Assessment of Vitamin Status in Patients with Nontuberculous Mycobacterial Pulmonary Disease: Potential Role of Vitamin A as a Risk Factor


Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Design, Diagnosis, and Definitions
2.2. Analytical Procedures
2.3. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Population
3.2. Vitamin Status in the Study Population
3.3. Factors Associated with Vitamin Concentrations of the Study Population
3.4. Associations between Vitamin Concentrations and Treatment Outcome of NTM-PD
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Prevots, D.R.; Marras, T.K. Epidemiology of human pulmonary infection with nontuberculous mycobacteria: A review. Clin. Chest Med. 2015, 36, 13–34. [Google Scholar] [CrossRef] [PubMed]
- Stout, J.E.; Koh, W.J.; Yew, W.W. Update on pulmonary disease due to non-tuberculous mycobacteria. Int. J. Infect. Dis. 2016, 45, 123–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, R.E.; Moon, S.M.; Ahn, S.; Jhun, B.W.; Jeon, K.; Kwon, O.J.; Huh, H.J.; Ki, C.S.; Lee, N.Y.; Koh, W.J. Changing epidemiology of nontuberculous mycobacterial lung diseases in a tertiary referral hospital in Korea between 2001 and 2015. J. Korean Med. Sci. 2018, 33, e65. [Google Scholar] [CrossRef] [PubMed]
- Philley, J.V.; Griffith, D.E. Treatment of slowly growing mycobacteria. Clin. Chest Med. 2015, 36, 79–90. [Google Scholar] [CrossRef]
- Koh, W.J.; Stout, J.E.; Yew, W.W. Advances in the management of pulmonary disease due to Mycobacterium abscessus complex. Int. J. Tuberc. Lung Dis. 2014, 18, 1141–1148. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Choi, R.; Park, H.D.; Lee, H.; Jeong, B.H.; Park, H.Y.; Jeon, K.; Kwon, O.J.; Koh, W.J.; Lee, S.Y. Evaluation of vitamin status in patients with pulmonary tuberculosis. J. Infect. 2017, 74, 272–280. [Google Scholar] [CrossRef]
- Pakasi, T.A.; Karyadi, E.; Wibowo, Y.; Simanjuntak, Y.; Suratih, N.M.; Salean, M.; Darmawidjaja, N.; van der Meer, J.W.; van der Velden, K.; Dolmans, W.M. Vitamin A deficiency and other factors associated with severe tuberculosis in Timor and Rote Islands, East Nusa Tenggara Province, Indonesia. Eur. J. Clin. Nutr. 2009, 63, 1130–1135. [Google Scholar] [CrossRef] [Green Version]
- Aibana, O.; Franke, M.F.; Huang, C.C.; Galea, J.T.; Calderon, R.; Zhang, Z.; Becerra, M.C.; Smith, E.R.; Ronnenberg, A.G.; Contreras, C.; et al. Impact of Vitamin A and carotenoids on the risk of tuberculosis progression. Clin. Infect. Dis. 2017, 65, 900–909. [Google Scholar] [CrossRef]
- Aibana, O.; Franke, M.F.; Huang, C.C.; Galea, J.T.; Calderon, R.; Zhang, Z.; Becerra, M.C.; Smith, E.R.; Contreras, C.; Yataco, R.; et al. Vitamin E status is inversely associated with risk of incident tuberculosis disease among household contacts. J. Nutr. 2018, 148, 56–62. [Google Scholar] [CrossRef]
- Plit, M.L.; Theron, A.J.; Fickl, H.; van Rensburg, C.E.; Pendel, S.; Anderson, R. Influence of antimicrobial chemotherapy and smoking status on the plasma concentrations of vitamin C, vitamin E, beta-carotene, acute phase reactants, iron and lipid peroxides in patients with pulmonary tuberculosis. Int. J. Tuberc. Lung Dis. 1998, 2, 590–596. [Google Scholar]
- Qrafli, M.; El Kari, K.; Aguenaou, H.; Bourkadi, J.E.; Sadki, K.; El Mzibri, M. Low plasma vitamin A concentration is associated with tuberculosis in Moroccan population: A preliminary case control study. BMC Res. Notes 2017, 10, 421. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Park, J.S.; Cho, Y.J.; Yoon, H.I.; Song, J.H.; Lee, C.T.; Lee, J.H. Low serum 25-hydroxyvitamin D level: An independent risk factor for tuberculosis? Clin. Nutr. 2014, 33, 1081–1086. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.Y.; Kim, S.Y.; Chung, K.S.; Kim, E.Y.; Jung, J.Y.; Park, M.S.; Kim, Y.S.; Kim, S.K.; Chang, J.; Kang, Y.A. Association between vitamin D deficiency and tuberculosis in a Korean population. Int. J. Tuberc. Lung Dis. 2014, 18, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Ustianowski, A.; Shaffer, R.; Collin, S.; Wilkinson, R.J.; Davidson, R.N. Prevalence and associations of vitamin D deficiency in foreign-born persons with tuberculosis in London. J. Infect. 2005, 50, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Wejse, C.; Olesen, R.; Rabna, P.; Kaestel, P.; Gustafson, P.; Aaby, P.; Andersen, P.L.; Glerup, H.; Sodemann, M. Serum 25-hydroxyvitamin D in a West African population of tuberculosis patients and unmatched healthy controls. Am. J. Clin. Nutr. 2007, 86, 1376–1383. [Google Scholar] [CrossRef] [PubMed]
- Ho-Pham, L.T.; Nguyen, N.D.; Nguyen, T.T.; Nguyen, D.H.; Bui, P.K.; Nguyen, V.N.; Nguyen, T.V. Association between vitamin D insufficiency and tuberculosis in a Vietnamese population. BMC Infect. Dis. 2010, 10, 306. [Google Scholar] [CrossRef] [PubMed]
- Mastala, Y.; Nyangulu, P.; Banda, R.V.; Mhemedi, B.; White, S.A.; Allain, T.J. Vitamin D deficiency in medical patients at a central hospital in Malawi: A comparison with TB patients from a previous study. PLoS ONE 2013, 8, e59017. [Google Scholar] [CrossRef]
- Venturini, E.; Facchini, L.; Martinez-Alier, N.; Novelli, V.; Galli, L.; de Martino, M.; Chiappini, E. Vitamin D and tuberculosis: A multicenter study in children. BMC Infect. Dis. 2014, 14, 652. [Google Scholar] [CrossRef]
- Gopinath, K.; Venclovas, C.; Ioerger, T.R.; Sacchettini, J.C.; McKinney, J.D.; Mizrahi, V.; Warner, D.F. A vitamin B12 transporter in Mycobacterium tuberculosis. Open Biol. 2013, 3, 120175. [Google Scholar] [CrossRef]
- Young, D.B.; Comas, I.; de Carvalho, L.P.S. Phylogenetic analysis of vitamin B12-related metabolism in Mycobacterium tuberculosis. Front. Mol. Biosci. 2015, 2, 6. [Google Scholar] [CrossRef]
- Griffith, D.E.; Aksamit, T.; Brown-Elliott, B.A.; Catanzaro, A.; Daley, C.; Gordin, F.; Holland, S.M.; Horsburgh, R.; Huitt, G.; Iademarco, M.F.; et al. An official ATS/IDSA statement: Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am. J. Respir. Crit. Care Med. 2007, 175, 367–416. [Google Scholar] [CrossRef] [PubMed]
- Koh, W.J.; Moon, S.M.; Kim, S.Y.; Woo, M.A.; Kim, S.; Jhun, B.W.; Park, H.Y.; Jeon, K.; Huh, H.J.; Ki, C.S.; et al. Outcomes of Mycobacterium avium complex lung disease based on clinical phenotype. Eur. Respir. J. 2017, 50, 1602503. [Google Scholar] [CrossRef] [PubMed]
- Koh, W.J.; Jeong, B.H.; Kim, S.Y.; Jeon, K.; Park, K.U.; Jhun, B.W.; Lee, H.; Park, H.Y.; Kim, D.H.; Huh, H.J.; et al. Mycobacterial characteristics and treatment outcomes in Mycobacterium abscessus lung disease. Clin. Infect. Dis. 2017, 64, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Koh, W.J.; Jeong, B.H.; Jeon, K.; Kim, S.Y.; Park, K.U.; Park, H.Y.; Huh, H.J.; Ki, C.S.; Lee, N.Y.; Lee, S.H.; et al. Oral macrolide therapy following short-term combination antibiotic treatment for Mycobacterium massiliense lung disease. Chest 2016, 150, 1211–1221. [Google Scholar] [CrossRef] [PubMed]
- Who Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- Van Ingen, J.; Aksamit, T.; Andrejak, C.; Bottger, E.C.; Cambau, E.; Daley, C.L.; Griffith, D.E.; Guglielmetti, L.; Holland, S.M.; Huitt, G.A.; et al. Treatment outcome definitions in nontuberculous mycobacterial pulmonary disease: An NTM-NET consensus statement. Eur. Respir. J. 2018, 51, 1800170. [Google Scholar] [CrossRef]
- Rwangabwoba, J.M.; Fischman, H.; Semba, R.D. Serum vitamin A levels during tuberculosis and human immunodeficiency virus infection. Int. J. Tuberc. Lung Dis. 1998, 2, 771–773. [Google Scholar] [PubMed]
- De Pee, S.; Dary, O. Biochemical indicators of vitamin A deficiency: Serum retinol and serum retinol binding protein. J. Nutr. 2002, 132, 2895s–2901s. [Google Scholar] [CrossRef]
- Erickson, K.L.; Medina, E.A.; Hubbard, N.E. Micronutrients and innate immunity. J. Infect. Dis. 2000, 182 (Suppl. 1), S5–S10. [Google Scholar] [CrossRef]
- Katona, P.; Katona-Apte, J. The interaction between nutrition and infection. Clin. Infect. Dis. 2008, 46, 1582–1588. [Google Scholar] [CrossRef]
- Pekmezci, D. Vitamin E and immunity. Vitam. Horm. 2011, 86, 179–215. [Google Scholar] [PubMed]
- Tamura, J.; Kubota, K.; Murakami, H.; Sawamura, M.; Matsushima, T.; Tamura, T.; Saitoh, T.; Kurabayshi, H.; Naruse, T. Immunomodulation by vitamin B12: Augmentation of CD8+ T lymphocytes and natural killer (NK) cell activity in vitamin B12-deficient patients by methyl-B12 treatment. Clin. Exp. Immunol. 1999, 116, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Boran, P.; Yildirim, S.; Karakoc-Aydiner, E.; Ogulur, I.; Ozen, A.; Haklar, G.; Koc, A.; Akkoc, T.; Barlan, I. Vitamin B12 deficiency among asymptomatic healthy infants: Its impact on the immune system. Available online: https://europepmc.org/abstract/med/26763692 (accessed on 4 Febraury 2019).
- Thurnham, D.I.; McCabe, G.P.; Northrop-Clewes, C.A.; Nestel, P. Effects of subclinical infection on plasma retinol concentrations and assessment of prevalence of vitamin A deficiency: Meta-analysis. Lancet 2003, 362, 2052–2058. [Google Scholar] [CrossRef]
- Coleman, M.M.; Basdeo, S.A.; Coleman, A.M.; Cheallaigh, C.N.; Peral de Castro, C.; McLaughlin, A.M.; Dunne, P.J.; Harris, J.; Keane, J. All-trans retinoic acid augments autophagy during intracellular bacterial infection. Am. J. Respir. Cell Mol. Biol. 2018, 59, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Wheelwright, M.; Kim, E.W.; Inkeles, M.S.; De Leon, A.; Pellegrini, M.; Krutzik, S.R.; Liu, P.T. All-trans retinoic acid-triggered antimicrobial activity against Mycobacterium tuberculosis is dependent on NPC2. J. Immunol. 2014, 192, 2280–2290. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, S.; DeBerry, J. Can a vitamin a day keep tuberculosis away? Am. J. Respir. Cell Mol. Biol. 2018, 59, 523–524. [Google Scholar] [CrossRef]
- Yamshchikov, A.V.; Desai, N.S.; Blumberg, H.M.; Ziegler, T.R.; Tangpricha, V. Vitamin D for treatment and prevention of infectious diseases: A systematic review of randomized controlled trials. Endocr. Pract. 2009, 15, 438–449. [Google Scholar] [CrossRef]
- Bar-On, O.; Mussaffi, H.; Mei-Zahav, M.; Prais, D.; Steuer, G.; Stafler, P.; Hananya, S.; Blau, H. Increasing nontuberculous mycobacteria infection in cystic fibrosis. J. Cyst. Fibros. 2015, 14, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Jeon, K.; Kim, S.Y.; Jeong, B.H.; Chang, B.; Shin, S.J.; Koh, W.J. Severe vitamin D deficiency is associated with non-tuberculous mycobacterial lung disease: A case-control study. Respirology 2013, 18, 983–988. [Google Scholar] [CrossRef]
- He, C.S.; Gleeson, M.; Fraser, W.D. Measurement of circulating 25-hydroxy vitamin d using three commercial enzyme-linked immunosorbent assay kits with comparison to liquid chromatography: Tandem mass spectrometry method. ISRN Nutr. 2013, 2013, 723139. [Google Scholar] [CrossRef]
- Kim, H.J.; Ji, M.; Song, J.; Moon, H.W.; Hur, M.; Yun, Y.M. Clinical utility of measurement of vitamin D-binding protein and calculation of bioavailable vitamin D in assessment of vitamin D status. Ann. Lab. Med. 2017, 37, 34–38. [Google Scholar] [CrossRef]
- Le Goff, C.; Cavalier, E.; Souberbielle, J.C.; Gonzalez-Antuna, A.; Delvin, E. Measurement of circulating 25-hydroxyvitamin D: A historical review. Pract. Lab. Med. 2015, 2, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arneson, W.L.; Arneson, D.L. Current methods for routine clinical laboratory testing of vitamin D levels. Lab. Med. 2013, 44, e38–e42. [Google Scholar] [CrossRef]
- Koivula, M.K.; Matinlassi, N.; Laitinen, P.; Risteli, J. Four automated 25-OH total vitamin D immunoassays and commercial liquid chromatography tandem-mass spectrometry in Finnish population. Clin. Lab. 2013, 59, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Kwak, H.-S.; Chung, H.-J.; Cho, D.-H.; Park, M.-H.; Ku, E.-S.; Park, E.J.; Oh, H.J. Efficacy of the measurement of 25-hydroxyvitamin D2 and D3 levels by using PerkinElmer liquid chromatography-tandem mass spectrometry vitamin D kit compared with DiaSorin radioimmunoassay kit and Elecsys vitamin D total assay. Ann. Lab. Med. 2015, 35, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Sexton, P.; Harrison, A.C. Susceptibility to nontuberculous mycobacterial lung disease. Eur. Respir. J. 2008, 31, 1322–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Chang, B.; Jeong, B.H.; Park, H.Y.; Jeon, K.; Shin, S.J.; Koh, W.J. Implication of vitamin D-associated factors in patients with non-tuberculous mycobacterial lung disease. Int. J. Tuberc. Lung Dis. 2016, 20, 1594–1602. [Google Scholar] [CrossRef]
- Lewis, S.J.; Baker, I.; Davey Smith, G. Meta-analysis of vitamin D receptor polymorphisms and pulmonary tuberculosis risk. Int. J. Tuberc. Lung Dis. 2005, 9, 1174–1177. [Google Scholar]
- Gao, L.; Tao, Y.; Zhang, L.; Jin, Q. Vitamin D receptor genetic polymorphisms and tuberculosis: Updated systematic review and meta-analysis. Int. J. Tuberc. Lung Dis. 2010, 14, 15–23. [Google Scholar]
- Gelder, C.M.; Hart, K.W.; Williams, O.M.; Lyons, E.; Welsh, K.I.; Campbell, I.A.; Marshall, S.E. Vitamin D receptor gene polymorphisms and susceptibility to Mycobacterium malmoense pulmonary disease. J. Infect. Dis. 2000, 181, 2099–2102. [Google Scholar] [CrossRef]
- Park, S.; Kim, E.J.; Lee, S.H.; Suh, G.Y.; Chung, M.P.; Kim, H.; Kwon, O.J.; Koh, W.J. Vitamin D-receptor polymorphisms and non-tuberculous mycobacterial lung disease in Korean patients. Int. J. Tuberc. Lung Dis. 2008, 12, 698–700. [Google Scholar] [PubMed]
- Madebo, T.; Lindtjorn, B.; Aukrust, P.; Berge, R.K. Circulating antioxidants and lipid peroxidation products in untreated tuberculosis patients in Ethiopia. Am. J. Clin. Nutr. 2003, 78, 117–122. [Google Scholar] [CrossRef]
- Traber, M.G.; Atkinson, J. Vitamin E, antioxidant and nothing more. Free Radic. Biol. Med. 2007, 43, 4–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.Y.; Man-Fan Wan, J. Vitamin E supplementation improves cell-mediated immunity and oxidative stress of Asian men and women. J. Nutr. 2000, 130, 2932–2937. [Google Scholar] [CrossRef] [PubMed]
- Kolleck, I.; Sinha, P.; Rustow, B. Vitamin E as an antioxidant of the lung: Mechanisms of vitamin E delivery to alveolar type II cells. Am. J. Respir. Crit. Care Med. 2002, 166, S62–S66. [Google Scholar] [CrossRef] [PubMed]
- Seyedrezazadeh, E.; Ostadrahimi, A.; Mahboob, S.; Assadi, Y.; Ghaemmagami, J.; Pourmogaddam, M. Effect of vitamin E and selenium supplementation on oxidative stress status in pulmonary tuberculosis patients. Respirology 2008, 13, 294–298. [Google Scholar] [CrossRef]
- Stabler, S.P. Vitamin B12 deficiency. N. Engl. J. Med. 2013, 368, 149–160. [Google Scholar] [CrossRef]
- Chan, E.D.; Iseman, M.D. Slender, older women appear to be more susceptible to nontuberculous mycobacterial lung disease. Gend. Med. 2010, 7, 5–18. [Google Scholar] [CrossRef]
- Wakamatsu, K.; Nagata, N.; Maki, S.; Omori, H.; Kumazoe, H.; Ueno, K.; Matsunaga, Y.; Hara, M.; Takakura, K.; Fukumoto, N.; et al. Patients with MAC lung disease have a low visceral fat area and low nutrient intake. Pulm. Med. 2015, 2015, 218253. [Google Scholar] [CrossRef]
- Ikegame, S.; Maki, S.; Wakamatsu, K.; Nagata, N.; Kumazoe, H.; Fujita, M.; Nakanishi, Y.; Kawasaki, M.; Kajiki, A. Nutritional assessment in patients with pulmonary nontuberculous mycobacteriosis. Intern. Med. 2011, 50, 2541–2546. [Google Scholar] [CrossRef]
- Hong, J.Y.; Yang, G.E.; Ko, Y.; Park, Y.B.; Sim, Y.S.; Park, S.H.; Lee, C.Y.; Jung, K.-S.; Lee, M.G. Changes in cholesterol level correlate with the course of pulmonary nontuberculous mycobacterial disease. J. Thorac. Dis. 2016, 8, 2885–2894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burtis, C.A.; Ashwood, E.R.; Bruns, D.E. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics-e-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Vyroubal, P.; Chiarla, C.; Giovannini, I.; Hyspler, R.; Ticha, A.; Hrnciarikova, D.; Zadak, Z. Hypocholesterolemia in clinically serious conditions—Review. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czechoslov. Repub. 2008, 152, 181–189. [Google Scholar] [CrossRef]
- Cham, B.E.; Smith, J.L.; Colquhoun, D.M. Correlations between cholesterol, vitamin E, and vitamin K1 in serum: Paradoxical relationships to established epidemiological risk factors for cardiovascular disease. Clin. Chem. 1998, 44, 1753–1755. [Google Scholar] [PubMed]
- Gey, K.F.; Puska, P. Plasma vitamins E and A inversely correlated to mortality from ischemic heart disease in cross-cultural epidemiology. Ann. N. Y. Acad. Sci. 1989, 570, 268–282. [Google Scholar] [CrossRef] [PubMed]
- Jordan, P.; Brubacher, D.; Moser, U.; Stahelin, H.B.; Gey, K.F. Vitamin E and vitamin A concentrations in plasma adjusted for cholesterol and triglycerides by multiple regression. Clin. Chem. 1995, 41, 924–927. [Google Scholar]
- Grobler, L.; Nagpal, S.; Sudarsanam, T.D.; Sinclair, D. Nutritional supplements for people being treated for active tuberculosis. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef]
- Mehta, S.; Mugusi, F.M.; Bosch, R.J.; Aboud, S.; Urassa, W.; Villamor, E.; Fawzi, W.W. Vitamin D status and TB treatment outcomes in adult patients in Tanzania: A cohort study. BMJ Open 2013, 3, e003703. [Google Scholar] [CrossRef]


{kind=link}
| NTM Patients (n = 150) | Controls (n = 150) | p-Value | |
|---|---|---|---|
| Demographic characteristics | |||
| Age, years | 59 (52–67) a | 58 (53–65) | 0.691 |
| Female, N (%) | 106 (70.7) | 106 (70.7) | 1.000 |
| BMI, kg/m2 | 20.7 (19.2–22.3) | 23.3 (21.2–24.8) | <0.001 |
| BMI < 18.5 kg/m2 | 25 (16.7) | 4 (2.7) | <0.001 |
| BMI ≥ 18.5 kg/m2 | 125 (83.3) | 146 (97.3) | |
| Serum chemistry results | |||
| Total protein (g/dL) | 7.4 (7.1–7.7) | 7.0 (6.8–7.4) | <0.001 |
| Albumin (g/dL) | 4.4 (4.3–4.6) | 4.3 (4.2–4.5) | 0.001 |
| Albumin/globulin ratio | 1.5 (1.4–1.7) | 1.6 (1.5–1.7) | 0.001 |
| CRP (mg/dL) | 0.12 (0.05–0.57) | 0.04 (0.03–0.07) | <0.001 |
| Total cholesterol (mg/dL) | 180.5 (158.8–201.0) | 196.5 (178.0–223.0) | <0.001 |
| AST (U/L) | 21.0 (18.0–25.0) | 21.0 (18.0–25.0) | 0.976 |
| ALT (U/L) | 17.0 (12.0–21.0) | 17.5 (13.8–24.3) | 0.165 |
| NTM Patients (n = 150) | Controls (n = 150) | p-Value | Odds Ratio (95% CI) | |
|---|---|---|---|---|
| Serum vitamin concentrations a | ||||
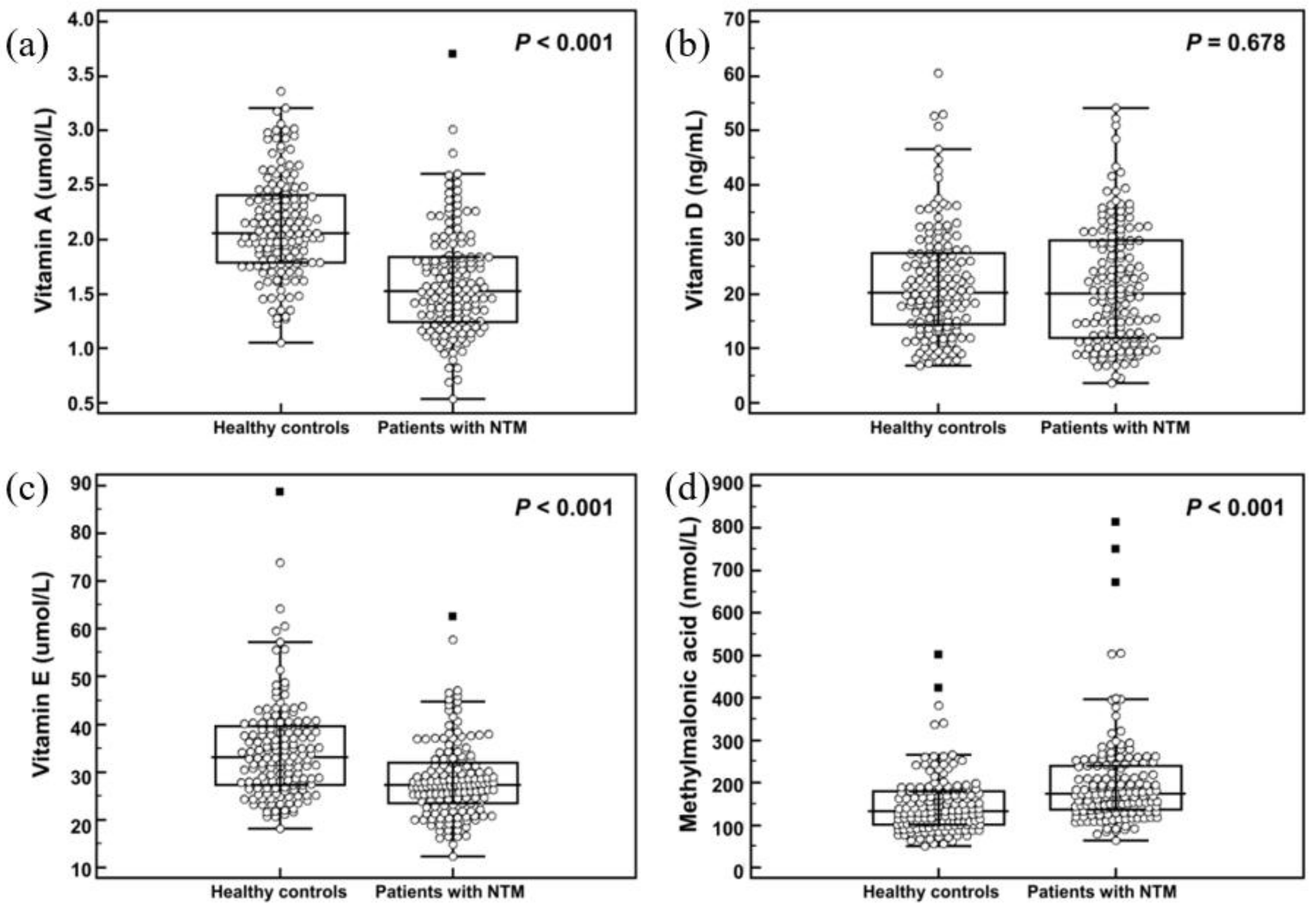
| Vitamin A (µmol/L) | 1.5 (1.2–1.8) | 2.1 (1.8–2.4) | < 0.001 | 0.091 (0.049–0.170) |
| Vitamin D (ng/mL) | 20.2 (11.9–29.8) | 20.3 (14.3–27.6) | 0.678 | 0.995 (0.974–1.017) |
| Vitamin E (µmol/L) | 27.3 (23.3–32.1) | 33.1 (27.4–39.6) | < 0.001 | 0.921 (0.892–0.950) |
| Homocysteine (µmol/L) | 10.2 (8.2–12.4) | 9.9 (8.2–11.8) | 0.101 | 1.063 (0.988–1.143) |
| Methylmalonic acid (nmol/L) | 173.8 (135.9–240.6) | 132.9 (101.5–180.8) | < 0.001 | 1.008 (1.005–1.012) |
| Vitamin deficiency b | ||||
| Vitamin A deficiency | 11 (7.3%) | 0 (0.0%) | 0.001 | |
| Vitamin D deficiency | 75 (50.0%) | 73 (48.7%) | 0.908 | |
| Vitamin E deficiency | 0 (0.0%) | 0 (0.0%) | 1.000 | |
| Vitamin B12 deficiency | 2 (1.3%) | 0 (0.0%) | 0.498 | |
| Vitamin A and D deficiency | 9 (6.0%) | 0 (0.0%) | 0.004 | |
| Vitamin D and B12 deficiency | 2 (2.6%) | 0 (0.0%) | 0.498 |
| Age | Sex | BMI | Total Protein | Albumin | CRP | Total Cholesterol | AST | ALT | |
|---|---|---|---|---|---|---|---|---|---|
| Vitamin A | 0.080 | −0.112 | 0.367 b | −0.253 b | 0.103 | −0.374 b | 0.314 b | 0.069 | 0.286 b |
| Vitamin D | 0.187 b | −0.078 | 0.132 b | −0.095 | −0.017 | −0.025 | 0.011 | 0.101 | 0.096 |
| Vitamin E | 0.154 b | 0.176 b | 0.141 b | −0.130 b | −0.081 | −0.109 | 0.593 b | 0.068 | 0.105 |
| Homocysteine | 0.277 b | −0.277 b | 0.032 | 0.147 b | 0.090 | 0.157 b | 0.004 | 0.054 | 0.026 |
| Methylmalonic acid | 0.114 b | 0.038 | −0.209 b | 0.069 | −0.036 | 0.193 b | −0.081 | 0.033 | −0.067 |
| Success (N = 77) | Failure (N = 33) | p-Value | |
|---|---|---|---|
| Demographic characteristics | |||
| Age, years | 59 (53–67) a | 58 (49–70) | 0.966 |
| Female, N (%) | 53 (69%) | 23 (70%) | 0.929 |
| BMI, kg/m2 | 20.8 (13.9–30.5) | 20.3 (19.5–21.2) | 0.650 |
| Sputum smear-positive | 31 (40%) | 20 (61%) | 0.051 |
| Cavitary lesion-positive | 33 (43%) | 14 (42%) | 0.967 |
| Serum chemistry results | |||
| Total protein (g/dL) | 7.4 (7.2–7.8) | 7.6 (7.4–7.9) | 0.133 |
| Albumin (g/dL) | 4.4 (4.3–4.7) | 4.4 (4.2–4.7) | 0.613 |
| Albumin/globulin ratio | 1.5 (1.4–1.7) | 1.5 (1.2–1.6) | 0.463 |
| CRP (mg/dL) | 0.16 (0.06–0.65) | 0.17 (0.07–1.04) | 0.511 |
| Total cholesterol (mg/dL) | 180 (155–201) | 176 (162–192) | 0.858 |
| AST (U/L) | 22 (18–25) | 19 (17–24) | 0.114 |
| ALT (U/L)) | 17 (14–21) | 15 (11–19) | 0.051 |
| ESR (mm) | 37 (22–52) | 49 (26–80) | 0.082 |
| Serum vitamin concentrations | |||
| Vitamin A (µmol/L) | 1.5 (1.2–1.8) | 1.3 (1.2–1.6) | 0.118 |
| Vitamin D (ng/mL) | 20.8 (12.5–29.6) | 16.6 (10.2–29.9) | 0.459 |
| Vitamin E (µmol/L) | 27.1 (23.3–32.6) | 26.3 (21.7–29.4) | 0.252 |
| Homocysteine (µmol/L) | 10.3 (8.4–12.7) | 9.6 (7.8–11.7) | 0.615 |
| Methylmalonic acid (nmol/L) | 173.4 (135.4–244.2) | 167.7 (131.3–223.1) | 0.148 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, J.; Park, H.-D.; Kim, S.-Y.; Koh, W.-J.; Lee, S.-Y. Assessment of Vitamin Status in Patients with Nontuberculous Mycobacterial Pulmonary Disease: Potential Role of Vitamin A as a Risk Factor. Nutrients 2019, 11, 343. https://doi.org/10.3390/nu11020343
Oh J, Park H-D, Kim S-Y, Koh W-J, Lee S-Y. Assessment of Vitamin Status in Patients with Nontuberculous Mycobacterial Pulmonary Disease: Potential Role of Vitamin A as a Risk Factor. Nutrients. 2019; 11(2):343. https://doi.org/10.3390/nu11020343
Chicago/Turabian StyleOh, Jongwon, Hyung-Doo Park, Su-Young Kim, Won-Jung Koh, and Soo-Youn Lee. 2019. "Assessment of Vitamin Status in Patients with Nontuberculous Mycobacterial Pulmonary Disease: Potential Role of Vitamin A as a Risk Factor" Nutrients 11, no. 2: 343. https://doi.org/10.3390/nu11020343