1. Introduction
The prevalence of gout, a disease of urate crystal deposition characterized by symptomatic hyperuricemia, has been increasing globally [
1,
2,
3,
4]. Gout is associated with an impaired quality of life [
5,
6,
7] because patients present with a variety of clinical symptoms including urinary stones, acute arthritis, chronic kidney disease and metabolic syndrome [
8]. The progression of gout is suggested to result from an imbalance between uric acid synthesis and excretion. The most important factor considered to increase the risk of gout is hyperuricemia with persistently high serum uric acid levels. [
9]. In particular, hyperuricemia has been suggested to be caused primarily by weakened kidney excretion of uric acid [
10].
Glycine, a non-essential amino acid, was revealed to enhance the urinary excretion of uric acid in healthy subjects as well as in patients with gout in previous studies [
11,
12,
13]. Although these reports suggested that serum uric acid levels in hyperuricemia could be managed with continual glycine administration, our preliminary studies hinted that higher glycine levels were needed for effective dosing. Therefore, this study aimed to identify other amino acids that might augment the effects of glycine on serum uric acid levels. In our preliminary studies in healthy individuals, transient declines of serum uric acid levels following the oral administration of glycine together with tryptophan were observed. The uric acid-lowering effects of tryptophan, an essential amino acid, are not well known. Therefore, the authors subsequently conducted a clinical trial to confirm the serum uric acid-lowering effects of continual combined supplementation with glycine and tryptophan under mild hyperuricemia. The results revealed that combined treatment with 3.0 g of glycine and 0.2 g of tryptophan daily for 6 weeks significantly decreased serum uric acid concentrations in subjects with mild hyperuricemia [
14]. The mixture of amino acids enhanced urate clearance, except in subjects with abnormally high urate clearance. The current study examined whether the combined administration of 6.0 g of glycine and 0.4 g of tryptophan suppressed the elevation in serum uric acid levels induced by purine ingestion and increased urinary uric acid excretion.
3. Results
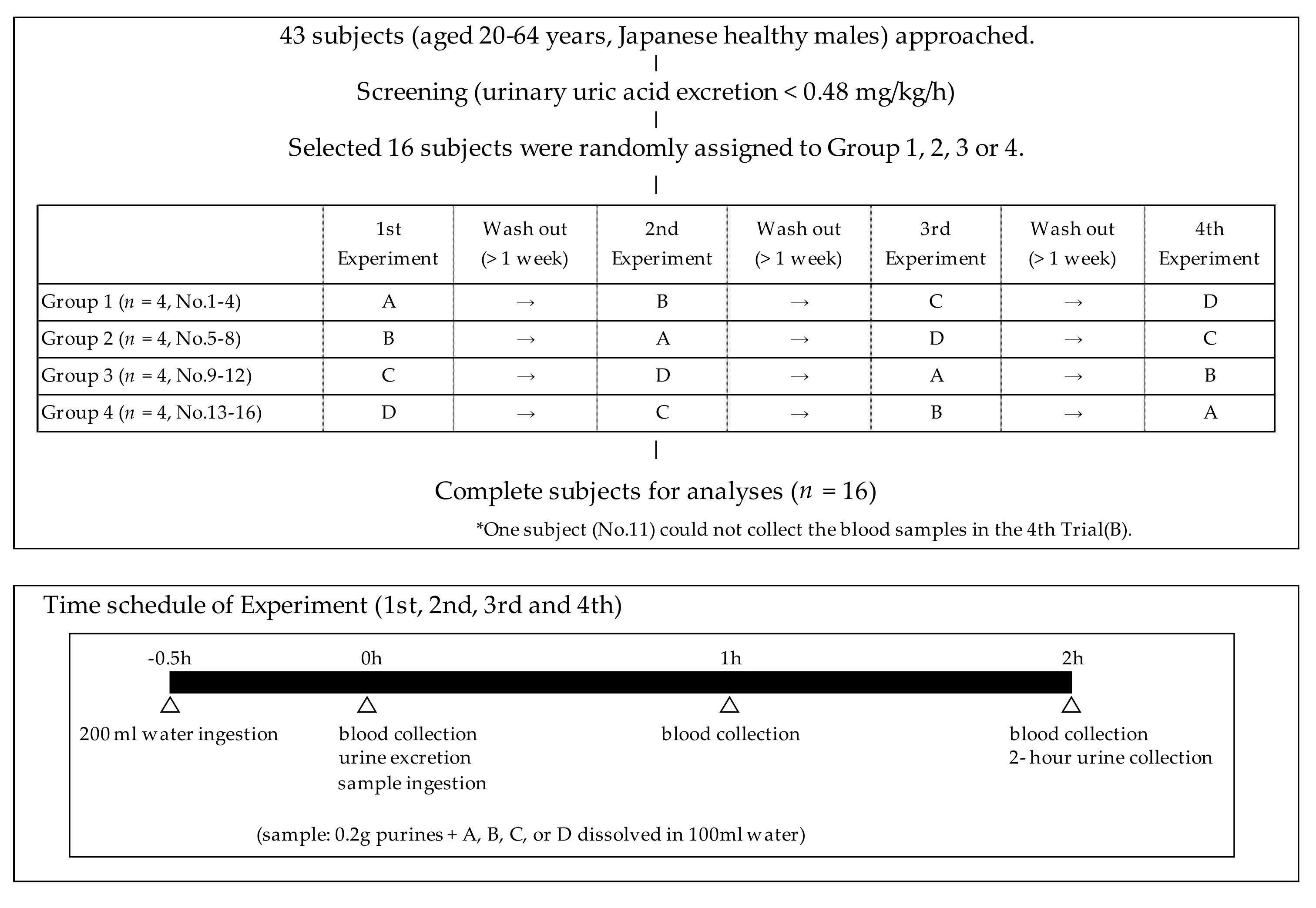
The characteristics of the subjects are shown in
Table 2. The final analyses were performed using the data from 16 healthy male subjects aged 38.3 ± 9.2 years with lower urinary uric acid excretion levels (<0.48 mg/kg/h). The average serum uric acid concentration of the 16 subjects was 6.7 ± 0.9 mg/dL. The blood samples during the fourth experiment of the crossover trial could not be collected from one subject (No. 11) who was assigned to group 3. Therefore, all serum parameters of group 3 were analyzed with
n = 15.
The transient changes in the serum uric acid concentrations induced by purine ingestion are summarized in
Table 3. Briefly, the serum uric acid levels were significantly higher at 1 h after ingestion than at the baseline (0 h) in all groups and the serum uric acid levels remained significantly higher at 2 h versus the baseline in the placebo and tryptophan groups. Conversely, the serum uric acid levels at 2 h were comparable to the baseline levels in the glycine and glycine + tryptophan groups. The change in the serum uric acid levels from the baseline at 1 h in the glycine + tryptophan group (0.15 ± 0.15 mg/dL) was significantly smaller than in the placebo group (0.30 ± 0.17 mg/dL,
p = 0.020). However, the change in the serum uric acid levels at 1 h was not significantly lower in the glycine (0.19 ± 0.11 mg/dL) or tryptophan groups (0.26 ± 0.13 mg/dL) than in the placebo group. The change in serum uric acid levels at 2 h versus the baseline was significantly smaller in both the glycine (0.05 ± 0.14 mg/dL) and glycine + tryptophan groups (0.01 ± 0.21 mg/dL) than in the placebo group (0.23 ± 0.11 mg/dL,
p = 0.017 and 0.002, respectively). There was no difference in the serum uric acid levels between the tryptophan group and the other three groups. Moreover, an additional analysis was conducted in which one subject whose average serum uric acids levels exceeded 8.0 mg/dL was excluded because only patients with serum uric acid levels lower than 8.0 mg/dL should be treated with uric acid-lowering drugs according to diagnostic criteria of hyperuricemia [
8]. Consequently, the change in the serum uric acid levels from the baseline to 1 h was significantly smaller in the glycine + tryptophan group (0.14 ± 0.15 mg/dL) than in the placebo group (0.28 ± 0.16 mg/dL,
p = 0.034). The change in the serum uric acid levels at 2 h from the baseline was significantly smaller in both the glycine (0.03 ± 0.13 mg/dL) and glycine + tryptophan groups (0.02 ± 0.21 mg/dL) than in the placebo group (0.22 ± 0.11 mg/dL,
p = 0.010 and 0.005, respectively).
The data on 2-h urinary uric acid excretion, creatinine excretion, urate clearance, creatinine clearance, and urinary pH are presented in
Table 4. Briefly, urinary uric acid excretion and urate clearance were significantly higher in the glycine (0.596 ± 0.129 mg/kg/h and 9.9 ± 2.6 mL/min, respectively) and glycine + tryptophan groups (0.653 ± 0.153 mg/kg/h and 11.0 ± 2.5 mL/min, respectively) than in the placebo (0.441 ± 0.079 mg/kg/h and 7.5 ± 1.5 mL/min, respectively) and tryptophan groups (0.453 ± 0.092 mg/kg/h and 7.7 ± 1.9 mL/min, respectively). Conversely, urinary uric acid excretion and urate clearance were not significantly different between the placebo and tryptophan groups. Urinary excretion and creatinine clearance were significantly higher in the glycine group (1.43 ± 0.33 mg/kg/h and 187 ± 39 mL/min, respectively) than in the placebo (1.15 ± 0.19 mg/kg/h and 150 ± 15 mL/min, respectively) and glycine + tryptophan groups (1.16 ± 0.26 mg/kg/h and 156 ± 29 mL/min, respectively), but not the tryptophan group (1.26 ± 0.22 mg/kg/h and 176 ± 41 mL/min, respectively). The urinary excretion of uric acid per creatinine (uric acid/creatinine) was higher in the glycine + tryptophan group (0.58 ± 0.16 mg/mg) than in the other three groups (0.40 ± 0.11 mg/mg in the placebo group, 0.37 ± 0.10 mg/mg in the tryptophan group, and 0.44 ± 0.13 mg/mg in the glycine groups). Urinary pH was higher in the glycine + tryptophan group (6.83 ± 0.35) than in the placebo (6.22 ± 0.44) and tryptophan groups (6.23 ± 0.55). Although urinary pH was higher in the glycine group (6.54 ± 0.64) than in the placebo, this difference was not statistically significant. Finally, urinary pH was comparable between the tryptophan and placebo groups.
The serum glycine, tryptophan, and creatinine concentrations as well as the urinary excretion of glycine and tryptophan for each group are summarized in
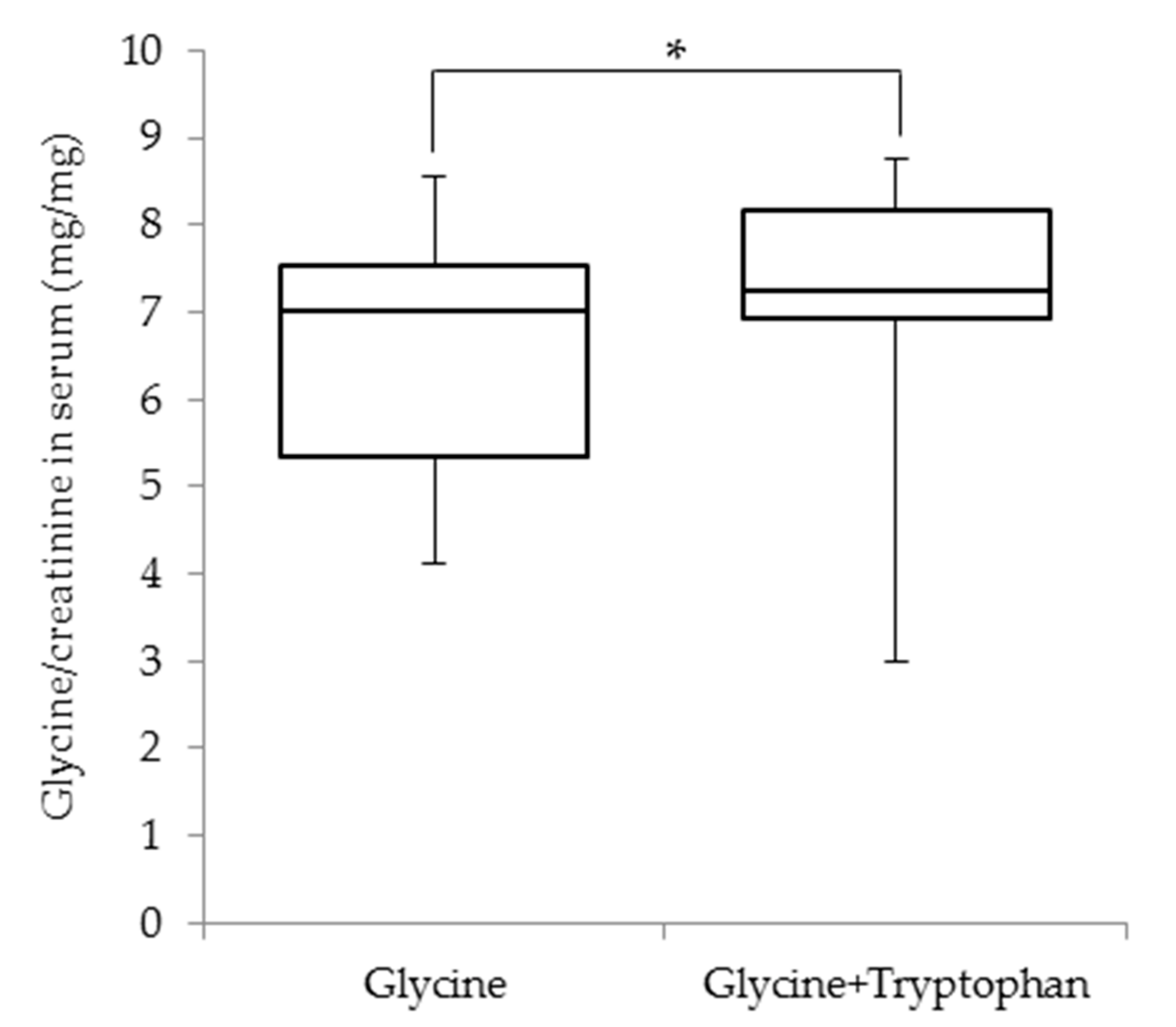
Table 5. Briefly, the serum glycine concentrations following the test drink ingestion peaked 1 h after ingestion and the serum glycine concentrations were significantly higher at 1 and 2 h than those before ingestion in the glycine (5.7 ± 1.4 and 2.6 ± 0.4 mg/dL, respectively, versus 1.3 ± 0.2 mg/dL) and glycine + tryptophan groups (6.0 ± 1.6 and 2.6 ± 0.5 mg/dL, respectively, versus 1.3 ± 0.2 mg/dL) groups. The serum glycine concentrations did not change following the test drink ingestion in the placebo and tryptophan groups. Conversely, there was a significant increase in serum tryptophan concentrations in the tryptophan and glycine + tryptophan groups, both of which received tryptophan. Conversely, the serum creatinine levels at 2 h in the placebo group (0.85 ± 0.09 mg/dL) and at 1 and 2 h in the tryptophan (0.81 ± 0.10 and 0.83 ± 0.10 mg/dL, respectively) and glycine + tryptophan groups (0.83 ± 0.11 and 0.84 ± 0.11 mg/dL, respectively) were significant lower than those before ingestion (0.89 ± 0.11, 0.88 ± 0.10, and 0.88 ± 0.11 mg/dL in the placebo, tryptophan, and glycine + tryptophan groups, respectively). However, the serum creatinine levels did not exhibit temporal changes in the glycine group (0.88 ± 0.10, 0.87 ± 0.10, and 0.86 ± 0.10 mg/dL at 0, 1, and 2 h, respectively). Additionally, the serum glycine/creatinine ratio was significantly higher in the glycine + tryptophan group (7.3 ± 1.2 mg/mg) than in the glycine group (7.0 ± 2.2 mg/mg) at 1 h after ingestion (
Figure 2). The urinary glycine excretion levels in the glycine (0.37 ± 0.23 mg/kg/h) and glycine + tryptophan (0.49 ± 0.35 mg/kg/h) groups significantly increased compared with those in the placebo (0.04 ± 0.02 mg/kg/h) and tryptophan groups (0.04 ± 0.02 mg/kg/h). Moreover, the urinary tryptophan excretion in the tryptophan (0.014 ± 0.006 mg/kg/h) and glycine + tryptophan (0.015 ± 0.005 mg/kg/h) groups significantly increased compared with those in the placebo (0.007 ± 0.003 mg/kg/h) and tryptophan groups (0.007 ± 0.003 mg/kg/h).
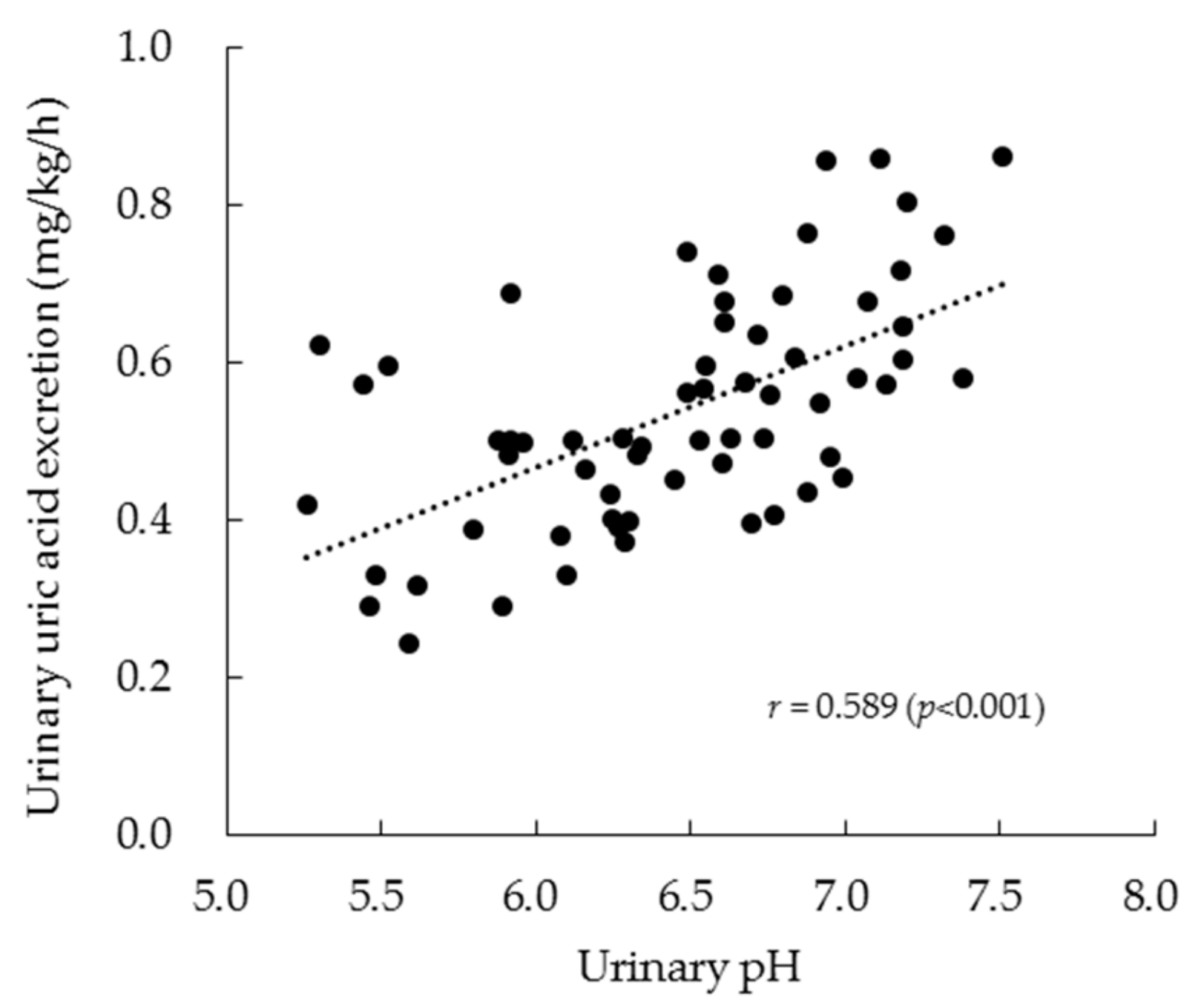
The relationship between urinary pH and urinary uric acid excretion is shown in
Figure 3. The two parameters exhibited a significant positive relationship (
r = 0.589,
p < 0.001) based on the analysis of all data points across the four experiments. Moreover, the relationships of serum glycine and tryptophan concentrations with urinary pH and uric acid excretion were examined (
Table 6). Briefly, the serum glycine levels at 1 and 2 h following ingestion of the test drinks exhibited a significant relationship with both urinary uric acid excretion and urinary pH. However, the serum tryptophan levels did not exhibit a significant relationship with either parameter.
4. Discussion
This study examined whether the combined administration of 6.0 g of glycine and 0.4 g of tryptophan suppressed the elevation in serum uric acid levels induced by purine ingestion and increased urinary uric acid excretion. The amino acid doses used for single ingestion were based on those used in continual supplementation [
14]. Both glycine and tryptophan are present in dietary proteins that are ingested in normal daily living. However, glycine at doses of up to 90 g per day administered over several weeks were reported no serious adverse effects [
18]. The oral administration of up to 5.0 g of
l-tryptophan per day did not lead to any adverse effects in young adult females [
19]. Therefore, no adverse effects were attributed to the combined administration of glycine and tryptophan in the current trial. This study confirmed the safety of combined glycine and tryptophan supplementation.
The current study demonstrated that the combined administration of glycine and tryptophan significantly suppressed the elevation in the serum uric acid levels caused by purine ingestion in healthy subjects. The effect of the combined amino acid administration was stronger than that of the same glycine dose alone, indicating that a small amount of tryptophan provides an additional benefit to glycine alone in reducing the elevation in the serum uric acid levels after the ingestion of dietary purines.
In agreement with previous reports [
11,
12], glycine increased urinary uric acid excretion and enhanced urate clearance in the current study. The authors previously reported that continual supplementation with glycine and tryptophan led to an increase in urinary pH [
14]. Glycine exhibits a buffering action and it is often used as an antacid. The water solubility of uric acid increases with increasing pH levels [
20] and uric acid excretion is more favorable in alkaline urine than in acidic urine [
21]. Therefore, it is possible that the elevation in urinary pH caused by glycine and tryptophan supplementation enhanced the solubility of urinary uric acid, thereby elevating urinary uric acid excretion and urate clearance. Previous studies provide physiological, physicochemical and clinical validation for the use of citrate salt in the treatment of some types of lithiasis [
22,
23]. Citrate salts treatment substantially increased urinary pH in patients with uric acid lithiasis, however, there was no significant change in the amount of urinary uric acid [
24]. The mixture of amino acids might be superior to citrate salts in the prevention or treatment of hyperuricemia. Herein, although the elevation of urinary pH induced by the ingestion of glycine alone was not significant compared with the effects of placebo, glycine administration enhanced uric acid excretion and urate clearance, raising the possibility of other mechanisms. Urate transporter 1 (URAT1), a primary reabsorptive urate transporter that is targeted by pyrazinamide [
25], reportedly disables glycine-induced uricosuria [
26]. Pyrazinamide may reflect the enhanced urate reabsorption following the exchange of its active metabolite [
27]. Thus, glycine may inhibit the reabsorptive action of uric acid, which is induced by URAT1. Further studies are needed to elucidate the action of glycine on URAT1.
In the current study, the supplementation with tryptophan alone had no influence on urinary pH, urinary uric acid excretion or urate clearance. As the effect of tryptophan on URAT1 might be structurally difficult, tryptophan might have exerted an indirect action against uric acid elevation via its influence on the action of glycine. Specifically, tryptophan might promote the direct action of glycine against uric acid elevation. The maximum serum levels of glycine and tryptophan are achieved within an hour of ingestion, which is followed by rapid decreases as the amino acids are metabolized. Glycine metabolizes various end-products, namely glutathione, nucleic acid bases, heme, creatine and bile acids [
28]. The increases in urinary creatinine excretion and creatinine clearance following the glycine challenge suggest that glycine might be partially absorbed back and metabolized to creatinine through creatine. Conversely, these urinary parameters did not change in response to the simultaneous supplementation with glycine and tryptophan, suggesting the suppression of the conversion of glycine to creatinine by tryptophan. In fact, the increases in the serum glycine/creatinine ratio and urinary glycine excretion were more pronounced in response to supplementation with glycine and tryptophan than with glycine alone. Further studies are required to clarify the mechanism underlying the contribution of tryptophan to the effects of glycine on uric acid excretion.
Among the limitations in the current clinical study, the modest sample size (n = 16) might have reduced the statistical power and increased the risk of type II error, particularly regarding the statistical differences in multiple comparisons between the glycine and glycine + tryptophan groups. Furthermore, the current study included only male subjects because of the known effects of sex differences on serum uric acid levels. Further studies are therefore needed, although our preliminary findings suggested that there were no effective differences between males and females in response to glycine and tryptophan supplementation (data not shown).





{kind=link}
{kind=link}
{kind=link}