Effects of Caffeine on Myocardial Blood Flow: A Systematic Review

 , ,
, ,
Abstract
1. Introduction
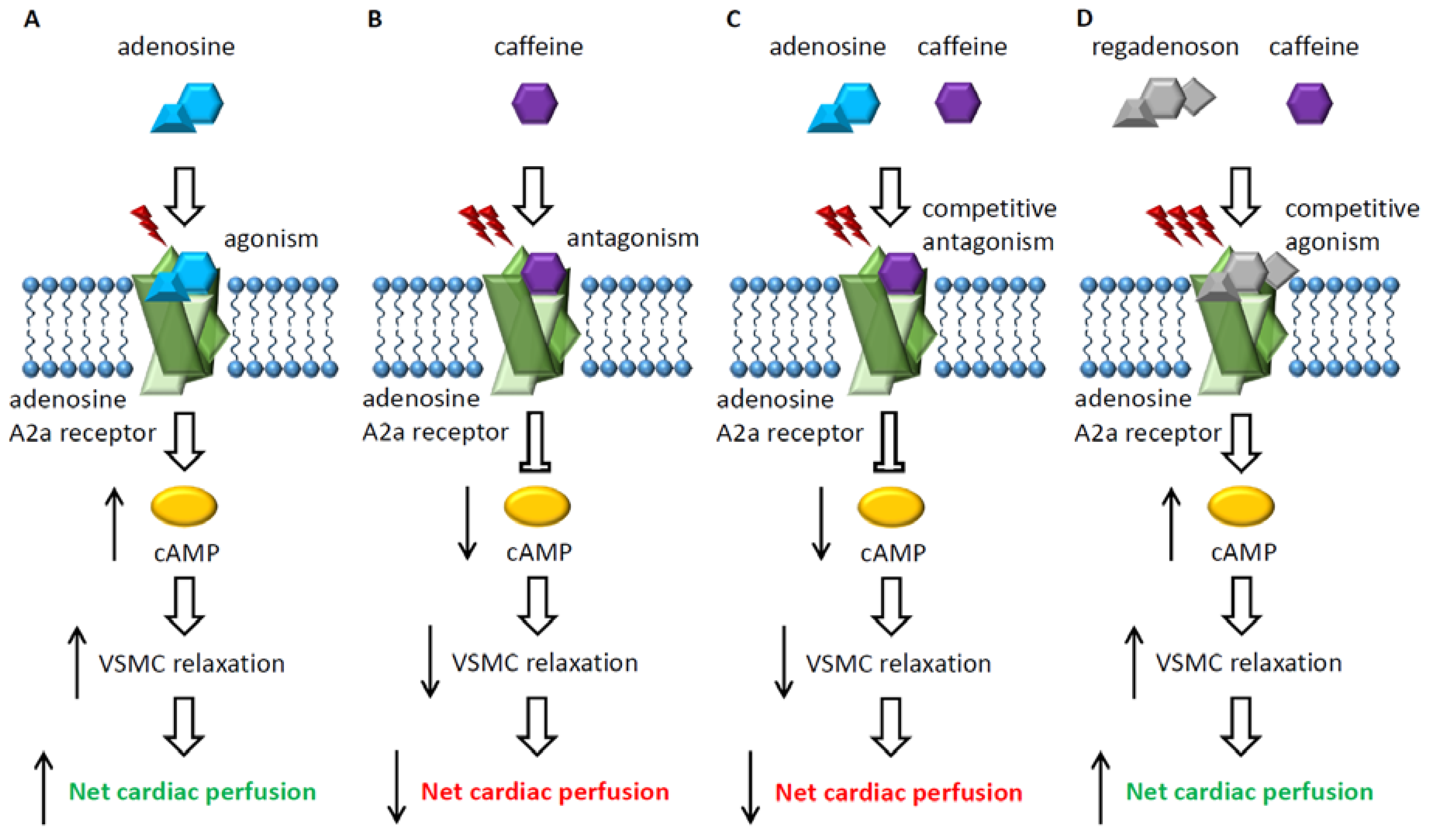
1.1. Vasodilator Agent Mechanisms of Action
1.2. Caffeine Antagonism
1.3. Caffeine Consumption
1.4. Clinical Practice
1.5. Aim of the Study
2. Methods and Results
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Study Selection and Data Collection
2.5. Search Results
2.6. Study Characteristics
2.7. Study Quality
3. Discussion
3.1. SPECT
3.2. PET
3.3. MRI
3.4. ICA
3.5. Contributing Factors
3.6. Clinical Relevance
3.7. Stress Adequacy
4. Conclusions
Implications of Key Findings
Author Contributions
Conflicts of Interest
References
- Buhr, C.; Gössl, M.; Erbel, R.; Eggebrecht, H. Regadenoson in the detection of coronary artery disease. Vasc. Health Risk Manag. 2008, 4, 337–340. [Google Scholar] [PubMed]
- Spicuzza, L.; Di Maria, G.; Polosa, R. Adenosine in the airways: Implications and applications. Eur. J. Pharmacol. 2005, 533, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Spicuzza, L.; Bonfiglio, C.; Polosa, R. Research applications and implications of adenosine in diseased airways. Trends Pharmacol. Sci. 2003, 24, 409–413. [Google Scholar] [CrossRef]
- Cerqueira, M.D. The future of pharmacologic stress: Selective A2A adenosine receptor agonists. Am. J. Cardiol. 2004, 94, 33D–40D. [Google Scholar] [CrossRef] [PubMed]
- Shryock, J.C.; Snowdy, S.; Baraldi, P.G.; Cacciari, B.; Spalluto, G.; Monopoli, A.; Ongini, E.; Baker, S.P.; Belardinelli, L. A2A-Adenosine receptor reserve for coronary vasodilation. Circulation 1998, 98, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Jaroudi, W.A.; Iskandrian, A.E. Regadenoson: A new myocardial stress agent. J. Am. Coll. Cardiol. 2009, 54, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Hendel, R.C.; Bateman, T.M.; Cerqueira, M.D.; Iskandrian, A.E.; Leppe, J.A.; Blackburn, B.; Mahmarian, J.J. Initial clinical experience with regadenoson, a novel selective A2A Agonist for pharmacologic stress single-photon emission computed tomography myocardial perfusion imaging. J. Am. Coll. Cardiol. 2005, 46, 2069–2075. [Google Scholar] [CrossRef]
- Thomas, G.S.; Tammelin, B.R.; Schiffman, G.L.; Marquez, R.; Rice, D.L.; Milikien, D.; Mathur, V. Safety of regadenoson, a selective adenosine A2A agonist, in patients with chronic obstructive pulmonary disease: A randomized, double-blind, placebo-controlled trial (RegCOPD trial). J. Nucl. Cardiol. 2008, 15, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Fredholm, B.B. Adenosine, adenosine receptors and the actions of caffeine. Pharmacol. Toxicol. 1995, 76, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Kidambi, A.; Sourbron, S.; Maredia, N.; Motwani, M.; Brown, J.M.; Nixon, J.; Everett, C.C.; Plein, S.; Greenwood, J.P. Factors associated with false-negative cardiovascular magnetic resonance perfusion studies: A clinical evaluation of magnetic resonance imaging in coronary artery disease (CE-MARC) substudy. J. Magn. Reson. Imaging 2016, 43, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Reyes, E. Caffeine reduces the sensitivity of vasodilator MPI for the detection of myoardial ischaemia: Pro. J. Nucl. Cardiol. 2016, 23, 447–453. [Google Scholar] [CrossRef]
- Saab, R.; Bajaj, N.S.; Hage, F.G. Caffeine does not significantly reduce the sensitivity of vasodilator stress myocardial perfusion imaging. J. Nucl. Cardiol. 2015, 23, 442–446. [Google Scholar] [CrossRef] [PubMed]
- Lapeyre, A.C.; Goraya, T.Y.; Johnston, D.L.; Gibbons, R.J. The impact of caffeine on vasodilator stress perfusion studies. J. Nucl. Cardiol. 2004, 11, 506–511. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Scientific opinion on the safety of caffeine1 EFSA panel on dietetic products, nutrition and allergies (NDA). ESFA J. 2015, 13, 4102. [Google Scholar]
- McCusker, R.R.; Goldberger, B.A.; Cone, E.J. Caffeine content of specialty coffees. J. Anal. Toxicol. 2003, 27, 520–522. [Google Scholar] [CrossRef] [PubMed]
- Banko, L.T.; Haq, S.A.; Rainaldi, D.A.; Klem, I.; Siegler, J.; Fogel, J.; Sacchi, T.J.; Heitner, J.F. Incidence of caffeine in serum of patients undergoing dipyridamole myocardial perfusion stress test by an intensive versus routine caffeine history screening. Am. J. Cardiol. 2009, 105, 1474–1479. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, M.; Jögi, J.; Bloch, K.M.; Hedén, B.; Ekelund, U.; Ståhlberg, F.; Arheden, H. Submaximal adenosine-induced coronary hyperaemia with 12 h caffeine abstinence: Implications for clinical adenosine perfusion imaging tests. Clin. Physiol. Funct. Imaging 2015, 35, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Windecker, S.; Kolh, P.; Alfonso, F.; Collet, J.P.; Cremer, J.; Falk, V.; Filippatos, G.; Hamm, C.; Head, S.J.; Jüni, P.; et al. 2014 ESC/EACTS Guidelines onmyocardial revascularization. The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2014, 35, 2541–2619. [Google Scholar] [PubMed]
- Takx, R.A.; Blomberg, B.A.; El Aidi, H.; Habets, J.; de Jong, P.A.; Nagel, E.; Hoffmann, U.; Leiner, T. Diagnostic accuracy of stress myocardial perfusion imaging compared to invasive coronary angiography with fractional flow reserve meta-analysis. Circ. Cardiovasc. Imaging 2015, 8, e002666. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.C.; Fraser, J.F.; Barnett, A.G.; Johnson, L.P.; Wilson, M.G.; McHenry, C.M.; Walters, D.L.; Warnholtz, C.R.; Khafagi, A. Effect of caffeine on adenosine-induced reversible perfusion defects assessed by automated analysis. J. Nucl. Cardiol. 2012, 19, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Zoghbi, G.J.; Htay, T.; Aqel, R.; Blackmon, L.; Heo, J.; Iskandrian, A.E. Effect of caffeine on ischemia detection by adenosine single-photon emission computed tomography perfusion imaging. J. Am. Coll. Cardiol. 2006, 47, 2296–2302. [Google Scholar] [CrossRef] [PubMed]
- Reyes, E.; Loong, C.Y.; Harbinson, M.; Donovan, J.; Anagnostopoulos, C.; Underwood, S.R. High-dose adenosine overcomes the attenuation of myocardial perfusion reserve caused by caffeine. J. Am. Coll. Cardiol. 2008, 52, 2008–2016. [Google Scholar] [CrossRef]
- Smits, P.; Corstens, F.H.; Aengevaeren, W.R.; Wackers, F.J.; Thien, T. False-negative dipyridamole-thallium-201 myocardial imaging after caffeine infusion. J. Nucl. Med. 1991, 32, 1538–1541. [Google Scholar]
- Tejani, F.H.; Thompson, R.C.; Kristy, R.; Bukofzer, S. Effect of caffeine on SPECT myocardial perfusion imaging during regadenoson pharmacologic stress: A prospective, randomized, multicenter study. Int. J. Cardiovasc. Imaging 2014, 30, 979–989. [Google Scholar] [CrossRef] [PubMed]
- Böttcher, M.; Czernin, J.; Sun, K.T.; Phelps, M.E.; Schelbert, H.R. Effect of caffeine on myocardial blood flow at rest and during pharmacological vasodilation. J. Nucl. Med. 1995, 36, 2016–2021. [Google Scholar]
- Kubo, S.; Tadamura, E.; Toyoda, H.; Mamede, M.; Yamamuro, M.; Magata, Y.; Mukai, T.; Kitano, H.; Tamaki, N.; Konishi, J. Effect of caffeine intake on myocardial hyperemic flow induced by adenosine triphosphate and dipyridamole. J. Nucl. Med. 2004, 45, 730–738. [Google Scholar] [PubMed]
- Greulich, S.; Kaesemann, P.; Seitz, A.; Birkmeier, S.; Abu-Zaid, E.; Vecchio, F.; Sechtem, U.; Mahrholdt, H. Effects of caffeine on the detection of ischemia in patients undergoing adenosine stress cardiovascular magnetic resonance imaging. J. Cardiovasc. Magn. Reson. 2017, 19, 103. [Google Scholar] [CrossRef]
- Van Dijk, R.; Kuijpers, D.; Kaandorp, T.A.M.; van Dijkman, P.R.M.; Vliegenthart, R.; van der Harst, P.; Oudkerk, M. Effects of caffeine intake prior to stress cardiac magnetic resonance perfusion imaging on regadenoson-versus adenosine-induced hyperemia as measured by T1 mapping. Int. J. Cardiovasc. Imaging 2017, 33, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, M.; Chikamori, T.; Uchiyama, T.; Kimura, Y.; Hijikata, N.; Ito, R.; Yuhara, M.; Sato, H.; Kobori, Y.; Yamashina, A. Effects of caffeine on fractional flow reserve values measured using intravenous adenosine triphosphate. Cardiovasc. Interv. Ther. 2018, 33, 116–124. [Google Scholar] [CrossRef]
- Matsumoto, H.; Nakatsuma, K.; Shimada, T.; Ushimaru, S.; Mikuri, M.; Yamazaki, T.; Matsuda, T. Effect of caffeine on intravenous adenosine-induced hyperemia in fractional flow reserve measurement. J. Invasive Cardiol. 2014, 26, 580–585. [Google Scholar] [PubMed]
- Mutha, V.; Ul Haq, M.A.; Van Gaal, W.J. Effects of intravenous caffeine on fractional flow reserve measurements in coronary artery disease. Open Heart 2014, 1, e000060. [Google Scholar] [CrossRef] [PubMed]
- Aqel, R.A.; Zoghbi, G.J.; Trimm, J.R.; Baldwin, S.A.; Iskandrian, A.E. Effect of caffeine administered intravenously on intracoronary-administered adenosine-induced coronary hemodynamics in patients with coronary artery disease. Am. J. Cardiol. 2004, 93, 343–346. [Google Scholar] [CrossRef]
- Montalescot, G.; Sechtem, U.; Achenbach, S.; Andreotti, F.; Arden, C.; Montalescot, G.; Arden, C.; Budaj, A.; Bugiardini, R.; Crea, F.; et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur. Heart J. 2013, 34, 2949–3003. [Google Scholar] [CrossRef] [PubMed]
- Hachamovitch, R.; Berman, D.S.; Shaw, L.J.; Kiat, H.; Cohen, I.; Cabico, J.A.; Friedman, J.; Diamond, G.A. Incremental prognostic value of myocardial perfusion single photon emission computed tomography for the prediction of cardiac death: Differential stratification for risk of cardiac death and myocardial infarction. Circulation 1998, 97, 535–543. [Google Scholar] [CrossRef]
- Leiner, T. Hold off on that shot of Java: More evidence that caffeine intake leads to false negative adenosine stress myocardial perfusion. Int. J. Cardiovasc. Imaging 2017, 33, 97–99. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N | Intervention/Controls * | Study Population | Age | Male | BMI | |
|---|---|---|---|---|---|---|
| SPECT | ||||||
| Smits 1991 | 8 | 8/0 | Ischemia on baseline MPI | 60 ± 7 | 3(38) | 28 ± 4 |
| Zoghbi 2006 | 30 | 30/0 | Ischemia on baseline MPI | 64 ± 9 | 22(73) | NS |
| Reyes 2008 | 30 | 12/0 | Ischemia on baseline MPI | 66 ± 6 | NS | 29 ± 4 |
| 18/0 | Ischemia on baseline MPI | 64 ± 7 | NS | 27 ± 3 | ||
| Lee 2012 | 30 | 30/0 | Ischemia on baseline MPI | 70 ± 8 | 21(70) | NS |
| Tejani 2014 | 207 | 0/66 70/0 71/0 | Ischemia on baseline MPI | 68 ± 10.0/65.7 ± 11/69.4 ± 8.2 | 55(83.3)/58(82.9/51(71.8) | NS |
| PET | ||||||
| Böttcher 1995 | 12 | 12/0 | healthy volunteers | 27 ± 6 | 7(58) | NS |
| Kubo 2004 | 10 | 10/0 | healthy volunteers | 31 ± 6 | 10(100) | NS |
| 10 | 10/0 | healthy volunteers | 31 ± 6 | 10(100) | NS | |
| MRI | ||||||
| Carlsson 2015 | 16 | 16/0 | healthy volunteers | 41 ± 3 | 8(50) | NS |
| Greulich 2017 | 30 | 30/0 | Ischemia on baseline MPI | 68 ± 8 | 25(83) | NS |
| van Dijk 2017 | 98 | 15/50 | suspected of CAD | 65 ± 11 | 46(49) | NS |
| 9/24 | suspected of CAD | 65 ± 11 | 46(49) | NS | ||
| ICA | ||||||
| Matsumoto 2014 | 42 | 28/14 | Intermediate stenosis | 70 ± 8/69 ± 10 | 21(75)/11(79) | 24 ± 3/23 ± 4 |
| 42 | 28/14 | Intermediate stenosis | 70 ± 8/69 ± 10 | 21(75)/11(79) | 24 ± 3/23 ± 4 | |
| 42 | 28/14 | Intermediate stenosis | 70 ± 8/69 ± 10 | 21(75)/11(79) | 24 ± 3/23 ± 4 | |
| Mutha 2014 | 10 | 10/0 | Intermediate stenosis | 60 ± 9 | 8(80) | NS |
| Aqel 2004 | 10 | 10/0 | patients with CAD | 53 ± 8 | 10(100) | NS |
| Nakayama 2018 | 30 | 15/15 | patients with significant CAD | 69 ± 10 | 25(83) | 24 ± 3 |
| 30 | 15/15 | patients with significant CAD | 69 ± 10 | 25(83) | 24 ± 3 |
| Vasodilator | Dosage | Caffeine Dosage | Serum Concentration | Timing * | Main Finding | p-Value | |
|---|---|---|---|---|---|---|---|
| SPECT | |||||||
| Smits 1991 | Dipyridamole | 0.56 mg/kg | 4 mg/kg i.v. | 9.7 ± 1.3 mg/L | 30 min | Redistribution score caffeine 2.0 ± 1.1 vs. 9.0 ± 0.9 baseline | <0.05 |
| Zoghbi 2006 | Adenosine | 140 µg/kg/min | 8 oz cup of coffee | 3.1 ± 1.6 mg/L | 1 h | SDS caffeine 3.9 ± 2.3 vs. 3.8 ± 1.9 without caffeine | 0.8 |
| Reyes 2008 | Adenosine | 140 µg/kg/min | 2 shots espresso | 6.2 ± 2.6 | 1 h | SDS caffeine 4.1 ± 2.1 vs. baseline 12.0 ± 4.4 | <0.001 |
| Adenosine | 210 µg/kg/min | 2 shots espresso | 5.7 ± 2.0 | 1 h | SDS caffeine 7.8 ± 4.2 vs. baseline 7.7 ± 4.0 | 0.7 | |
| Lee 2012 | Adenosine | 140 µg/kg/min | one cup of coffee | 3.4 mg/L range 0.7–10.4 | 1 h | mean difference stress percent defect −1.6 | 0.3 |
| Tejani 2014 | Regadenoson | 400 µg | placebo, 200 mg or 400 mg caffeine orally | NS | 1.5 h | mean difference number of ischemic segments after 200 mg −0.61 ± 1.097, 400 mg −0.62 ± 1.367, placebo −0.12 ± 0.981 | <0.001 |
| PET | |||||||
| Böttcher 1995 | Dipyridamole | 560 µg/kg | 1–2 cups of coffee | range 0–8 mg/L | 1–4 h | Flow reserve caffeine 2.3 ± 0.7 vs. 3.4 ± 0.8 | <0.001 |
| Kubo 2004 | Dipyridamole | 560 µg/kg | 2–3 cups of coffee | 3.3 ± 1.3 mg/L | 1.5 h | MFR caffeine 2.25 ± 0.94 vs. baseline 4.11 ± 1.44 | <0.005 |
| ATP | 160 µg/kg/min | 2–3 cups of coffee | 3.1 ± 1.6 mg/L | 1.5 h | MFR caffeine 2.44 ± 0.88 vs. baseline 5.15 ± 1.64 | <0.005 | |
| MRI | |||||||
| Carlsson 2015 | Adenosine | 140 µg/kg/min | minimal 6 g instant coffee | NS | 12 vs. 24 h | CsFR 12 h 4.31 ± 0.57 vs. 24 h 5.32 ± 0.76 | 0.03 |
| Greulich 2017 | Adenosine | 140 µg/kg/min | 200 mg orally | 4.6 ± 2.2 mg/L | 1 h | Ischemic burden 6.9 ± 3.5 caffeine vs. 7.9 ± 3.5 baseline | <.001 |
| van Dijk 2017 | Adenosine | 140 µg/kg/min | 1–2 cups of coffee | NS | <4 h | T1 reactivity caffeine −7.8 ± 5.0 vs. control 4.3 ± 2.8 | <0.001 |
| Regadenoson | 400 µg | 1–2 cups of coffee | NS | <4 h | T1 reactivity caffeine 4.4 ± 3.2 vs. control 5.4 ± 2.4 | 0.4 | |
| ICA | |||||||
| Matsumoto 2014 | Adenosine | 140 µg/kg/min | 20 patients 100 or 200 mg orally | 2.9[1.8–4.6] mg/L | NS | FFR caffeine 0.81 ± 0.09 vs. 0.78 ± 0.09 papaverine | <0.001 |
| Adenosine | 170 µg/kg/min | 20 patients 100 or 200 mg orally | 2.9[1.8–4.6] mg/L | NS | FFR caffeine 0.81 ± 0.09 vs. 0.78 ± 0.09 papaverine | <0.01 | |
| Adenosine | 210 µg/kg/min | 20 patients 100 or 200 mg orally | 2.9[1.8–4.6] mg/L | NS | FFR caffeine 0.79 ± 0.09 vs. 0.78 ± 0.09 papaverine | 0.01 | |
| Mutha 2014 | Adenosine | 140 µg/kg/min | 4 mg/kg i.v. | 16.4 ± 5.5 mg/L | 7 min | FFR caffeine 0.82 ± 0.11 vs. 0.79 ± 0.07 baseline | 0.15 |
| Aqel 2004 | Adenosine | 30–50 µg bolus i.c. | 4 mg/kg i.v. | 3.8 ± 1.3 mg/L | 5 min | FFR caffeine 0.75 ± 0.14 vs. 0.76 ± 0.13 | 0.7 |
| Nakayama 2018 | ATP | 140 µg/kg/min | 222 mg orally | 7.3 ± 2.0 mg/L | 2 min | FFR caffeine 0.78 ± 0.12 vs. FFR papaverine 0.75 ± 0.14 | 0.002 |
| ATP | 170 µg/kg/min | 222 mg orally | 7.3 ± 2.0 mg/L | 2 h | FFR caffeine 0.77 ± 0.12 vs. FFR papaverine 0.75 ± 0.14 | 0.007 | |
| Patient Selection | Intervention | Analysis | Timing Interval | |
|---|---|---|---|---|
| SPECT | ||||
| Smits 1991 | ||||
| Zoghbi 2006 | ||||
| Reyes 2008 | ||||
| Lee 2012 | ||||
| Tejani 2014 | ||||
| PET | ||||
| Böttcher 1995 | ||||
| Kubo 2004 | ||||
| CMR | ||||
| Carlsson 2015 | ||||
| Greulich 2017 | ||||
| van Dijk 2017 | ||||
| ICA | ||||
| Matsumoto 2014 | ||||
| Mutha 2004 | ||||
| Aqel 2004 | ||||
| Nakayama 2018 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Dijk, R.; Ties, D.; Kuijpers, D.; Van der Harst, P.; Oudkerk, M. Effects of Caffeine on Myocardial Blood Flow: A Systematic Review. Nutrients 2018, 10, 1083. https://doi.org/10.3390/nu10081083
Van Dijk R, Ties D, Kuijpers D, Van der Harst P, Oudkerk M. Effects of Caffeine on Myocardial Blood Flow: A Systematic Review. Nutrients. 2018; 10(8):1083. https://doi.org/10.3390/nu10081083
Chicago/Turabian StyleVan Dijk, Randy, Daan Ties, Dirkjan Kuijpers, Pim Van der Harst, and Matthijs Oudkerk. 2018. "Effects of Caffeine on Myocardial Blood Flow: A Systematic Review" Nutrients 10, no. 8: 1083. https://doi.org/10.3390/nu10081083
APA StyleVan Dijk, R., Ties, D., Kuijpers, D., Van der Harst, P., & Oudkerk, M. (2018). Effects of Caffeine on Myocardial Blood Flow: A Systematic Review. Nutrients, 10(8), 1083. https://doi.org/10.3390/nu10081083