Multi-Micronutrient Fortified Rice Improved Serum Zinc and Folate Concentrations of Cambodian School Children. A Double-Blinded Cluster-Randomized Controlled Trial

 and
and
Abstract
:1. Introduction
2. Materials and Methods
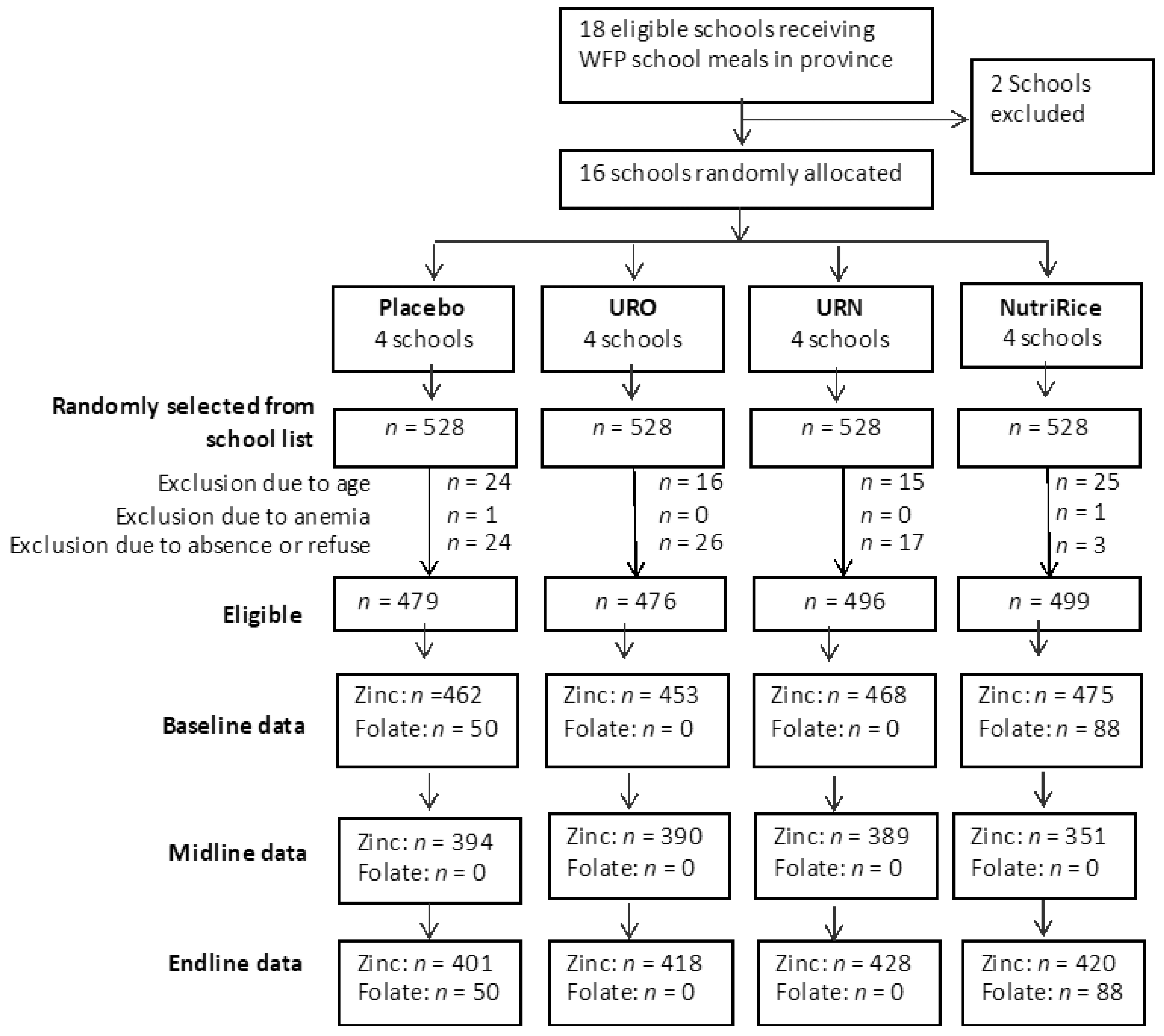
2.1. Study Design and Population
2.2. Intervention
2.3. Food Preparation
2.4. Randomization and Blinding
2.5. Blood Sample and Measurement
2.6. School Attendance
2.7. Estimation of Zinc Intake
2.8. Data Management and Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. School Attendance and Dietary Intake
3.3. Effect of Intervention on Zinc Concentration
3.4. Effect of Intervention on Prevalence of Zinc Deficiency
3.5. Effect of Intervention on Folate Status
4. Discussion
4.1. MMFR Increased Zinc Concentration and Reduced Deficiency
4.2. MMFR Increased Folate Concentration and Reduced Deficiency
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Muthayya, S.; Rah, J.H.; Sugimoto, J.D.; Roos, F.F.; Kraemer, K.; Black, R.E. The global hidden hunger indices and maps: An advocacy tool for action. PLoS ONE 2013, 8. [Google Scholar] [CrossRef]
- International Food Policy Research Institute. Global Nutrition Report 2015: Actions and Accountability to Advance Nutrition and Sustainable Development; International Food Policy Research Institute (IFPRI): Washington, DC, USA, 2015. [Google Scholar]
- Bailey, R.L.; West, K.P., Jr.; Black, R.E. The epidemiology of global micronutrient deficiencies. Ann. Nutr. Metab. 2015, 66, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.J.; Qaim, M. The human and economic cost of hidden hunger. Food Nutr. Bull. 2007, 28, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Moench-Pfanner, R.; Silo, S.; Laillou, A.; Wieringa, F.; Hong, R.; Hong, R.; Poirot, E.; Bagriansky, J. The Economic Burden of Malnutrition in Pregnant Women and Children under 5 Years of Age in Cambodia. Nutrients 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Copenhagen consensus. Expert panel findings of the Copehagen Concensus. In Third Copenhagen Consensus Outcome Document; Copenhagen Consensus Center: Copenhagen, Denmark, 2012. [Google Scholar]
- NIS. Cambodia Demographic and Health Survey (CDHS) 2014; National Institute of Statistic, Ministry of Planning: Phnom Penh, Cambodia, 2015. [Google Scholar]
- Wieringa, F.T.; Dahl, M.; Chamnan, C.; Poirot, E.; Kuong, K.; Sophonneary, P.; Sinuon, M.; Greuffeille, V.; Hong, R.; Berger, J. The high prevalence of anemia in cambodian children and women cannot be satisfactorily explained by nutritional deficiencies or hemoglobin disorders. Nutrients 2016, 8, 348. [Google Scholar] [CrossRef]
- Krebs, N.F.; Miller, L.V.; Michael Hambidge, K. Zinc deficiency in infants and children: A review of its complex and synergistic interactions. Paediatr. Int. Child Health 2014, 34, 279–288. [Google Scholar] [CrossRef]
- Brown, K.H.; Peerson, J.M.; Baker, S.K.; Hess, S.Y. Preventive zinc supplementation among infants, preschoolers, and older prepubertal children. Food Nutr. Bull. 2009, 30, S12–S40. [Google Scholar] [CrossRef]
- Yakoob, M.Y.; Theodoratou, E.; Jabeen, A.; Imdad, A.; Eisele, T.P.; Ferguson, J.; Jhass, A.; Rudan, I.; Campbell, H.; Black, R.E.; et al. Preventive zinc supplementation in developing countries: Impact on mortality and morbidity due to diarrhea, pneumonia and malaria. BMC Public Health 2011, 11, S23. [Google Scholar] [CrossRef]
- Sazawal, S.; Black, R.E.; Menon, V.P.; Dinghra, P.; Caulfield, L.E.; Dhingra, U.; Bagati, A. Zinc supplementation in infants born small for gestational age reduces mortality: A prospective, randomized, controlled trial. PEDIATRICS 2001, 108, 1280–1286. [Google Scholar] [CrossRef]
- Black, M.M. The evidence linking zinc deficiency with children’s cognitive and motor functioning. J. Nutr. 2003, 133, 1473–1476. [Google Scholar] [CrossRef]
- Morris, M.S.; Jacques, P.F.; Rosenberg, I.H.; Selhub, J. Folate and vitamin B-12 status in relation to anemia, macrocytosis, and cognitive impairment in older Americans in the age of folic acid fortification. Am. J. Clin. Nutr. 2007, 85, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Black, M.M. Effects of vitamin B12 and folate deficiency on brain development in children. Food Nutr. Bull. 2008, 29, S126–S131. [Google Scholar] [CrossRef]
- Martí-Carvajal, A.; Peña-Martí, G.; Comunián-Carrasco, G.; Muñoz-Navarro, S.; Luco, M.; Martí-Peña, A.; Medina-Laurentín, C. Prematurity and maternal folate deficiency: Anemia during pregnancy study group results in Valencia, Venezuela. Arch. Latinoam. Nutr. 2004, 54, 45–49. [Google Scholar] [PubMed]
- Best, C.; Neufingerl, N.; Van Geel, L.; van den Briel, T.; Osendarp, S. The nutritional status of school-aged children: Why should we care? Food Nutr. Bull. 2010, 31, 400–417. [Google Scholar] [CrossRef] [PubMed]
- Best, C.; Neufingerl, N.; Del Rosso, J.M.; Transler, C.; van den Briel, T.; Osendarp, S. Can multi-micronutrient food fortification improve the micronutrient status, growth, health, and cognition of schoolchildren? A systematic review. Nutr. Rev. 2011, 69, 186–204. [Google Scholar] [CrossRef]
- Shrestha, R.M. Effect of Iodine and Iron Supplementation on Physical, Psychomotor and Mental Development in Primary School Children in Malawi. Ph.D. Thesis, Wageningen University, Wageningen, The Netherlands, 1994. [Google Scholar]
- De-Regil, L.M.; Pena-Rosas, J.P.; Laillou, A.; Moench-Pfanner, R. Considerations for rice fortification in public health: Conclusions of a technical consultation. Ann. N. Y. Acad. Sci. 2014, 1324, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Piot, P.; Semba, R.D.; Bloem, M.W. Nutrition and Health in Developing Countries; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Perignon, M.; Fiorentino, M.; Kuong, K.; Dijkhuizen, M.A.; Burja, K.; Parker, M.; Chamnan, C.; Berger, J.; Wieringa, F.T. Impact of Multi-Micronutrient Fortified Rice on Hemoglobin, Iron and Vitamin A Status of Cambodian Schoolchildren: A Double-Blind Cluster-Randomized Controlled Trial. Nutrients 2016, 8, 29. [Google Scholar] [CrossRef] [PubMed]
- PATH. Introduction of Fortified Rice Using the Ultra Rice® Technology; PATH: Seatle, DC, USA, 2008. [Google Scholar]
- Brown, K.H.; Rivera, J.; Bhutta, Z.; Gibson, R.; King, J.; Lönnerdal, B.; Ruel, M.; Sandtröm, B.; Wasantwisut, E.; Hotz, C. International Zinc Nutrition Consultative Group (IZiNCG) technical document# 1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr. Bull. 2004, 25, 99–203. [Google Scholar]
- World Health Organization. Serum and Red Blood Cell Folate Concentrations for Assessing Folate Status in Populations; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Pinkaew, S.; Winichagoon, P.; Hurrell, R.F.; Wegmuller, R. Extruded Rice Grains Fortified with Zinc, Iron, and Vitamin A Increase Zinc Status of Thai School Children When Incorporated into a School Lunch Program. J. Nutr. 2013, 143, 362–368. [Google Scholar] [CrossRef]
- Hess, S.Y.; Peerson, J.M.; King, J.C.; Brown, K.H. Use of serum zinc concentration as an indicator of population zinc status. Food Nutr. Bull. 2007, 28, S403–S429. [Google Scholar] [CrossRef]
- Baran, E.; van Zalinge, N.; Bun, N.P. Analysis of the Cambodian Bagnet (“Dai”) Fishery Data; ICLARM: Penang, Malaysia; Mekong River Commission Secretariat and Department of Fisheries: Phnom Penh, Cambodia, 2001. [Google Scholar]
- Ben Sokhean MG-s. Season’s bountiful fish catch means prahok will be plentiful. The Cambodia Daily Newspaper. 20 January 2014. Available online: https://english.cambodiadaily.com/news/seasons-bountiful-fish-catch-means-prahok-will-be-plentiful-50893/ (accessed on 25 September 2019).
- Chamnan, C.; Thilsted, S.H.; Rottana, B.; Sopha, L.; Gerpacio, R.V.; Roos, N. The Role of Fisheries Resources in Rural Cambodia: Combating Micronutrient Deficiencies in Women and Children; Department of Fisheries Post-Harvest Technologies and Quality Control: Phnom Penh, Cambodia, 2009. [Google Scholar]
- Roos, N.; Wahab, M.A.; Chamnan, C.; Thilsted, S.H. The role of fish in food-based strategies to combat vitamin A and mineral deficiencies in developing countries. J. Nutr. 2007, 137, 1106–1109. [Google Scholar] [CrossRef] [PubMed]
- Lutter, C.K.; Rodríguez, A.; Fuenmayor, G.; Avila, L.; Sempertegui, F.; Escobar, J. Growth and micronutrient status in children receiving a fortified complementary food. J. Nutr. 2008, 138, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.H.; Hess, S.Y.; Vosti, S.A.; Baker, S.K. Comparison of the estimated cost-effectiveness of preventive and therapeutic zinc supplementation strategies for reducing child morbidity and mortality in sub-Saharan Africa. Food Nutr. Bull. 2013, 34, 199–214. [Google Scholar] [CrossRef] [PubMed]
- de Romaña, D.L.; Salazar, M.; Hambidge, K.M.; Penny, M.E.; Peerson, J.M.; Krebs, N.F.; Brown, K.H. Longitudinal measurements of zinc absorption in Peruvian children consuming wheat products fortified with iron only or iron and 1 of 2 amounts of zinc. Am. J. Clin. Nutr. 2005, 81, 637–647. [Google Scholar] [CrossRef] [PubMed]
- Lönnerdal, B. Dietary factors influencing zinc absorption. J. Nutr. 2000, 130, 1378S–1383S. [Google Scholar] [CrossRef] [PubMed]
- Aaron, G.J.; Lo, N.B.; Hess, S.Y.; Guiro, A.T.; Wade, S.; Brown, K.H. Plasma Zinc Concentration Increases within 2 Weeks in Healthy Senegalese Men Given Liquid Supplemental Zinc, but Not Zinc-Fortified Wheat Bread. J. Nutr. 2011, 141, 1369–1374. [Google Scholar] [CrossRef]
- Lo, N.B.; Aaron, G.J.; Hess, S.Y.; Dossou, N.I.; Guiro, A.T.; Wade, S.; Brown, K.H. Plasma zinc concentration responds to short-term zinc supplementation, but not zinc fortification, in young children in Senegal. Am. J. Clin. Nutr. 2011, 93, 1348–1355. [Google Scholar] [CrossRef]
- Hess, S.Y.; Brown, K.H. Impact of zinc fortification on zinc nutrition. Food. Nutr. Bull. 2009, 30, S79–S107. [Google Scholar] [CrossRef]
- Gibson, R.S.; Bailey, K.B.; Gibbs, M.; Ferguson, E.L. A review of phytate, iron, zinc, and calcium concentrations in plant-based complementary foods used in low-income countries and implications for bioavailability. Food. Nutr. Bull. 2010, 31, S134–S146. [Google Scholar] [CrossRef]
- Adams, C.L.; Hambidge, M.; Raboy, V.; Dorsch, J.A.; Sian, L.; Westcott, J.L.; Krebs, N.F. Zinc absorption from a low–phytic acid maize. Am. J. Clin. Nutr. 2002, 76, 556–559. [Google Scholar] [CrossRef]
- Roos, N.; Sørensen, J.C.; Sørensen, H.; Rasmussen, S.K.; Briend, A.; Yang, Z.; Huffman, S.L. Screening for anti-nutritional compounds in complementary foods and food aid products for infants and young children. Matern. Child Nutr. 2013, 9, 47–71. [Google Scholar] [CrossRef] [PubMed]
- Faber, M.; Kvalsvig, J.D.; Lombard, C.J.; Benadé, A.S. Effect of a fortified maize-meal porridge on anemia, micronutrient status, and motor development of infants. Am. J. Clin. Nutr. 2005, 82, 1032–1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, M.; Samman, S.; Madsen, L.T.; Jensen, M.; Sørensen, S.S.; Sandström, B. Folic acid enrichment of bread does not appear to affect zinc absorption in young women. Am. J. Clin. Nutr. 2001, 74, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Winichagoon, P.; McKenzie, J.E.; Chavasit, V.; Pongcharoen, T.; Gowachirapant, S.; Boonpraderm, A.; Manger, M.S.; Bailey, K.B.; Wasantwisut, E.; Gibson, R.S. A multimicronutrient-fortified seasoning powder enhances the hemoglobin, zinc, and iodine status of primary school children in North East Thailand: A randomized controlled trial of efficacy. J. Nutr. 2006, 136, 1617–1623. [Google Scholar] [CrossRef] [Green Version]
- Nga, T.T.; Winichagoon, P.; Dijkhuizen, M.A.; Khan, N.C.; Wasantwisut, E.; Furr, H.; Wieringa, F.T. Multi-micronutrient–fortified biscuits decreased prevalence of anemia and improved micronutrient status and effectiveness of deworming in rural Vietnamese school children. J. Nutr. 2009, 139, 1013–1021. [Google Scholar] [CrossRef]
- Jansen, E.H.; Beekhof, P.K.; Cremers, J.W.; Schenk, E. Long-term (in) stability of folate and vitamin B12 in human serum. Clin. Chem. Lab. Med. 2012, 50, 1761–1763. [Google Scholar] [CrossRef]
- Jacques, P.F.; Selhub, J.; Bostom, A.G.; Wilson, P.W.; Rosenberg, I.H. The effect of folic acid fortification on plasma folate and total homocysteine concentrations. N. Eng. J. Med. 1999, 340, 1449–1454. [Google Scholar] [CrossRef]
- Choumenkovitch, S.F.; Selhub, J.; Wilson, P.W.; Rader, J.I.; Rosenberg, I.H.; Jacques, P.F. Folic acid intake from fortification in United States exceeds predictions. J. Nutr. 2002, 132, 2792–2798. [Google Scholar] [CrossRef]
- Cuskelly, G.J.; McNulty, H.; Scott, J.M. Fortification with Low Amounts of Folic Acid Makes a Significant Difference in Folate Status in Young Women: Implications for the Prevention of Neural Tube Defects. Am. J. Clin. Nutr. 2000, 55, 74. [Google Scholar] [CrossRef]
- Pfeiffer, C.M.; Rogers, L.M.; Bailey, L.B.; Gregory, J. Absorption of folate from fortified cereal-grain products and of supplemental folate consumed with or without food determined by using a dual-label stable-isotope protocol. Am. J. Clin. Nutr. 1997, 66, 1388–1397. [Google Scholar] [CrossRef] [Green Version]
- Bar-Oz, B.; Koren, G.; Nguyen, P.; Kapur, B.M. Folate fortification and supplementation—are we there yet? Reprod. Toxicol. 2008, 25, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Wieringa, F.T.; Laillou, A.; Guyondet, C.; Jallier, V.; Moench-Pfanner, R.; Berger, J. Stability and retention of micronutrients in fortified rice prepared using different cooking methods. Ann. N. Y. Acad. Sci. 2014, 1324, 40–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Micronutrients | Normal Rice 1 | URO | URN | NutriRice | Target Value |
|---|---|---|---|---|---|
| Iron (mg) | 0.3 | 10.67 | 7.55 | 7.46 | 7.26 |
| Zinc (mg) | 1.0 | 3.04 | 2.02 | 3.68 | 3.50 |
| Vitamin B1 (mg) | ND | 1.06 | 1.43 | 0.69 | 0.60 |
| Folic Acid (mg) | ND | 0.17 | 0.28 | 0.14 | 0.20 |
| Vitamin A (mg) | 0.03 | - | 0.64 | 0.29 | 0.30 |
| Vitamin B3 (mg) | ND | - | 12.57 | 7.98 | 8.00 |
| Vitamin B12 (μg) | 0.4 | - | 3.8 | 1.3 | 1.2 |
| Vitamin B6 (mg) | 0.1 | - | - | 0.92 | 0.65 |
| Outcomes | Placebo | URO | URN | NutriRice |
|---|---|---|---|---|
| n | 462 | 453 | 468 | 475 |
| Age (y) | 9.62 ± 2.29 | 9.63 ± 2.18 | 9.61 ± 2.20 | 9.73 ± 2.42 |
| % girls | 50.2 (n = 232) | 49.4 (n = 224) | 50.0 (n = 234) | 49.9 (n = 237) |
| % inflammations | 42.9 (n = 195) | 42.4 (n = 191) | 32.5 (n = 151) | 32.2 (n = 150) |
| % parasite infection | 22.9 (n = 78) | 25.8 (n = 90) | 19.8 (n = 70) | 12.9 (n = 39) |
| % Hemoglobinopathy (Hb E ≥5%) | 41.8 (n = 193) | 43.9 (n = 199) | 43.4 (n = 203) | 41.7 (n = 198) |
| Anthropometric status | ||||
| Underweight (WAZ ≤2) (only for <10 years) | 43.1% (n = 109) | 40.1% (n = 108) | 49.6% (n = 135) | 40.1% (n = 107) |
| Stunted (HAZ ≤2) | 43.8% (n = 202) | 39.6% (n = 179) | 44.5% (n = 208) | 45.5% (n = 214) |
| Wasted (BAZ ≤2) | 25.4% (n = 117) | 27.0% (n = 122) | 29.8% (n = 139) | 21.5% (n = 101) |
| Micronutrient status | ||||
| Hb (g/L) | 123.5 ± 10.2 | 124.2 ± 9.8 | 123.7 ± 9.2 | 123.9 ± 10.4 |
| % anemia | 18.7 (n = 86) | 15.3 (n = 69) | 17.5 (n = 82) | 17.2 (n = 81) |
| ID total | 55.2 (n = 251) | 56.8 (n = 256) | 48.6 (n = 226) | 49.0 (n = 229) |
| ID with anemia | 11.9 (n = 54) | 10.2 (n = 46) | 10.5 (n = 49) | 10.3 (n = 48) |
| Body Iron (mg/kg) | 6.49 ± 2.0 | 6.53 ± 2.2 | 6.16 ± 2.4 | 6.16 ± 2.4 |
| % 0 < BI < 4 mg/kg | 9.0 (n = 41) | 10.9 (n = 49) | 11.6 (n = 54) | 13.3 (n = 62) |
| % BI < 0 mg/kg | 1.3 (n = 6) | 1.3 (n = 6) | 3.0 (n = 14) | 2.6 (n = 12) |
| RBP (µmol/L) | 1.62 ± 0.43 | 1.68 ± 0.43 | 1.48 ± 0.43 | 1.51 ± 0.43 |
| % marginal VA status | 7.5 (n = 34) | 3.8 (n = 17) | 13.8 (n = 64) | 12.4 (n = 58) |
| % VAD | 0.7 (n = 3) | 0.2 (n = 1) | 1.3 (n = 6) | 1.1 (n = 5) |
| Serum Zinc (µmol/L) | 7.7 ± 1.86 | 7.74 ± 1.69 | 7.61 ± 1.70 | 8.11 ± 1.88 |
| % zinc deficiency | 89.4 (n = 413) | 90.1 (n = 408) | 92.3 (n = 432) | 83.6 (n = 397) |
| % Severe zinc deficiency (<7.6 µmol/L) | 49.8 (n = 230) | 49.7 (n = 225) | 53.8 (n = 252) | 43.6 (n = 207) |
| Serum Folate (ng/mL) | 5.40 ± 1.60 | N/A | N/A | 6.25 ± 2.06 |
| % Folate deficiency (<4 ng/mL) | 18.0 (n = 9 out of 50) | N/A | N/A | 9.1 (n = 8 out of 88) |
| Variables | Placebo | URO | URN | NutriRice |
|---|---|---|---|---|
| Attendance | ||||
| n | 462 | 453 | 468 | 475 |
| Number of school days over the whole study period | 127 | 126 | 126 | 132 |
| % of attendance over the study period | 86.6% | 82.0% | 83.6% | 84.1% |
| Number school days in the BL–ML period | 75 | 81 | 82 | 86 |
| % attendance over the BL–ML period | 88.5% | 85.0% | 87.7% | 87.2% |
| Number of school days in the ML–EL period | 68 | 61 | 62 | 52 |
| % attendance over the ML–EL period | 87.6% | 88.4% | 87.7% | 86.5% |
| % attendance within 10 days before ML | 89.9% | 87.7% | 88.4% | 87.0% |
| % attendance within 10 days before EL | 86.3% | 86.5% | 87.8% | 85.7% |
| Zinc intake | ||||
| Zinc in fortified rice, mg/100g | - | 3.0 | 2.0 | 3.7 |
| Estimated zinc intake at school meal (%RDA)* | - | 3.5 (44%) | 2.3 (29%) | 4.2 (53%) |
| Estimated zinc intake per child from BL–EL, mg | - | 441.0 | 292.3 | 558.4 |
| Estimated zinc intake per child from BL–ML, mg | - | 283.5 | 190.2 | 363.8 |
| Estimated zinc intake per child from ML–EL, mg | - | 213.5 | 143.8 | 219.9 |
| Molar ratio | ||||
| Phytate content, mg/100g of cooked rice | 108.9 | 108.9 | 108.9 | 108.9 |
| Phytate:zinc molar ratio | - | 3.55 | 5.34 | 2.93 |
| Intake of folic Acid | ||||
| N | 50 | 88 | ||
| Folic acid in fortified rice, mg/100g | - | 0.17 | 0.28 | 0.14 |
| Estimated folic acid intake per meal (% RDA)* | - | 0.2 (50%) | 0.32 (80%) | 0.16 (40%) |
| Estimated folic acid intake per child from BL-EL, mg | - | 25.4 | 35.3 | 21.1 |
| Time Point | Group | n | Mean (μmol/L) | SE | Estimated Effect Coefficient 1 (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Baseline | Placebo | 462 | 7.83 | 0.08 | - | |
| URO | 453 | 7.83 | 0.08 | - | ||
| URN | 468 | 7.67 | 0.08 | - | ||
| NutriRice | 475 | 8.15 | 0.08 | - | ||
| Midline | Placebo | 393 | 9.71 | 0.09 | - | |
| URO | 389 | 8.69 | 0.09 | −1.02 (−1.43; −0.61) | <0.001 | |
| URN | 389 | 9.72 | 0.09 | −0.17 (−0.24; 0.58) | 0.422 | |
| NutriRice | 351 | 9.54 | 1.00 | −0.50 (−0.93; 0.07) | 0.024 | |
| Endline | Placebo | 401 | 7.57 | 0.09 | - | |
| URO | 418 | 8.56 | 0.09 | 0.98 (0.58; 1.38) | <0.001 | |
| URN | 428 | 8.27 | 0.09 | 0.85 (0.45; 1.25) | <0.001 | |
| NutriRice | 420 | 9.29 | 0.09 | 1.40 (0.98; 1.82) | <0.001 |
| Zinc Deficiency | Severe Zinc Deficiency | |||||||
|---|---|---|---|---|---|---|---|---|
| (<9.9 µmol/L) | (<7.6 µmol/L) | |||||||
| Time Point Group | n | Estimated Effect | Estimated Effect | |||||
| % | Adjusted OR1 | p-Value | % | Adjusted OR1 | p-Value | |||
| (95% CI) | (95% CI) | |||||||
| Placebo | 462 | 89.4 | - | 49.8 | - | |||
| URO | 453 | 90.1 | - | 49.7 | - | |||
| Baseline | URN | 468 | 92.3 | - | 53.8 | - | ||
| NutriRice | 475 | 83.6 | - | 43.6 | - | |||
| Placebo | 393 | 60.6 | - | 15.5 | - | |||
| URO | 389 | 79.2 | 2.25(1.23;4.10) | 0.08 | 22.4 | 1.56(0.93;2.62) | 0.09 | |
| Midline | URN | 389 | 55.8 | 0.05(0.30;1.02) | 0.059 | 15.4 | 0.79(0.46;1.37) | 0.4 |
| NutriRice | 351 | 60.1 | 1.25(0.69;2.26) | 0.461 | 17.7 | 1.36(0.76;2.42) | 0.29 | |
| Placebo | 401 | 93.3 | - | 53.6 | - | |||
| URO | 418 | 80.6 | 0.25(0.12;0.52) | <0.001 | 29.7 | 0.35(0.22;0.55) | <0.001 | |
| Endline | URN | 428 | 83.4 | 0.25(0.11;0.53) | <0.001 | 37.1 | 0.39(0.25;0.60) | <0.001 |
| NutriRice | 420 | 65.7 | 0.16(0.08;0.34) | <0.001 | 25.7 | 0.28(0.17;0.47) | <0.001 | |
| Biochemical Indicator | Placebo | Nutririce |
|---|---|---|
| Serum Concentration | ||
| n | 50 | 88 |
| Baseline (± SD), ng/mL | 5.40 ± 1.60 | 6.25 ± 2.06 |
| Endline (± SD), ng/mL | 7.13 ± 1.70 | 9.54 ± 2.76 |
| Coefficient 1 (95% CI) | - | 2.25 * (0.63; 3.87) |
| Deficiency Prevalence | ||
| n | 50 | 88 |
| Baseline (%) | 18.0% | 9.1% |
| Endline (%) | 2.0% | 0% |
| Adjusted OR 1 (95% CI) | - | 1.59 (0.11; 23.47) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuong, K.; Tor, P.; Perignon, M.; Fiorentino, M.; Chamnan, C.; Berger, J.; Burja, K.; Dijkhuizen, M.A.; Parker, M.; Roos, N.; et al. Multi-Micronutrient Fortified Rice Improved Serum Zinc and Folate Concentrations of Cambodian School Children. A Double-Blinded Cluster-Randomized Controlled Trial. Nutrients 2019, 11, 2843. https://doi.org/10.3390/nu11122843
Kuong K, Tor P, Perignon M, Fiorentino M, Chamnan C, Berger J, Burja K, Dijkhuizen MA, Parker M, Roos N, et al. Multi-Micronutrient Fortified Rice Improved Serum Zinc and Folate Concentrations of Cambodian School Children. A Double-Blinded Cluster-Randomized Controlled Trial. Nutrients. 2019; 11(12):2843. https://doi.org/10.3390/nu11122843
Chicago/Turabian StyleKuong, Khov, Pety Tor, Marlene Perignon, Marion Fiorentino, Chhoun Chamnan, Jacques Berger, Kurt Burja, Marjoleine A. Dijkhuizen, Megan Parker, Nanna Roos, and et al. 2019. "Multi-Micronutrient Fortified Rice Improved Serum Zinc and Folate Concentrations of Cambodian School Children. A Double-Blinded Cluster-Randomized Controlled Trial" Nutrients 11, no. 12: 2843. https://doi.org/10.3390/nu11122843