Effect of Weight Loss after Bariatric Surgery on Thyroid-Stimulating Hormone Levels in Euthyroid Patients with Morbid Obesity

 ,
,  , and
, and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients and Controls
2.2. Study Procedure
2.3. Assays and Other Methods
2.4. Calculations
2.5. Statistical Analysis
3. Results
3.1. Preoperative Characteristics of the Study Population and the Control Group
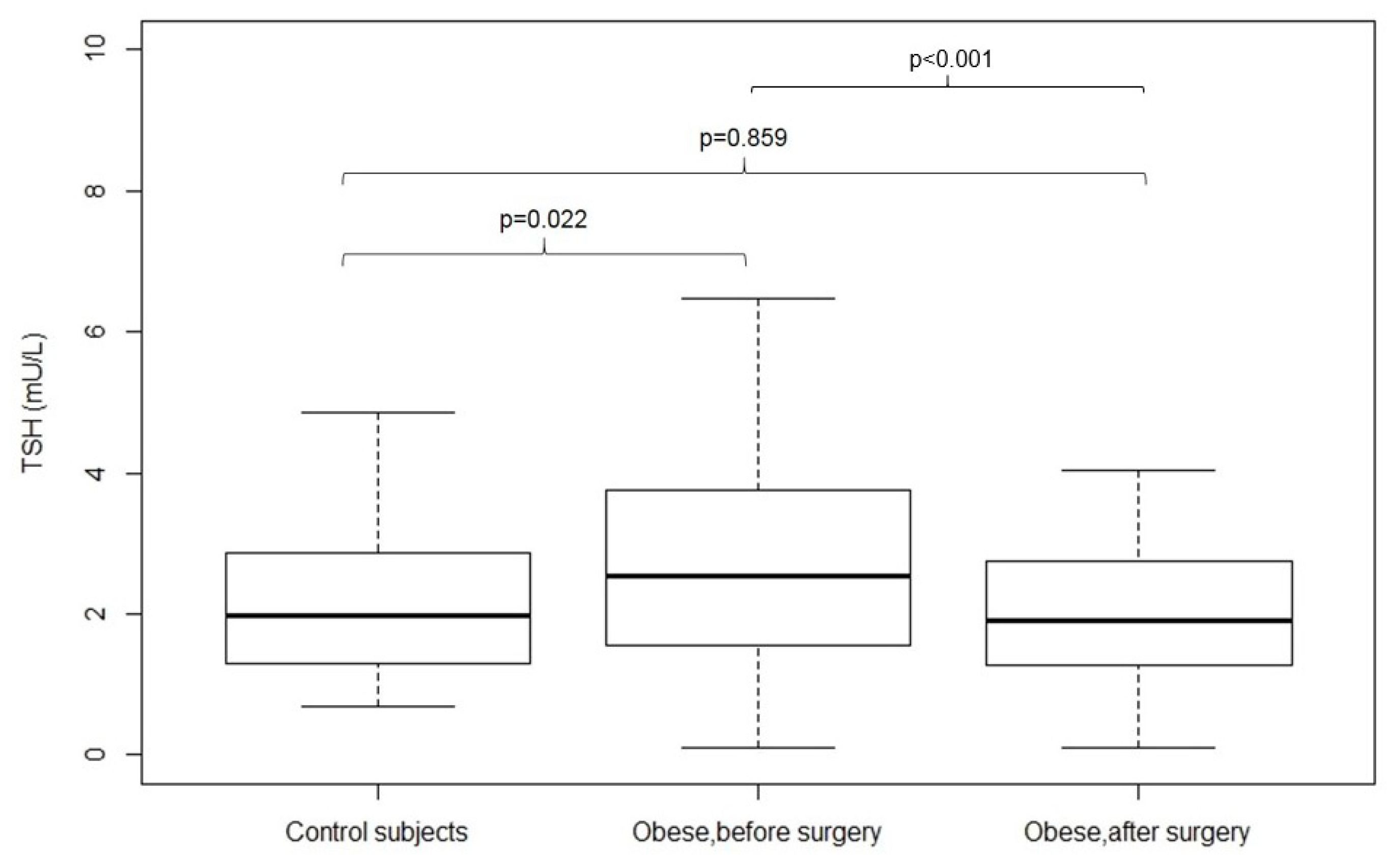
3.2. Fasting Serum Levels
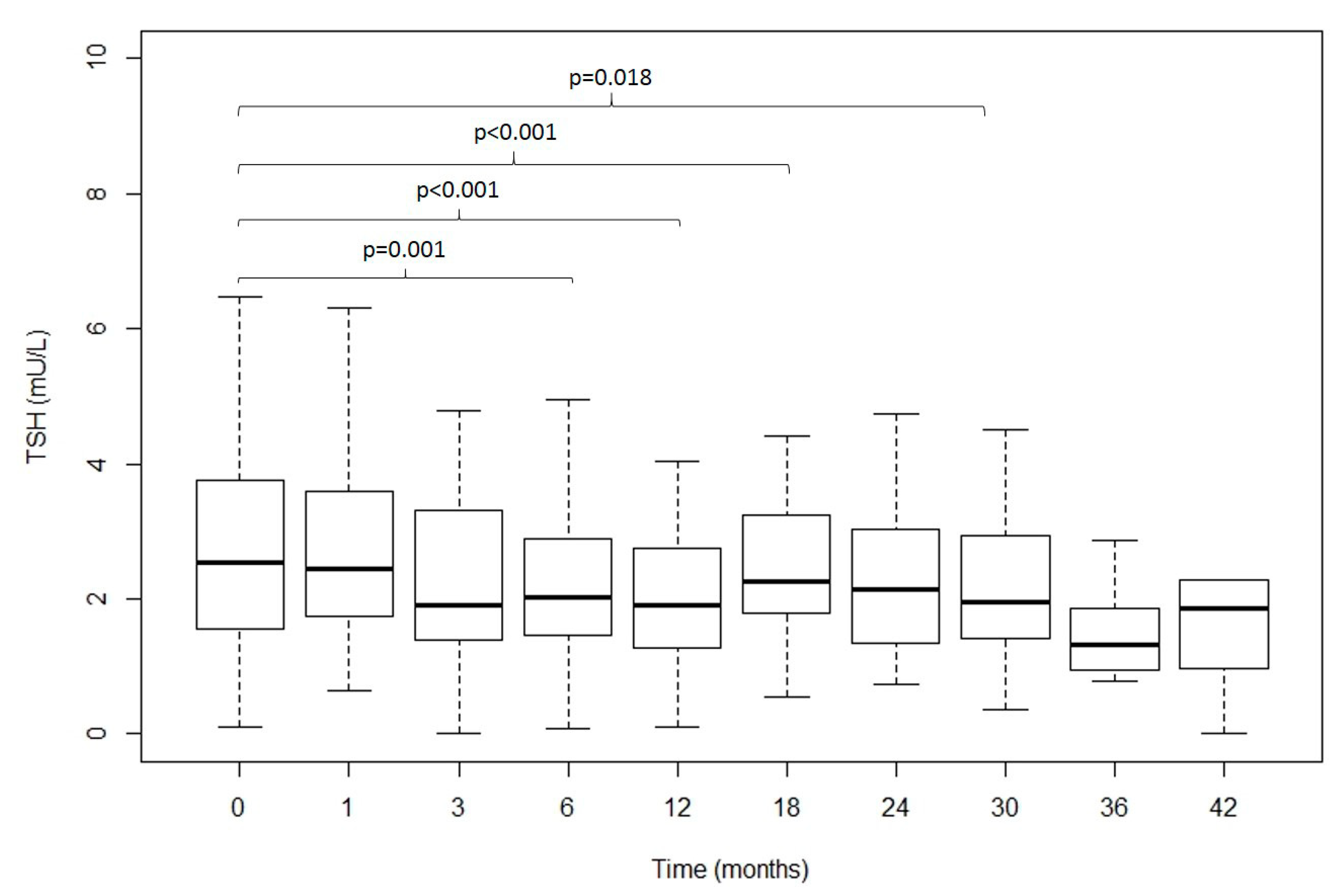
3.3. Evolution over Time of the Clinical and Analytical Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- GBD 2015 Obesity Collaborators. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Flegal, K.M.; Kruszon-Moran, D.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Trends in Obesity Among Adults in the United States, 2005 to 2014. JAMA 2016, 315, 2284–2291. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Fisac, J.L.; Guallar-Castillon, P.; Leon-Munoz, L.M.; Graciani, A.; Banegas, J.R.; Rodriguez-Artalejo, F. Prevalence of general and abdominal obesity in the adult population of Spain, 2008–2010: The ENRICA study. Obes. Rev. 2012, 13, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Magkos, F.; Fraterrigo, G.; Yoshino, J.; Luecking, C.; Kirbach, K.; Kelly, S.C.; de Las Fuentes, L.; He, S.; Okunade, A.L.; Patterson, B.W.; et al. Effects of Moderate and Subsequent Progressive Weight Loss on Metabolic Function and Adipose Tissue Biology in Humans with Obesity. Cell Metab. 2016, 23, 591–601. [Google Scholar] [CrossRef]
- Reges, O.; Greenland, P.; Dicker, D.; Leibowitz, M.; Hoshen, M.; Gofer, I.; Rasmussen-Torvik, L.J.; Balicer, R.D. Association of Bariatric Surgery Using Laparoscopic Banding, Roux-en-Y Gastric Bypass, or Laparoscopic Sleeve Gastrectomy vs Usual Care Obesity Management With All-Cause Mortality. JAMA 2018, 319, 279–290. [Google Scholar] [CrossRef] [PubMed]
- Pena-Bello, L.; Seoane-Pillado, T.; Sangiao-Alvarellos, S.; Outeirino-Blanco, E.; Varela-Rodriguez, B.; Juiz-Valina, P.; Cordido, M.; Cordido, F. Oral glucose-stimulated growth hormone (GH) test in adult GH deficiency patients and controls: Potential utility of a novel test. Eur. J. Int. Med. 2017, 44, 55–61. [Google Scholar] [CrossRef]
- Pena-Bello, L.; Pertega-Diaz, S.; Outeirino-Blanco, E.; Garcia-Buela, J.; Tovar, S.; Sangiao-Alvarellos, S.; Dieguez, C.; Cordido, F. Effect of oral glucose administration on rebound growth hormone release in normal and obese women: The role of adiposity, insulin sensitivity and ghrelin. PLoS ONE 2015, 10, e0121087. [Google Scholar] [CrossRef]
- Alvarez-Castro, P.; Sangiao-Alvarellos, S.; Brandon-Sanda, I.; Cordido, F. Endocrine function in obesity. Endocrinol. Nutr. 2011, 58, 422–432. [Google Scholar] [CrossRef] [PubMed]
- Biondi, B. Thyroid and obesity: An intriguing relationship. J. Clin. Endocrinol. Metab. 2010, 95, 3614–3617. [Google Scholar] [CrossRef]
- Reinehr, T. Obesity and thyroid function. Mol. Cell Endocrinol. 2010, 316, 165–171. [Google Scholar] [CrossRef]
- Rotondi, M.; Leporati, P.; La Manna, A.; Pirali, B.; Mondello, T.; Fonte, R.; Magri, F.; Chiovato, L. Raised serum TSH levels in patients with morbid obesity: Is it enough to diagnose subclinical hypothyroidism? Eur. J. Endocrinol. 2009, 160, 403–408. [Google Scholar] [CrossRef]
- Reinehr, T.; Andler, W. Thyroid hormones before and after weight loss in obesity. Arch. Dis. Child. 2002, 87, 320–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valdes, S.; Maldonado-Araque, C.; Lago-Sampedro, A.; Lillo-Munoz, J.A.; Garcia-Fuentes, E.; Perez-Valero, V.; Gutierrez-Repiso, C.; Garcia-Escobar, E.; Goday, A.; Urrutia, I.; et al. Reference values for TSH may be inadequate to define hypothyroidism in persons with morbid obesity: [email protected] study. Obesity 2017, 25, 788–793. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Liu, W.; Han, X.; Yu, H.; Zhang, P.; Jia, W. Effect of Laparoscopic Roux-en-Y Gastric Bypass Surgery on Thyroid Hormone Levels in Chinese Patients, Could It Be a Risk for Thyroid Nodules? Obes. Surg. 2017, 27, 2619–2627. [Google Scholar] [CrossRef] [PubMed]
- Guan, B.; Chen, Y.; Yang, J.; Yang, W.; Wang, C. Effect of Bariatric Surgery on Thyroid Function in Obese Patients: A Systematic Review and Meta-Analysis. Obes. Surg. 2017, 27, 3292–3305. [Google Scholar] [CrossRef]
- Yang, J.; Gao, Z.; Yang, W.; Zhou, X.; Lee, S.; Wang, C. Effect of Sleeve Gastrectomy on Thyroid Function in Chinese Euthyroid Obese Patients. Surg. Laparosc. Endosc. Percutan. Tech. 2017, 27, e66–e68. [Google Scholar] [CrossRef]
- Liu, G.; Liang, L.; Bray, G.A.; Qi, L.; Hu, F.B.; Rood, J.; Sacks, F.M.; Sun, Q. Thyroid hormones and changes in body weight and metabolic parameters in response to weight loss diets: The POUNDS LOST trial. Int. J. Obes. 2017, 41, 878–886. [Google Scholar] [CrossRef] [PubMed]
- Neves, J.S.; Oliveira, S.C.; Souteiro, P.; Pedro, J.; Magalhaes, D.; Guerreiro, V.; Bettencourt-Silva, R.; Costa, M.M.; Santos, A.C.; Queiros, J.; et al. Effect of Weight Loss after Bariatric Surgery on Thyroid-Stimulating Hormone Levels in Patients with Morbid Obesity and Normal Thyroid Function. Obes. Surg. 2018, 28, 97–103. [Google Scholar] [CrossRef]
- Dall’Asta, C.; Paganelli, M.; Morabito, A.; Vedani, P.; Barbieri, M.; Paolisso, G.; Folli, F.; Pontiroli, A.E. Weight loss through gastric banding: Effects on TSH and thyroid hormones in obese subjects with normal thyroid function. Obesity 2010, 18, 854–857. [Google Scholar] [CrossRef]
- Santini, F.; Pinchera, A.; Marsili, A.; Ceccarini, G.; Castagna, M.G.; Valeriano, R.; Giannetti, M.; Taddei, D.; Centoni, R.; Scartabelli, G.; et al. Lean body mass is a major determinant of levothyroxine dosage in the treatment of thyroid diseases. J. Clin. Endocrinol. Metab. 2005, 90, 124–127. [Google Scholar] [CrossRef]
- Fallahi, P.; Ferrari, S.M.; Camastra, S.; Politti, U.; Ruffilli, I.; Vita, R.; Navarra, G.; Benvenga, S.; Antonelli, A. TSH Normalization in Bariatric Surgery Patients After the Switch from L-Thyroxine in Tablet to an Oral Liquid Formulation. Obes. Surg. 2017, 27, 78–82. [Google Scholar] [CrossRef]
- Pedro, J.; Cunha, F.; Souteiro, P.; Neves, J.S.; Guerreiro, V.; Magalhaes, D.; Bettencourt-Silva, R.; Oliveira, S.C.; Costa, M.M.; Queiros, J.; et al. The Effect of the Bariatric Surgery Type on the Levothyroxine Dose of Morbidly Obese Hypothyroid Patients. Obes. Surg. 2018, 28, 3538–3543. [Google Scholar] [CrossRef]
- Ylli, D.; Wartofsky, L. Can We Link Thyroid Status, Energy Expenditure, and Body Composition to Management of Subclinical Thyroid Dysfunction? J. Clin. Endocrinol. Metab. 2019, 104, 209–212. [Google Scholar] [CrossRef]
- Endo, T.; Kobayashi, T. Thyroid-stimulating hormone receptor in brown adipose tissue is involved in the regulation of thermogenesis. Am. J. Physiol. Endocrinol. Metab. 2008, 295, E514–E518. [Google Scholar] [CrossRef] [Green Version]
- Nannipieri, M.; Cecchetti, F.; Anselmino, M.; Camastra, S.; Niccolini, P.; Lamacchia, M.; Rossi, M.; Iervasi, G.; Ferrannini, E. Expression of thyrotropin and thyroid hormone receptors in adipose tissue of patients with morbid obesity and/or type 2 diabetes: Effects of weight loss. Int. J. Obes. 2009, 33, 1001–1006. [Google Scholar] [CrossRef]
- Marzullo, P.; Minocci, A.; Mele, C.; Fessehatsion, R.; Tagliaferri, M.; Pagano, L.; Scacchi, M.; Aimaretti, G.; Sartorio, A. The relationship between resting energy expenditure and thyroid hormones in response to short-term weight loss in severe obesity. PLoS ONE 2018, 13, e0205293. [Google Scholar] [CrossRef]
- Betry, C.; Challan-Belval, M.A.; Bernard, A.; Charrie, A.; Drai, J.; Laville, M.; Thivolet, C.; Disse, E. Increased TSH in obesity: Evidence for a BMI-independent association with leptin. Diabetes Metab. 2015, 41, 248–251. [Google Scholar] [CrossRef]
- Marzullo, P.; Minocci, A.; Tagliaferri, M.A.; Guzzaloni, G.; Di Blasio, A.; De Medici, C.; Aimaretti, G.; Liuzzi, A. Investigations of thyroid hormones and antibodies in obesity: Leptin levels are associated with thyroid autoimmunity independent of bioanthropometric, hormonal, and weight-related determinants. J. Clin. Endocrinol. Metab. 2010, 95, 3965–3972. [Google Scholar] [CrossRef]
- Yoshihara, A.; Noh, J.Y.; Watanabe, N.; Iwaku, K.; Kunii, Y.; Ohye, H.; Suzuki, M.; Matsumoto, M.; Suzuki, N.; Sugino, K.; et al. Seasonal Changes in Serum Thyrotropin Concentrations Observed from Big Data Obtained During Six Consecutive Years from 2010 to 2015 at a Single Hospital in Japan. Thyroid 2018, 28, 429–436. [Google Scholar] [CrossRef]
- Das, G.; Taylor, P.N.; Javaid, H.; Tennant, B.P.; Geen, J.; Aldridge, A.; Okosieme, O. Seasonal Variation of Vitamin D and Serum Thyrotropin Levels and Its Relationship in a Euthyroid Caucasian Population. Endocr. Pract. 2018, 24, 53–59. [Google Scholar] [CrossRef]
- Ehrenkranz, J.; Bach, P.R.; Snow, G.L.; Schneider, A.; Lee, J.L.; Ilstrup, S.; Bennett, S.T.; Benvenga, S. Circadian and Circannual Rhythms in Thyroid Hormones: Determining the TSH and Free T4 Reference Intervals Based Upon Time of Day, Age, and Sex. Thyroid 2015, 25, 954–961. [Google Scholar] [CrossRef]
- Roelfsema, F.; Pijl, H.; Kok, P.; Endert, E.; Fliers, E.; Biermasz, N.R.; Pereira, A.M.; Veldhuis, J.D. Thyrotropin Secretion in Healthy Subjects Is Robust and Independent of Age and Gender, and Only Weakly Dependent on Body Mass Index. J. Clin. Endocrinol. Metab. 2014, 99, 570–578. [Google Scholar] [CrossRef] [Green Version]
- Reinehr, T.; de Sousa, G.; Andler, W. Hyperthyrotropinemia in obese children is reversible after weight loss and is not related to lipids. J. Clin. Endocrinol. Metab. 2006, 91, 3088–3091. [Google Scholar] [CrossRef]
- Crujeiras, A.B.; Goyenechea, E.; Abete, I.; Lage, M.; Carreira, M.C.; Martinez, J.A.; Casanueva, F.F. Weight regain after a diet-induced loss is predicted by higher baseline leptin and lower ghrelin plasma levels. J. Clin. Endocrinol. Metab. 2010, 95, 5037–5044. [Google Scholar] [CrossRef]
- Hogild, M.L.; Bak, A.M.; Pedersen, S.B.; Rungby, J.; Frystyk, J.; Moller, N.; Jessen, N.; Jorgensen, J.O.L. Growth Hormone Signaling and Action in Obese versus Lean Human Subjects. Am. J. Physiol. Endocrinol. Metab. 2018, 316, E333–E344. [Google Scholar] [CrossRef]
- Glad, C.A.M.; Svensson, P.A.; Nystrom, F.H.; Jacobson, P.; Carlsson, L.M.S.; Johannsson, G.; Andersson-Assarsson, J.C. Expression of GHR and downstream signaling genes in human adipose tissue—Relation to obesity and weight-change. J. Clin. Endocrinol. Metab. 2018, 104, 1459–1470. [Google Scholar] [CrossRef]
- Giavoli, C.; Profka, E.; Rodari, G.; Lania, A.; Beck-Peccoz, P. Focus on GH deficiency and thyroid function. Best Pract. Res. Clin. Endocrinol. Metab. 2017, 31, 71–78. [Google Scholar] [CrossRef]
- Rodriguez-Arnao, J.; Miell, J.P.; Ross, R.J. Influence of thyroid hormones on the GH-IGF-I axis. Trends Endocrinol. Metab. 1993, 4, 169–173. [Google Scholar] [CrossRef]
- Curto, L.; Giovinazzo, S.; Alibrandi, A.; Campenni, A.; Trimarchi, F.; Cannavo, S.; Ruggeri, R.M. Effects of GH replacement therapy on thyroid volume and nodule development in GH deficient adults: A retrospective cohort study. Eur. J. Endocrinol. 2015, 172, 543–552. [Google Scholar] [CrossRef]
- Yamauchi, I.; Sakane, Y.; Yamashita, T.; Hirota, K.; Ueda, Y.; Kanai, Y.; Yamashita, Y.; Kondo, E.; Fujii, T.; Taura, D.; et al. Effects of growth hormone on thyroid function are mediated by type 2 iodothyronine deiodinase in humans. Endocrine 2018, 59, 353–363. [Google Scholar] [CrossRef]
- Oomizu, S.; Takeuchi, S.; Takahashi, S. Stimulatory effect of insulin-like growth factor I on proliferation of mouse pituitary cells in serum-free culture. J. Endocrinol. 1998, 157, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Krieger, C.C.; Perry, J.D.; Morgan, S.J.; Kahaly, G.J.; Gershengorn, M.C. TSH/IGF-1 Receptor Cross-Talk Rapidly Activates Extracellular Signal-Regulated Kinases in Multiple Cell Types. Endocrinology 2017, 158, 3676–3683. [Google Scholar] [CrossRef] [Green Version]
- Dickey, R.A.; Wartofsky, L.; Feld, S. Optimal thyrotropin level: Normal ranges and reference intervals are not equivalent. Thyroid 2005, 15, 1035–1039. [Google Scholar] [CrossRef]
- Wartofsky, L.; Dickey, R.A. The evidence for a narrower thyrotropin reference range is compelling. J. Clin. Endocrinol. Metab. 2005, 90, 5483–5488. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Control Subjects | Obese Subjects | p | |||
|---|---|---|---|---|---|
| Mean ± SE | Median (IR) | Mean ± SE | Median (IR) | ||
| Age (years) | 44.4 ± 1.7 | 42.0 (37.1–53.0) | 46.6 ± 0.8 | 45.8 (43.8–53.7) | 0.234 |
| Sex (n, %) | 0.695 | ||||
| Female | 21 | 67.7% | 92 | 71.3% | |
| Male | 10 | 32.3% | 37 | 28.7% | |
| BMI (Kg/m2) | 24.1 ± 0.7 | 23.6 (21.1–25.7) | 49.3 ± 0.7 | 47.8 (43.8–53.7) | <0.001 |
| Body fat (%) | 26.4 ± 1.5 | 24.6 (20.6–31.8) | 48.8 ± 0.6 | 50.1 (45.9–52.5) | <0.001 |
| Diabetes (%) | 0 | 0% | 51 | 39.5% | <0.001 |
| HTA (%) | 0 | 0% | 55 | 42.6% | <0.001 |
| Type of surgery (%) | |||||
| Roux-en-Y gastric bypass | 88 | 68.2% | |||
| Sleeve gastrectomy | 41 | 31.8% | |||
| Control Subjects | Obese Subjects | p | |||
|---|---|---|---|---|---|
| Mean ± SE | Median (IR) | Mean ± SE | Median (IR) | ||
| TSH (µU/mL) | 2.1 ± 0.2 | 2.0 (1.3–2.9) | 3.3 ± 0.2 | 2.5 (1.5–3.7) | 0.022 |
| Free T4 (ng/dL) | 1.1 ± 0.01 | 1.1 (1.1–1.2) | 1.47 ± 0.02 | 1.4 (1.3–1.7) | <0.001 |
| Fasting Glucose (mg/dL) | 89.5 ± 1.4 | 88.0 (85.0–94.0) | 105.7 ± 2.6 | 103.0 (85.0–122.5) | 0.002 |
| GH (µg/L) | 1.4 ± 0.3 | 0.5 (0.2–1.9) | 1.0 ± 0.2 | 0.3 (0.1–1.0) | 0.256 |
| IGF-I (µg/L) | 139.1 ± 7.9 | 131.0 (100.0–174.0) | 90.0 ± 4.2 | 83.0 (58.8–109.0) | <0.001 |
| Cortisol (µg/dL) | 16.5 ± 1.1 | 15.6 (12.8–19.3) | 20.1 ± 2.1 | 12.8 (8.7–20.45) | 0.1 |
| C-Reactive Protein (mg/dL) | 0.2 ± 0.1 | 0.05 (0.02–0.19) | 0.9 ± 0.1 | 0.7 (0.3–1.2) | <0.001 |
| Obese Patientsbefore Surgery | Obese Subjects 12 Monthsafter Surgery | Change | p | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SE | Median (IR) | Mean ± SE | Median (IR) | Mean ± SE | Median (IR) | ||
| BMI (Kg/m2) | 49.3 ± 0.7 | 47.8 (43.8–53.7) | 32.5 ± 0.7 | 31.1 (27.8–35.7) | 17.2 ± 0.6 | 16.2 (13.7; 20.5) | <0.001 |
| Weight (Kg) | 134.5 ± 2.2 | 126.0 (115.5–153.4) | 88.1 ± 2.1 | 87.7 (73.7–98.6) | 46.7 ± 1.7 | 42.6 (36.9; 57.0) | <0.001 |
| Body fat (%) | 48.8 ± 0.6 | 50.1 (45.9–52.5) | 31.9 ± 1.3 | 32.8 (23.9–39.3) | 18.2 ± 1.2 | 17.0 (11.7; 20.6) | <0.001 |
| EBMIL (%) | 72.7 ± 2.1 | 73.5 (58.5–83.7) | |||||
| TSH (µU/mL) | 3.3 ± 0.2 | 2.5 (1.5–3.7) | 2.1 ± 0.2 | 1.9 (1.2–2.8) | 1.2 ± 0.3 | 0.8 (−0.1; 1.7) | <0.001 |
| Free T4 (ng/dL) | 1.47 ± 0.02 | 1.4 (1.3–1.7) | 1.12 ± 0.02 | 1.1 (1.0–1.2) | 0.3 ± 0.0 | 0.3 (0.2; 0.6) | <0.001 |
| Fasting Glucose (mg/dL) | 105.7 ± 2.6 | 103.0 (85.0–122.5) | 90.2 ± 2.1 | 84.0 (77.0–93.0) | 16.7 ± 2.8 | 16 (0.0; 34.0) | <0.001 |
| GH (µg/L) | 1.0 ± 0.2 | 0.3 (0.1–1.0) | 3.4 ± 0.8 | 1.6 (0.3–5.0) | −2.1 ± 0.9 | −0.3 (−4.1; 0.5) | 0.014 |
| IGF-I (µg/L) | 90.0 ± 4.2 | 83.0 (58.8–109.0) | 115.2 ± 5.0 | 113.0 (90.2–125.0) | −28.5 ± 6.9 | −33.9 (−59.5; −8.0) | <0.001 |
| Cortisol (µg/dL) | 20.1 ± 2.1 | 12.8 (8.7–20.45) | 15.4 ± 1.1 | 15.2 (11.9–17.8) | 6.3 ± 4.9 | −2.6 (−9.6; 8.1) | 0.894 |
| C-Reactive Protein (mg/dL) | 0.9 ± 0.1 | 0.7 (0.3–1.2) | 0.2 ± 0.1 | 0.05 (0.01–0.13) | 0.4 ± 1.2 | 0.6 (0.1; 0.8) | 0.001 |
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | B | SE | |
| Main Effects | ||||||||||||||
| Linear time (months after surgery) | −0.034 | 0.009 *** | −0.033 | 0.009 *** | 0.067 | 0.084 | 0.001 | 0.014 | −0.021 | 0.036 | −0.019 | 0.036 | −0.019 | 0.038 |
| Preoperative values | ||||||||||||||
| BMI | 0.035 | 0.019 | 0.050 | 0.027 | 0.031 | 0.019 | 0.044 | 0.025 | 0.038 | 0.026 | 0.039 | 0.026 | ||
| Post-surgery values | ||||||||||||||
| EBMIL | −0.013 | 0.003 *** | −0.012 | 0.005 * | −0.012 | 0.005 * | −0.015 | 0.007 * | ||||||
| GH | −0.008 | 0.040 | 0.001 | 0.041 | 0.001 | 0.043 | ||||||||
| IGF-I | −0.004 | 0.003 | −0.004 | 0.003 | ||||||||||
| Free Thyroxine | −0.468 | 0.595 | ||||||||||||
| Interaction Effects | ||||||||||||||
| Time × BMI | −0.002 | 0.002 | ||||||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juiz-Valiña, P.; Outeiriño-Blanco, E.; Pértega, S.; Varela-Rodriguez, B.M.; García-Brao, M.J.; Mena, E.; Pena-Bello, L.; Cordido, M.; Sangiao-Alvarellos, S.; Cordido, F. Effect of Weight Loss after Bariatric Surgery on Thyroid-Stimulating Hormone Levels in Euthyroid Patients with Morbid Obesity. Nutrients 2019, 11, 1121. https://doi.org/10.3390/nu11051121
Juiz-Valiña P, Outeiriño-Blanco E, Pértega S, Varela-Rodriguez BM, García-Brao MJ, Mena E, Pena-Bello L, Cordido M, Sangiao-Alvarellos S, Cordido F. Effect of Weight Loss after Bariatric Surgery on Thyroid-Stimulating Hormone Levels in Euthyroid Patients with Morbid Obesity. Nutrients. 2019; 11(5):1121. https://doi.org/10.3390/nu11051121
Chicago/Turabian StyleJuiz-Valiña, Paula, Elena Outeiriño-Blanco, Sonia Pértega, Bárbara María Varela-Rodriguez, María Jesús García-Brao, Enrique Mena, Lara Pena-Bello, María Cordido, Susana Sangiao-Alvarellos, and Fernando Cordido. 2019. "Effect of Weight Loss after Bariatric Surgery on Thyroid-Stimulating Hormone Levels in Euthyroid Patients with Morbid Obesity" Nutrients 11, no. 5: 1121. https://doi.org/10.3390/nu11051121