–267S. [Google Scholar] [CrossRef]
- Dougkas, A.; Barr, S.; Reddy, S.; Summerbell, C.D. A critical review of the role of milk and other dairy products in the development of obesity in children and adolescents. Nutr. Res. Rev. 2018, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Sonestedt, E.; Wirfält, E.; Wallström, P.; Gullberg, B.; Orho-Melander, M.; Hedblad, B. Dairy products and its association with incidence of cardiovascular disease: The malmö diet and cancer cohort. Eur. J. Epidemiol. 2011, 26, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Choi, H.K.; Ford, E.; Song, Y.; Klevak, A.; Buring, J.E.; Manson, J.E. A prospective study of dairy intake and the risk of type 2 diabetes in women. Diabetes Care 2006, 29, 1579–1584. [Google Scholar] [CrossRef] [PubMed]
- Thorning, T.K.; Raben, A.; Tholstrup, T.; Soedamah-Muthu, S.S.; Givens, I.; Astrup, A. Milk and dairy products: Good or bad for human health? An assessment of the totality of scientific evidence. Food Nutr. Res. 2016, 60, 32527. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Baseline Sample (n = 135) | Noncontinuing (n = 54) | |
|---|---|---|---|
| Age (y) | 55.8 ± 4.3 | 55.9 ± 3.6 | |
| Years Since Menopause (y) | 6.1 ± 2.8 | 5.8 ± 2.6 | |
| Anthropometry/Body Composition | |||
| Weight (kg) | 84.2 ± 14.0 | 82.4 ± 10.4 | |
| Height (cm) | 163.5 ± 5.5 | 162.6 ± 5.3 | |
| Body Mass Index (kg/m2) | 31.5 ± 5.1 | 30.7 ± 4.2 | |
| Waist Circumference (cm) | 97.2 ± 11.3 | 96.4 ± 10.2 | |
| Abdominal Circumference (cm) | 110.3 ± 12.3 | 108 ± 12.0 | |
| Hip Circumference (cm) | 117.1 ± 11.3 | 116.5 ± 10.8 | |
| Total body fat (kg) Total body fat (%) Total body lean mass (kg) | 39.3 ± 11.5 45.9 ± 6.8 42.7 ± 6.9 | 37.7 ± 8.6 45.4 ± 4.5 42.0 ± 5.0 | |
| Android fat (kg) Android fat (%) Android lean (kg) | 3.9 ± 1.4 55.5 ± 8.5 2.9 ± 0.5 | 3.7 ± 1.1 54.8 ± 7.6 2.8 ± 0.4 | |
| Gynoid fat (kg) Gynoid fat (%) Gynoid lean (kg) | 7.6 ± 2.1 55.4 ± 7.5 5.8 ± 1.0 | 7.5 ± 1.7 54.9 ± 4.8 5.7 ± 0.7 | |
| Bone Mineral Density (BMD) (g/cm2) | T-score | ||
| Total Body Lumbar Spine (L2–L4) Femoral Necks * Whole Femurs * Radius 1/3 of Styloid Process * Whole Forearms * | 1.137 ± 0.2 0.989 ± 0.2 0.933 ± 0.1 1.193 ± 0.2 0.685 ± 0.1 0.503 ± 0.1 | 1.133 ± 0.2 0.984 ± 0.2 0.930 ± 0.1 1.189 ± 0.2 0.681 ± 0.1 0.498 ± 0.1 | -- −0.23 ± 1.4 −1.14 ± 1.2 −0.07 ± 1.3 −0.47 ± 1.2 -- |
| Lab Values | Normal range | ||
| Serum PTH (pmol/L) | 3.2 ± 1.7 | 3.1 ± 1.7 | 1.6–6.9 |
| Serum 25(OH)D (nmol/L) | 66.6 ± 27.9 | 66.3 ± 26.0 | 50–125 |
| Serum Osteocalcin (ng/mL) | 19.4 ± 7.1 | 19.5 ± 7.0 | 9–42 |
| Serum NTx (nM BCE) | 16.4 ± 4.4 | 16.0 ± 4.5 | Elevated ≥26 |
| Urine-CTx (ng/L) | 13.8 ± 11.2 | 13.1 ± 11.0 | Not established |
| Urine Ca/Creatinine (mg/24h) | 135.4 ± 71.7 | 129.2 ± 51.8 | 30–275 |
| BMD (g/cm2) * | Baseline | pab | 6 Months | p” | ||||
|---|---|---|---|---|---|---|---|---|
| C | S | D | C | S | D | |||
| Total Body | 1.159 a ± 0.11 | 1.098 b ± 0.10 | 1.123 a ± 0.09 | 1.154 ± 0.11 | 1.096 ± 0.10 | 1.112 ± 0.10 | NS | |
| Lumbar Spine (L2–L4) | 1.201 ± 0.16 | 1.140 ± 0.14 | 1.174 ± 0.14 | NS | 1.176 ± 0.16 | 1.128 ± 0.15 | 1.156 ± 0.14 | NS |
| Femoral Necks | 0.962 a ± 0.13 | 0.888 b ± 0.09 | 0.919 ab ± 0.10 | 0.954 ± 0.12 | 0.896 ± 0.10 | 0.911 ± 0.10 | NS | |
| Whole Femurs | 1.009 a ± 0.12 | 0.942 b ± 0.10 | 0.972 ab ± 0.10 | 1.004 ± 0.11 | 0.951 ± 0.11 | 0.968 ± 0.10 | NS | |
| Radius 1/3 of Styloid Process | 0.700 ± 0.06 | 0.669 ± 0.08 | 0.672 ± 0.06 | NS | 0.695 ± 0.06 | 0.665 ± 0.08 | 0.651 ± 0.07 | NS |
| Whole Forearms | 0.512 a ± 0.05 | 0.485 b ± 0.05 | 0.494 ab ± 0.05 | 0.482” ± 0.05 | 0.482 ± 0.06 | 0.480 ± 0.05 | ||
| Markers of Bone Turnover | ||||||||
| Serum Osteocalcin (ng/mL) | 20.8 ± 7.2 | 20.2 ± 5.9 | 18.4 ± 6.2 | NS | 20.9 ± 8.4 | 19.7 ± 7.3 | 17.8 ± 7.0 | NS |
| Serum NTx (nM BCE) | 17.5 ± 3.9 | 16.5 ± 3.1 | 15.7 ± 4.8 | NS | 16.1 ± 4.7 | 15.0 ± 5.6 | 15.7 ± 4.6 | NS |
| Urinary CTx | 14.3 a ± 8.6 | 14.7 a ± 11.5 | 11.4 b ± 7.5 | 17.3” ± 15.7 | 11.7” ± 9.7 | 12.2 ± 10.6 | ||
| Serum Markers | ||||||||
| Serum PTH (pmol/L) | 3.0 ± 1.4 | 3.1 ± 1.7 | 3.2 ± 1.8 | NS | 3.5 ± 1.3 | 2.8” ± 1.2 | 3.0 ± 0.9 | |
| Serum 25(OH)D (nmol/L) | 65.8 ± 24.4 | 70.7 ± 32.7 | 66.6 ± 27.5 | NS | 71.9 ± 30.9 | 83.0” ± 23.4 | 82.8” ± 46.8 | |
| Variable | Baseline | 6 Months | ||||||
|---|---|---|---|---|---|---|---|---|
| C | S | D | pab | C | S | D | p” | |
| Nutrients † | ||||||||
| Energy (kcal/day) | 1744.4 ± 383.9 | 1781.0 ± 420.9 | 1782.2 ± 473.4 | NS | 1375.3” ± 367.7 | 1367.7” ± 340.2 | 1502.1” ± 342.2 | |
| Protein (g/day) | 70.4 ± 16.9 | 76.0 ± 21.1 | 75.4 ± 22.0 | NS | 63.8” ± 13.7 | 66.0” ± 17.6 | 75.1 ± 23.8 | |
| Protein (g/kg/day) | 0.87 ± 1.7 | 0.93 ± 1.5 | 0.91 ± 1.6 | NS | 0.73” ± 1.8 | 0.86 ± 1.6 | 0.98 ± 1.7 | |
| Carb (g/day) | 210.7 ± 55.2 | 208.0 ± 66.3 | 208.4 ± 59.5 | NS | 169.2” ± 61.9 | 164.8” ± 44.1 | 187.2 ± 44.7 | |
| Fat (g/day) | 67.3 ± 19.6 | 69.4 ± 20.0 | 69.3 ± 29.9 | NS | 48.6” ± 17.1 | 49.3” ± 22.6 | 50.8” ± 24.3 | |
| Total calcium (mg/day) * | 863.9 a ± 323.6 | 910.5 ab ± 493.1 | 942.4 b ± 334.9 | 712.0” ± 236.0 | 1672.3” ± 494.6 | 1170.0” ± 476.7 | ||
| Total vitamin D (IU/day) * | 372.3 a ± 304.8 | 276.0 b ± 270.0 | 382.4 a ± 290.0 | 382.8 ± 454.2 | 808.6” ± 401.0 | 375.8” ± 255.1 | ||
| Physical activity (hr/week) †† | ||||||||
| Housework | 1.3 ± 1.4 | 1.5 ± 1.6 | 1.5 ± 1.7 | NS | 1.6 ± 1.5 | 2.1 ± 1.7 | 1.6 ± 1.3 | NS |
| Gardening | 1.7 ± 2.8 | 1.4 ± 2.6 | 1.3 ± 1.9 | NS | 1.0 ± 1.2 | 1.3 ± 2.2 | 2.0 ± 3.0 | NS |
| Do-it-yourself | 0.2 ± 0.4 | 0.3 ± 0.7 | 0.2 ± 0.6 | NS | 0.1 ± 0.2 | 0.3 ± 0.7 | 0.4 ± 0.7 | NS |
| Walking | 2.4 ± 3.2 | 1.7 ± 2.7 | 1.9 ± 3.3 | NS | 2.8 ± 2.9 | 3.0 ± 3.4” | 3.4 ± 3.6” | |
| Recreation | 3.1 ± 6.2 | 2.5 ± 3.4 | 3.1 ± 3.3 | NS | 2.2 ± 2.5 | 4.3 ± 5.7” | 3.6 ± 4.3 | NS |
| Total Activity | 8.4 ± 8.5 | 7.3 ± 6.5 | 8.1 ± 5.5 | NS | 7.7 ± 4.4 | 11.0 ± 8.1” | 11.1 ± 8.0” | |
| MET | 44.0 ± 4.6 | 43.8 ± 5.3 | 44.6 ± 6.1 | NS | 43.4 ± 19.3 | 62.5 ± 18.9” | 64.9 ± 21.3” | |
| Total Fat | Stand Beta | t | p | Android Fat | Stand Beta | t | p | Total Lean | Stand Beta | t | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Constant | 0.197 | 0.845 | Constant | 0.56 | 0.955 | Constant | −1.296 | 0.201 | |||
| Age | −0.098 | −0.777 | 0.441 | Age | −0.080 | −0.625 | 0.535 | Age | 0.129 | 1.001 | 0.322 |
| MET | 0.278 | 2.049 | 0.046 | MET | 0.272 | 1.979 | 0.053 | MET | −0.169 | −1.214 | 0.203 |
| 25(OH)D | −0.184 | −1.430 | 0.159 | 25(OH)D | −0.173 | −1.326 | 0.191 | 25(OH)D | 0.297 | 2.249 | 0.029 |
| Ca/Creat | −0.385 | −2.869 | 0.060 | Ca/Creat | −0.362 | −2.671 | 0.010 | Ca/Creat | 0.174 | 1.270 | 0.210 |
| Dairy Gr | −0.242 | −1.923 | 0.060 | Dairy Gr | −0.249 | −1.956 | 0.056 | Dairy Gr | 0.243 | 1.889 | 0.065 |
| Femoral Neck BMD | Stand Beta | t | p | Whole femurs BMD | Stand Beta | t | p |
|---|---|---|---|---|---|---|---|
| Constant | −0.235 | 0.815 | Constant | −0.020 | 0.984 | ||
| Age | 0.048 | 0.375 | 0.709 | Age | −0.010 | −0.082 | 0.935 |
| MET | −0.110 | −0.837 | 0.406 | MET | −0.066 | −0.511 | 0.611 |
| 25(OH)D | 0.027 | 0.200 | 0.842 | 25(OH)D | −0.038 | −0.294 | 0.770 |
| Ca/Creatinine | 0.219 | 1.555 | 0.125 | Ca/Creat | 0.296 | 2.158 | 0.035 |
| Supplement Gr | 0.276 | 1.973 | 0.058 | Supplement Gr | 0.234 | 1.946 | 0.063 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilich, J.Z.; Kelly, O.J.; Liu, P.-Y.; Shin, H.; Kim, Y.; Chi, Y.; Wickrama, K.K.A.S.; Colic-Baric, I. Role of Calcium and Low-Fat Dairy Foods in Weight-Loss Outcomes Revisited: Results from the Randomized Trial of Effects on Bone and Body Composition in Overweight/Obese Postmenopausal Women. Nutrients 2019, 11, 1157. https://doi.org/10.3390/nu11051157
Ilich JZ, Kelly OJ, Liu P-Y, Shin H, Kim Y, Chi Y, Wickrama KKAS, Colic-Baric I. Role of Calcium and Low-Fat Dairy Foods in Weight-Loss Outcomes Revisited: Results from the Randomized Trial of Effects on Bone and Body Composition in Overweight/Obese Postmenopausal Women. Nutrients. 2019; 11(5):1157. https://doi.org/10.3390/nu11051157
Chicago/Turabian StyleIlich, Jasminka Z., Owen J. Kelly, Pei-Yang Liu, Hyehyung Shin, Youjin Kim, Yichih Chi, Kandauda K. A. S. Wickrama, and Irena Colic-Baric. 2019. "Role of Calcium and Low-Fat Dairy Foods in Weight-Loss Outcomes Revisited: Results from the Randomized Trial of Effects on Bone and Body Composition in Overweight/Obese Postmenopausal Women" Nutrients 11, no. 5: 1157. https://doi.org/10.3390/nu11051157