Dietary Patterns and Poor Semen Quality Risk in Men: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
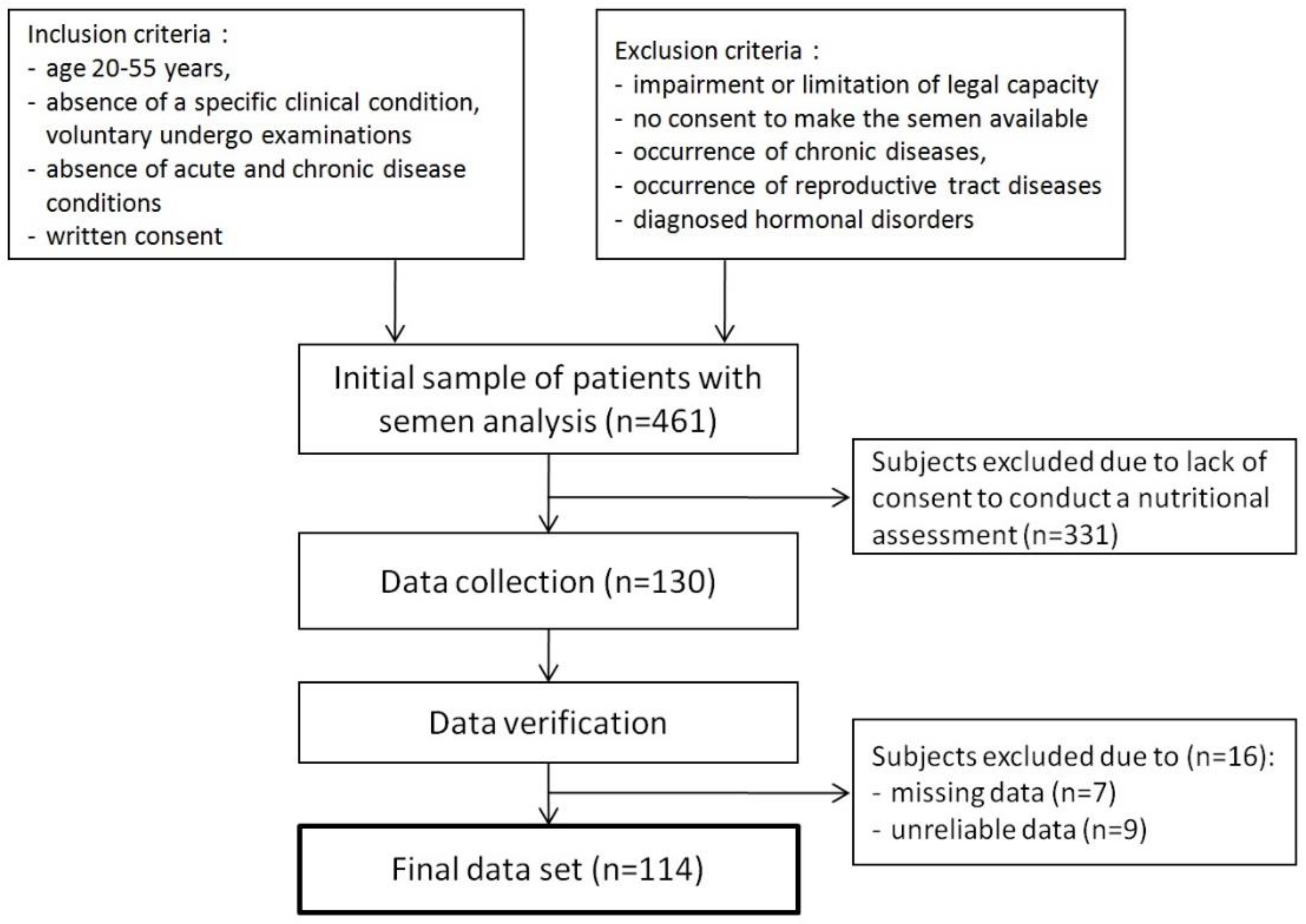
2.1. Participants
2.2. Dietary Data Collection
2.3. Semen Analysis
2.4. Other Measurements
2.5. Statistical Analysis
3. Results
3.1. Dietary Patterns
3.2. Population Characteristics
3.3. Dietary Patterns and the Risk of Abnormal Semen Quality Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Zegers-Hochschild, F.; Adamson, G.D.; de Mouzon, J.; Ishihara, O.; Mansour, R.; Nygren, K.; Sullivan, E.; Vanderpoel, S.; International Committee for Monitoring Assisted Reproductive Technology; World Health Organization. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil. Steril. 2009, 92, 1520–1524. [Google Scholar] [PubMed]
- Agarwal, A.; Mulgund, A.; Hamada, A.; Chyatte, M.R. A unique view on male infertility around the Globe. Reprod. Biol. Endocrinol. 2015, 26, 13–37. [Google Scholar] [CrossRef] [PubMed]
- Bablok, L.; Dziadecki, W.; Szymusik, I.; Wolczynski, S.; Kurzawa, R.; Pawelczyk, L.; Jedrzejczak, P.; Hanke, W.; Kaminski, P.; Wielgos, M. Patterns of infertility in Poland—Multicenter study. Neuro Endocrinol. Lett. 2011, 32, 799–804. [Google Scholar] [PubMed]
- Salas-Huetos, A.; Bulló, M.; Salas-Salvadó, J. Dietary patterns, foods and nutrients in male fertility parameters and fecundability: A systematic review of observational studies. Hum. Reprod. Update 2017, 23, 371–389. [Google Scholar] [CrossRef] [PubMed]
- Gaskins, A.J.; Afeiche, M.C.; Hauser, R.; Williams, P.L.; Gillman, M.W.; Tanrikut, C.; Petrozza, J.C.; Chavarro, J.E. Paternal physical and sedentary activities in relation to semen quality and reproductive outcomes among couples from a fertility center. Hum. Reprod. 2014, 29, 2575–2582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Mendiola, J.; Torres-Cantero, A.M.; Vioque, J.; Moreno-Grau, J.M.; Ten, J.; Roca, M.; Moreno-Grau, S.; Bernabeu, R. A low intake of antioxidant nutrients is associated with poor semen quality in patients attending fertility clinics. Fertil. Steril. 2010, 93, 1128–1133. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.; Chiu, Y.H.; Afeiche, M.C.; Williams, P.L.; Ford, J.B.; Tanrikut, C.; Souter, I.; Hauser, R.; Chavarro, J.E.; EARTH Study Team. Impact of men’s dairy intake on assisted reproductive technology outcomes among couples attending a fertility clinic. Andrology 2016, 4, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Schowell, M.G.; Mackenzie-Proctor, R.; Brown, J.; Yazdani, A.; Stankiewicz, M.T.; Kart, R.J. Antioxidants for mate subfertility. Cochrane Database Syst. Rev. 2014, 12, CD007411. [Google Scholar]
- Eslamian, G.; Amirjannati, N.; Rashidkhani, B.; Sadeghi, M.R.; Hekmatdoost, A. Intake of food groups and idiopathic asthenozoospermia: A case control study. Hum. Reprod. 2012, 27, 3328–3336. [Google Scholar] [CrossRef] [PubMed]
- Eslamian, G.; Amirjannati, N.; Rashidkhani, B.; Sadeghi, M.R.; Baghestani, A.R.; Hekmatdoost, A. Adherence to the Western Pattern Is Potentially an Unfavorable Indicator of Asthenozoospermia Risk: A Case-Control Study. J. Am. Coll. Nutr. 2016, 35, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Mendiola, J.; Torres-Cantero, A.M.; Moreno-Grau, J.M.; Ten, J.; Roca, M.; Moreno-Grau, S.; Bernabeu, R. Food intake and its relationship with semen quality: A case-control study. Fertil. Steril. 2009, 91, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Chiu, Y.H.; Afeiche, M.C.; Gaskins, A.J.; Williams, P.L.; Petrozza, J.C.; Tanrikut, C.; Hauser, R.; Chavarro, J.E. Fruit and vegetable intake and their pesticide residues in relation to semen quality among men from a fertility clinic. Hum. Reprod. 2015, 30, 1342–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chavarro, J.E. Healthy diets and men’s contribution to fertility; is semen quality good enough? Fertil. Steril. 2017, 107, 906–907. [Google Scholar] [CrossRef] [PubMed]
- Levine, H.; Jørgensen, N.; Martino-Andrade, A.; Mendiola, J.; Weksler-Derri, D.; Mindlis, I.; Pinotti, R.; Swan, S.H. Temporal trends in sperm count: A systematic review and meta-regression analysis. Hum. Reprod. Update 2017, 23, 646–659. [Google Scholar] [CrossRef] [PubMed]
- Wądołowska, L. Walidacja kwestionariusza częstotliwości spożycia żywności–FFQ. Ocena powtarzalności. [Validation of food frequency questionaire–FFQ. Rreproducibility assessment]. Bromat. Chem. Toksykol. 2005, 38, 27–33. [Google Scholar]
- World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen, 5th ed.; WHO Press: Geneva, Switzerland, 2010; ISBN 978-924-154-778-9. [Google Scholar]
- World Health Organization. Global Database on Body Mass Index. BMI Classification. Available online: http://apps.who.int/bmi/index.jsp?introPage=intro_3.html (accessed on 23 February 2018).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Y.; Chou, Y.C.; Chao, J.C.; Hsu, C.Y.; Cha, T.L.; Tsao, C.W. The association between Dietary Patterns ans Demen Quality in a General Asian Population of 7282 Males. PLoS ONE 2015, 10, e0134224. [Google Scholar]
- Gaskins, A.J.; Colaci, D.S.; Mendiola, J.; Swan, S.H.; Chavarro, J.E. Dietary patterns and semen quality in young men. Hum. Reprod. 2012, 27, 2899–2907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oostingh, E.C.; Steegers-Theunissen, R.P.; de Vries, J.H.; Laven, J.S.; Koster, M.P. Strong adherence to a healthy dietary pattern is associated with better semen quality, especially in men with poor semen quality. Fertil. Steril. 2017, 107, 916–923. [Google Scholar] [CrossRef] [PubMed]
- Attaman, J.A.; Toth, T.L.; Furtado, J.; Campos, H.; Hauser, R.; Chavarro, J.E. Dietary fat and semen quality among men attending a fertility clinic. Hum. Reprod. 2012, 27, 1466–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, T.K.; Heitmann, B.L.; Blomberg Jensen, M.; Halldorsson, T.I.; Andersson, A.M.; Skakkebæk, N.E.; Joensen, U.N.; Lauritsen, M.P.; Christiansen, P.; Dalgård, C.; et al. High dietary intake of saturated fat is associated with reduced semen quality among 701 young Danish men from the general population. Am. J. Clin. Nutr. 2013, 97, 411–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanis, T.; Zidek, V.; Sachova, J.; Klir, P.; Deyl, Z. Effects of dietary trans-fatty acids on reproductive performance of Wistar rats. Br. J. Nutr. 1989, 61, 519–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veaute, C.; Andreoli, M.F.; Racca, A.; Bailat, A.; Scalerandi, M.V.; Bernal, C.; Malan Borel, I. Effects of isomeric fatty acids on reproductive parameters in mice. Am. J. Reprod. Immunol. 2007, 58, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Afeiche, M.C.; Bridges, N.D.; Williams, P.L.; Gaskins, A.J.; Tanrikut, C.; Petrozza, J.C.; Hauser, R.; Chavarro, J.E. Dairy intake and semen quality among men attending a fertility clinic. Fertil. Steril. 2014, 101, 1280–1287. [Google Scholar] [CrossRef] [PubMed]
- Afeiche, M.; Williams, P.L.; Mendiola, J.; Gaskins, A.J.; Jørgensen, N.; Swan, S.H.; Chavarro, J.E. Dairy food intake in relation to semen quality and reproductive hormone levels among physically active young men. Hum. Reprod. 2013, 28, 2265–2275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rozati, R.; Reddy, P.P.; Reddanna, P.; Mujtaba, R. Role of environmental estrogens in the deterioration of male factor fertility. Fertil. Steril. 2002, 78, 1187–1194. [Google Scholar] [CrossRef]
- Afeiche, M.C.; Gaskins, A.J.; Williams, P.L.; Toth, T.L.; Wright, D.L.; Tanrikut, C.; Hauser, R.; Chavarro, J.E. Processed meat intake is unfavorably and fish intake favorably associated with semen quality indicators among men attending a fertilityclinic. J. Nutr. 2014, 144, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Gross, M.; Lee, D.H.; Holvoet, P.; Himes, J.H.; Shikany, J.M.; Jacobs, D.R., Jr. Oxidative stress and insulin resistance: The coronary artery risk development in young adults study. Diabetes Care 2009, 32, 1302–1307. [Google Scholar] [CrossRef] [PubMed]
- Schoeller, E.L.; Albanna, G.; Frolova, A.I.; Moley, K.H. Insulin rescues impaired spermatogenesis via the hypothalamic-pituitary-gonadal axis in Akita diabetic mice and restores male fertility. Diabetes 2012, 61, 1869–1878. [Google Scholar] [CrossRef] [PubMed]
- Hayden, R.P.; Flannigan, R.; Schlegel, P.N. The Role of Lifestyle in Male Infertility: Diet, Physical Activity, and Body Habitus. Curr. Urol. Rep. 2018, 19, 56. [Google Scholar] [CrossRef] [PubMed]
- Chavarro, J.E.; Toth, T.L.; Sadio, S.M.; Hauser, R. Soy food and isoflavone intake in relation to semen quality parameters among men from an infertility clinic. Hum. Reprod. 2008, 23, 2584–2590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mínguez-Alarcón, L.; Afeiche, M.C.; Chiu, Y.H.; Vanegas, J.C.; Williams, P.L.; Tanrikut, C.; Toth, T.L.; Hauser, R.; Chavarro, J.E. Male soy food intake was not associated with in vitro fertilization outcomes among couples attending a fertility center. Andrology 2015, 3, 702–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jurewicz, J.; Radwan, M.; Sobala, W.; Radwan, P.; Bochenek, M.; Hanke, W. Dietary Patterns and Their Relationship with Semen Quality. Am. J. Mens Health 2018, 12, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Jurewicz, J.; Radwan, M.; Sobala, W.; Gromadzińska, J.; Jabłońska, E.; Radwan, P.; Jakubowski, L.; Wąsowicz, W.; Hanke, W. Dietary Patterns and the Frequency of Disomy in Human Sperm. Urology 2016, 93, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Karayiannis, D.; Kontogianni, M.D.; Mendorou, C.; Douka, L.; Mastrominas, M.; Yiannakouris, N. Association between adherence to the Mediterranean diet and semen quality parameters in male partners of couples attempting fertility. Hum. Reprod. 2017, 32, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Eslamian, G.; Amirjannati, N.; Rashidkhani, B.; Sadeghi, M.R.; Hekmatdoost, A. Nutrient patterns and asthenozoospermia: A case control study. Andrologia 2017, 49, e12624. [Google Scholar] [CrossRef] [PubMed]
- Luck, M.R.; Jeyaseelan, I.; Scholes, R.A. Ascorbic acid and fertility. Biol. Reprod. 1995, 52, 262–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greco, E.; Iacobelli, M.; Rienzi, L.; Ubaldi, F.; Ferrero, S.; Tesarik, J. Reduction of the incidence of sperm DNA fragmentation by oral antioxidant treatment. J. Androl. 2005, 26, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Favier, A.E. The role of zinc in reproduction. Hormonal mechanisms. Biol. Trace Elem. Res. 1992, 32, 363–382. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.Y.; Merkus, H.M.; Thomas, C.M.; Menkveld, R.; Zielhuis, G.A.; Steegers-Theunissen, R.P. Effects of folic acid and zinc sulfate on male factor subfertility: A double-blind, randomized, placebo-controlled trial. Fertil. Steril. 2002, 77, 491–498. [Google Scholar] [CrossRef]
- Vaamonde, D.; Da Silva-Grigoletto, M.E.; García-Manso, J.M.; Barrera, N.; Vaamonde-Lemos, R. Physically active men show better semen parameters and hormone values than sedentary men. Eur. J. Appl. Physiol. 2012, 112, 3267–3273. [Google Scholar] [CrossRef] [PubMed]
- Mínguez-Alarcón, L.; Chavarro, J.E.; Mendiola, J.; Gaskins, A.J.; Torres-Cantero, A.M. Physical activity is not related to semen quality in young healthy men. Fertil. Steril. 2014, 102, 1103–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Yang, H.; Zhou, N.; Sun, L.; Bao, H.; Tan, L.; Chen, H.; Ling, X.; Zhang, G.; Huang, L.; et al. Inverse U-shaped Association between Sleep Duration and Semen Quality: Longitudinal Observational Study (MARHCS) in Chongqing, China. Sleep 2016, 39, 79–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, T.K.; Andersson, A.M.; Skakkebæk, N.E.; Joensen, U.N.; Blomberg Jensen, M.; Lassen, T.H.; Nordkap, L.; Olesen, I.A.; Hansen, Å.M.; Rod, N.H.; et al. Association of sleep disturbances with reduced semen quality: A cross-sectional study among 953 healthy young Danish men. Am. J. Epidemiol. 2013, 177, 1027–1037. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Semen Parameters | Cut-Off Points |
|---|---|
| Sperm concentration | <15 × 106/ml |
| Sperm count | <39 × 106/ejaculate |
| Total motility | <40% |
| Progressive motility | <32% |
| Morphology | <4% of normal forms |
| Variables | Dietary Patterns | |
|---|---|---|
| Pro-Healthy | Western | |
| Fruits | 0.76 | 0.11 |
| Vegetables | 0.76 | 0.12 |
| Legumes | 0.66 | 0.32 |
| Soups | 0.55 | 0.25 |
| Mixed dishes | 0.47 | 0.28 |
| Whole-grain products | 0.43 | −0.24 |
| Juices | 0.43 | 0.39 |
| Nuts | 0.42 | 0.09 |
| Sweets and snacks | −0.04 | 0.71 |
| Processed meat | 0.07 | 0.59 |
| Animal fat | 0.09 | 0.57 |
| Refined grain products | 0.24 | 0.56 |
| Red meat | 0.04 | 0.53 |
| Potatoes | 0.30 | 0.50 |
| Dairy products | 0.20 | 0.44 |
| Fish and seafood | 0.39 | −0.03 |
| Sweetened fruit products | 0.39 | 0.37 |
| Eggs | 0.38 | −0.04 |
| Plant oils | −0.01 | 0.38 |
| Coffee and tea | 0.03 | 0.38 |
| Beverages | −0.00 | 0.32 |
| Alcohol drinks | −0.24 | 0.29 |
| Poultry | 0.20 | −0.00 |
| Variance explained (%) | 20.2 | 9.1 |
| Variables | Total Sample | Pro-Healthy Dietary Pattern | p1 | Western Dietary Pattern | p1 | ||||
|---|---|---|---|---|---|---|---|---|---|
| Bottom | Middle | Upper | Bottom | Middle | Upper | ||||
| n | 114 | 37 | 38 | 39 | 38 | 37 | 39 | ||
| Factor scores of dietary patterns | −2.57 to −0.48 | > −048 to 0.20 | >0.20 to 4.42 | −2.06 to −0.51 | > −0.51 to 0.30 | >0.30 to 3.26 | |||
| Age (years) | 27.2 ± 7.6 | 27.1 ± 7.5 | 27.6 ± 7.8 | 26.9 ± 7.6 | 0.718 | 28.4 ± 8.9 | 26.3 ± 6.6 | 26.9 ± 7.0 | 0.894 |
| Place of residence | 0.299 | 0.197 | |||||||
| Village and city < 50 thousand citizens | 75 (65.8) | 25 (67.6) | 24 (31.2) | 26 (66.7) | 23 (60.5) | 27 (72.9) | 25 (64.1) | ||
| City 50–100 thousand citizens | 19 (16.7) | 3 (8.1) | 7 (18.4) | 9 (23.1) | 6 (15.8) | 3 (8.1) | 10 (25.6) | ||
| City > 100 thousand citizens | 20 (17.5) | 9 (24.3) | 7 (18.4) | 4 (10.2) | 9 (23.7) | 7 (18.9) | 4 (10.3) | ||
| Economic status | 0.826 | 0.531 | |||||||
| Below average | 2 (1.8) | 1 (2.7) | 0 (0.0) | 1 (2.6) | 0 (0.0) | 1 (2.7) | 1 (2.6) | ||
| Average | 95 (83.3) | 31 (83.8) | 31 (81.6) | 33 (84.6) | 34 (89.5) | 28 (75.7) | 33 (84.6) | ||
| Above average | 17 (14.9) | 5 (13.5) | 7 (18.4) | 5 (12.8) | 4 (10.5) | 8 (21.6) | 5 (12.8) | ||
| Educational level | 0.983 | 0.006 | |||||||
| Basic and vocational | 16 (14.0) | 6 (16.2) | 5 (13.2) | 5 (12.8) | 2 (5.3) | 4 (10.8) | 10 (25.6) | ||
| Intermediate | 54 (47.4) | 18 (48.7) | 18 (47.4) | 18 (46.2) | 14 (36.8) | 19 (51.4) | 21 (53.9) | ||
| High | 44 (38.6) | 13 (35.1) | 15 (39.5) | 16 (41.0) | 22 (57.9) | 14 (37.8) | 8 (20.5) | ||
| Socioeconomic status (tertiles) | 0.827 | 0.205 | |||||||
| Bottom | 32 (28.1) | 12 (32.4) | 11 (28.9) | 9 (23.1) | 6 (15.8) | 11 (29.7) | 15 (38.5) | ||
| Middle | 34 (29.8) | 9 (24.3) | 11 (28.9) | 14 (35.9) | 12 (31.6) | 10 (27.1) | 12 (30.8) | ||
| Upper | 48 (41.1) | 16 (43.3) | 16 (42.1) | 16 (41.0) | 20 (52.6) | 16 (43.2) | 12 (30.8) | ||
| BMI (kg/m2) | 24.7 ± 2.3 | 24.7 ± 2.7 | 24.8 ± 2.1 | 24.7 ± 2.2 | 0.953 | 24.8 ± 1.9 | 24.7 ± 2.6 | 24.6 ± 2.4 | 0.750 |
| BMI < 25 kg/m2 | 67 (58.8) | 21 (56.8) | 22 (57.9) | 24 (61.5) | 0.906 | 20 (52.6) | 25 (67.6) | 22 (56.4) | 0.394 |
| BMI ≥ 25 kg/m2 | 47 (41.2) | 16 (43.2) | 16 (42.1) | 15 (38.5) | 18 (47.4) | 12 (32.4) | 17 (43.6) | ||
| Physical activity (MET-h/week) | 135.2 ± 78.9 | 122.2 ± 74.3 | 138.2 ± 79.4 | 144.6 ± 83.1 | 0.574 | 120.2 ± 84.0 | 121.0 ± 65.2 | 163.3 ± 80.1 | 0.014 |
| Sedentary time (h/day) | 3.0 ± 2.5 | 4.0 ± 3.1 | 2.7 ± 2.1 | 2.3 ± 1.7 | 0.020 | 2.5 ± 1.8 | 3.0 ± 2.6 | 3.5 ± 2.8 | 0.360 |
| Sleep duration (h/day) | 7.1 ± 1.1 | 7.1 ± 1.2 | 6.9 ± 1.0 | 7.2 ± 1.1 | 0.572 | 7.1 ± 1.2 | 7.0 ± 1.2 | 7.3 ± 1.0 | 0.492 |
| Sperm concentration (106/ml) | 53.9 ± 65.4 | 52.5 ± 51.4 | 50.9 ± 59.4 | 58.0 ± 82.2 | 0.702 | 62.5 ± 68.9 | 57.0 ± 59.8 | 42.4 ± 67.1 | 0.423 |
| Abnormal sperm concentration 2 | 37 (32.5) | 10 (27.0) | 12 (31.6) | 15 (38.5) | 0.562 | 9 (23.7) | 13 (35.1) | 15 (38.5) | 0.351 |
| Sperm count (106/ejaculate) | 178.7 ± 225.5 | 173.0 ± 185.7 | 169.1 ± 187.2 | 193.3 ± 290.1 | 0.686 | 226.1 ± 252.9 | 180.6 ± 196.9 | 130.6 ± 218.2 | 0.274 |
| Abnormal sperm count 2 | 32 (28.1) | 10 (27.0) | 8 (21.1) | 14 (35.9) | 0.345 | 8 (21.1) | 11 (29.7) | 13 (33.3) | 0.469 |
| Total motility (%) | 48.0 ± 16.3 | 50.5 ± 16.1 | 47.1 ± 15.9 | 46.6 ± 16.9 | 0.611 | 51.7 ± 15.2 | 45.2 ± 17.7 | 47.1 ± 15.6 | 0.239 |
| Abnormal total motility 2 | 39 (34.2) | 12 (32.4) | 12 (31.6) | 15 (38.5) | 0.786 | 9 (23.7) | 15 (40.5) | 15 (38.5) | 0.241 |
| Progressive motility (%) | 30.4 ± 14.0 | 32.6 ± 13.6 | 29.8 ± 13.7 | 28.9 ± 14.8 | 0.596 | 34.6 ± 13.8 | 28.6 ± 14.7 | 28.0 ± 12.9 | 0.055 |
| Abnormal progressive motility 2 | 63 (55,3) | 20 (54.1) | 22 (57.9) | 21 (53.9) | 0.923 | 14 (36.8) | 22 (59.5) | 27 (69.2) | 0.014 |
| Morphology (% of normal forms) | 7.8 ± 5.9 | 7.7 ± 5.6 | 7.4 ± 6.0 | 8.1 ± 6.4 | 0.856 | 7.9 ± 6.3 | 7.8 ± 6.2 | 7.5 ± 5.4 | 0.989 |
| Abnormal morphology 2 | 28 (25.6) | 8 (21.6) | 9 (23.7) | 11 (28.2) | 0.791 | 9 (23.7) | 8 (21.6) | 11 (28.2) | 0.791 |
| Abnormal Semen Quality Parameters | Dietary Patterns | |||||||
|---|---|---|---|---|---|---|---|---|
| Pro-Healthy | Western | |||||||
| Bottom | Middle | Upper | P-trend | Bottom | Middle | Upper | P-trend | |
| n | 37 | 38 | 39 | 38 | 37 | 39 | ||
| Total count | ||||||||
| Crude | ref | 0.72 (0.24; 2.13) | 1.51 (0.56; 4.08) | 0.561 | ref | 1.58 (0.54; 4.62) | 1.88 (0.66; 5.32) | 0.116 |
| Adjusted | ref | 0.66 (0.21; 2.09) | 1.49 (0.50; 4.41) | 0.600 | ref | 1.43 (0.47; 4.36) | 1.86 (0.58; 6.01) | <0.050 |
| Sperm concentration | ||||||||
| Crude | ref | 1.25 (0.45; 3.44) | 1.68 (0.63; 4.53) | 0.097 | ref | 1.75 (0.63; 4.86) | 2.01 (0.74; 5.50) | 0.134 |
| Adjusted | ref | 1.07 (0.37; 3.10) | 1.82 (0.62; 5.33) | 0.284 | ref | 1.72 (0.60; 4.93) | 2.01 (0.65; 6.20) | 0.153 |
| Progressive motility | ||||||||
| Crude | ref | 1.17 (0.44; 3.13) | 0.99 (0.40; 2.45) | 0.969 | ref | 2.51 (0.98; 6.47) | 3.86 (1.47; 10.10) *** | <0.050 |
| Adjusted | ref | 1.46 (0.54; 3.97) | 1.21 (0.43; 3.34) | 0.699 | ref | 2.89 (1.03; 8.09) * | 4.78 (1.52; 15.06) *** | <0.050 |
| Total motility | ||||||||
| Crude | ref | 0.96 (0.36; 2.58) | 1.30 (0.50; 3.40) | 0.402 | ref | 2.20 (0.80; 6.04) | 2.01 (0.74; 5.50) | 0.427 |
| Adjusted | ref | 1.30 (0.44; 3.82) | 1.46 (0.50; 4.29) | 0.111 | ref | 2.31 (0.76; 7.01) | 2.43 (0.76; 7.75) | 0.285 |
| Morphology | ||||||||
| Crude | ref | 1.13 (0.37; 3.38) | 1.42 (0.49; 4.13) | 0.138 | ref | 0.89 (0.30; 2.67) | 1.26 (0.45; 3.58) | 0.154 |
| Adjusted | ref | 1.22 (0.37; 4.07) | 1.32 (0.41; 4.23) | 0.136 | ref | 1.11 (0.34; 3.57) | 1.22 (0.37; 4.01) | <0.050 |
| TMSC | ||||||||
| Crude | ref | 0.84 (0.49; 2.41) | 1.88 (0.70; 5.02) | 0.425 | ref | 1.75 (0.63; 4.86) | 1.61 (0.58; 4.46) | 0.446 |
| Adjusted | ref | 0.95 (0.29; 3.06) | 1.76 (0.61; 5.07) | 0.368 | ref | 1.60 (0.55; 4.66) | 1.56 (0.49; 5.01) | 0.371 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Danielewicz, A.; Przybyłowicz, K.E.; Przybyłowicz, M. Dietary Patterns and Poor Semen Quality Risk in Men: A Cross-Sectional Study. Nutrients 2018, 10, 1162. https://doi.org/10.3390/nu10091162
Danielewicz A, Przybyłowicz KE, Przybyłowicz M. Dietary Patterns and Poor Semen Quality Risk in Men: A Cross-Sectional Study. Nutrients. 2018; 10(9):1162. https://doi.org/10.3390/nu10091162
Chicago/Turabian StyleDanielewicz, Anna, Katarzyna Eufemia Przybyłowicz, and Mariusz Przybyłowicz. 2018. "Dietary Patterns and Poor Semen Quality Risk in Men: A Cross-Sectional Study" Nutrients 10, no. 9: 1162. https://doi.org/10.3390/nu10091162
APA StyleDanielewicz, A., Przybyłowicz, K. E., & Przybyłowicz, M. (2018). Dietary Patterns and Poor Semen Quality Risk in Men: A Cross-Sectional Study. Nutrients, 10(9), 1162. https://doi.org/10.3390/nu10091162