Usability and Engagement Evaluation of an Unguided Online Program for Promoting a Healthy Lifestyle and Reducing the Risk for Eating Disorders and Obesity in the School Setting


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment
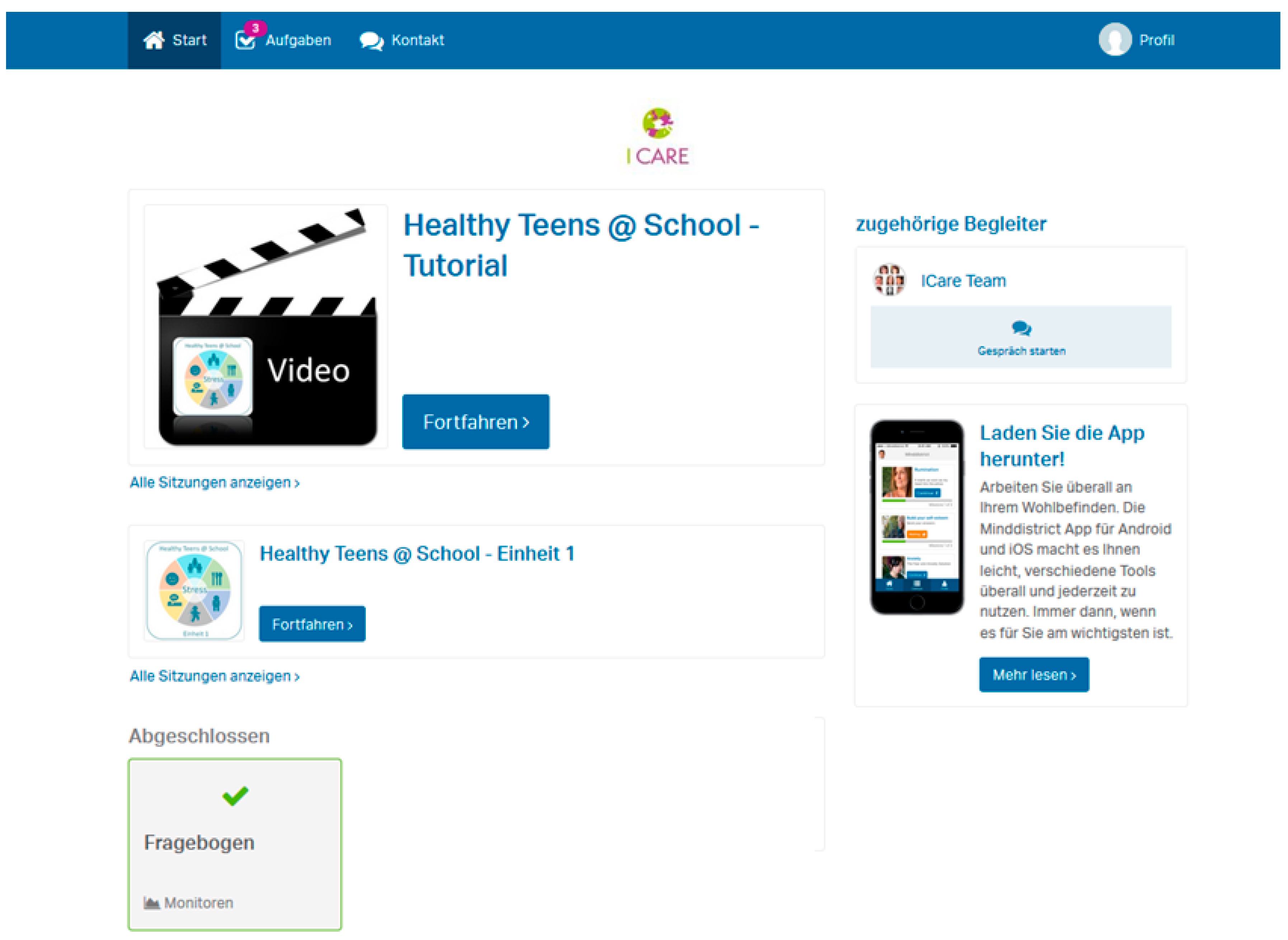
2.2. Program/Intervention
2.3. Procedure
2.4. Analysis
3. Results
3.1. Participants
3.2. SUS-Questionnaire
3.3. Think-Aloud Task and Semi-Structured Interview
3.3.1. Visual Design
3.3.2. Navigation
3.3.3. Mode of Transfer
3.3.4. Content
3.3.5. Engagement Conditions
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of obesity among adults and youth: United States, 2015-2016. NCHS Data Brief 2017, 288. [Google Scholar]
- Ahluwalia, N.; Dalmasso, P.; Rasmussen, M.; Lipsky, L.; Currie, C.; Haug, E.; Kelly, C.; Damsgaard, M.T.; Due, P.; Tabak, I.; et al. Trends in overweight prevalence among 11-, 13- and 15-year-olds in 25 countries in Europe, Canada and USA from 2002 to 2010. Eur. J. Public Health 2015, 25 (Suppl. 2), 28–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. 2000. Available online: https://www.who.int/nutrition/publications/obesity/ WHO_TRS_894/en/ (accessed on 14 February 2019).
- Hay, P.J.; Mond, J.; Buttner, P.; Darby, A. Eating disorder behaviors are increasing: Findings from two sequential community surveys in South Australia. PLoS ONE 2008, 3, e1541. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, C.; Hütter, K.; Fittig, E. Psychosocial risk factors for eating disorders. In The Oxford Handbook of Eating Disorders, 2nd ed.; Agras, W.S., Robinson, A., Eds.; Oxford University Press: New York, NY, USA, 2017. [Google Scholar]
- Shisslak, C.M.; Crago, M.; Estes, L.S. The spectrum of eating disturbances. Int. J. Eat. Disord. 1995, 18, 209–219. [Google Scholar] [CrossRef]
- Zeiler, M.; Waldherr, K.; Philipp, J.; Nitsch, M.; Dür, W.; Karwautz, A.; Wagner, G. Prevalence of eating disorder risk and associations with health-related quality of life: results from a large school-based population screening. Eur. Eat. Disord. Rev. 2016, 24, 9–18. [Google Scholar] [CrossRef]
- French, S.A.; Jeffery, R.W.; Sherwood, N.E.; Neumark-Sztainer, D. Prevalence and correlates of binge eating in a nonclinical sample of women enrolled in a weight gain prevention program. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 1999, 23, 576–585. [Google Scholar] [CrossRef] [Green Version]
- Boutelle, K.; Neumark-Sztainer, D.; Story, M.; Resnick, M. Weight control behaviors among obese, overweight, and nonoverweight adolescents. J. Pediatr. Psychol. 2002, 27, 531–540. [Google Scholar] [CrossRef]
- Field, A.E.; Austin, S.B.; Taylor, C.B.; Malspeis, S.; Rosner, B.; Rockett, H.R.; Gillman, M.W.; Colditz, G.A. Relation between dieting and weight change among preadolescents and adolescents. Pediatrics 2003, 112, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Cameron, R.P.; Killen, J.D.; Hayward, C.; Taylor, C.B. Naturalistic weight-reduction efforts prospectively predict growth in relative weight and onset of obesity among female adolescents. J. Consult. Clin. Psychol. 1999, 67, 967–974. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Wall, M.; Guo, J.; Story, M.; Haines, J.; Eisenberg, M. Obesity, disordered eating, and eating disorders in a longitudinal study of adolescents: How do dieters fare 5 years later? J. Am. Diet. Assoc. 2006, 106, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Wall, M.; Story, M.; Standish, A.R. Dieting and unhealthy weight control behaviors during adolescence: associations with 10-year changes in body mass index. J. Adolesc. Health 2012, 50, 80–86. [Google Scholar] [CrossRef]
- Haines, J.; Neumark-Sztainer, D. Prevention of obesity and eating disorders: A consideration of shared risk factors. Health Educ. Res. 2006, 21, 770–782. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Carracedo, D.; Neumark-Sztainer, D.; López-Guimerà, G. Integrated prevention of obesity and eating disorders: Barriers, developments and opportunities. Public Health Nutr. 2012, 15, 2295–2309. [Google Scholar] [CrossRef]
- Kazdin, A.E.; Fitzsimmons-Craft, E.E.; Wilfley, D.E. Addressing critical gaps in the treatment of eating disorders. Int. J. Eat. Disord. 2017, 50, 170–189. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.; Taylor Lynch, K.; Kass, A.E.; Burrows, A.; Williams, J.; Wilfley, D.E.; Taylor, C.B. Healthy weight regulation and eating disorder prevention in high school students: A universal and targeted Web-based intervention. J. Med. Internet Res. 2014, 16, e57. [Google Scholar] [CrossRef] [PubMed]
- Hollis, C.; Falconer, C.J.; Martin, J.L.; Whittington, C.; Stockton, S.; Glazebrook, C.; Davies, E.B. Annual Research Review: Digital health interventions for children and young people with mental health problems—A systematic and meta-review. J. Child Psychol. Psychiatry 2017, 58, 474–503. [Google Scholar] [CrossRef]
- European Commission Internet Access and Use Statistics—Households and Individuals 2017. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Internet_access_and_use_statistics_-_households_and_individuals&oldid=324579#Internet_use_by_individuals (accessed on 14 February 2019).
- Lee, Y.Y.; Barendregt, J.J.; Stockings, E.A.; Ferrari, A.J.; Whiteford, H.A.; Patton, G.A.; Mihalopoulos, C. The population cost-effectiveness of delivering universal and indicated school-based interventions to prevent the onset of major depression among youth in Australia. Epidemiol. Psychiatr. Sci. 2017, 26, 545–564. [Google Scholar] [CrossRef]
- Werner-Seidler, A.; Perry, Y.; Calear, A.L.; Newby, J.M.; Christensen, H. School-based depression and anxiety prevention programs for young people: A systematic review and meta-analysis. Clin. Psychol. Rev. 2017, 51, 30–47. [Google Scholar] [CrossRef] [Green Version]
- Dray, J.; Bowman, J.; Campbell, E.; Freund, M.; Wolfenden, L.; Hodder, R.K.; McElwaine, K.; Tremain, D.; Bartlem, K.; Bailey, J.; et al. Systematic review of universal resilience-focused interventions targeting child and adolescent mental health in the school setting. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 813–824. [Google Scholar] [CrossRef]
- Eysenbach, G. The law of attrition. J. Med. Internet Res. 2005, 7, e11. [Google Scholar] [CrossRef]
- Kelders, S.M.; Kok, R.N.; Ossebaard, H.C.; Gemert-Pijnen, J.E.V. Persuasive system design does matter: A systematic review of adherence to web-based interventions. J. Med. Internet Res. 2012, 14, e152. [Google Scholar] [CrossRef] [PubMed]
- Van Gemert-Pijnen, J.E.; Nijland, N.; van Limburg, M.; Ossebaard, H.C.; Kelders, S.M.; Eysenbach, G.; Seydel, E.R. A holistic framework to improve the uptake and impact of ehealth technologies. J. Med. Internet Res. 2011, 13, e111. [Google Scholar] [CrossRef]
- Jones Bell, M.; Zeiler, M.; Herrero, R.; Kuso, S.; Nitsch, M.; Etchemendy, E.; Fonseca-Baeza, S.; Oliver, E.; Adamcik, T.; Karwautz, A.; et al. Healthy Teens @ School: Evaluating and disseminating transdiagnostic preventive interventions for eating disorders and obesity for adolescents in school settings. Internet Interv. 2019, 16, 65–75. [Google Scholar] [CrossRef]
- Taylor, C.B.; Taylor, K.; Jones, M.; Shorter, A.; Yee, M.; Genkin, B.; Burrows, A.; Kass, A.E.; Rizk, M.; Redman, M.; et al. Obesity prevention in defined (high school) populations. Int. J. Obes. Suppl. 2012, 2, S30–S32. [Google Scholar] [CrossRef]
- Zeiler, M.; Kuso, S.; Nitsch, M.; Simek, M.; Adamcik, T.; Herrero, R.; Etchemendy, E.; Mira, A.; Oliver, E.; Jones Bell, M.; et al. Online Interventions to prevent mental health problems implemented in school settings: The perspectives from key stakeholders in Austria and Spain. Eur. J. Public Health 2019, in press. [Google Scholar]
- Nitsch, M.; Dimopoulos, C.N.; Flaschberger, E.; Saffran, K.; Kruger, J.F.; Garlock, L.; Wilfley, D.E.; Taylor, C.B.; Jones, M. A Guided online and mobile self-help program for individuals with eating disorders: An iterative engagement and usability study. J. Med. Internet Res. 2016, 18, e7. [Google Scholar] [CrossRef]
- Wangberg, S.C.; Bergmo, T.S.; Johnsen, J.-A.K. Adherence in Internet-based interventions. Patient Prefer. Adherence 2008, 2, 57–65. [Google Scholar]
- Wanner, M.; Martin-Diener, E.; Bauer, G.; Braun-Fahrländer, C.; Martin, B.W. Comparison of trial participants and open access users of a web-based physical activity intervention regarding adherence, attrition, and repeated participation. J. Med. Internet Res. 2010, 12, e3. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J. Iterative user-interface design. Computer 1993, 26, 32–41. [Google Scholar] [CrossRef]
- Nielsen, J.; Landauer, T.K. A Mathematical Model of the Finding of Usability Problems. In Proceedings of the INTERACT ’93 and CHI ’93 Conference on Human Factors in Computing Systems, Amsterdam, The Netherlands, 24–29 April 1993; ACM: New York, NY, USA, 1993; pp. 206–213. [Google Scholar]
- Spirito, A.; Stark, L.J.; Williams, C. Development of a brief coping checklist for use with pediatric populations. J. Pediatr. Psychol. 1988, 13, 555–574. [Google Scholar] [CrossRef]
- Tylka, T.L.; Kroon Van Diest, A.M. The Intuitive Eating Scale-2: Item refinement and psychometric evaluation with college women and men. J. Couns. Psychol. 2013, 60, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Van Dyck, Z.; Herbert, B.M.; Happ, C.; Kleveman, G.V.; Vögele, C. German version of the intuitive eating scale: Psychometric evaluation and application to an eating disordered population. Appetite 2016, 105, 798–807. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Roth, M.; Decker, O.; Herzberg, P.Y.; Brähler, E. Dimensionality and Norms of the Rosenberg Self-esteem Scale in a German General Population Sample. Eur. J. Psychol. Assess. 2008, 24, 190–197. [Google Scholar] [CrossRef]
- Mattejat, F.; Remschmidt, H. ILK-Inventar zur Erfassung der Lebensqualität bei Kindern und Jugendlichen: Ratingbogen für Kinder, Jugendliche und Eltern: Manual; Huber: Bern, Switzerland, 2006. [Google Scholar]
- Brooke, J. System usability scale (SUS): A quick-and-dirty method of system evaluation user information. Read. UK Digit. Equip. Co Ltd. 1986, 43. [Google Scholar]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An empirical evaluation of the system usability scale. Int. J. Hum. Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Froschauer, U.; Lueger, M. Das Qualitative Interview, 1st ed.; Facultas: Vienna, Austria, 1993. [Google Scholar]
- Grieben, C.; Stassen, G.; Froböse, I. How should web-based physical activity and healthy eating interventions be designed for young office workers? A Qualitative Approach. J. Healthc. Commun. 2018, 3, 1–15. [Google Scholar]
- Schaarup, C.; Hartvigsen, G.; Larsen, L.B.; Tan, Z.-H.; Årsand, E.; Hejlesen, O.K. Assessing the potential use of eye-tracking triangulation for evaluating the usability of an online diabetes exercise system. Stud. Health Technol. Inform. 2015, 216, 84–88. [Google Scholar] [PubMed]
- Ludden, G.D.S.; van Rompay, T.J.L.; Kelders, S.M.; van Gemert-Pijnen, J.E.W.C. How to increase reach and adherence of web-based interventions: A design research viewpoint. J. Med. Internet Res. 2015, 17, e172. [Google Scholar] [CrossRef] [PubMed]
- Kuosmanen, T.; Fleming, T.M.; Barry, M.M. Using computerized mental health programs in alternative education: Understanding the requirements of students and staff. Health Commun. 2018, 33, 753–761. [Google Scholar] [CrossRef]
- Neil, A.L.; Batterham, P.; Christensen, H.; Bennett, K.; Griffiths, K.M. Predictors of adherence by adolescents to a cognitive behavior therapy website in school and community-based settings. J. Med. Internet Res. 2009, 11, e6. [Google Scholar] [CrossRef]
- Masia-Warner, C.; Nangle, D.W.; Hansen, D.J. Bringing evidence-based child mental health services to the schools: General issues and specific populations. Educ. Treat. Child. 2006, 29, 165–172. [Google Scholar]
- Kern, L.; Mathur, S.R.; Albrecht, S.F.; Poland, S.; Rozalski, M.; Skiba, R.J. The need for school-based mental health services and recommendations for implementation. School Ment. Health 2017, 9, 205–217. [Google Scholar] [CrossRef]
- Arango, C.; Díaz-Caneja, C.M.; McGorry, P.D.; Rapoport, J.; Sommer, I.E.; Vorstman, J.A.; McDaid, D.; Marín, O.; Serrano-Drozdowskyj, E.; Freedman, R.; et al. Preventive strategies for mental health. Lancet Psychiatry 2018, 5, 591–604. [Google Scholar] [CrossRef]
- Dopp, A.R.; Parisi, K.E.; Munson, S.A.; Lyon, A.R. A glossary of user-centered design strategies for implementation experts. Transl. Behav. Med. 2018, in press. [Google Scholar] [CrossRef] [PubMed]
- Mohr, D.C.; Lyon, A.R.; Lattie, E.G.; Reddy, M.; Schueller, S.M. Accelerating digital mental health research from early design and creation to successful implementation and sustainment. J. Med. Internet Res. 2017, 19, e153. [Google Scholar] [CrossRef] [PubMed]
- Dopp, A.R.; Parisi, K.E.; Munson, S.A.; Lyon, A.R. Integrating implementation and user-centred design strategies to enhance the impact of health services: Protocol from a concept mapping study. Health Res. Policy Syst. 2019, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Lyon, A.R.; Koerner, K. User-Centered Design for Psychosocial Intervention Development and Implementation. Clin. Psychol. Publ. Div. Clin. Psychol. Am. Psychol. Assoc. 2016, 23, 180–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beecham, J.; Bonin, E.-M.; Görlich, D.; Baños, R.; Beintner, I.; Buntrock, C.; Bolinski, F.; Botella, C.; Ebert, D.D.; Herrero, R.; et al. Assessing the costs and cost-effectiveness of ICare internet-based interventions (protocol). Internet Interv. 2019, 16, 12–19. [Google Scholar] [CrossRef]
- Beintner, I.; Görlich, D.; Berger, T.; Ebert, D.D.; Zeiler, M.; Herrero Camarano, R.; Waldherr, K.; Jacobi, C. Interrelations between participant and intervention characteristics, process variables and outcomes in online interventions: A protocol for overarching analyses within and across seven clinical trials in ICare. Internet Interv. 2019, 16, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nitsch, M.; Adamcik, T.; Kuso, S.; Zeiler, M.; Waldherr, K. Usability and Engagement Evaluation of an Unguided Online Program for Promoting a Healthy Lifestyle and Reducing the Risk for Eating Disorders and Obesity in the School Setting. Nutrients 2019, 11, 713. https://doi.org/10.3390/nu11040713
Nitsch M, Adamcik T, Kuso S, Zeiler M, Waldherr K. Usability and Engagement Evaluation of an Unguided Online Program for Promoting a Healthy Lifestyle and Reducing the Risk for Eating Disorders and Obesity in the School Setting. Nutrients. 2019; 11(4):713. https://doi.org/10.3390/nu11040713
Chicago/Turabian StyleNitsch, Martina, Tanja Adamcik, Stefanie Kuso, Michael Zeiler, and Karin Waldherr. 2019. "Usability and Engagement Evaluation of an Unguided Online Program for Promoting a Healthy Lifestyle and Reducing the Risk for Eating Disorders and Obesity in the School Setting" Nutrients 11, no. 4: 713. https://doi.org/10.3390/nu11040713