Iodine as Essential Nutrient during the First 1000 Days of Life


Abstract
1. Introduction
2. Methods
2.1. Thyroid Physiology in Pregnancy
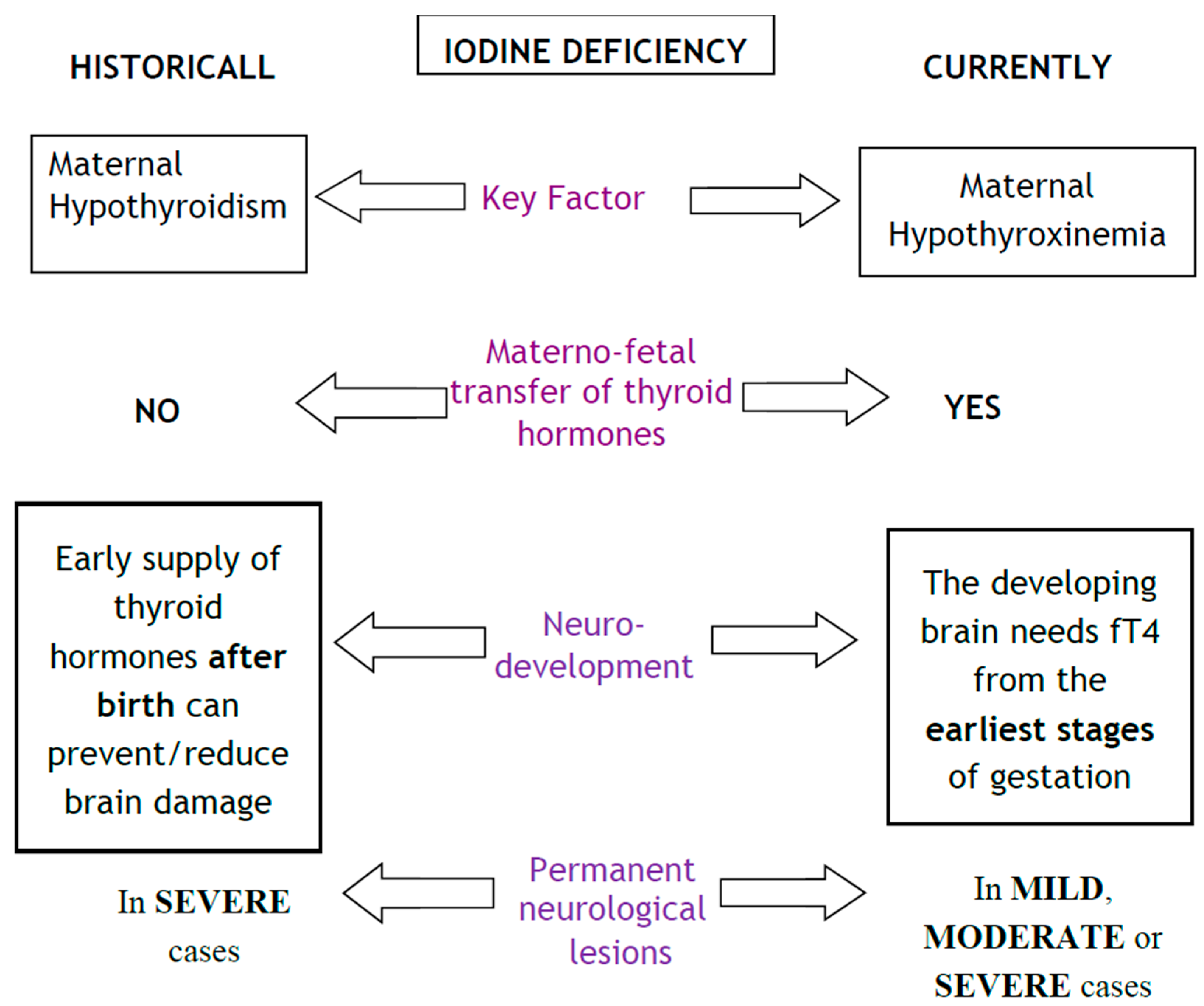
2.2. Changing the Paradigm of Pre-Natal Iodine Deficiency
2.3. Maternal–Foetal Transference of Iodine and Thyroid Hormones
2.4. Foetal Neurological Development and Consequences of Prenatal Iodine Deficiency
- -
- lack of damage at the encephalic trunk or spinal cord will prevent direct motor symptoms, but motor coordination will be altered [60];
- -
- lesions will affect higher-order integrative cortical areas with a poorly defined anatomical basis, including silent areas of the associative cortex [61];
- -
- there will be no clinical expression during the perinatal period, with later onset of symptoms during infancy or school age [57];
- -
- such lesions can hardly be detected by the current techniques for prenatal diagnosis such as ultrasounds or foetal MRI [62].
2.5. The Evolving Picture of Brain Damage Due to Iodine Deficiency
2.6. Iodine Deficiency and Foetal Programming
- -
- for both entities, the nutritional predisposing conditions are known;
- -
- the mechanisms that trigger morphological alterations are known; in both cases, the neuronal migration process is disturbed. In the case of NTD, neurones are stopped in their migration to the neural crest, whereas in iodine deficiency, neurones are stopped in their migration to the upper layers of cerebral cortex (Figure 2).
- -
- an effective prophylaxis is available, ideally from preconception to the end of neurogenesis.
2.7. Iodine Deficiency during Early Childhood
3. Summary
Acknowledgments
Conflict of Interest
References
- Springer, D.; Jiskra, J.; Limanova, Z.; Zima, T.; Potlukova, E. Thyroid in pregnancy: From physiology to screening. Crit. Rev. Clin. Lab. Sci. 2017, 54, 102–116. [Google Scholar] [CrossRef] [PubMed]
- Forhead, A.J.; Fowden, A.L. Thyroid hormones in fetal growth and prepartum maturation. J. Endocrinol. 2014, 221, R87–R103. [Google Scholar] [CrossRef] [PubMed]
- Pearce, E.N.; Lazarus, J.H.; Moreno-Reyes, R.; Zimmermann, M.B. Consequences of iodine deficiency and excess in pregnant women: An overview of current knowns and unknowns. Am. J. Clin. Nutr. 2016, 104, 918S–923S. [Google Scholar] [CrossRef] [PubMed]
- Niwattisaiwong, S.; Burman, K.D.; Li-Ng, M. Iodine deficiency: Clinical implications. Cleve Clin. J. Med. 2017, 84, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Gizak, M.; Abbott, K.; Andersson, M.; Lazarus, J.H. Iodine deficiency in pregnant women in Europe. Lancet Diabetes Endocrinol. 2015, 3, 672–674. [Google Scholar] [CrossRef]
- Vanderpump, M.P. Epidemiology of iodine deficiency. Minerva Med. 2017, 108, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Hetzel, B.S. Iodine deficiency disorders (IDD) and their eradication. Lancet 1983, 2, 1126–1129. [Google Scholar] [CrossRef]
- Trumpff, C.; De Schepper, J.; Tafforeau, J.; Van Oyen, H.; Vanderfaeillie, J.; Vandevijvere, S. Mild iodine deficiency in pregnancy in Europe and its consequences for cognitive and psychomotor development of children: A review. J. Trace Elem. Med. Biol. 2013, 27, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P.; Bath, S.C. The new emergence of iodine deficiency in the UK: Consequences for child neurodevelopment. Ann. Clin. Biochem. 2015, 52, 705–708. [Google Scholar] [CrossRef] [PubMed]
- Lane, R.H. Fetal programming, epigenetics, and adult onset disease. Clin. Perinatol. 2014, 41, 815–831. [Google Scholar] [CrossRef] [PubMed]
- Baye, K.; Faber, M. Windows of opportunity for setting the critical path for healthy growth. Public Health Nutr. 2015, 18, 1715–1717. [Google Scholar] [CrossRef] [PubMed]
- Moleti, M.; Trimarchi, F.; Vermiglio, F. Thyroid physiology in pregnancy. Endocr. Pract. 2014, 20, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J.; Guadaño-Ferraz, A.; Morte, B. Thyroid hormone transporters—functions and clinical implications. Nat. Rev. Endocrinol. 2015, 11, 406–417. [Google Scholar] [CrossRef] [PubMed]
- Rovet, J.F. The role of thyroid hormones for brain development and cognitive function. Endocr. Dev. 2014, 26, 26–43. [Google Scholar] [CrossRef] [PubMed]
- Obregon, M.J.; Calvo, R.M.; Del Rey, F.E.; de Escobar, G.M. Ontogenesis of thyroid function and interactions with maternal function. Endocr. Dev. 2007, 10, 86–98. [Google Scholar] [PubMed]
- Tingi, E.; Syed, A.A.; Kyriacou, A.; Mastorakos, G.; Kyriacou, A. Benign thyroid disease in pregnancy: A state of the art review. J. Clin. Transl. Endocrinol. 2016, 6, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Oguz Kutlu, A.; Kara, C. Iodine deficiency in pregnant women in the apparently iodine-sufficient capital city of Turkey. Clin. Endocrinol. 2012, 77, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C.; Pop, V.J.; Furmidge-Owen, V.L.; Broeren, M.A.; Rayman, M.P. Thyroglobulin as a Functional Biomarker of Iodine Status in a Cohort Study of Pregnant Women in the United Kingdom. Thyroid 2016, 27, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Pharoah, P.O.; Buttfield, I.H.; Hetzel, B.S. Neurological damage to the fetus resulting from severe iodine deficiency during pregnancy. Lancet 1971, 1, 308–310. [Google Scholar] [CrossRef]
- Thilly, C.H.; Delange, F.; Lagasse, R.; Bourdoux, P.; Ramioul, L.; Berquist, H.; Ermans, A.M. Fetal hypothyroidism and maternal thyroid status in severe endemic goiter. J. Clin. Endocrinol. Metab. 1978, 47, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Lavado-Autric, R.; Ausó, E.; García-Velasco, J.V.; Arufe Mdel, C.; Escobar del Rey, F.; Berbel, P.; Morreale de Escobar, G. Early maternal hypothyroxinemia alters histogenesis and cerebral cortex cytoarchitecture of the progeny. J. Clin. Investig. 2003, 111, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Ausó, E.; Lavado-Autric, R.; Cuevas, E.; Del Rey, F.E.; Morreale De Escobar, G.; Berbel, P. A moderate and transient deficiency of maternal thyroid function at the beginning of fetal neocorticogenesis alters neuronal migration. Endocrinology 2004, 145, 4037–4047. [Google Scholar] [CrossRef] [PubMed]
- Opazo, M.C.; Gianini, A.; Pancetti, F.; Azkcona, G.; Alarcón, L.; Lizana, R.; Noches, V.; Gonzalez, P.A.; Porto, M.; Mora, S.; et al. Maternal hypothyroxinemia impairs spatial learning and synaptic nature and function in the offspring. Endocrinology 2008, 149, 5097–5106. [Google Scholar] [CrossRef] [PubMed]
- Babu, S.; Sinha, R.A.; Mohan, V.; Rao, G.; Pal, A.; Pathak, A.; Singh, M.; Godbole, M.M. Effect of hypothyroxinemia on thyroid hormone responsiveness and action during rat postnatal neocortical development. Exp. Neurol. 2011, 228, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Pinazo-Durán, M.D.; Pons-Vázquez, S.; Gallego-Pinazo, R.; Galbis Estrada, C.; Zanón-Moreno, V.; Vila Bou, V.; Sanz Solana, P. Thyroid hormone deficiency disrupts rat eye neurodevelopment. Brain Res. 2011, 1392, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Wang, Y.; Wang, Y.; Dong, J.; Min, H.; Song, B.; Teng, W.; Xi, Q.; Chen, J. Developmental hypothyroxinaemia induced by maternal mild iodine deficiency delays hippocampal axonal growth in the rat offspring. J. Neuroendocrinol. 2013, 25, 852–862. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, M.E.; Ramos, R.L.; McCloskey, D.P.; Goodman, J.H. Subcortical band heterotopia in rat offspring following maternal hypothyroxinaemia: Structural and functional characteristics. J. Neuroendocrinol. 2014, 26, 528–541. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, Y.; Dong, J.; Wei, W.; Song, B.; Min, H.; Yu, Y.; Lei, X.; Zhao, M.; Teng, W.; et al. Developmental hypothyroxinemia and hypothyroidism reduce proliferation of cerebellar granule neuron precursors in rat offspring by downregulation of the sonic hedgehog signaling pathway. Mol. Neurobiol. 2014, 49, 1143–1152. [Google Scholar] [CrossRef] [PubMed]
- Cisternas, P.; Louveau, A.; Bueno, S.M.; Kalergis, A.M.; Boudin, H.; Riedel, C.A. Gestational Hypothyroxinemia Affects Glutamatergic Synaptic Protein Distribution and Neuronal Plasticity Through Neuron-Astrocyte Interplay. Mol. Neurobiol. 2016, 53, 7158–7169. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, M.E.; Sanchez-Huerta, K.; Wood, C. Mild Thyroid Hormone Insufficiency during Development Compromises Activity-Dependent Neuroplasticity in the Hippocampus of Adult Male Rats. Endocrinology 2016, 157, 774–787. [Google Scholar] [CrossRef] [PubMed]
- Opazo, M.C.; González, P.A.; Flores, B.D.; Venegas, L.F.; Albornoz, E.A.; Cisternas, P.; Bohmwald, K.; Nieto, P.A.; Bueno, S.M.; Kalergis, A.M.; et al. Gestational Hypothyroxinemia Imprints a Switch in the Capacity of Astrocytes and Microglial Cells of the Offspring to React in Inflammation. Mol. Neurobiol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Bleichrodt, N.; Born, M.P. A meta-analysis of research on iodine and its relationship to cognitive development. In The Damaged Brain of Iodine Deficiency: Cognitive, Behavioral, Neuromotor and Educative Aspects; Standbury, J.B., Ed.; Cognizant Communication Corporation: New York, NY, USA, 1994; pp. 195–200. [Google Scholar]
- Verhoef, H.; West, C.E.; Bleichrodt, N.; Dekker, P.H.; Born, M.P. Effects of micronutrients during pregnancy and early infancy on mental and psychomotor development. In Micronutrient Deficiencies in the First Months of Life; Delange, F., West, J.K.P., Eds.; S. Karger AG: Basel, Switzerland, 2003; pp. 327–357. [Google Scholar]
- Qian, M.; Wang, D.; Watkins, W.E.; Gebski, V.; Yan, Y.Q.; Li, M.; Chen, Z.P. The effects of iodine on intelligence on children: A meta-analysis of studies conducted in China. Asia Pac. J. Clin. Nutr. 2005, 14, 32–42. [Google Scholar] [PubMed]
- Melse-Boonstra, A.; Jaiswal, N. Iodine deficiency in pregnancy, infancy and childhood and its consequences for brain development. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Skeaff, S.A. Iodine deficiency in pregnancy: The effect on neurodevelopment in the child. Nutrients 2011, 3, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Bougma, K.; Aboud, F.E.; Harding, K.B.; Marquis, G.S. Iodine and mental development of children 5 years old and under: A systematic review and meta-analysis. Nutrients 2013, 5, 1384–1416. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.J.; Anderson, A.J.; Gibson, R.A.; Makrides, M. Effect of iodine supplementation in pregnancy on child development and other clinical outcomes: A systematic review of randomized controlled trials. Am. J. Clin. Nutr. 2013, 98, 1241–1254. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.N.; Okosieme, O.E.; Dayan, C.M.; Lazarus, J.H. Therapy of endocrine disease: Impact of iodine supplementation in mild-to-moderate iodine deficiency: Systematic review and meta-analysis. Eur. J. Endocrinol. 2014, 170, R1–R15. [Google Scholar] [CrossRef] [PubMed]
- Lam, L.F.; Lawlis, T.R. Feeding the brain—The effects of micronutrient interventions on cognitive performance among school-aged children: A systematic review of randomized controlled trials. Clin. Nutr. 2017, 36, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.M.; Fealy, S.M.; Bisquera, A.; Smith, R.; Collins, C.E.; Evans, T.J.; Hure, A.J. Effects of Nutritional Interventions during Pregnancy on Infant and Child Cognitive Outcomes: A Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1265. [Google Scholar] [CrossRef] [PubMed]
- Haddow, J.E.; Palomaki, G.E.; Allan, W.C.; Williams, J.R.; Knight, G.J.; Gagnon, J.; O’Heir, C.E.; Mitchell, M.L.; Hermos, R.J.; Waisbren, S.E.; et al. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N. Engl. J. Med. 1999, 341, 549–555. [Google Scholar] [CrossRef] [PubMed]
- De Escobar, G.M.; Obregón, M.J.; del Rey, F.E. Iodine deficiency and brain development in the first half of pregnancy. Public Health Nutr. 2007, 10, 1554–1570. [Google Scholar] [CrossRef] [PubMed]
- Min, H.; Dong, J.; Wang, Y.; Wang, Y.; Teng, W.; Xi, Q.; Chen, J. Maternal Hypothyroxinemia-Induced Neurodevelopmental Impairments in the Progeny. Mol. Neurobiol. 2016, 53, 1613–1624. [Google Scholar] [CrossRef] [PubMed]
- Furnica, R.M.; Lazarus, J.H.; Gruson, D.; Daumerie, C. Update on a new controversy in endocrinology: Isolated maternal hypothyroxinemia. J. Endocrinol. Investig. 2015, 38, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Akturk, M.; Oruc, A.S.; Danisman, N.; Erkek, S.; Buyukkagnici, U.; Unlu, E.; Tazebay, U.H. Na+/I- symporter and type 3 iodothyronine deiodinase gene expression in amniotic membrane and placenta and its relationship to maternal thyroid hormones. Biol. Trace Elem. Res. 2013, 154, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Calvo, R.M.; Jauniaux, E.; Gulbis, B.; Asunción, M.; Gervy, C.; Contempré, B.; Morreale de Escobar, G. Fetal tissues are exposed to biologically relevant free thyroxine concentrations during early phases of development. J. Clin. Endocrinol. Metab. 2002, 87, 1768–1777. [Google Scholar] [CrossRef] [PubMed]
- Kester, M.H.; Martinez de Mena, R.; Obregon, M.J.; Marinkovic, D.; Howatson, A.; Visser, T.J.; Hume, R.; Morreale de Escobar, G. Iodothyronine levels in the human developing brain: Major regulatory roles of iodothyronine deiodinases in different areas. J. Clin. Endocrinol. Metab. 2004, 89, 3117–3128. [Google Scholar] [CrossRef] [PubMed]
- Maia, A.L.; Goemann, I.M.; Meyer, E.L.; Wajner, S.M. Deiodinases: The balance of thyroid hormone: Type 1 iodothyronine deiodinase in human physiology and disease. J. Endocrinol. 2011, 209, 283–297. [Google Scholar] [CrossRef] [PubMed]
- Strich, D.; Karavani, G.; Edri, S.; Gillis, D. TSH enhancement of FT4 to FT3 conversion is age dependent. Eur. J. Endocrinol. 2016, 175, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Dosiou, C.; Medici, M. Management of endocrine disease: Isolated maternal hypothyroxinemia during pregnancy: Knowns and unknowns. Eur. J. Endocrinol. 2017, 176, R21–R38. [Google Scholar] [CrossRef] [PubMed]
- Henrichs, J.; Ghassabian, A.; Peeters, R.P.; Tiemeier, H. Maternal hypothyroxinemia and effects on cognitive functioning in childhood: How and why? Clin. Endocrinol. 2013, 79, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Hynes, K.L.; Otahal, P.; Hay, I.; Burgess, J.R. Mild iodine deficiency during pregnancy is associated with reduced educational outcomes in the offspring: 9-year follow-up of the gestational iodine cohort. J. Clin. Endocrinol. Metab. 2013, 98, 1954–1962. [Google Scholar] [CrossRef] [PubMed]
- Abel, M.H.; Caspersen, I.H.; Meltzer, H.M.; Haugen, M.; Brandlistuen, R.E.; Aase, H.; Alexander, J.; Torheim, L.E.; Brantsæter, A.L. Suboptimal Maternal Iodine Intake Is Associated with Impaired Child Neurodevelopment at 3 Years of Age in the Norwegian Mother and Child Cohort Study. J. Nutr. 2017, 147, 1314–1324. [Google Scholar] [CrossRef] [PubMed]
- Zoeller, R.T.; Rovet, J. Timing of thyroid hormone action in the developing brain: Clinical observations and experimental findings. J. Neuroendocrinol. 2004, 16, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Stenzel, D.; Huttner, W.B. Role of maternal thyroid hormones in the developing neocortex and during human evolution. Front. Neuroanat. 2013, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Moog, N.K.; Entringer, S.; Heim, C.; Wadhwa, P.D.; Kathmann, N.; Buss, C. Influence of maternal thyroid hormones during gestation on fetal brain development. Neuroscience 2017, 342, 68–100. [Google Scholar] [CrossRef] [PubMed]
- Mohan, V.; Sinha, R.A.; Pathak, A.; Rastogi, L.; Kumar, P.; Pal, A.; Godbole, M.M. Maternal thyroid hormone deficiency affects the fetal neocorticogenesis by reducing the proliferating pool, rate of neurogenesis and indirect neurogenesis. Exp. Neurol. 2012, 237, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Kohwi, M.; Doe, C.Q. Temporal fate specification and neural progenitor competence during development. Nat. Rev. Neurosci. 2013, 14, 823–838. [Google Scholar] [CrossRef] [PubMed]
- Williams, G.R. Neurodevelopmental and Neurophysiological actions of thyroid hormone. J. Neuroendocrinol. 2009, 20, 784–794. [Google Scholar] [CrossRef] [PubMed]
- Berbel, P.; Navarro, D.; Román, G.C. An evo-devo approach to thyroid hormones in cerebral and cerebellar cortical development: Etiological implications for autism. Front. Endocrinol. (Lausanne) 2014, 5, 146. [Google Scholar] [CrossRef] [PubMed]
- Valdés Hernández, M.C.; Wilson, K.L.; Combet, E.; Wardlaw, J.M. Brain Findings Associated with Iodine Deficiency identified by Magnetic Resonance Methods: A Systematic Review. Open J. Radiol. 2013, 3, 180–195. [Google Scholar] [CrossRef]
- Li, M.; Eastman, C.J. The changing epidemiology of iodine deficiency. Nat. Rev. Endocrinol. 2012, 8, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Moleti, M.; Sturniolo, G.; Trimarchi, F.; Vermiglio, F. The changing phenotype of iodine deficiency disorders: A review of thirty-five years of research in north-eastern Sicily. Ann. lst. Super. Sanita 2016, 52, 550–557. [Google Scholar] [CrossRef]
- Gowachirapant, S.; Jaiswal, N.; Melse-Boonstra, A.; Galetti, V.; Stinca, S.; Mackenzie, I.; Thomas, S.; Thomas, T.; Winichagoon, P.; Srinivasan, K.; et al. Effect of iodine supplementation in pregnant women on child neurodevelopment: A randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017, 5, 853–863. [Google Scholar] [CrossRef]
- Bath, S.C. Iodine supplementation in pregnancy in mildly deficient regions. Lancet Diabetes Endocrinol. 2017, 5, 840–841. [Google Scholar] [CrossRef]
- Bath, S.C.; Steer, C.D.; Golding, J.; Emmett, P.; Rayman, M.P. Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: Results from the Avon Longitudinal Study of Parents and Children (ALSPAC). Lancet 2013, 382, 331–337. [Google Scholar] [CrossRef]
- Hynes, K.L.; Otahal, P.; Burgess, J.R.; Oddy, W.H.; Hay, I. Reduced Educational Outcomes Persist into Adolescence Following Mild Iodine Deficiency in Utero, Despite Adequacy in Childhood: 15-Year Follow-Up of the Gestational Iodine Cohort Investigating Auditory Processing Speed and Working Memory. Nutrients 2017, 9, 1354. [Google Scholar] [CrossRef] [PubMed]
- Ghassabian, A.; Steenweg-de Graaff, J.; Peeters, R.P.; Ross, H.A.; Jaddoe, V.W.; Hofman, A.; Verhulst, F.C.; White, T.; Tiemeier, H. Maternal urinary iodine concentration in pregnancy and children’s cognition: Results from a population-based birth cohort in an iodine-sufficient area. BMJ Open 2014, 4, e005520. [Google Scholar] [CrossRef] [PubMed]
- Fetene, D.M.; Betts, K.S.; Alati, R. Mechanisms in Endocrinology: Maternal thyroid dysfunction during pregnancy and behavioural and psychiatric disorders of children: A systematic review. Eur. J. Endocrinol. 2017, 177, R261–R273. [Google Scholar] [CrossRef] [PubMed]
- Andersen, S.L.; Laurberg, P.; Wu, C.S.; Olsen, J. Attention deficit hyperactivity disorder and autism spectrum disorder in children born to mothers with thyroid dysfunction: A Danish nationwide cohort study. BJOG 2014, 121, 1365–1374. [Google Scholar] [CrossRef] [PubMed]
- Vermiglio, F.; Lo Presti, V.P.; Moleti, M.; Sidoti, M.; Tortorella, G.; Scaffidi, G.; Castagna, M.G.; Mattina, F.; Violi, M.A.; Crisà, A.; et al. Attention deficit and hyperactivity disorders in the offspring of mothers exposed to mild-moderate iodine deficiency: A possible novel iodine deficiency disorder in developed countries. J. Clin. Endocrinol. Metab. 2004, 89, 6054–6060. [Google Scholar] [CrossRef] [PubMed]
- Oostenbroek, M.H.W.; Kersten, R.H.J.; Tros, B.; Kunst, A.E.; Vrijkotte, T.G.M.; Finken, M.J.J. Maternal hypothyroxinaemia in early pregnancy and problem behavior in 5-year-old offspring. Psychoneuroendocrinology 2017, 81, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Modesto, T.; Tiemeier, H.; Peeters, R.P.; Jaddoe, V.W.; Hofman, A.; Verhulst, F.C.; Ghassabian, A. Maternal Mild Thyroid Hormone Insufficiency in Early Pregnancy and Attention-Deficit/Hyperactivity Disorder Symptoms in Children. JAMA Pediatr. 2015, 169, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Abel, M.H.; Ystrom, E.; Caspersen, I.H.; Meltzer, H.M.; Aase, H.; Torheim, L.E.; Askeland, R.B.; Reichborn-Kjennerud, T.; Brantsæter, A.L. Maternal Iodine Intake and Offspring Attention-Deficit/Hyperactivity Disorder: Results from a Large Prospective Cohort Study. Nutrients 2017, 9, 1239. [Google Scholar] [CrossRef] [PubMed]
- Moleti, M.; Trimarchi, F.; Tortorella, G.; Candia Longo, A.; Giorgianni, G.; Sturniolo, G.; Alibrandi, A.; Vermiglio, F. Effects of Maternal Iodine Nutrition and Thyroid Status on Cognitive Development in Offspring: A Pilot Study. Thyroid 2016, 26, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Román, G.C.; Ghassabian, A.; Bongers-Schokking, J.J.; Jaddoe, V.W.; Hofman, A.; de Rijke, Y.B.; Verhulst, F.C.; Tiemeier, H. Association of gestational maternal hypothyroxinemia and increased autism risk. Ann. Neurol. 2013, 74, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Van Mil, N.H.; Tiemeier, H.; Bongers-Schokking, J.J.; Ghassabian, A.; Hofman, A.; Hooijkaas, H.; Jaddoe, V.W.; de Muinck Keizer-Schrama, S.M.; Steegers, E.A.; Visser, T.J.; et al. Low urinary iodine excretion during early pregnancy is associated with alterations in executive functioning in children. J. Nutr. 2012, 142, 2167–2174. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, K.J.; Meaney, M.J. Fetal Origins of Mental Health: The Developmental Origins of Health and Disease Hypothesis. Am. J. Psychiatry. 2017, 174, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; You, S.H.; Williams, A.; Wade, M.G.; Yauk, C.L.; Thomas Zoeller, R. Transient Maternal Hypothyroxinemia Potentiates the Transcriptional Response to Exogenous Thyroid Hormone in the Fetal Cerebral Cortex Before the Onset of Fetal Thyroid Function: A Messenger and MicroRNA Profiling Study. Cereb. Cortex 2015, 25, 1735–1745. [Google Scholar] [CrossRef] [PubMed]
- Black, M.M.; Walker, S.P.; Fernald, L.C.H.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early childhood development coming of age: Science through the life course. Lancet 2017, 389, 77–90. [Google Scholar] [CrossRef]
- John, C.C.; Black, M.M.; Nelson, C.A., 3rd. Neurodevelopment: The Impact of Nutrition and Inflammation during Early to Middle Childhood in Low-Resource Settings. Pediatrics 2017, 139, S59–S71. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C. Direct or indirect iodine supplementation of infants? Lancet Diabetes Endocrinol. 2014, 2, 184–185. [Google Scholar] [CrossRef]
- Hess, S.Y. The impact of common micronutrient deficiencies on iodine and thyroid metabolism: The evidence from human studies. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 117–132. [Google Scholar] [CrossRef] [PubMed]
- Bouhouch, R.R.; Bouhouch, S.; Cherkaoui, M.; Aboussad, A.; Stinca, S.; Haldimann, M.; Andersson, M.; Zimmermann, M.B. Direct iodine supplementation of infants versus supplementation of their breastfeeding mothers: A double-blind, randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2014, 2, 197–209. [Google Scholar] [CrossRef]
- Britto, P.R.; Lye, S.J.; Proulx, K.; Yousafzai, A.K.; Matthews, S.G.; Vaivada, T.; Perez-Escamilla, R.; Rao, N.; Ip, P.; Fernald, L.C.H.; et al. Nurturing care: Promoting early childhood development. Lancet 2017, 389, 91–102. [Google Scholar] [CrossRef]
- Daelmans, B.; Darmstadt, G.L.; Lombardi, J.; Black, M.M.; Britto, P.R.; Lye, S.; Dua, T.; Bhutta, Z.A.; Richter, L.M.; Lancet Early Childhood Development Series Steering Committee. Early childhood development: The foundation of sustainable development. Lancet 2017, 389, 9–11. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Design | Structural Alterations | Functional or Clinical Consequences | |
|---|---|---|---|
| Lavado-Autric (2003) [21] | Rat dams fed a low iodine diet | Significant proportion of neurons found at locations that were aberrant or inappropriate with respect to birth date | Alteration in foetal brain histogenesis and cytoarchitecture might explain cognitive impairment in the progeny |
| Ausó (2004) [22] | Inducement of mild and transient hypothyroxinemia in rat dams by methimazole (MMI) | The cytoarchitecture and the radial distribution of neurons was significantly affected in the somatosensory cortex and hippocampus | Increased frequency of abnormal responses to acoustic stimulus Susceptibility to audiogenic seizures |
| Opazo (2008) [23] | Inducement of maternal hypothyroxinemia in rat dams by MMI | A significant reduction in the capacity of the brain for spatial learning Impaired dendrite and synapse stability Detrimental changes in long-term potentiation, affecting cognitive processes | Impaired learning capacity, prolonged latency of learning process |
| Babu (2011) [24] | Rat dams were fed a low iodine diet and given 1% KClO4 in drinking water (to lower the iodine content in the thyroid gland) | Significant decrease in myelin basic protein (MBP) and mitochondrial gene for cytochrome c oxidase III (Cox III) levels during neocortical development Increased number of apoptotic neurons distributed in all the layers of the neocortex | Thyroid hormone responsiveness in postnatal cortex is more sensitive to decrease in T4 than T3 concentration |
| Pinazo-Durán (2011) [25] | A rat model of controlled thyroid hormone deficiency | Delayed glial development and myelination in optic nerve | Reduction in the volume of the eye and optic nerve cross-sectional area Thinning of the retinal layers |
| Wei (2013) [26] | Four groups of rat dams: control group, mild ID, severe ID and MMI-treatment group | Impaired growth of axonal-related proteins Delayed axonal growth in hippocampus Damage of the morphological axon in the developing hippocampus | The deficits in axonal development might promote axonal regeneration in the hippocampus, but this process might not fully compensate for the damage induced by low thyroxine. |
| Gilbert (2014) [27] | Rat dams were exposed to propylthiouracil (PTU) in their drinking water to inhibit the thyroid hormone synthesis | Presence of subcortical-band heterotopia (SBH), a type of neuronal migration error resulting in neurones, oligodendrocytes and microglia in the corpus callosum of the offspring. | SBH in humans is an important type of malformation often associated with intractable epilepsy of childhood. |
| Wang (2014) [28] | A maternal hypothyroxinemia model (using mild ID diet) and two maternal hypothyroidism models (through a severe ID diet and MMI water respectively) | Reduced proliferation of cerebellar granule neuron precursors (CGNPs) Decreased total dendritic length of Purkinje cells (the most important neurons in the cerebellum) | Affected motor coordination and motor activity in which the cerebellum plays a critical role. |
| Cisternas (2016) [29] | Inducement of maternal hypothyroxinemia in rat dams by MMI | Affected synaptic protein distribution and impaired neuronal function. This deleterious effect is dependent on astrocyte and neuron integrity. | Affected neuronal plasticity which is dependent on interplay between astrocytes and neurons. |
| Gilbert (2016) [30] | Rat dams were exposed to propylthiouracil (PTU) in their drinking water to inhibit thyroid hormone synthesis | Reduced expression of neurotrophins that are important for neural processing. Restricted activity-dependent induction of neuroplasticity in the hippocampus. Changes persisted into adulthood despite the return to euthyroidism. | Altered structural and functional pathways in both the developing and adult brain. |
| Opazo (2017) [31] | Inducement of maternal hypothyroxinemia in rat dams by MMI | Unbalanced reactivity of microglia (decreased) and astrocytes (increased) to inflammatory stimuli. | Astrocytes could react strongly in inflammation, inducing neuronal death in the central nervous system. |
| Year | N of Studies | N of Subjects | Comments | Conclusions | |
|---|---|---|---|---|---|
| Bleichrodt [32] | 1994 | 21 18 | 2676 2214 | Systematic review (21 studies) and meta-analysis (18 studies). Observational and intervention studies carried out from 1969 to 1991 were pooled | A number of studies point to a negative effect of ID on cognitive development in children and adults from seriously ID areas, but other studies do not clearly show such an effect. Meta-analysis: The difference between iodine-deficient and non-ID groups is 13.5 IQ points. |
| Verhoef [33] | 2003 | 12 15 | -- -- | Meta-analysis Observational and intervention studies were analysed separately. | Observational studies indicate that ID is associated with impaired cognitive development. ID in the first half of pregnancy is irreversible. |
| Qian [34] | 2004 | 37 | 12,291 | Meta-analysis of Chinese studies Analysis of observational studies, intervention studies both during and after pregnancy. | The damage to the intelligence of children exposed to severe ID was profound, demonstrated by a 12.5 IQ point loss; children recovered 8.7 IQ points with iodine supplementation or iodine sufficiency during and after pregnancy. |
| Melse-Boonstra [35] | 2010 | 7 | 615 | Review of controlled trials (most of them randomized) of iodine supplementation in children. | Iodine supplementation in school-aged children can reverse certain delays in cognitive performance. Iodine supplementation in early life may be more beneficial than supplementation at school age. |
| Skeaff [36] | 2011 | 8 | 844 | Review of intervention studies carried out in pregnant women in areas of mild-to-moderate ID. | There is a need for well-designed trials to determine the effect of iodine supplementation in mildly to moderately iodine-deficient pregnant women on child neurodevelopment. |
| Trumpff [8] | 2013 | 7 5 5 | 3660 425 935 | Three different reviews (all of European studies) of the effect on children’s cognitive/psychomotor development of:
| It is difficult to establish a direct link between maternal ID and maternal hypothyroxinemia, as well as between maternal ID and elevated neonatal TSH levels at birth. Some studies suggest that iodine supplementation from the first trimester until the end of pregnancy may decrease the risk of cognitive and psychomotor developmental delay in the offspring. |
| Bougma [37] | 2013 | 2 8 9 4 | 147 1943 2027 2441 | Systematic review and meta-analysis. Four different analyses:
| Iodine deficiency has a substantial impact of mental development. Average effect sizes were 6.9 to 10.2 IQ points lower in ID children than in iodine replete children. Quantifying more precisely the contribution of ID to delayed mental development in young children requires more well-designed RCTs, including trials on the role of iodized salt. |
| Zhou [38] | 2013 | 2 6 | 19,683 719 | Systematic review. 2 RCTs conducted in severe ID areas and 6 RCTs in mild-to-moderate ID regions. | Iodine supplementation during pregnancy or the peri-conceptional period in regions of severe ID reduced the risk of cretinism, but there were no improvements in childhood intelligence, gross development, growth or pregnancy outcomes, although there was an improvement in some motor functions. |
| Taylor [39] | 2014 | 17 | 641 | Systematic review and meta-analysis. 9 RCTs and 8 observational studies of iodine supplementation during pregnancy from mild-to-moderate ID regions. | Iodine supplementation improves some maternal thyroid indices and may benefit aspects of cognitive function in school-age children, even in marginally ID areas. |
| Lam [40] | 2017 | 2 | 494 | Systematic review. RCTs that evaluate the effect of iodine on cognitive performance or academic performance among children aged 4–18 were included. | Iodine supplementation achieved a significant improvement in non-verbal fluid intelligence in ID children but no significant change in memory. |
| Taylor [41] | 2017 | 3 | 507 | Systematic review and Meta-analysis. RCTs of iodine intervention during pregnancy. | There was no significant difference between the intervention and control groups for child cognition in any of the RCTs. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velasco, I.; Bath, S.C.; Rayman, M.P. Iodine as Essential Nutrient during the First 1000 Days of Life. Nutrients 2018, 10, 290. https://doi.org/10.3390/nu10030290
Velasco I, Bath SC, Rayman MP. Iodine as Essential Nutrient during the First 1000 Days of Life. Nutrients. 2018; 10(3):290. https://doi.org/10.3390/nu10030290
Chicago/Turabian StyleVelasco, Inés, Sarah C. Bath, and Margaret P. Rayman. 2018. "Iodine as Essential Nutrient during the First 1000 Days of Life" Nutrients 10, no. 3: 290. https://doi.org/10.3390/nu10030290
APA StyleVelasco, I., Bath, S. C., & Rayman, M. P. (2018). Iodine as Essential Nutrient during the First 1000 Days of Life. Nutrients, 10(3), 290. https://doi.org/10.3390/nu10030290