A Review of A Priori Defined Oxidative Balance Scores Relative to Their Components and Impact on Health Outcomes

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
3. Results
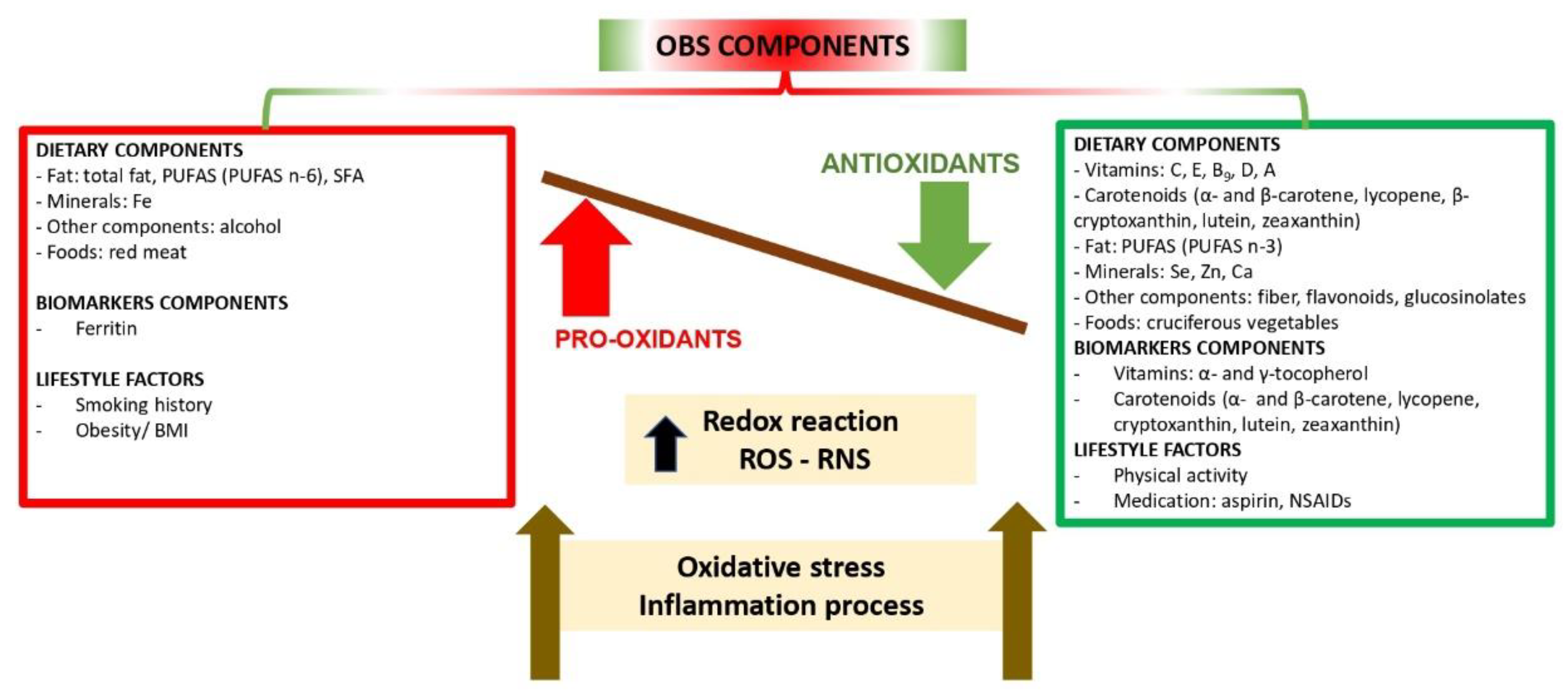
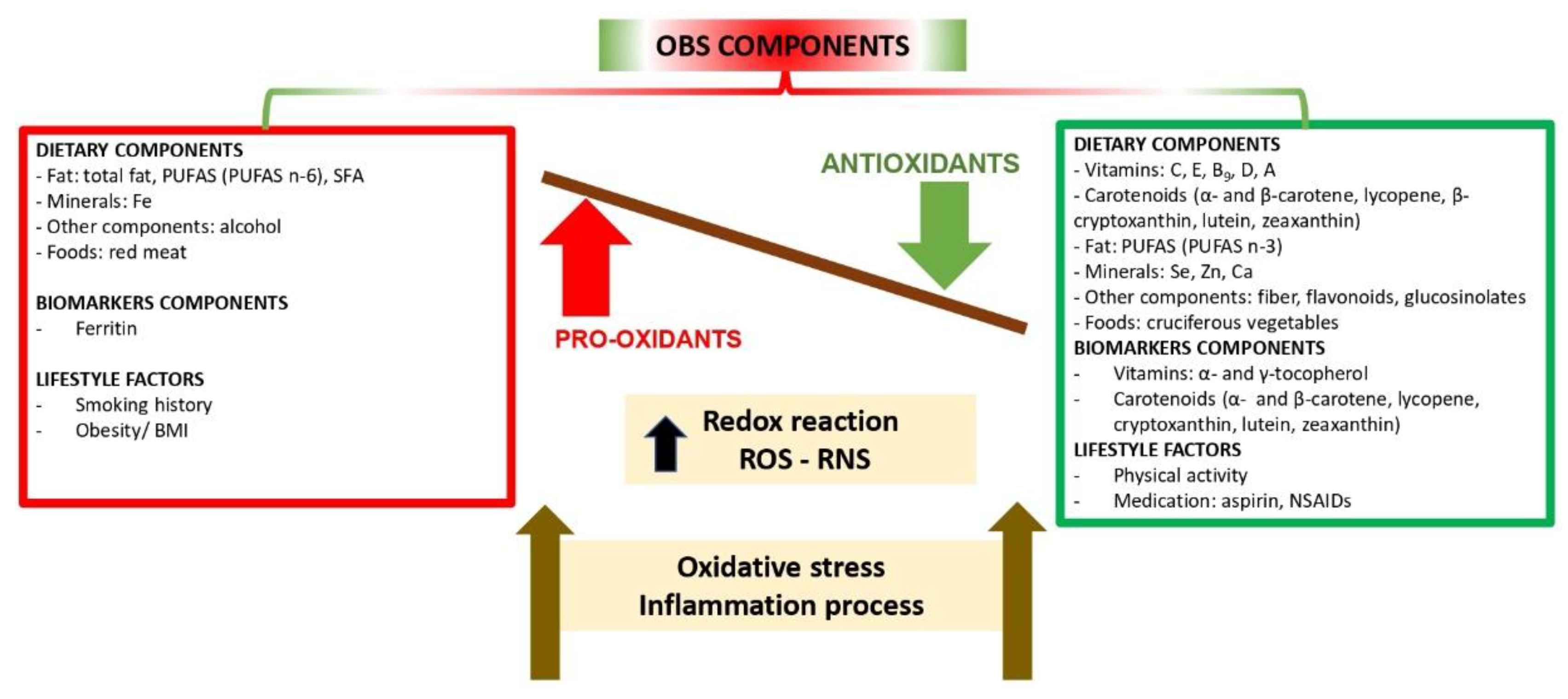
3.1. Components of the OBSs
3.2. Scoring Systems
3.3. Rationale for the Inclusion of Antioxidant and Pro-Oxidant Components in OBSs
3.4. OBSs and Their Association with Health Outcomes
3.4.1. OBS and Mortality Risk
3.4.2. OBSs and Colorectal Adenoma Risk
3.4.3. OBSs and Colorectal Cancer Risk
3.4.4. OBS and Breast Cancer Risk
3.4.5. OBSs and Prostate Cancer Risk
3.4.6. OBS and Cardiovascular Disease (CVD) Risk Factors
3.4.7. OBS and Oxidative Stress and Inflammation Biomarkers
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BER GRS | Base Excision Repair Genetic Scores |
| BIRNH study | Belgian Interuniversity Research on Nutrition and Health study |
| BMI | Body Mass Index |
| CAD | Coronary Artery Disease |
| CI | Confidence Interval |
| CKD | Chronic Kidney Disease |
| CPRU study | Cancer Prevention Research Unit study |
| CP study II Nutrition Cohort | Cancer Prevention Study II Nutrition Cohort |
| CRP | C-Reactive Protein |
| CSDLH cohort | Canadian Study of Diet, Lifestyle and Health cohort |
| CVD | Cardiovascular disease |
| DBP | Diastolic Blood Pressure |
| DNA | Deoxyribonucleic acid |
| ESRD | End-Stage Renal Disease |
| FFQ | Food Frequency Questionnaire |
| FIP | F2-isoprostanes |
| FOP | Fluorescent Oxidative Products |
| GCS | Glucosinolates |
| GGT | γ-glutamyltransferase |
| GRS | Genetic Risk Score |
| HDL-cholesterol | High-Density Lipoproteins-Cholesterol |
| HR | Hazard Ratio |
| KARE study | Korea Association Resource study |
| KNHANES-V | Korea National Health and Nutrition Examination survey study |
| KPMCP | Kaiser Permanente Care Program of Northern California |
| LDL-cholesterol | Low-Density Lipoproteins-Cholesterol |
| MAP study | Markers of Adenomatous Polyps study |
| MetS | Metabolic syndrome |
| MPC study | Markers of Prostate Cancer study |
| mtDNA | Mitochondrial DNA copy number |
| NOS2A | Nitric oxide synthase |
| NSAID | Non-steroidal anti-inflammatory drug |
| OBS | Oxidative Balance Score |
| OR | Odds Ratio |
| OS | Oxidative stress |
| OS biomarkers | Oxidative stress biomarkers |
| OSS | Oxidative Stress Score |
| PUFAS | Polyunsaturated fatty acids |
| SBP | Systolic blood pressure |
| SEER summary stage | Surveillance Epidemiology and End Results summary stage |
| SES | Socioeconomic status |
| SFA | Saturated Fatty Acids |
| SRSH | Study of Race, Stress, and Hypertension |
| REGARDs study | Reasons for Geographic and Racial Difference in stroke study |
| RNS | Reactive Nitrogen Species |
| ROS | Reactive Oxygen Species |
| RR | Relative Risk |
| US | United States |
| WBC count | Waist B circumference count |
References
- Rahman, I.; Biswas, S.K.; Kode, A. Oxidant and antioxidant balance in the airways and airway diseases. Eur. J. Pharmacol. 2006, 533, 222–239. [Google Scholar] [CrossRef]
- Jones, D.P. Radical-free biology of oxidative stress. AJP Cell-Physiol. 2008, 295, C849–C868. [Google Scholar] [CrossRef]
- Poljsak, B.; Šuput, D.; Milisav, I. Achieving the balance between ROS and antioxidants: When to use the synthetic antioxidants. Oxid. Med. Cell. Longev. 2013, 2013, 956792. [Google Scholar] [CrossRef] [PubMed]
- Simone Reuter, B.B.A. Oxidative stress, inflammation, and cancer: How are they linked? Free Radic. Biol. Med. 2011, 49, 1603–1616. [Google Scholar] [CrossRef]
- Kryston, T.B.; Georgiev, A.B.; Pissis, P.; Georgakilas, A.G. Role of oxidative stress and DNA damage in human carcinogenesis. Mutat. Res.-Fundam. Mol. Mech. Mutagen. 2011, 711, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Nagel, G.; Linseisen, J.; Van Gils, C.H.; Peeters, P.H.; Boutron-Ruault, M.C.; Clavel-Chapelon, F.; Romieu, I.; Tjønneland, A.; Olsen, A.; Roswall, N.; et al. Dietary β-carotene, vitamin C and e intake and breast cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC). Breast Cancer Res. Treat. 2010, 119, 753–765. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Yang, K.; Tian, J.; Guan, Q.; Yao, N.; Cao, N.; Mi, D.; Wu, J.; Ma, B.; Yang, S. Efficacy of Antioxidant Vitamins and Selenium Supplement in Prostate Cancer Prevention: A Meta-Analysis of Randomized Controlled Trials. Nutr. Cancer 2010, 62, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.D.; Mazur, M.; Telser, J. Free radicals and antioxidants in normal physiological functions and human disease. Int. J. Biochem. Cell. Biol. 2007, 39, 44–84. [Google Scholar] [CrossRef] [PubMed]
- Van Hoydonck, P.G.; Temme, E.H.M.; Schouten, E.G. A dietary oxidative balance score of vitamin C, beta-carotene and iron intakes and mortality risk in male smoking Belgians. J. Nutr. 2002, 132, 756–761. [Google Scholar] [CrossRef] [PubMed]
- Goodman, M.; Bostick, R.M.; Dash, C.; Flanders, W.D.; Mandel, J.S. Hypothesis: Oxidative Stress Score as a Combined Measure of Pro-oxidant and Antioxidant Exposures. Ann. Epidemiol. 2007, 17, 394–399. [Google Scholar] [CrossRef]
- Kong, S.Y.J.; Bostick, R.M.; Flanders, W.D.; McClellan, W.M.; Thyagarajan, B.; Gross, M.D.; Judd, S.; Goodman, M. Oxidative balance score, colorectal adenoma, and markers of oxidative stress and inflammation. Cancer Epidemiol. Biomark. Prev. 2014, 23, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Lakkur, S.; Goodman, M.; Bostick, R.M.; Citronberg, J.; McClellan, W.; Flanders, W.D.; Judd, S.; Stevens, V.L. Oxidative balance score and risk for incident prostate cancer in a prospective U.S. cohort study. Ann. Epidemiol. 2014, 24, 475–478. [Google Scholar] [CrossRef] [PubMed]
- Dash, C.; Goodman, M.; Flanders, W.D.; Mink, P.J.; McCullough, M.L.; Bostick, R.M. Using pathway-specific comprehensive exposure scores in epidemiology: Application to oxidative balance in a pooled case-control study of incident, sporadic colorectal adenomas. Am. J. Epidemiol. 2013, 178, 610–624. [Google Scholar] [CrossRef]
- Wright, M.E.; Mayne, S.T.; Stolzenberg-Solomon, R.Z.; Li, Z.; Pietinen, P.; Taylor, P.R.; Virtamo, J.; Albanes, D. Development of a comprehensive dietary antioxidant index and application to lung cancer risk in a cohort of male smokers. Am. J. Epidemiol. 2004, 160, 68–76. [Google Scholar] [CrossRef]
- Goodman, M.; Bostick, R.M.; Dash, C.; Terry, P.; Flanders, W.D.; Mandel, J. A summary measure of pro- and anti-oxidant exposures and risk of incident, sporadic, colorectal adenomas. Cancer Causes Control 2008, 19, 1051–1064. [Google Scholar] [CrossRef]
- Agalliu, I.; Kirsh, V.A.; Kreiger, N.; Soskolne, C.L.; Rohan, T.E. Oxidative balance score and risk of prostate cancer: Results from a case-cohort study. Cancer Epidemiol. 2011, 35, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Geybels, M.S.; Verhage, B.A.J.; Van Schooten, F.J.; Van den Brandt, P.A. Measures of combined antioxidant and pro-oxidant exposures and risk of overall and advanced stage prostate cancer. Ann. Epidemiol. 2012, 22, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Goodman, M.; Bostick, R.M.; Gross, M.; Thyagarajan, B.; Dash, C.; Flanders, W.D. Combined measure of pro- and anti-oxidant exposures in relation to prostate cancer and colorectal adenoma risk: An update. Ann. Epidemiol. 2010, 20, 955–957. [Google Scholar] [CrossRef] [PubMed]
- Slattery, M.L.; Lundgreen, A.; Welbourn, B.; Wolff, R.K.; Corcoran, C. Oxidative balance and colon and rectal cancer: Interaction of lifestyle factors and genes. Mutat. Res.-Fundam. Mol. Mech. Mutagen. 2012, 734, 30–40. [Google Scholar] [CrossRef]
- Labadie, J.; Goodman, M.; Thyagarajan, B.; Gross, M.; Sun, Y.; Fedirko, V.; Bostick, R.M. Associations of oxidative balance-related exposures with incident, sporadic colorectal adenoma according to antioxidant enzyme genotypes. Ann. Epidemiol. 2013, 23, 223–226. [Google Scholar] [CrossRef]
- Slattery, M.L.; John, E.M.; Torres-Mejia, G.; Lundgreen, A.; Lewinger, J.P.; Stern, M.C.; Hines, L.; Baumgartner, K.B.; Giuliano, A.R.; Wolff, R.K. Angiogenesis genes, dietary oxidative balance and breast cancer risk and progression: The breast cancer health disparities study. Int. J. Cancer 2013, 134, 629–644. [Google Scholar] [CrossRef]
- Lakkur, S.; Bostick, R.M.; Roblin, D.; Ndirangu, M.; Okosun, I.; Annor, F.; Judd, S.; Flanders, W.D.; Stevens, V.L.; Goodman, M. Oxidative balance score and oxidative stress biomarkers in a study of Whites, African Americans, and African immigrants. Biomarkers 2014, 19, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Dash, C.; Bostick, R.M.; Goodman, M.; Flanders, W.D.; Patel, R.; Shah, R.; Campbell, P.T.; McCullough, M.L. Oxidative balance scores and risk of incident colorectal cancer in a US prospective cohort study. Am. J. Epidemiol. 2015, 181, 584–594. [Google Scholar] [CrossRef] [PubMed]
- Kong, S.Y.; Goodman, M.; Judd, S.M.; Bostick, R.; Flanders, W.D.; Mcclellan, W. Oxidative Balance Score as Predictor of All-Cause, Cancer, and Non-cancer Mortality in a Biracial US Cohort. Ann. Epidemiol. 2015, 25, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Annor, F.B.; Goodman, M.; Okosun, I.S.; Wilmot, D.W.; Il’yasova, D.; Ndirangu, M.; Lakkur, S. Oxidative stress, oxidative balance score, and hypertension among a racially diverse population. J. Am. Soc. Hypertens. 2017, 9, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Lakkur, S.; Judd, S.; Bostick, R.M.; McClellan, W.; Flanders, W.D.; Stevens, V.L.; Goodman, M. Oxidative stress, inflammation, and markers of cardiovascular health. Atherosclerosis 2015, 243, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Ilori, T.O.; Sun Ro, Y.; Kong, S.Y.; Gutierrez, O.M.; Ojo, A.O.; Judd, S.E.; Narayan, K.M.V.; Goodman, M.; Plantinga, L.; McClellan, W. Oxidative Balance Score and Chronic Kidney Disease. Am. J. Nephrol. 2015, 42, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Goodman, M.; Sun, Y.V.; Thyagarajan, B.; Gross, M.; Bostick, R.M. DNA base excision repair genetic risk scores, oxidative balance, and incident, sporadic colorectal adenoma. Mol. Carcinog. 2017, 56, 1642–1652. [Google Scholar] [CrossRef] [PubMed]
- Cho, A.R.; Kwon, Y.J.; Lim, H.J.; Lee, H.S.; Kim, S.; Shim, J.Y.; Lee, H.R.; Lee, Y.J. Oxidative balance score and serum γ-glutamyltransferase level among Korean adults: A nationwide population-based study. Eur. J. Nutr. 2018, 57, 1237–1244. [Google Scholar] [CrossRef]
- Lee, H.; Park, T. Pathway-Driven Approaches of Interaction between Oxidative Balance and Genetic Polymorphism on Metabolic Syndrome. Oxid. Med. Cell. Longev. 2017, 2017, 6873197. [Google Scholar] [CrossRef] [PubMed]
- Arrigoni, O.; De Tullio, M.C. Ascorbic acid: Much more than just an antioxidant. Biochim. Biophys. Acta-Gen. Subj. 2002, 1569, 1–9. [Google Scholar] [CrossRef]
- Kojo, S. Vitamin C: Basic Metabolism and Its Function as an Index of Oxidative Stress. Curr. Med. Chem. 2004, 11, 1041–1064. [Google Scholar] [CrossRef]
- Mortensen, A.; Skibsted, L.H.; Truscott, T.G. The Interaction of Dietary Carotenoids with Radical Species. Arch. Biochem. Biophys. 2001, 385, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Stahl, W.; Sies, H. Antioxidant activity of carotenoids. Mol. Asp. Med. 2003, 24, 345–351. [Google Scholar] [CrossRef]
- Rao, A.V.; Rao, L.G. Carotenoids and human health. Pharmacol. Res. 2007, 55, 207–216. [Google Scholar] [CrossRef]
- Edge, R.; Gaikwad, P.; Navaratnam, S.; Rao, B.S.M.; George Truscott, T. Reduction of oxidized guanosine by dietary carotenoids: A pulse radiolysis study. Arch. Biochem. Biophys. 2010, 504, 100–103. [Google Scholar] [CrossRef]
- Di Mascio, P.; Kaiser, S.; Sies, H. Lycopene as the most efficient biological carotenoid singlet oxygen quencher. Arch. Biochem. Biophys. 1989, 274, 532–538. [Google Scholar] [CrossRef]
- Heber, D.; Lu, Q.-Y. Overview of mechanisms of action of lycopene. Exp. Biol. Med. 2002, 227, 920–923. [Google Scholar] [CrossRef]
- Palozza, P.; Krinsky, N.I. Antioxidant effects of carotenoids in vivo and in vitro: An overview. Methods Enzymol. 1992, 213, 403–420. [Google Scholar]
- Manach, C.; Donovan, J.L. Pharmacokinetics and metabolism of dietary flavonoids in humans. Free Radic. Res. 2004, 38, 771–785. [Google Scholar] [CrossRef] [PubMed]
- Fraga, C.G. Plant polyphenols: How to translate their in vitro antioxidant actions to in vivo conditions. IUBMB Life 2007, 59, 308–315. [Google Scholar] [CrossRef]
- Pietta, P.G. Flavonoids as antioxidants. J. Nat. Prod. 2000, 63, 1035–1042. [Google Scholar] [CrossRef]
- Fahey, J.W.; Zalcmann, A.T.; Talalay, P. The chemical diversity and distribution of glucosinolates and isothiocyanates among plants. Phytochemistry 2001, 56, 5–51. [Google Scholar] [CrossRef]
- Juge, N.; Mithen, R.F.; Traka, M. Molecular basis for chemoprevention by sulforaphane: A comprehensive review. Cell. Mol. Life Sci. 2007, 64, 1105–1127. [Google Scholar] [CrossRef] [PubMed]
- Dinkova-Kostova, A.T.; Kostov, R. V Glucosinolates and isothiocyanates in health and disease. Trends Mol. Med. 2012, 18, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P.; Blundell-Pound, G.; Pastor-Barriuso, R.; Guallar, E.; Steinbrenner, H.; Stranges, S. A randomized trial of selenium supplementation and risk of type-2 diabetes, as assessed by plasma adiponectin. PLoS ONE 2012, 7, e45269. [Google Scholar] [CrossRef] [PubMed]
- Powis, G.; Mustacich, D.; Coon, A. The role of the redox protein thioredoxin in cell growth and cancer. Free Radic. Biol. Med. 2000, 29, 312–322. [Google Scholar] [CrossRef]
- Marreiro, D.; Cruz, K.; Morais, J.; Beserra, J.; Severo, J.; de Oliveira, A. Zinc and Oxidative Stress: Current Mechanisms. Antioxidants 2017, 6, 24. [Google Scholar] [CrossRef]
- Joshi, R.; Adhikari, S.; Patro, B.S.; Chattopadhyay, S.; Mukherjee, T. Free radical scavenging behavior of folic acid: Evidence for possible antioxidant activity. Free Radic. Biol. Med. 2001, 30, 1390–1399. [Google Scholar] [CrossRef]
- Chang, C.-M.; Yu, C.-C.; Lu, H.-T.; Chou, Y.-F.; Huang, R.-F.S. Folate deprivation promotes mitochondrial oxidative decay: DNA large deletions, cytochrome c oxidase dysfunction, membrane depolarization and superoxide overproduction in rat liver. Br. J. Nutr. 2007, 97, 855. [Google Scholar] [CrossRef]
- Moens, J.; Jaque, P.; De Proft, F.; Geerlings, P. The study of redox reactions on the basis of conceptual DFT principles: EEM and vertical quantities. J. Phys. Chem. 2008, 112, 6023–6031. [Google Scholar] [CrossRef]
- Berridge, M.J. Vitamin D cell signalling in health and disease. Biochem. Biophys. Res. Commun. 2015, 460, 53–71. [Google Scholar] [CrossRef]
- Zeng, L.; Wu, G.Z.; Goh, K.J.; Lee, Y.M.; Ng, C.C.; You, A.B.; Wang, J.; Jia, D.; Hao, A.; Yu, Q.; et al. Saturated Fatty Acids Modulate Cell Response to DNA Damage: Implication for Their Role in Tumorigenesis. PLoS ONE 2008, 3, e2329. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Tsuboyama-Kasaoka, N.; Nakatani, T.; Ishii, M.; Tsutsumi, S.; Aburatani, H.; Ezaki, O. Fish oil feeding alters liver gene expressions to defend against PPARalpha activation and ROS production. Am. J. Physiol. Gastrointest. Liver Physiol. 2002, 282, G338–G348. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. n-3 Polyunsaturated fatty acids, inflammation, and inflammatory. Am. J. Clin. Nutr. 2006, 83, 1505S–1519S. [Google Scholar] [CrossRef] [PubMed]
- Wiest, E.F.; Walsh-Wilcox, M.T.; Walker, M.K. Omega-3 Polyunsaturated Fatty Acids Protect Against Cigarette Smoke-Induced Oxidative Stress and Vascular Dysfunction. Toxicol. Sci. 2017, 156, 300–310. [Google Scholar] [CrossRef]
- Ghosh, S.; Kewalramani, G.; Yuen, G.; Pulinilkunnil, T.; An, D.; Innis, S.M.; Allard, M.F.; Wambolt, R.B.; Qi, D.; Abrahani, A.; et al. Induction of mitochondrial nitrative damage and cardiac dysfunction by chronic provision of dietary ω-6 polyunsaturated fatty acids. Free Radic. Biol. Med. 2006, 41, 1413–1424. [Google Scholar] [CrossRef]
- Ayala, A.; Munoz, M.F.; Arguelles, S. Lipid peroxidation: Production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxid. Med. Cell. Longev. 2014, 2014, 360438. [Google Scholar] [CrossRef]
- Puntarulo, S. Iron, oxidative stress and human health. Mol. Asp. Med. 2005, 26, 299–312. [Google Scholar] [CrossRef]
- Vinchi, F.; Muckenthaler, M.U.; Da Silva, M.C.; Balla, G.; Balla, J.; Jeney, V. Atherogenesis and iron: From epidemiology to cellular level. Front. Pharmacol. 2014, 94, 1–20. [Google Scholar] [CrossRef]
- Glei, M.; Latunde-Dada, G.O.; Klinder, A.; Becker, T.W.; Hermann, U.; Voigt, K.; Pool-Zobel, B.L. Iron-overload induces oxidative DNA damage in the human colon carcinoma cell line HT29 clone 19A. Mutat. Res. Toxicol. Environ. Mutagen. 2002, 519, 151–161. [Google Scholar] [CrossRef]
- Swain, J.H.; Alekel, D.L.; Dent, S.B.; Peterson, C.T.; Reddy, M.B. Iron indexes and total antioxidant status in response to soy protein intake in perimenopausal women. Am. J. Clin. Nutr. 2002, 1, 165–171. [Google Scholar] [CrossRef]
- De Sousa, C.V.; Sales, M.M.; Rosa, T.S.; Lewis, J.E.; de Andrade, R.V.; Simoes, H.G. The Antioxidant Effect of Exercise: A Systematic Review and Meta-Analysis. Sports Med. 2017, 47, 277–293. [Google Scholar] [CrossRef]
- Ji, L.L.; Gomez-Cabrera, M.C.; Vina, J. Exercise and hormesis: Activation of cellular antioxidant signaling pathway. Ann. N. Y. Acad. Sci. 2006, 1067, 425–435. [Google Scholar] [CrossRef]
- Albano, E. Alcohol, oxidative stress and free radical damage. Proc. Nutr. Soc. 2006, 65, 278–290. [Google Scholar] [CrossRef]
- Alberg, A.J. The influence of cigarette smoking on circulating concentrations of antioxidant micronutrients. Toxicology 2002, 180, 121–137. [Google Scholar] [CrossRef]
- Van der Vaart, H. Acute effects of cigarette smoke on inflammation and oxidative stress: A review. Thorax 2004, 59, 713–721. [Google Scholar] [CrossRef]
- Chow, C.K. Cigarette Smoking and Oxidative Damage in the Lung. Ann. N. Y. Acad. Sci. 1993, 686, 289–298. [Google Scholar] [CrossRef]
- Barreiro, E.; Peinado, V.I.; Galdiz, J.B.; Ferrer, E.; Marin-Corral, J.; Sánchez, F.; Gea, J.; Barberà, J.A. Cigarette smoke-induced oxidative stress: A role in chronic obstructive pulmonary disease skeletal muscle dysfunction. Am. J. Respir. Crit. Care Med. 2010, 182, 477–488. [Google Scholar] [CrossRef]
- Pryor, W.A. Cigarette smoke radicals and the role of free radicals in chemical carcinogenicity. Environ. Health Perspect. 1997, 105, 875–882. [Google Scholar]
- Le Lay, S.; Simard, G.; Martinez, M.C.; Andriantsitohaina, R. Oxidative stress and metabolic pathologies: From an adipocentric point of view. Oxid. Med. Cell. Longev. 2014, 2014, 908539. [Google Scholar] [CrossRef]
- Chen, B.; Zhao, J.; Zhang, S.; Wu, W.; Qi, R. Aspirin Inhibits the Production of Reactive Oxygen Species by Downregulating Nox4 and Inducible Nitric Oxide Synthase in Human Endothelial Cells Exposed to Oxidized Low-density Lipoprotein. J. Cardiovasc. Pharmacol. 2012, 59, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Ely, L.S.; Valle Gottlieb, M.G.; Engroff, P.; Gomes, I.; Moresco, R.N.; Tatsch, E.; Bochi, G.V.; Morrone, F.B.; De Carli, G.A. The association between the chronic use of non-steroidal anti- inflammatory drugs and oxidative and inflammatory markers in the elderly. Inflamm. Allergy Drug Targets 2014, 13, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Kono, Y.; Kawano, S.; Takaki, A.; Shimomura, Y.; Onji, M.; Ishikawa, H.; Takahashi, S.; Horii, J.; Kobayashi, S.; Kawai, D.; et al. Oxidative stress controlling agents are effective for small intestinal injuries induced by non-steroidal anti-inflammatory drugs. J. Gastroenterol. Hepatol. 2017, 32, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Santilli, F.; Lapenna, D.; La Barba, S.; Davi, G. Oxidative stress-related mechanisms affecting response to aspirin in diabetes mellitus. Free Radic. Biol. Med. 2015, 80, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, R.; Alajbegovic, A.; Gomes, A.V. NSAIDs and Cardiovascular Diseases: Role of Reactive Oxygen Species. Oxid. Med. Cell. Longev. 2015, 2015, 536962. [Google Scholar] [CrossRef]
- Van Beelen, V.A.; Aarts, J.M.M.J.G.; Reus, A.; Mooibroek, H.; Sijtsma, L.; Bosch, D.; Rietjens, I.M.C.M.; Alink, G.M. Differential induction of electrophile-responsive element-regulated genes by n-3 and n-6 polyunsaturated fatty acids. FEBS Lett. 2006, 580, 4587–4590. [Google Scholar] [CrossRef]
- Das, S.K.; Vasudevan, D.M. Alcohol-induced oxidative stress. Life Sci. 2007, 81, 177–187. [Google Scholar] [CrossRef]
- Wu, D.; Zhai, Q.; Shi, X. Alcohol-induced oxidative stress and cell responses. J. Gastroenterol. Hepatol. 2006, 21 (Suppl. 3), S26–S29. [Google Scholar] [CrossRef]
- Willett, W.C.; Stampfer, M.J. Total energy intake: Implications for epidemiologic analyses. Am. J. Epidemiol. 1986, 124, 17–27. [Google Scholar] [CrossRef]
- Carrión-García, C.J.; Guerra-Hernández, E.J.; García-Villanova, B.; Molina-Montes, E. Non-enzymatic antioxidant capacity (NEAC) estimated by two different dietary assessment methods and its relationship with NEAC plasma levels. Eur. J. Nutr. 2017, 56, 1561–1576. [Google Scholar] [CrossRef] [PubMed]
- Bjelakovic, G.; Nikolova, D.; Gluud, C. Antioxidant supplements and mortality. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Bjørklund, G.; Chirumbolo, S. Role of oxidative stress and antioxidants in daily nutrition and human health. Nutrition 2017, 33, 311–321. [Google Scholar] [CrossRef]
- Kristal, A.R.; Peters, U.; Potter, J.D. Is it time to abandon the food frequency questionnaire? Cancer Epidemiol. Biomarkers Prev. 2005, 14, 2826–2828. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author (s), Year | N Components | OBSs Components | Type of Components | Scoring per Component | Score Range |
|---|---|---|---|---|---|
| Van Hoydonck et al., 2002 [9] | 3 | 2 Antioxidant/ 1 Pro-oxidant | Dietary | 1–3 | 3–9 |
| Goodman et al., 2007 [10] | 12 | 9 Antioxidant/ 3 Pro-oxidant | Dietary, biomarkers, lifestyle and medication | 0–1 | 0–12 |
| Goodman et al., 2008 [15] | 12 | 8 Antioxidant/ 5 Pro-oxidant | Dietary, lifestyle and medication | 0–2 | 0–24 |
| Goodman et al., 2010 [18] | 14 | 11 Antioxidant/ 3 Pro-oxidant | Dietary, biomarkers, lifestyle and medication | 0–2 | 0–28 |
| Agalliu et al., 2011 [16] | 13 | 8 Antioxidant/ 5 Pro-oxidant | Dietary and lifestyle | 0–4 | 0–52 |
| Slattery et al., 2012 [19] | 13 | 10 Antioxidant/ 3 Pro-oxidant | Dietary, lifestyle and medication | 0–2 | 0–26 |
| Geybels et al., 2012 [17] | 8 | 5 Antioxidant/ 3 Pro-oxidant | Dietary and lifestyle | 0–3 | 0–24 |
| Dash et al., 2013 [13] | 15 | 9 Antioxidant/ 6 Pro-oxidant | Dietary and lifestyle | −1–1 | −6–9 |
| Labadie et al., 2013 [20] | 11 | 7 Antioxidant/ 4 Pro-oxidant | Dietary, lifestyle and medication | 0–2 | 0–22 |
| Kong et al., 2014 [11] | 14 | 10 Antioxidant/ 4 Pro-oxidant | Dietary, biomarkers, lifestyle and medication | 0–2 | 0–28 |
| Slattery et al., 2014 [21] | 6 | 5 Antioxidant/ 1 Pro-oxidant | Dietary | 0–2 | 0–12 |
| Lakkur et al., 2014a [12] | 20 | 14 Antioxidant/ 6 Pro-oxidant | Dietary, lifestyle and medication | 0–3 | 0–60 |
| Lakkur et al., 2014b [22] | 13 | 10 Antioxidant/ 3 Pro-oxidant | Dietary, biomarkers, lifestyle and medication | 0–2 | 0–26 |
| Dash et al., 2015 [23] | 16 | 10 Antioxidant/ 6 Pro-oxidant | Dietary and lifestyle | −1–1 | −6–10 |
| Kong et al., 2015 [24] | 14 | 10 Antioxidant/ 4 Pro-oxidant | Dietary, lifestyle and medication | 0–2 | 0–28 |
| Annor et al., 2015 [25] | 13 | 9 Antioxidant/ 4 Pro-oxidant | Dietary, biomarkers, lifestyle and medication | 0–2 | 0–26 |
| Lakkur et al., 2015 [26] | 14 | 10 Antioxidant/ 4 Pro-oxidant | Dietary, lifestyle and medication | 0–2 | 0-–28 |
| Ilori et al., 2015 [27] | 13 | 10 Antioxidant/ 3 Pro-oxidant | Dietary and medication | 0–2 | 0–26 |
| Wang et al., 2017 [28] | 15 | 9 Antioxidant/ 6 Pro-oxidant | Dietary and lifestyle | 0–2 | 0–30 |
| Cho et al., 2017 [29] | 8 | 3 Antioxidant/ 5 Pro-oxidant | Dietary and lifestyle | 0–3 | 0–24 |
| Lee et al., 2017 [30] | 7 | 4 Antioxidant/ 3 Pro-oxidant | Dietary and lifestyle | 0–2 | 0–14 |
| Author (s), Year | Lifestyle Factors Components | Medication Components | |||
|---|---|---|---|---|---|
| Antioxidant | Pro-Oxidant | Antioxidant | |||
| Physical Activity | Smoking History | BMI | Aspirin | Other NSAID | |
| Van Hoydonck et al., 2002 [9] | |||||
| Goodman et al., 2007 [10] | X | X | X | ||
| Goodman et al., 2008 [15] | X | X | X | ||
| Goodman et al., 2010 [18] | X | X | X | ||
| Agalliu et al., 2011 [16] | X | ||||
| Slattery et al., 2012 [19] | X | X | |||
| Geybels et al., 2012 [17] | X | ||||
| Dash et al., 2013 [13] | X | X | X | ||
| Labadie et al., 2013 [20] | X | X | X | ||
| Kong et al., 2014 [11] | X | X | X | ||
| Slattery et al., 2014 [21] | |||||
| Lakkur et al., 2014a [12] | X | X | X | X | |
| Lakkur et al., 2014b [22] | X | X | X | X | |
| Dash et al., 2015 [23] | X | X | X | ||
| Kong et al., 2015 [24] | X | X | X | ||
| Annor et al., 2015 [25] | X | X | X | X | X |
| Lakkur et al., 2015 [26] | X | X | X | ||
| Ilori et al., 2015 [27] | X | X | |||
| Wang et al., 2017 [28] | X | X | X a | ||
| Cho et al., 2017 [29] | X | X | X | ||
| Lee et al., 2017 [30] | X | X | |||
| Author (s), Year | Dietary Antioxidants a | Dietary Pro-Oxidants a | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C | B9 | β-car | Lyco | β-cryp | Lute/Zeaxan | Retinol | D | E | Se | Zn | Ca | Fiber | Flav | GCS | Catechin | Fat | PUFAS | SFA | Fe | Alcohol | |
| Van Hoydonck et al., 2002 [9] | X | X | X | ||||||||||||||||||
| Goodman et al., 2007 [10] | X | X b | X | X | X c | X d | X e | X | X f | ||||||||||||
| Goodman et al., 2008 [15] | X f | X f,g | X | X | X f | X e | X | X f | X | ||||||||||||
| Goodman et al., 2010 [18] | X | X e | X | ||||||||||||||||||
| Agalliu et al., 2011 [16] | X f | X f | X | X | X c | X f | X e | X | X f | X | |||||||||||
| Slattery et al., 2012 [19] | X | X | X | X | X | X | X | X | X | X | X | ||||||||||
| Geybels et al., 2012 [17] | X | X | X | X | X | X n | X | ||||||||||||||
| Dash et al., 2013 f [13] | X | X g | X | X | X | X | X | X | X h | X | X | X | |||||||||
| Labadie et al., 2013 [20] | X f | X f,i | X f | X f | X f | X | X | X | |||||||||||||
| Kong et al., 2014 [11] | X f | X e | X | X | |||||||||||||||||
| Slattery et al., 2014 [21] | X | X | X | X | X | X | |||||||||||||||
| Lakkur et al., 2014a [12] | X f | X j | X | X | X | X f | X f | X | X | X | X | X | X f | X | |||||||
| Lakkur et al., 2014b [22] | X | ||||||||||||||||||||
| Dash et al., 2015 f [23] | X | X g | X | X | X | X | X e | X | X | X h | X | X | X | ||||||||
| Kong et al., 2015 [24] | X f | X f,j | X f | x f | X f | X f,k | X | X | X f | X | |||||||||||
| Annor et al., 2015 [25] | X | ||||||||||||||||||||
| Lakkur et al., 2015 f [26] | X f | X j | X | X | X | X f | X f | X | X | X | |||||||||||
| Ilori et al., 2015 [27] | X f | X j | X | X l | X | X f | X e | X | X f | X | |||||||||||
| Wang et al., 2017 f [28] | X f | X g | X | X m | X f | X | X | X h | X | X f | X | ||||||||||
| Cho et al., 2017 [29] | X | X | X | X | X | ||||||||||||||||
| Lee et al., 2017 [30] | X | X g | X | X | X | ||||||||||||||||
| Author (s), Year | Biomarker Components a | Food Components | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Antioxidant | Pro-Oxidant | Antioxidant | Pro-Oxidant | ||||||||
| α-carotene | β-carotene | Lycopene | Cryptoxanthin | Zeaxanthin | Lutein | α-tocopherol | γ-tocopherol | Ferritin | Crucifers | Red Meat | |
| Van Hoydonck et al., 2002 [9] | |||||||||||
| Goodman et al., 2007 [10] | X b | X c | |||||||||
| Goodman et al., 2008 [15] | |||||||||||
| Goodman et al., 2010 [18] | X | X | X | X d | X e | X | X | X | X f | ||
| Agalliu et al., 2011 [16] | X | X | |||||||||
| Slattery et al., 2012 [19] | |||||||||||
| Geybels et al., 2012 [17] | |||||||||||
| Dash et al., 2013 [13] | |||||||||||
| Labadie et al., 2013 [20] | |||||||||||
| Kong et al., 2014 [11] | X | X | X | X d | X | X | X | ||||
| Slattery et al., 2014 [21] | |||||||||||
| Lakkur et al., 2014a [12] | |||||||||||
| Lakkur et al., 2014b [22] | X | X | X | X | X | X | X | X | |||
| Dash et al., 2015 [23] | |||||||||||
| Kong et al., 2015 [24] | |||||||||||
| Annor et al., 2015 [25] | X | X | X | X | X | X | X | ||||
| Lakkur et al., 2015 [26] | |||||||||||
| Ilori et al., 2015 [27] | |||||||||||
| Wang et al., 2017 [28] | |||||||||||
| Cho et al., 2017 [29] | |||||||||||
| Lee et al., 2017 [30] | |||||||||||
| Author (s), Year | Cut-off Values | Scoring System for Each Component | Overall Score | Energy Adjustment and Other Methodological Issues | |
|---|---|---|---|---|---|
| Van Hoydonck et al., 2002 [9] | Population-dependent | 3 population-dependent dietary components (based on tertiles of intake). | The intakes were scored from 1 to 3 for pro-oxidant factors and from 3 to 1 for antioxidant factors. High score group (a diet poor in antioxidant and rich in iron). | The overall score ranged between 3 and 9 points. The score was divided into three groups: low (score 3–5), intermediate (score 6) and highest group (score 7–9). | Questionnaire-based (24-h recall) dietary components were considered. Energy adjustment was not considered. |
| Goodman et al., 2007 [10] | Predefined and population-dependent | 8 population-dependent dietary/biomarker components (based on median intakes); four predefined components for smoking (never, ever), Se supplements (yes, no), and medication (NSAID or aspirin use, non-use). | All dietary/biomarker components were divided into dichotomous categories based on the median value. For antioxidants, one point was awarded for high-level exposure and 0 for low-level exposure. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (e.g., non-smokers, and NSAID users), and fewer points to pro-oxidant categories. | The overall score ranged between 0 and 24 points. The score was divided into three groups: low (score ≤2), intermediate (score 3–6) and highest antioxidant group (score ≥7). | Questionnaire and biomarker-based dietary components were considered. Energy adjustment was not considered. |
| Goodman et al., 2008 [15] | Predefined and population-dependent | 7 population-dependent dietary components (based on sex-specific tertiles); five predefined components for smoking (never, former, current), Se supplements (yes, no), alcohol intake (low, moderate, heavy), and medication (NSAID or aspirin use, non-use). | All dietary components were divided into three categories based on the tertile values. For antioxidants, two points were awarded for high-level exposure, one point for intermediate, and 0 for low-level exposure. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (e.g., non-smokers and NSAID users), and conversely; fewer points to pro-oxidant categories. | The overall score ranged between 0 and 24 points. The OBSs was considered an ordinal variable. | Questionnaire-based (FFQ) dietary components were considered. Dietary components were adjusted for total energy intake. |
| Goodman et al., 2010 [18] | Predefined and population-dependent | 10 population-dependent dietary/biomarker components (based on tertiles) and four predefined components for smoking (never, former, current), Se supplements (yes, no), and medication (NSAID or aspirin use, non-use). | All dietary/biomarker components divided into three categories based on the tertile values. For antioxidants, two points were awarded for high-level exposure, one point for intermediate, and 0 for low-level exposure. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (e.g., non-smokers, and NSAID users), and fewer points to pro-oxidant categories. | The overall score ranged between 0 and 24 points. The score was divided into three equal intervals: low (score 1–7), intermediate score (8–14), and highest antioxidant group (score 15–22). | Questionnaire and biomarker-based dietary components were considered. Energy adjustment was not considered. |
| Agalliu et al., 2011 [16] | Population-dependent | 11 population-dependent dietary components (based on quintiles) and two population-dependent lifestyle components for smoking in pack-years and alcohol intake (in quartiles). | All dietary components were divided into five categories based on the quintile values. For antioxidants, four points were awarded for high-level exposure, one to three point for intermediate levels, and 0 for low-level exposure. The score was reversed for pro-oxidant components. | The overall score ranged between 0 and 52 points. The score was divided into five equal intervals. | Questionnaire-based (FFQ) dietary components were considered. All nutrients were energy-adjusted. Nutrient values included dietary and supplemental sources. |
| Slattery et al., 2012 [19] | Predefined and population-dependent | 11 population-dependent dietary components (three categories for every component) and two predefined components for smoking (never, current smokers) and medication (NSAID use: never or recent/current use). | All dietary components were divided into three categories based on the tertile values. For antioxidants, two points were awarded for high-level exposure, one point for intermediate, and 0 for low-level exposure. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (e.g., non-smokers, and NSAID users), and fewer points to pro-oxidant categories. | The overall score ranged between 0 and 26 points. The score was divided into four groups: high risk (3–10), intermediate (11–13 and 14–16) and low risk (17–23). | Questionnaire-based (FFQ) dietary components were considered. Energy adjustment was considered in analyses evaluating the interaction between the polygenic score and the dietary variables. |
| Geybels et al., 2012 [17] | Predefined and population-dependent | 5 population-dependent dietary components (based on quartiles for every component) and two predefined components for smoking (never, current smokers) and alcohol (abstainers, and predefined levels of intake). | All dietary components were divided into four categories based on the quartile values. For antioxidants, two points were awarded for high-level exposure, one point for intermediate, and 0 for low-level exposure. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (e.g., non-smokers, and alcohol abstainers), and fewer points to pro-oxidant categories. | The overall score ranged between 0 and 26 points. The score was divided into four groups: low (score 4), intermediate (score 7 and 9), and highest antioxidant group (score 12). | Questionnaire-based (FFQ) dietary components were considered. Energy adjustment was not considered. |
| Dash et al., 2013 [13] | Predefined and population-dependent | 11 population-dependent dietary components (two categories for every component) and four non-dietary components for smoking, alcohol intake, obesity and physical activity. | Four methods were used of weighting all components: OBS-equal weight, OBS-lit review, OBS-a posteriori and OBS-Bayesian. For OBS-equal weight, all components were transformed to a standard normal distribution and multiplied by weights considered as +1 for antioxidants and −1 for pro-oxidants. For the other OBS, weights were calculated based on reported risk estimates, risks estimated within the study population or Bayesian analysis. | Transformed variables were multiplied by their weights and summed to generate the overall OBS. The scores were divided into tertiles: low, intermediate, and highest antioxidant group. | Questionnaire-based (FFQ) dietary components were considered. All nutrients were energy-adjusted. Nutrient values included dietary and supplemental sources. |
| Labadie et al., 2013 [20] | Predefined and population-dependent | 7 population-dependent dietary components (based on sex-specific tertiles) and four predefined components for smoking (never, former, current), alcohol intake (low, moderate and heavy), and medication (NSAID or aspirin use, non-use). | All dietary components were divided into three categories based on the tertile values. For antioxidants, two points were awarded for high-level exposure, one point for intermediate, and 0 for low-level exposure. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (e.g., non-smokers, and NSAID users), and fewer points to pro-oxidant categories. | The overall score ranged between 0 and 22 points. The score was divided into two categories (high vs. low). | Questionnaire-based dietary components were considered. Dietary components were adjusted for total energy intake. |
| Kong et al., 2014 [11] | Predefined and population-dependent | 9 population-dependent dietary/biomarkers components (tertiles for every component) and five predefined components for smoking (never, former, current), Se supplements (yes, no), alcohol intake (low, moderate, heavy), and medication (NSAID or aspirin use, non-use). | All dietary/biomarker components were divided into three categories based on the tertile values. For antioxidants, two points were awarded for high-level exposure, one point for intermediate, and 0 for low-level exposure. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (e.g., non-smokers, and NSAID users), and fewer points to pro-oxidant categories. | The overall score ranged between 0 and 28 points. The score was divided into three equal intervals: low (score 2–9), intermediate (score 10–16), and highest antioxidant group (score 17–24). | Questionnaire and biomarker-based dietary components were considered. Energy adjustment was not considered. |
| Slattery et al., 2014 [21] | Population-dependent | 6 population-dependent dietary components (quartiles for every component) including alcohol. | All dietary components were divided into four categories based on the quartile values. For antioxidants, two points were awarded for high-level exposure (4th quartile), one point for intermediate levels, and 0 for low-level exposure (1st quartile). The score was reversed for pro-oxidant components. | The overall score ranged between 0 and 12 points. The score was divided into quartiles: low, intermediate and high antioxidant group. | Questionnaire-based (FFQ) dietary components were considered. Energy adjustment of nutrients per 1000 calories. |
| Lakkur et al., 2014a [12] | Predefined and population-dependent | 15 population-dependent dietary components (quartiles); five predefined components for smoking (never, former, current), alcohol, BMI (normal, overweight, obese), physical activity and medication (NSAID use, non-use). | All dietary components were divided into four categories based on the quartile values. For antioxidants, two points were awarded for high-level exposure (4th quartile), one point for intermediate levels, and 0 for low-level exposure (1st quartile). The score was reversed for pro-oxidant components. Two weighting methods were applied: equal weights and literature-based weights. | The overall score ranged between 0 and 60 points. The score was divided into tertiles intervals or quartiles: low (scores 4–11, 5–10 and 4–12), intermediate (score 12–14, 11–15 and 13–15), and highest antioxidant group (score 15–22, 16–21 and 16–23). | Questionnaire-based (FFQ) dietary components were considered. Energy adjustment was not considered. |
| Lakkur et al., 2014b [22] | Predefined and population-dependent | 8 population-dependent dietary/biomarkers components (tertiles) and one population-dependent lifestyle factors (physical activity in tertiles) and four predefined components for smoking (non-smokers and smokers), alcohol intake (non-drinkers and drinkers), and aspirin or NSAID medication (use, non-use). | All dietary/biomarker components were divided into three tertile values. For antioxidant components: two points were awarded for high-level exposure, one point for intermediate, and 0 for low predominance of antioxidants. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (non-smokers, non-drinkers and NSAID use), and fewer points to pro-oxidant categories. | The overall score ranged between 0 and 23 points. The score was divided into three groups based on tertiles. | Biomarker-based and dietary (FFQ) components were considered. |
| Dash et al., 2015 [23] | Predefined and population-dependent | 11 population-dependent dietary components (two categories for every component) and four non-dietary components for smoking, alcohol intake, obesity and physical activity. | Four methods were used of weighting all components: OBS-equal weight, OBS-lit review, OBS-a posteriori and OBS-Bayesian For OBS-equal weight, all components were multiplied by their weights considered as +1 for antioxidants and −1 for pro-oxidants. For the other OBS, these weights were calculated based on reported risk estimates derived from reviews/ meta-analysis or study data or Bayesian analysis. | All components were multiplied by their weights and summed to generate the overall OBS. The scores were divided into quartiles. | Questionnaire-based (FFQ) dietary components were considered. All nutrients were energy-adjusted. Nutrient values included dietary and supplemental sources, except selenium intake (only supplemental intake). |
| Kong et al., 2015 [24] | Predefined and population-dependent | 10 population-dependent dietary components (sex-specific tertiles for every component) and four predefined components for smoking (never, former, current), alcohol consumption (non-drinkers, moderate and heavy drinkers), and NSAID medication (use, non-use). | All dietary components were divided into three tertile values. For antioxidant components: two points were awarded for high-level exposure, one point for intermediate, and 0 for low predominance of antioxidants. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (non-smokers, non-drinkers and NSAID use), and fewer points to pro-oxidant categories. Four weighting methods were applied: equal weights, literature-based weights, weights based on the association with biomarkers levels | The overall OBS ranged between 0 and 28 points. The score was divided into four groups based on quartiles. | Questionnaire-based (FFQ) dietary components were considered. |
| Annor et al., 2015 [25] | Predefined and population-dependent | 7 population-dependent dietary/biomarkers components (tertiles); one population-dependent lifestyle factors (physical activity tertiles) and five predefined components for smoking (non-smokers, current smokers), alcohol intake (non-drinkers, drinkers), and aspirin or NSAID medication (use, non-use), and BMI (normal, overweight and obese). | All dietary/biomarker components were divided into three tertile values. For antioxidant components: two points were awarded for high-level exposure, one point for intermediate, and 0 for low predominance of antioxidants. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (non-smokers, non-drinkers, normal weight, and NSAID use), and fewer points to pro-oxidant categories. | The overall score ranged between 0 and 26 points. The score was divided into three groups based on tertiles. | Biomarker-based and dietary components were considered. |
| Lakkur et al., 2015 [26] | Predefined and population-dependent | 10 population-dependent dietary components (tertiles) and four predefined components for smoking (non-smokers and current smokers), alcohol intake (non-drinkers, moderate, heavier drinkers), and aspirin or NSAID medication (use, non-use). | All dietary components were divided into three tertile values. For antioxidant components: two points for high-level exposure, one point for intermediate, and 0 for low predominance of antioxidants. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (non-smokers, non-drinkers and NSAID use), and fewer points to pro-oxidant categories. | The overall score ranged between 0 and 28 points. The score was divided into five equal groups: score 3–7, score 8–12, score 13–17, score 18–21 and score 22–26. | Questionnaire-based (FFQ) dietary components were considered. Energy adjustment was not considered. |
| Llori et al., 2015 [27] | Predefined and population-dependent | 10 population-dependent components (sex-specific tertiles for every component) and three predefined components for alcohol (non-drinkers, moderate, heavy drinkers) and aspirin/NSAID medication (use, non-use). | All dietary components were divided into three tertile values. For antioxidant components: two points were awarded for high-level exposure, one point for intermediate, and 0 for low predominance of antioxidants. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (non-drinkers and NSAID use), and fewer points to pro-oxidant categories. | The overall OBS ranged between 0 and 26 points. The score was divided into quartiles. | Questionnaire-based (FFQ) dietary components were considered. Energy adjustment was not considered. Smoking was excluded from the original OBS score because it is a well-known risk factor for CKD. |
| Wang et al., 2017 [28] | Predefined and population-dependent | Similar OBS components as Dash et al., 2013 [13]: 11 population-dependent dietary components (three categories for every component) and four non-dietary components for smoking, alcohol intake, obesity, and physical activity. | The OBS was built using the weighted method as described by Dash et al., 2013 [13], but with different scoring points. All dietary components were divided into three groups. For antioxidant components: two points were awarded for high-level exposure, one point for intermediate, and 0 for low predominance of antioxidants. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (non-smokers, non-drinkers, non-obese and physically active), and fewer points to pro-oxidant categories. | The overall OBS ranged between 0 and 30 points. The score was divided into two or three equal groups (low vs. high and low, intermediate and high). | Questionnaire-based (FFQ) dietary components were considered. Dietary components were adjusted for total energy intake. Nutrient values included dietary and supplemental sources. |
| Cho et al., 2017 [29] | Predefined and population-dependent | 6 population-dependent components (sex-specific quartiles), including four dietary and two non-dietary components (BMI and physical activity), and two non-dietary predefined components for smoking (never, former, current), and alcohol (levels of intake). | For antioxidant components: three points were awarded for high-level exposure, one or two points for intermediate, and 0 for low predominance of antioxidants. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categorical variables (non-smokers, non-drinkers), and fewer points to pro-oxidant categories. | The overall OBS ranged between 0 and 24 points. The score was divided into five categories. | Questionnaire-based (24-h recall) dietary components were considered. Energy adjustment was not considered. |
| Lee et al., 2017 [30] | Predefined and population-dependent | 5 population-dependent components including four dietary components and one lifestyle factor (tertiles) and two predefined components for smoking (never, former, current) and alcohol intake (levels of alcohol intake). | For antioxidant components: three points were awarded for high-level exposure, one or two points for intermediate, and 0 for low predominance of antioxidants. The score was reversed for pro-oxidant components. More points were awarded to antioxidant categories (non-smokers, non-drinkers), and fewer points to pro-oxidants. Three weighting methods were applied: equal weights, weights based on the association with MetS components and weights estimated by Principal Component Analysis. | The overall OBS ranged between 0 and 14 points. The score was divided into quartiles. | Questionnaire-based (24-h recall) dietary components were considered. |
| Dietary, Biomarkers, Food, Lifestyle Factors, and Medication Components | |
|---|---|
| Antioxidants | |
| Vitamin C [31,32] | Antioxidant that scavenges ROS and RNS Prevention of lipid peroxidation Regeneration of α-tocopherol |
| Total Carotenoids, Lutein, β-carotene, Lycopene, β-cryptoxantin, Zeaxantin [33,34,35,36,37,38] | Deactivators of singlet oxygen and lipid peroxidation Generation of free radical at high oxygen concentration Synergistic antioxidants in biological membranes inhibiting lipid peroxidation Activation transcription factors of antioxidant enzymes Induce the expression of genes encoders for the synthesis of some of the antioxidant enzymes |
| Vitamin E [39] | Lipophilic antioxidant, suppressor of the oxidative damage of polyunsaturated fatty acids present in lipoproteins, biological membranes, and tissues, through the elimination of free radicals such as the radical peroxide Protection of the cell membrane, as well as of various subcellular membranes, against the effects of lipid peroxidation Inhibition of lipid peroxidation in biological membranes Protection against the oxidation of LDL-cholesterol Prevention against risk factors or diseases initiated or promoted by ROS and RNS |
| Flavonoids [40,41,42] | Donation of hydrogen to free radicals Prevention of the formation of free radicals, metal chelators Inhibition of expression, synthesis or activity of pro-oxidant enzymes Induce the expression of genes encoders for the synthesis of some of the antioxidant enzymes |
| Glucosinolates [43,44,45] | Sensitive to induction of electrophiles such as omega-3 PUFAs and hemoxygenase-1, which catalyzes heme to biliverdin and the induction of glutathione peroxidase Induce the expression of genes encoding the synthesis of some of the antioxidant enzymes |
| Minerals: Se and Zn [46,47,48] | Cofactors of enzymes involved in the endogenous antioxidant system that interrupt cellular oxidative processes |
| Prooxidants | |
| Total Fats | Intake of lipids can contribute to oxidative stress through lipid peroxidation |
| PUFAS [54,55,56,57,58,77] | Increase the formation of lipid peroxides that contribute to oxidative stress PUFAs are involved in the regulation of inflammatory activity. Fatty acids n-6 are pro-inflammatory and fatty acids of n-3 are anti-inflammatory |
| SFA [53] | Oxidative DNA damage |
| Iron/Ferritin [59,60,61,62] | Association with oxygen transport; can catalyze oxidative reactions in the formation of free radicals Oxidative damage to lipid membranes (atherogenesis promotion) by increasing the formation of free radicals and oxidative stress that induces the peroxidation of proteins and lipids Possible intensification of oxidative stress by catalyzing the production of highly reactive hydroxyl radicals through the Haber-Weiss reaction |
| Red Meat [62] | Possible intensification of oxidative stress mediated by iron intake contained in red meat Promotion of atherogenesis |
| Lifestyle factors | |
| Antioxidants | |
| Physical Activity [63,64] | Increase in the adaptive response to oxidative stress by activating the cellular antioxidant signaling systems and improving the expression of antioxidant enzymes |
| Prooxidants | |
| Alcohol [65,78,79] | Possible increase in ROS generation and increase of inflammatory processes Induction of OS by oxidation of ethanol to acetaldehyde, which can lead to the production of ROS and RNS, oxidation of nucleic acids and decrease in the activity of antioxidant enzymes |
| Smoking Status [66,67,68,69,70] | Exogenous prooxidant: increased oxidative stress and oxidative imbalance in cellular tissues The increase of the OS load of inhaled tobacco smoke could increase through the secondary release of oxygen radicals from the inflammatory cells Increase in markers of oxidative stress in blood and tissues |
| BMI, Obesity [71] | Related to increased ROS markers Leads to redox imbalance and increased lipid peroxidation, which can lead to ROS production |
| Medication | |
| Antioxidants | |
| Aspirin [72,73,74,75] | Inhibition of ROS production in human endothelial cells exposed to oxidized LDL-cholesterol Regulation of ROS and RNS to reduce inflammation and cell damage |
| NSAIDs [72,73,74,75] | Regulation of ROS and RNS to reduce inflammation and cell damage |
| Author (s), Year | Country, Population (N), Year of Recruitment, Age at Entry | Study, Design, Follow-up Time (Years) | Main Outcome | Covariables in Adjusted Model | OR/RR/HR (95 % CI) a, Multivariable Adjusted |
|---|---|---|---|---|---|
| Van Hoydonck et al., 2002 [9] | Belgium 2814 male smokers 1980–1984; 25–74 years | BIRNH study Cohort study (10 years) | All-cause mortality Cancer mortality CVD mortality | Age, educational level, BMI, total energy intake and smoking (pack-years) | RR for high vs. low OBS: 1.44 (1.13–1.82) for all-cause mortality 1.62 (1.07–2.45) for cancer mortality 1.31 (0.86–2.00) for CVD mortality (not significant) |
| Goodman et al., 2007 [10] | USA MAP study 170 cases and 230 controls 1995–1997; ≥50 years MPC study 89 cases and 197 controls 1994–1996; ≥50 years | MAP and MPC studies Case-control studies | Adenomatous polyps Prostate cancer | Age, sex, race, energy intake | MAP study (adenomas) OR for high vs. low OSS = 0.45, (0.21–0.99) MPC study (prostate cancer) OR high vs. low OSS = 0.28, (0.28–0.82) |
| Goodman et al., 2008 [15] | USA 574 cases, 1227 endoscopy controls and 550 community controls 1991–1994; 30–74 years | Minnesota Digestive Healthcare Case-control study | Colorectal adenomas | Age, sex, hormone therapy, race, education, family history of colorectal cancer, energy intake, BMI, alcohol consumption, calcium, vitamin D, folic acid, red meat, multivitamin and dietary fiber | OR for high vs. low OBS 0.19 (0.06–0.57; p-trend < 0.001) for endoscopy controls 0.24 (0.06–0.94; p-trend = 0.002) for community controls |
| Goodman et al., 2010 [18] | USA MAP study 111 cases and 115 controls 1995–1997; ≥50 years MPC study 97 cases and 226 controls 1994–1996; ≥50 year | MAP and MCP studies Case-control studies | Colorectal adenomas Prostate cancer | Age, race, total energy intake, blood cholesterol, BMI, and family history of prostate cancer or colorectal cancer In addition, the MAP study controlled for sex, and for hormone replacement therapy among women | OBS (continuous, per unit increment) OR = 0.90 (0.83, 0.97) in both studies MAP study (adenomas) OR high vs. low OBS = 0.34 (0.13–0.88) MPC study (prostate cancer) OR high vs. low OBS = 0.34 (0.14–0.86) |
| Agalliu et al., 2011 [16] | Canada 661 cases and 1864 subcohort 1992–2003; 66.2 years (mean cases) and 69.3 years (mean subcohort) | CSDLH study Case-cohort (4.3 vs. 7.7) | Prostate cancer | Age, race, BMI, physicalactivity, and education | No association HRs high vs. low OBS across quintiles: 1.02, 1.03, 0.97 and 1.01; p-trend = 0.71. No association by aggressiveness types |
| Slattery et al., 2012 [19] | Utah, USA KPMCP Colon cancer: 1555 cases and 1956 controls: 1991–1994 Rectal cancer: 974 cases and controls; 1997–2001; 30–79 years | Case-control study | Colon cancer Rectal cancer | Total energy intake in analyses with dietary variables | OR high vs. low OBS: 0.52 (95% CI: 0.41–0.66) for colon cancer 0.49 (95% CI: 0.35–0.70) for rectal cancer |
| Geybels et al., 2012 [17] | The Netherlands 3451 cases and 2191 subcohort 62.8 years (mean cases) | NLCS study Case-cohort study 17.3 years | Prostate cancer | Age, smoking intensity and duration | HR for high vs. low OBS: 1.16 (95% CI: 0.98–1.37) No association by stage of the disease |
| Dash et al., 2013 [13] | USA 789 cases and 1500 controls 1991–2002; 30–74 years | CPRU study, MAP I study, MAP study Case-control studies | Colorectal adenomas Validation study with FIP levels | Age, sex, education, family history of colorectal cancer, aspirin, nonsteroidal anti-inflammatory, calcium, vitamin D, folate, fiber, energy intake, cumulative estrogen exposure, excluding oral contraceptive use and use of menopausal hormone therapy | OR for high vs. low OBS ranged from 0.38–0.54 for the 4 OBS (all were statically significant). OR-equal weight = 0.54 (0.43–0.69) OR-lit review = 0.45 (0.35–0.58) OR-a posteriori = 0.38 (0.29–0.49) OR-Bayesian = 0.45 (0.35–0.58) Negative association between the OBS and FIP |
| Labadie et al., 2013 [20] | USA 472 cases and 578 controls 1991–2002 59 years in cases and 54 years in controls | CPRU study; MAP I study, MAP II study Case-control studies | Colorectal adenomas by genetic variants of antioxidant genes (SOD2, CAT, GSTP1) | Age, sex, hormone therapy, family history of colorectal cancer, body composition, energy intake, physical activity, calcium, fiber, red meat, vitamin D (dietary + supplemental) | The OBS was not associated with colorectal adenoma risk by the genetic polymorphisms, individually or in combined gene scores |
| Kong et al., 2014 [11] | USA 139 cases and 201 controls 1991–2002 56.9 years in cases and 55.9 years in controls | MAP I MAP II Case-control studies | Colorectal adenoma Validation study with FIP, FOP and CRP levels | Age, race, sex, BMI d, energy intake, plasma cholesterol, family history of colorectal cancer, hormone replacement therapy, fiber, physical activity, study (MAP I or MAP II) | OR for high vs. low OBS = 0.39 (0.17–0.89) Biomarkers associations between the OBS and CRP (negative), FOP (positive) and FIP (negative) |
| Slattery et al., 2014 [21] | USA Hispanic: 2111 cases and 2597 controls Non-Hispanic: 1481 cases and 1586 controls 1995–2007; 25–79 years | Breast Cancer Health Disparities study Case-control | Breast cancer | Age, study center, BMI in referent year, parity, genetic admixture | OR for high vs. low OBS = 0.74 (0.64–0.84) |
| Lakkur et al., 2014a [22] | USA 43,325 men and 3386 cases 1999–2007; 70 years (mean) | CP Study II Nutrition Cohort Cohort study (8 years) | Prostate cancer Aggressive disease Non-aggressive disease | Age, energy intake, calcium, vitamin D and folate intake, race, education, family history of prostate cancer, cholesterol lowering drug use, finasteride use, history of prostate cancer screening | HR for high vs. low OBS: HR-equal weight = 1.17 (1.04–1.32) HR literature-weight = 1.15 (1.03–1.30) p for interaction by aggressiveness types > 0.05 |
| Lakkur et al., 2014b [12] | USA 321 participants; 25–74 years | SRSH study Cross-sectional | FIP, FOP, mtDNA | Age, sex, BMI, and race/origin | Negative association with FIP (OR high vs. low OBS = 0.04; 95% CI: 0.01–0.17) but positive with FOP (OR high vs. low OBS = 5.64; 95% CI: 2.35–13.54). The association for mtDNA copy number was unstable. Varying associations with FIP, FOP or mtDNA. |
| Dash et al., 2015 [23] | USA 80,063 1999–2009; 68–70 years | CP Study II Nutrition Prospective cohort study (10 years) | Colorectal cancer | Age, sex, education, family history of colorectal cancer in a first-degree relative, colorectal cancer screening, nonsteroidal anti-inflammatory, calcium, vitamin D, energy intake, and hormone replacement therapy | RR for high vs. low quartile: OBS-equal weight 0.59 (0.49–0.70) OBS-literature review 0.60 (0.50–0.73) OBS-a posteriori 0.47 (0.39–0.57) OBS Bayesian 0.50 (0.41–0.61) |
| Kong et al., 2015 [24] | USA 21,031 2003–2007, ≥45 years | REGARDs study Prospective cohort study (5.8 years) | All-cause mortality Cancer mortality Non-cancer mortality CVD mortality | Age, sex, race, SES, region, BMI, energy intake, and physical activity | HR for high vs. low OBS: 0.70 (0.61–0.81) for all-cause mortality; 0.50 (0.37–0.67) for cancer-mortality; 0.77 (0.66–0.89) for non-cancer mortality; Not significant for CVD mortality |
| Annor et al., 2015 [25] | USA 317 participants; 25–74 years | SRSH study Cross-sectional | Hypertension Oxidative stress markers FIP, FOP and mtDNA | Age, sex, education, and race/origin | OR for high vs. low OBS = 0.17 (0.79–0.96) OR per 1 unit increase in OBS = 0.87 (0.79–0.96) Negative correlation between OBS and FIP, but positive for FOP |
| Lakkur et al., 2015 [26] | USA 19,825 participants 2003–2007; ≥45 years | REGARDs study Cohort study (4 years) | CRP Waist circumference LDL-cholesterol HDL-cholesterol Total cholesterol Serum albumin Triglycerides | Age, sex, energy intake, BMI, race, educational level, region, and physical activity | OR for high vs. low OBS: 0.50 (0.38–0.66) for CRP; 0.50 (0.36–0.71) for waist circumference; 0.75 (0.58–0.98) for LDL-cholesterol. 0.48 (0.28–0.83) for HDL-cholesterol in women and 1.63 (1.09–2.45) in men No significant associations for serum albumin, total cholesterol and triglycerides. |
| Ilori et al., 2015 [27] | USA 19,461 participants (90 incident ESRD cases; 2519 prevalent albuminuria; 1957 prevalent CKD) 2003–2007; ≥45 years | REGARDs study Cohort study (3.5 years) and cross-sectional study for baseline markers of chronic kidney disease | ESRD CKD Albuminuria Macroalbuminuria Incident ESR | Age, sex, race, region and calories, BMI, smoking, waist circumference, physical activity, education, income, SBP, DBP, total cholesterol, CAD, diabetes and statin medications | OR/HR for high vs. low OBS: 0.67 (0.49–0.92) for macroalbuminuria; 0.79 (0.67–0.92) for CKD OR per 5-units OBS: 0.83 (0.72–0.96) for macroalbuminuria; 0.90 (0.84–0.97) for CKD Not significant for ESRD and albuminuria |
| Wang et al., 2017 [28] | USA 488 cases and 604 controls 1991–2002; 30–74 years | CPRU, MAP I, MAP II Case-control study | Interaction between based excision repair genes (BER) in genetic scores and OBS with colorectal adenoma risk | Age, sex, family history of colorectal cancer in a first degree relative, NSAID use, energy intake, fiber, circulating 25-OH-vitamin D3 concentration | OR for high weighted BER score and low OBS = 2.19 (1.19–3.99); OR for low weighted BER score and low OBS = 1.07 (0.61–1.93); OR for high weighted BER score and high OBS = 1.38 (0.75–2.53) p-value for interaction = 0.42 |
| Cho et al., 2017 [29] | Korea 2087 men and 2071 women 2010–2011; 19–65 years | KNHANES-V study Cross-sectional study | GGT | Age, energy intake, fasting plasma glucose, total cholesterol, SBP, and alanine aminotransferase | OR for high vs. low OBS = 0.05 (0.01–0.19) for men and 0.27 (0.09–0.78) for women (p for trend < 0.01). |
| Lee et al., 2017 [30] | Korea 6414 subjects 2001–2002; ≥40 years | KARE cohort study Cross-sectional study | MetS Inflammatory markers: CRP | Age, geographic area, sex, and BMI | OR for high vs. low OBS: for equal weights = 0.65 (0.51–0.83); for beta-coefficients weights = 0.56 (0.76–0.41); for principal components weights = 0.55 (0.40–0.75) No association between the OBS with any of the MetS components except for waist circumference (β = −0.98; p-value =< 0.01). |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Ruiz, Á.; García-Villanova, B.; Guerra-Hernández, E.; Amiano, P.; Ruiz-Canela, M.; Molina-Montes, E. A Review of A Priori Defined Oxidative Balance Scores Relative to Their Components and Impact on Health Outcomes. Nutrients 2019, 11, 774. https://doi.org/10.3390/nu11040774
Hernández-Ruiz Á, García-Villanova B, Guerra-Hernández E, Amiano P, Ruiz-Canela M, Molina-Montes E. A Review of A Priori Defined Oxidative Balance Scores Relative to Their Components and Impact on Health Outcomes. Nutrients. 2019; 11(4):774. https://doi.org/10.3390/nu11040774
Chicago/Turabian StyleHernández-Ruiz, Ángela, Belén García-Villanova, Eduardo Guerra-Hernández, Pilar Amiano, Miguel Ruiz-Canela, and Esther Molina-Montes. 2019. "A Review of A Priori Defined Oxidative Balance Scores Relative to Their Components and Impact on Health Outcomes" Nutrients 11, no. 4: 774. https://doi.org/10.3390/nu11040774