Vegetable Diversity, Injurious Falls, and Fracture Risk in Older Women: A Prospective Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Assessment
2.3. Injurious Falls and Fracture Outcome Assessment
2.4. Baseline Characteristic Assessment
2.5. Statistical Analysis
2.6. Additional Analysis
3. Results
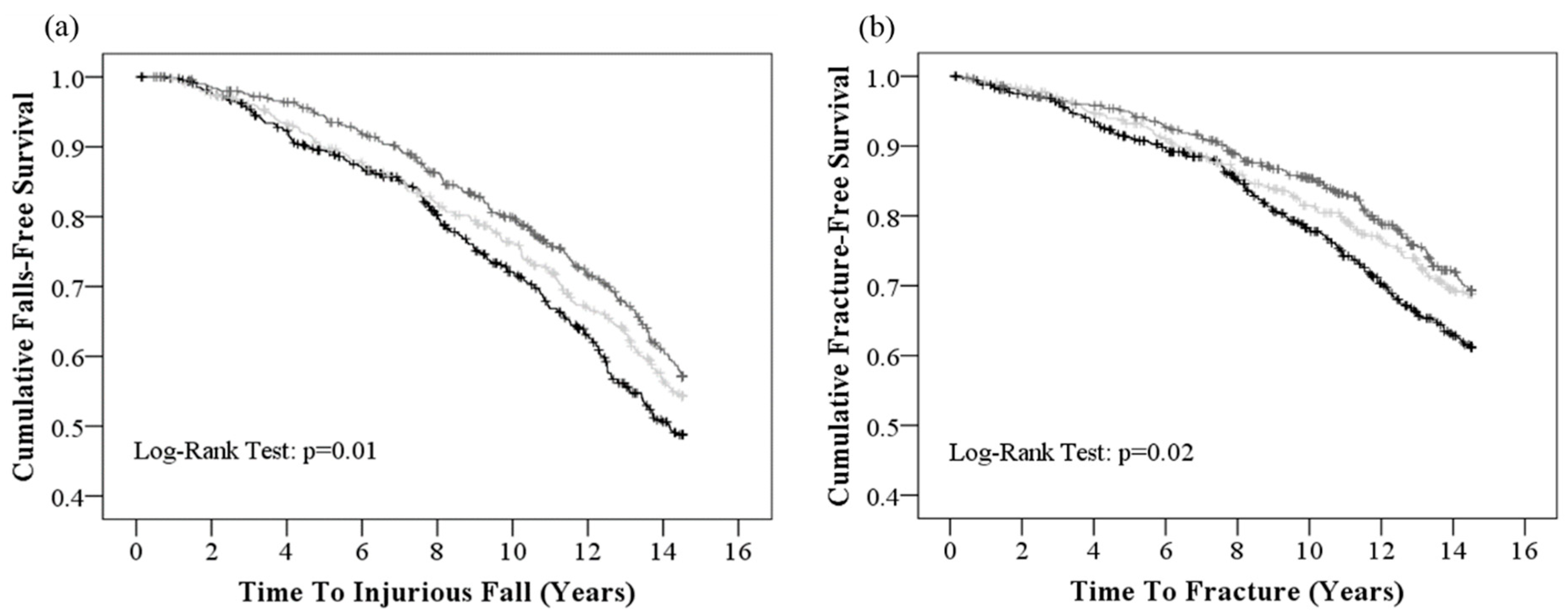
3.1. Vegetable Diversity and Injurious Falls (Falls-Related Hospitalization)
3.2. Vegetable Diversity and Fracture-Related Hospitalization
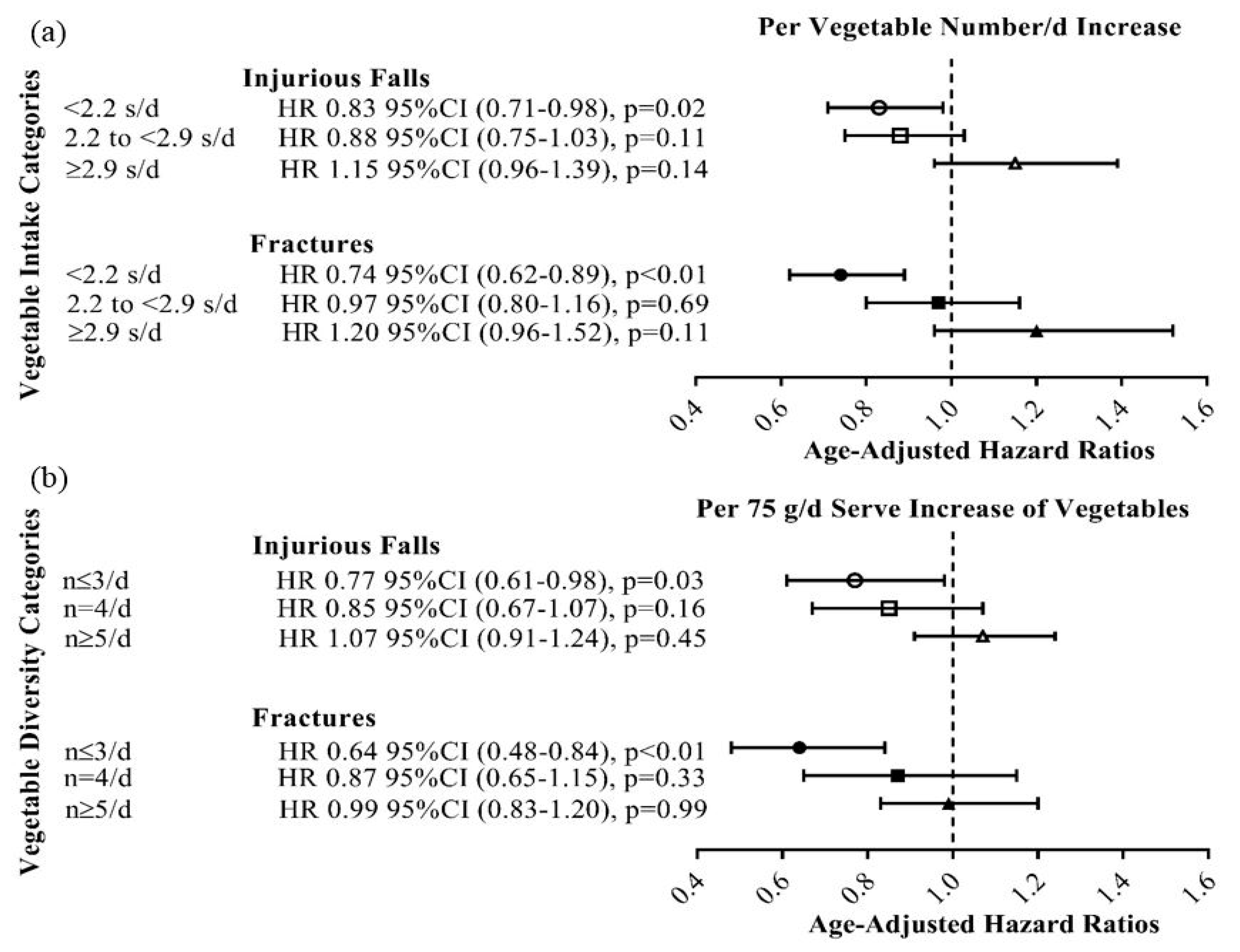
3.3. Additional Analysis
3.3.1. Vegetable Diversity and Total Vegetable Intake
3.3.2. Self-Reported Falls
3.3.3. Hip Fractures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Australian Dietary Guidelines (2013). Available online: https://www.nhmrc.gov.au/guidelines-publications/n55 (accessed on 3 April 2018).
- 2015–2020 Dietary Guidelines for Americans. Available online: https://health.gov/dietaryguidelines/2015/ (accessed on 3 April 2018).
- Blekkenhorst, L.C.; Sim, M.; Bondonno, C.P.; Bondonno, N.P.; Ward, N.C.; Prince, R.L.; Devine, A.; Lewis, J.R.; Hodgson, J.M. Cardiovascular health benefits of specific vegetable types: A narrative review. Nutrients 2018, 10, 595. [Google Scholar] [CrossRef] [PubMed]
- Downton, J.H.; Andrews, K. Prevalence, characteristics and factors associated with falls among the elderly living at home. Aging Clin. Exp. Res. 1991, 3, 219–228. [Google Scholar] [CrossRef]
- King, M.B.; Tinetti, M.E. Falls in community-dwelling older persons. J. Am. Geriatr. Soc. 1995, 43, 1146–1154. [Google Scholar] [CrossRef] [PubMed]
- Francis, R.M. Falls and fractures. Age. Ageing 2001, 30, 25–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, S.D.; Miller, R.R. Falls: Epidemiology, pathophysiology, and relationship to fracture. Curr. Osteopodos. Rep. 2008, 6, 149–154. [Google Scholar] [CrossRef] [Green Version]
- Robinson, S.M.; Jameson, K.A.; Batelaan, S.F.; Martin, H.J.; Syddall, H.E.; Dennison, E.M.; Cooper, C.; Sayer, A.A. Diet and its relationship with grip strength in community-dwelling older men and women: The hertfordshire cohort study. J. Am. Geriatr. Soc. 2008, 56, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Myint, P.K.; Welch, A.A.; Bingham, S.A.; Surtees, P.G.; Wainwright, N.W.J.; Luben, R.N.; Wareham, N.J.; Smith, R.D.; Harvey, I.M.; Day, N.E. Fruit and vegetable consumption and self-reported functional health in men and women in the european prospective investigation into cancer-norfolk (epic-norfolk): A population-based cross-sectional study. Public. Health. Nutr. 2007, 10, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Houston, D.K.; Stevens, J.; Cai, J.; Haines, P.S. Dairy, fruit, and vegetable intakes and functional limitations and disability in a biracial cohort: The atherosclerosis risk in communities study. Am. J. Clin. Nutr. 2005, 81, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, Y.; Kye, S.; Chung, Y.-S.; Kim, K.-M. Association of vegetables and fruits consumption with sarcopenia in older adults: The fourth korea national health and nutrition examination survey. Age. Ageing 2014, 44, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Blekkenhorst, L.C.; Hodgson, J.M.; Lewis, J.R.; Devine, A.; Woodman, R.J.; Lim, W.H.; Wong, G.; Zhu, K.; Bondonno, C.P.; Ward, N.C. Vegetable and fruit intake and fracture-related hospitalisations: A prospective study of older women. Nutrients 2017, 9, E511. [Google Scholar] [CrossRef] [PubMed]
- Prince, R.L.; Devine, A.; Dhaliwal, S.S.; Dick, I.M. Effects of calcium supplementation on clinical fracture and bone structure: Results of a 5-year, double-blind, placebo-controlled trial in elderly women. Arch. Intern. Med. 2006, 166, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Willett, W.C.; Staehelin, H.B.; Bazemore, M.G.; Zee, R.Y.; Wong, J.B. Effect of vitamin d on falls: A meta-analysis. JAMA Intern. Med. 2004, 291, 1999–2006. [Google Scholar] [CrossRef] [PubMed]
- Ireland, P.; Jolley, D.; Giles, G.; O’Dea, K.; Powles, J.; Rutishauser, I.; Wahlqvist, M.L.; Williams, J. Development of the melbourne ffq: A food frequency questionnaire for use in an australian prospective study involving an ethnically diverse cohort. Asia Pac. J. Clin. Nutr. 1994, 3, 19–31. [Google Scholar] [PubMed]
- Hodge, A.; Patterson, A.J.; Brown, W.J.; Ireland, P.; Giles, G. The anti cancer council of victoria ffq: Relative validity of nutrient intakes compared with weighed food records in young to middle-aged women in a study of iron supplementation. Aust. NZ J. Public. Health 2000, 24, 576–583. [Google Scholar] [CrossRef]
- Bruce, D.G.; Devine, A.; Prince, R.L. Recreational physical activity levels in healthy older women: The importance of fear of falling. J. Am. Geriatr. Soc. 2002, 50, 84–89. [Google Scholar] [CrossRef] [PubMed]
- McArdle, W.D.; Katch, F.I.; Katch, V.L. Nutrition, energy, and human performance. In Exercise Physiology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010. [Google Scholar]
- Britt, H.; Scahill, S.; Miller, G. Icpc plus© for community health? A feasibility study. Health. Inf. Manag. J. 1997, 27, 171–175. [Google Scholar] [CrossRef]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-A systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiology 2017, 46, 1029–1056. [Google Scholar] [CrossRef] [PubMed]
- Pennington, J.A.; Fisher, R.A. Classification of fruits and vegetables. J. Food Comp. Anal. 2009, 22, S23–S31. [Google Scholar] [CrossRef]
- Kiefte-de Jong, J.C.; Mathers, J.C.; Franco, O.H. Nutrition and healthy ageing: The key ingredients. Proc. Nutr. Soc. 2014, 73, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Vina, J.; Borras, C.; Miquel, J. Theories of ageing. Int. UN Biochem. Mol. Biol. Life 2007, 59, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fougère, B.; Boulanger, E.; Nourhashémi, F.; Guyonnet, S.; Cesari, M. Chronic inflammation: Accelerator of biological aging. J. Gerontol. Series A: Bio. Sci. Med. Sci. 2017, 72, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Deandrea, S.; Lucenteforte, E.; Bravi, F.; Foschi, R.; La Vecchia, C.; Negri, E. Risk factors for falls in community-dwelling older people: A systematic review and meta-analysis. Epidemiology 2010, 21, 658–668. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Kanaya, A.; Lindquist, K.; Simonsick, E.M.; Harris, T.; Shorr, R.I.; Tylavsky, F.A.; Newman, A.B. The metabolic syndrome, inflammation, and risk of cognitive decline. JAMA Arch. Intern. Med. 2004, 292, 2237–2242. [Google Scholar] [CrossRef] [PubMed]
- Brinkley, T.E.; Leng, X.; Miller, M.E.; Kitzman, D.W.; Pahor, M.; Berry, M.J.; Marsh, A.P.; Kritchevsky, S.B.; Nicklas, B.J. Chronic inflammation is associated with low physical function in older adults across multiple comorbidities. J. Gerontol. Ser. A Bio. Sci. Med. Sci. 2009, 64, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Pahor, M.; Bartali, B.; Cherubini, A.; Penninx, B.W.J.H.; Williams, G.R.; Atkinson, H.; Martin, A.; Guralnik, J.M.; Ferrucci, L. Antioxidants and physical performance in elderly persons: The invecchiare in chianti (inchianti) study. Am. J. Clin. Nutr. 2004, 79, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Al-Solaiman, Y.; Jesri, A.; Zhao, Y.; Morrow, J.D.; Egan, B.M. Low-sodium dash reduces oxidative stress and improves vascular function in salt-sensitive humans. J. Hum. Hypertens 2009, 23, 826. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Jones, D.P.; Goldberg, J.; Ziegler, T.R.; Bostick, R.M.; Wilson, P.W.; Manatunga, A.K.; Shallenberger, L.; Jones, L.; Vaccarino, V. Association between adherence to the mediterranean diet and oxidative stress. Am. J. Clin. Nutr. 2008, 88, 1364–1370. [Google Scholar] [PubMed]
- Thompson, H.J.; Heimendinger, J.; Diker, A.; O’Neill, C.; Haegele, A.; Meinecke, B.; Wolfe, P.; Sedlacek, S.; Zhu, Z.; Jiang, W. Dietary botanical diversity affects the reduction of oxidative biomarkers in women due to high vegetable and fruit intake. J. Nutr. 2006, 136, 2207–2212. [Google Scholar] [CrossRef] [PubMed]
- Holt, E.M.; Steffen, L.M.; Moran, A.; Basu, S.; Steinberger, J.; Ross, J.A.; Hong, C.-P.; Sinaiko, A.R. Fruit and vegetable consumption and its relation to markers of inflammation and oxidative stress in adolescents. J. Am. Diet. Assoc. 2009, 109, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age. Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef] [PubMed]
- Habauzit, V.; Horcajada, M.-N. Phenolic phytochemicals and bone. Phytochem Rev. 2008, 7, 313–344. [Google Scholar] [CrossRef]
- Banfi, G.; Iorio, E.L.; Corsi, M.M. Oxidative stress, free radicals and bone remodeling. Clin. Chem. Lab. Med. 2008, 46, 1550–1555. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Madyastha, P.; Bingel, S.; Ries, W.; Key, L. A new superoxide-generating oxidase in murine osteoclasts. J. Biol. Chem. 2001, 276, 5452–5458. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Michaëlsson, K.; Olofsson, H.; Johansson, S.; Melhus, H. Association between oxidative stress and bone mineral density. Biochem. Biophys. Res. Commun. 2001, 288, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Sahni, S.; Hannan, M.T.; Blumberg, J.; Cupples, L.A.; Kiel, D.P.; Tucker, K.L. Inverse association of carotenoid intakes with 4-y change in bone mineral density in elderly men and women: The framingham osteoporosis study. Am. J. Clin. Nutr. 2008, 89, 416–424. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, H.M.; New, S.A.; Golden, M.H.N.; Campbell, M.K.; Reid, D.M. Nutritional associations with bone loss during the menopausal transition: Evidence of a beneficial effect of calcium, alcohol, and fruit and vegetable nutrients and of a detrimental effect of fatty acids. Am. J. Clin. Nutr. 2004, 79, 155–165. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All Participants 1 | Vegetable Diversity 2 | |||
|---|---|---|---|---|
| ≤3 number/d | 4 number/d | ≥5 number/d | ||
| Number (%) | 1429 | 484 (34) | 440 (31) | 505 (35) |
| Demographics | ||||
| Age, years | 75.2 ± 2.7 | 75.3 ± 2.8 | 75.2 ± 2.7 | 75.0 ± 2.7 |
| Treatment group (calcium) 3 | 716 (50.1) | 240 (49.6) | 222 (50.6) | 254 (50.3) |
| Body mass index (BMI) 4, kg/m2 | 27.2 ± 4.8 | 27.3 ± 4.7 | 27.2 ± 4.9 | 27.1 ± 4.7 |
| Smoked ever 5 | 531 (37.4) | 179 (37.2) | 165 (37.7) | 187 (37.3) |
| Physical activity 4, kJ/day | 470.6 (0.0–746.3) | 451.5 (0.0–861.1) | 444.3 (149.5–821.4) | 865.5 (488.2–865.4) |
| Prevalent diabetes mellitus | 90 (6.3) | 36 (7.4) | 22 (5.0) | 32 (6.3) |
| Socioeconomic status 6 | ||||
| Top 10% most highly disadvantaged | 63 (4.4) | 21 (4.4) | 13 (3.0) | 29 (5.8) |
| Highly disadvantaged | 171 (12.1) | 65 (13.5) | 49 (11.2) | 57 (11.4) |
| Moderate-highly disadvantaged | 229 (16.2) | 81 (16.8) | 69 (15.8) | 79 (15.8) |
| Low-moderately disadvantaged | 216 (15.2) | 77 (16.0) | 63 (14.4) | 76 (15.2) |
| Low disadvantaged | 298 (21.0) | 96 (19.9) | 97 (22.2) | 105 (21.0) |
| Top 10% least disadvantaged | 440 (31.1) | 142 (29.5) | 145 (33.3) | 153 (30.7) |
| Dietary intakes | ||||
| Energy, kJ/day | 7102.3 ± 2078.1 | 6745.5 ± 2088.7 | 7177.4 ± 2056.5 | 7378.8 ± 2041.4 |
| Vegetable intake, g/day | 196.7 ± 79.3 | 128.5 ± 46.8 | 197.5 ± 49.4 | 261.3 ± 70.3 |
| Protein, g/day | 79.5 ± 26.6 | 73.6±26.9 | 80.6 ± 26.6 | 84.4 ± 25.2 |
| Calcium, mg/day | 954.0 ± 346.8 | 883.6 ± 340.9 | 973.5 ± 339.2 | 1004.5 ± 348.5 |
| Alcohol, g/day | 1.8 (0.3–9.8) | 1.4 (0.3–9.0) | 1.9 (0.3–9.2) | 2.2 (0.3–10.6) |
| HR per number/d Increase | P-Value | Vegetable diversity | |||||
|---|---|---|---|---|---|---|---|
| ≤3 number/d | 4 number/d | ≥5 number/d | p-Trend 2 | ||||
| Injurious Falls | Number | 1429 | - | 484 | 440 | 505 | - |
| Events, n (%) | 568 (39.7) | - | 206 (42.6) | 177 (40.2) | 185 (36.6) | - | |
| Age-adjusted | 0.91 (0.85–0.98) | 0.01 | 1.00 (Referent) | 0.86 (0.71–1.10) | 0.76 (0.62–0.93) | 0.01 | |
| Multivariable-adjusted 3 | 0.92 (0.86–0.99) | 0.02 | 1.00 (Referent) | 0.88 (0.71–1.08) | 0.77 (0.63–0.95) | 0.01 | |
| Fractures | Number | 1429 | - | 484 | 440 | 505 | - |
| Events, n (%) | 404 (28.3) | - | 153 (37.9) | 120 (29.7) | 131 (32.4) | - | |
| Age-adjusted | 0.90 (0.83–0.97) | 0.01 | 1.00 (Referent) | 0.79 (0.62–1.00) | 0.74 (0.59–0.93) | 0.01 | |
| Multivariable-adjusted 3 | 0.91 (0.84–0.99) | 0.03 | 1.00 (Referent) | 0.81 (0.64–1.04) | 0.78 (0.61–0.99) | 0.04 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sim, M.; Blekkenhorst, L.C.; Lewis, J.R.; Bondonno, C.P.; Devine, A.; Zhu, K.; Woodman, R.J.; Prince, R.L.; Hodgson, J.M. Vegetable Diversity, Injurious Falls, and Fracture Risk in Older Women: A Prospective Cohort Study. Nutrients 2018, 10, 1081. https://doi.org/10.3390/nu10081081
Sim M, Blekkenhorst LC, Lewis JR, Bondonno CP, Devine A, Zhu K, Woodman RJ, Prince RL, Hodgson JM. Vegetable Diversity, Injurious Falls, and Fracture Risk in Older Women: A Prospective Cohort Study. Nutrients. 2018; 10(8):1081. https://doi.org/10.3390/nu10081081
Chicago/Turabian StyleSim, Marc, Lauren C. Blekkenhorst, Joshua R. Lewis, Catherine P. Bondonno, Amanda Devine, Kun Zhu, Richard J. Woodman, Richard L. Prince, and Jonathan M. Hodgson. 2018. "Vegetable Diversity, Injurious Falls, and Fracture Risk in Older Women: A Prospective Cohort Study" Nutrients 10, no. 8: 1081. https://doi.org/10.3390/nu10081081