Suboptimal Iodine Status among Pregnant Women in the Oslo Area, Norway

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Population and Study Design
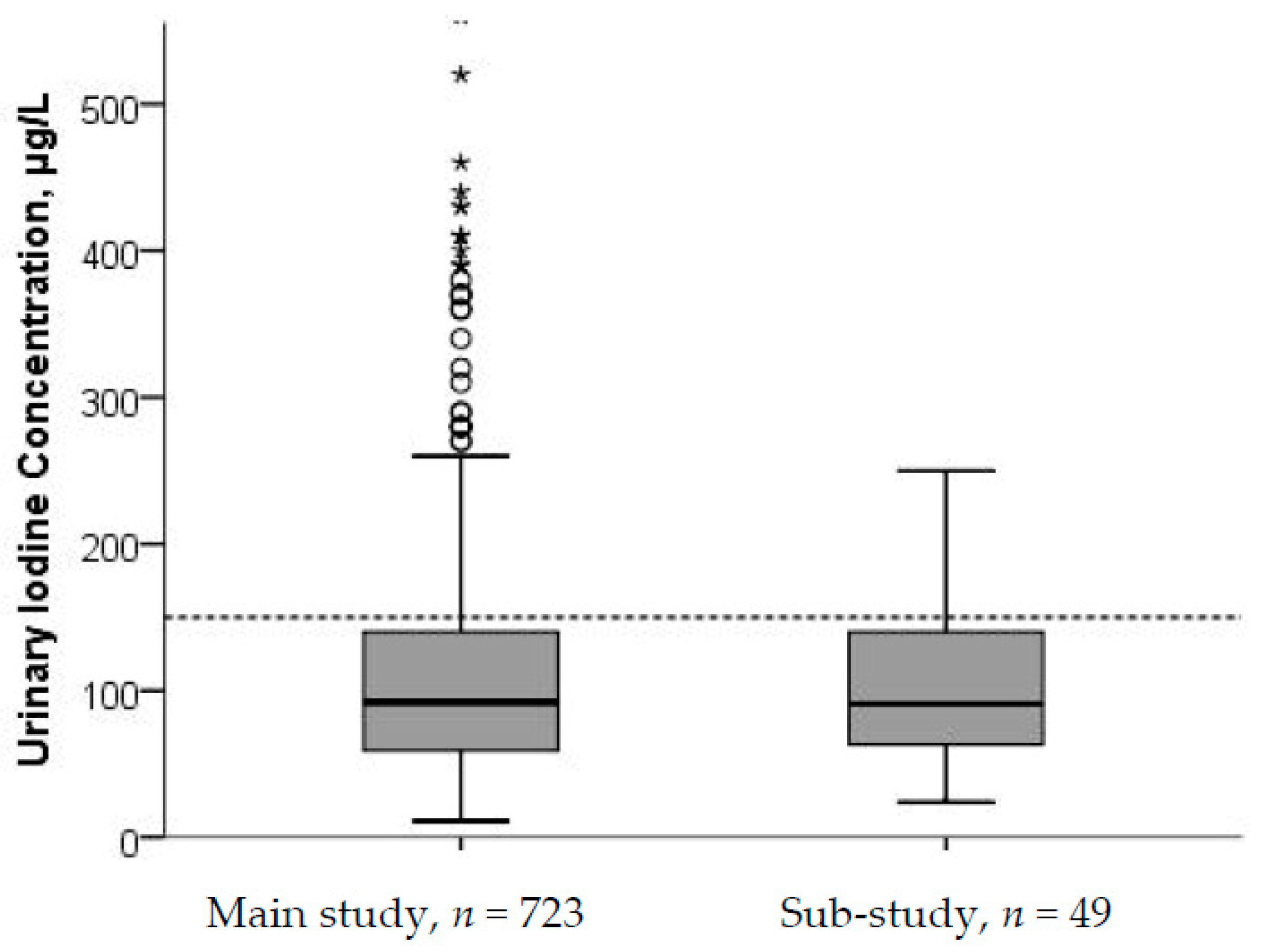
2.2. Urinary Iodine Concentration
2.3. Assessment of Iodine from Food and Dietary Supplements
2.4. Definitions of Iodine Status and Recommendations for Iodine Intake
2.5. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Abel, M.H.; Caspersen, I.H.; Meltzer, H.M.; Haugen, M.; Brandlistuen, R.E.; Aase, H.; Alexander, J.; Torheim, L.E.; Brantsaeter, A.L. Suboptimal Maternal Iodine Intake Is Associated with Impaired Child Neurodevelopment at 3 Years of Age in the Norwegian Mother and Child Cohort Study. J. Nutr. 2017, 147, 1314–1324. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C.; Steer, C.D.; Golding, J.; Emmett, P.; Rayman, M.P. Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: Results from the Avon Longitudinal Study of Parents and Children (ALSPAC). Lancet 2013, 382, 331–337. [Google Scholar] [CrossRef]
- Hynes, K.L.; Otahal, P.; Hay, I.; Burgess, J.R. Mild iodine deficiency during pregnancy is associated with reduced educational outcomes in the offspring: 9-year follow-up of the gestational iodine cohort. J. Clin. Endocrinol. Metab. 2013, 98, 1954–1962. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.N.; Okosieme, O.E.; Dayan, C.M.; Lazarus, J.H. Therapy of endocrine disease: Impact of iodine supplementation in mild-to-moderate iodine deficiency: Systematic review and meta-analysis. Eur. J. Endocrinol. 2014, 170, R1–R15. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO); The United Nations Children’s Fund (UNICEF); International Council for Control of Iodine Deficiency Disorders (ICCIDD). Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Pearce, E.N.; Lazarus, J.H.; Moreno-Reyes, R.; Zimmermann, M.B. Consequences of iodine deficiency and excess in pregnant women: An overview of current knowns and unknowns. Am. J. Clin. Nutr. 2016, 104 (Suppl. 3), S918–S923. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Karumbunathan, V.; Zimmermann, M.B. Global iodine status in 2011 and trends over the past decade. J. Nutr. 2012, 142, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Gizak, M.; Gorstein, J.; Andersson, M. Epidemiology of Iodine Deficiency in Iodine Deficiency Disorders and Their Elimination; Pearce, E.N., Ed.; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Nystrom, H.F.; Brantsaeter, A.L.; Erlund, I.; Gunnarsdottir, I.; Hulthen, L.; Laurberg, P.; Mattisson, I.; Rasmussen, L.B.; Virtanen, S.; Meltzer, H.M. Iodine status in the Nordic countries—Past and present. Food Nutr. Res. 2016, 60, 31969. [Google Scholar] [CrossRef] [PubMed]
- Brantsaeter, A.L.; Abel, M.H.; Haugen, M.; Meltzer, H.M. Risk of suboptimal iodine intake in pregnant Norwegian women. Nutrients 2013, 5, 424–440. [Google Scholar] [CrossRef] [PubMed]
- Henjum, S.; Lilleengen, A.M.; Aakre, I.; Dudareva, A.; Gjengedal, E.L.F.; Meltzer, H.M.; Brantsaeter, A.L. Suboptimal Iodine Concentration in Breastmilk and Inadequate Iodine Intake among Lactating Women in Norway. Nutrients 2017, 9, 643. [Google Scholar] [CrossRef] [PubMed]
- National Nutrition Council. The Risk of Iodine Deficeincy in Norway. Identification of an Acute Need for Action, in Norwegian; Technical Report; The Norwegian Directorate of Health: Oslo, Norway, 2016.
- Vejbjerg, P.; Knudsen, N.; Perrild, H.; Laurberg, P.; Carle, A.; Pedersen, I.B.; Rasmussen, L.B.; Ovesen, L.; Jorgensen, T. Thyroglobulin as a marker of iodine nutrition status in the general population. Eur. J. Endocrinol. 2009, 161, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Andersson, M. Assessment of iodine nutrition in populations: Past, present, and future. Nutr. Rev. 2012, 70, 553–570. [Google Scholar] [CrossRef] [PubMed]
- Lauritsen, J.; FoodCalc. Data Program from the Project “Diet, Cancer and Health” at the Danish Cancer Society, Denmark. Available online: http://ibt.ku.dk/jesper/foodcalc (accessed on 1 February 2005).
- Norwegian Food Safety Authority. The Norwegian Food Composition Table; The Norwegian Directorate of Health and University of Oslo: Oslo, Norway, 2016.
- Troan, G.; Dahl, L.; Meltzer, H.M.; Abel, M.H.; Indahl, U.G.; Haug, A.; Prestlokken, E. A model to secure a stable iodine concentration in milk. Food Nutr. Res. 2015, 59, 29829. [Google Scholar] [CrossRef] [PubMed]
- Kielland, E.; Dalane, J.Ø.; Håland, J.T.; Tharaldsen, A. Analyses of Eggs and Chicken, Nutrients and Environmental Contaminants, in Norwegian; The Norwegian Food Safety Authority: Oslo, Norway, 2016.
- Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; Institute of Medicine: Washington, DC, USA, 2001. [Google Scholar]
- Nordic Council of Ministers. Nordic Nutrition Recommendations; Nordic Council of Ministers: Copenhagen, Denmark, 2012. [Google Scholar]
- WHO Secretariat; Andersson, M.; de Benoist, B.; Delange, F.; Zupan, J. Prevention and control of iodine deficiency in pregnant and lactating women and in children less than 2-years-old: Conclusions and recommendations of the Technical Consultation. Public Health Nutr. 2007, 10, 1606–1611. [Google Scholar] [CrossRef] [PubMed]
- Skeaff, S.A. Iodine deficiency in pregnancy: The effect on neurodevelopment in the child. Nutrients 2011, 3, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B. The Importance of Adequate Iodine during Pregnancy and Infancy. World Rev. Nutr. Diet. 2016, 115, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Trumpff, C.; De Schepper, J.; Tafforeau, J.; Van Oyen, H.; Vanderfaeillie, J.; Vandevijvere, S. Mild iodine deficiency in pregnancy in Europe and its consequences for cognitive and psychomotor development of children: A review. J. Trace Elem. Med. Biol. 2013, 27, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, P.V.R. Urinary Iodine Concentration and Iodine Intake in Pregnant Norwegian Women. Results from the “Little in Norway” Study (LiN). Master’s Thesis, University of Bergen, Bergen, Norway, 2015. [Google Scholar]
- Berg, V.; Nost, T.H.; Skeie, G.; Thomassen, Y.; Berlinger, B.; Veyhe, A.S.; Jorde, R.; Odland, J.O.; Hansen, S. Thyroid homeostasis in mother-child pairs in relation to maternal iodine status: The MISA study. Eur. J. Clin. Nutr. 2017, 71, 1002–1007. [Google Scholar] [CrossRef] [PubMed]
- Dahl, L.; Meltzer, H.M.; Opsahl, J.A.; Julshamn, K. Iodine intake and status in two groups of Norwegians. Scand. J. Nutr. 2003, 47, 170–178. [Google Scholar] [CrossRef]
- Andersen, S.L.; Sorensen, L.K.; Krejbjerg, A.; Moller, M.; Laurberg, P. Challenges in the evaluation of urinary iodine status in pregnancy: The importance of iodine supplement intake and time of sampling. Eur. Thyroid J. 2014, 3, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Granfors, M.; Andersson, M.; Stinca, S.; Akerud, H.; Skalkidou, A.; Poromaa, I.S.; Wikstrom, A.K.; Nystrom, H.F. Iodine deficiency in a study population of pregnant women in Sweden. Acta Obstet. Gynecol. Scand. 2015, 94, 1168–1174. [Google Scholar] [CrossRef] [PubMed]
- The Norwegian Directorate of Health. Dietary Intake for Pregnant Women 2018. Available online: https://helsedirektoratet.no/folkehelse/graviditet-fodsel-og-barsel/graviditet-og-svangerskap/kosthold-for-gravide (accessed on 18 February 2018).
- Stagnaro-Green, A.; Sullivan, S.; Pearce, E.N. Iodine supplementation during pregnancy and lactation. JAMA 2012, 308, 2463–2464. [Google Scholar] [CrossRef] [PubMed]
- Pearce, E.N. Effects of iodine deficiency in pregnancy. J. Trace Elem. Med. Biol. 2012, 26, 131–133. [Google Scholar] [CrossRef] [PubMed]
- Dahl, L.; Johansson, L.; Julshamn, K.; Meltzer, H.M. The iodine content of Norwegian foods and diets. Public Health Nutr. 2004, 7, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Gunnarsdottir, I.; Dahl, L. Iodine intake in human nutrition: A systematic literature review. Food Nutr. Res. 2012, 56. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C.; Walter, A.; Taylor, A.; Wright, J.; Rayman, M.P. Iodine deficiency in pregnant women living in the South East of the UK: The influence of diet and nutritional supplements on iodine status. Br. J. Nutr. 2014, 111, 1622–1631. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.I.K.; Gregory, J.; Bates, C.J.; Prentice, A.; Perks, J.; Swan, G.; Farron, M. National Diet and Nutrition Survey: Adults Aged 19 to 64 Years. Vitamin and Mineral Intake and Urinary Analytes; The Stationery Office: London, UK, 2003. [Google Scholar]
- Grewal, E.; Khadgawat, R.; Gupta, N.; Desai, A.; Tandon, N. Assessment of iodine nutrition in pregnant north Indian subjects in three trimesters. Indian J. Endocrinol. Metab. 2013, 17, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Lindorfer, H.; Krebs, M.; Kautzky-Willer, A.; Bancher-Todesca, D.; Sager, M.; Gessl, A. Iodine deficiency in pregnant women in Austria. Eur. J. Clin. Nutr. 2015, 69, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Stilwell, G.; Reynolds, P.J.; Parameswaran, V.; Blizzard, L.; Greenaway, T.M.; Burgess, J.R. The influence of gestational stage on urinary iodine excretion in pregnancy. J. Clin. Endocrinol. Metab. 2008, 93, 1737–1742. [Google Scholar] [CrossRef] [PubMed]
- Brantsæter, A.L.; Knutsen, H.K.; Johansen, N.C.; Nyheim, K.A.; Erlund, I.; Meltzer, H.M.; Henjum, S. Inadequate Iodine Intake in Population Groups Defined by Age, Life Stage and Vegetarian Dietary Practice in a Norwegian Convenience Sample. Nutrients 2018, 10, 230. [Google Scholar] [CrossRef]
- Wiersinga, W.M. Smoking and thyroid. Clin Endocrinol. 2013, 79, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Hamrosi, M.A.; Wallace, E.M.; Riley, M.D. Iodine status in pregnant women living in Melbourne differs by ethnic group. Asia Pac. J. Clin. Nutr. 2005, 14, 27–31. [Google Scholar] [PubMed]
- Konig, F.; Andersson, M.; Hotz, K.; Aeberli, I.; Zimmermann, M.B. Ten repeat collections for urinary iodine from spot samples or 24-h samples are needed to reliably estimate individual iodine status in women. J. Nutr. 2011, 141, 2049–2054. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, N.; Christiansen, E.; Brandt-Christensen, M.; Nygaard, B.; Perrild, H. Age- and sex-adjusted iodine/creatinine ratio. A new standard in epidemiological surveys? Evaluation of three different estimates of iodine excretion based on casual urine samples and comparison to 24 h values. Eur. J. Clin. Nutr. 2000, 54, 361–363. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, R.M.; Vollset, S.E.; Gjessing, H.K.; Skjaerven, R.; Melve, K.K.; Schreuder, P.; Alsaker, E.R.; Haug, K.; Daltveit, A.K.; Magnus, P. Self-selection and bias in a large prospective pregnancy cohort in Norway. Paediatr. Perinat. Epidemiol. 2009, 23, 597–608. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Study (n = 804) | Main Study (n = 755) | Sub-Study (n = 49) |
|---|---|---|---|
| Age, years | 31.1 ± 4.4 | 31.1 ± 4.5 | 30.7 ± 3.5 |
| Pre-pregnancy BMI, kg/m2 | 22.8 (21.0–25.2) | 22.8 (20.9–25.3) | 22.5 (21.2–24.3) |
| Gestational weeks b | |||
| 1st trimester | 28 (3.5) | 27 (3.6) | 1 (2.0) |
| 2nd trimester | 344 (42.8) | 329 (43.6) | 15 (30.6) |
| 3rd trimester | 426 (53.0) | 393 (52.1) | 33 (67.3) |
| Parity | |||
| Nulliparous | 426 (53.0) | 384 (50.9) | 42 (85.7) |
| Primiparous | 296 (36.8) | 289 (38.3) | 7 (14.3) |
| Multiparous | 82 (10.2) | 82 (10.8) | 0 |
| Country of birth | |||
| Norway | 620 (77.1) | 579 (76.7) | 41 (83.7) |
| Other | 184 (22.9) | 176 (23.3) | 8 (16.3) |
| HDI birth country | |||
| Very high HDI | 710 (88.3) | 663 (87.8) | 46 (93.9) |
| High HDI | 37 (4.6) | 36 (4.8) | 2 (4.1) |
| Medium HDI | 23 (2.9) | 23 (3.0) | 0 |
| Low HDI | 30 (3.8) | 30 (4.0) | 0 |
| Relationship status | |||
| Cohabiting | 429 (53.4) | 393 (52.1) | 36 (73.5) |
| Married | 347 (43.2) | 336 (44.5) | 11 (22.4) |
| Single | 19 (2.4) | 19 (2.5) | 0 |
| Other | 9 (1.1) | 7 (0.9) | 2 (4.1) |
| Education | |||
| Lower secondary school | 25 (3.1) | 24 (3.2) | 1 (2.0) |
| Higher secondary school | 137 (17.0) | 133 (17.6) | 4 (8.2) |
| <4 years of University c | 334 (41.5) | 317 (42.0) | 17 (34.7) |
| ≥4 years of University c | 308 (38.3) | 281 (37.2) | 27 (55.1) |
| Employment status | |||
| Employed | 696 (86.6) | 653 (86.5) | 43 (87.8) |
| Stay at home/Unemployed | 30 (3.7) | 29 (3.8) | 1 (2.0) |
| Student | 38 (4.7) | 34 (4.5) | 4 (8.2) |
| Other | 30 (3.7) | 29 (3.8) | 1 (2.0) |
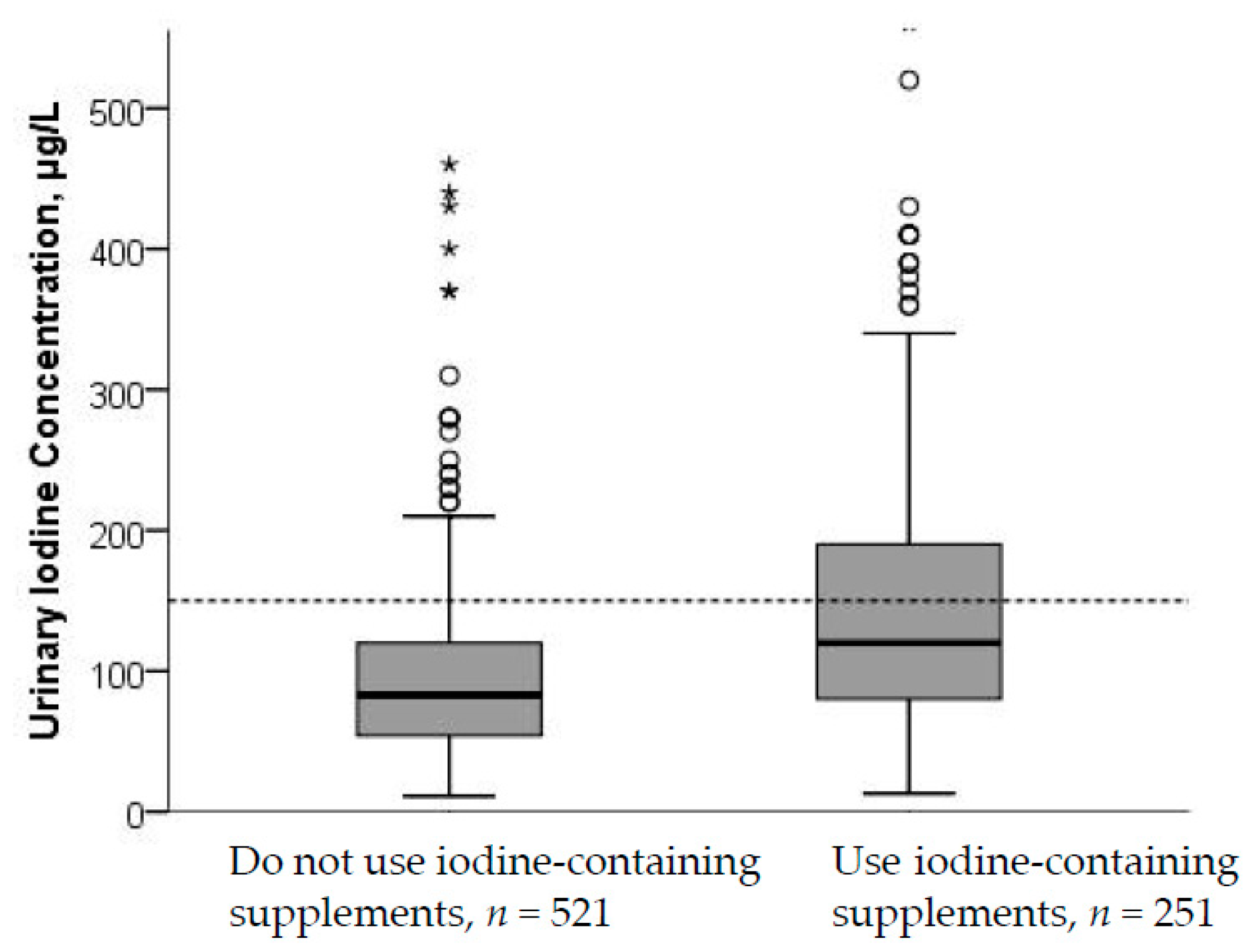
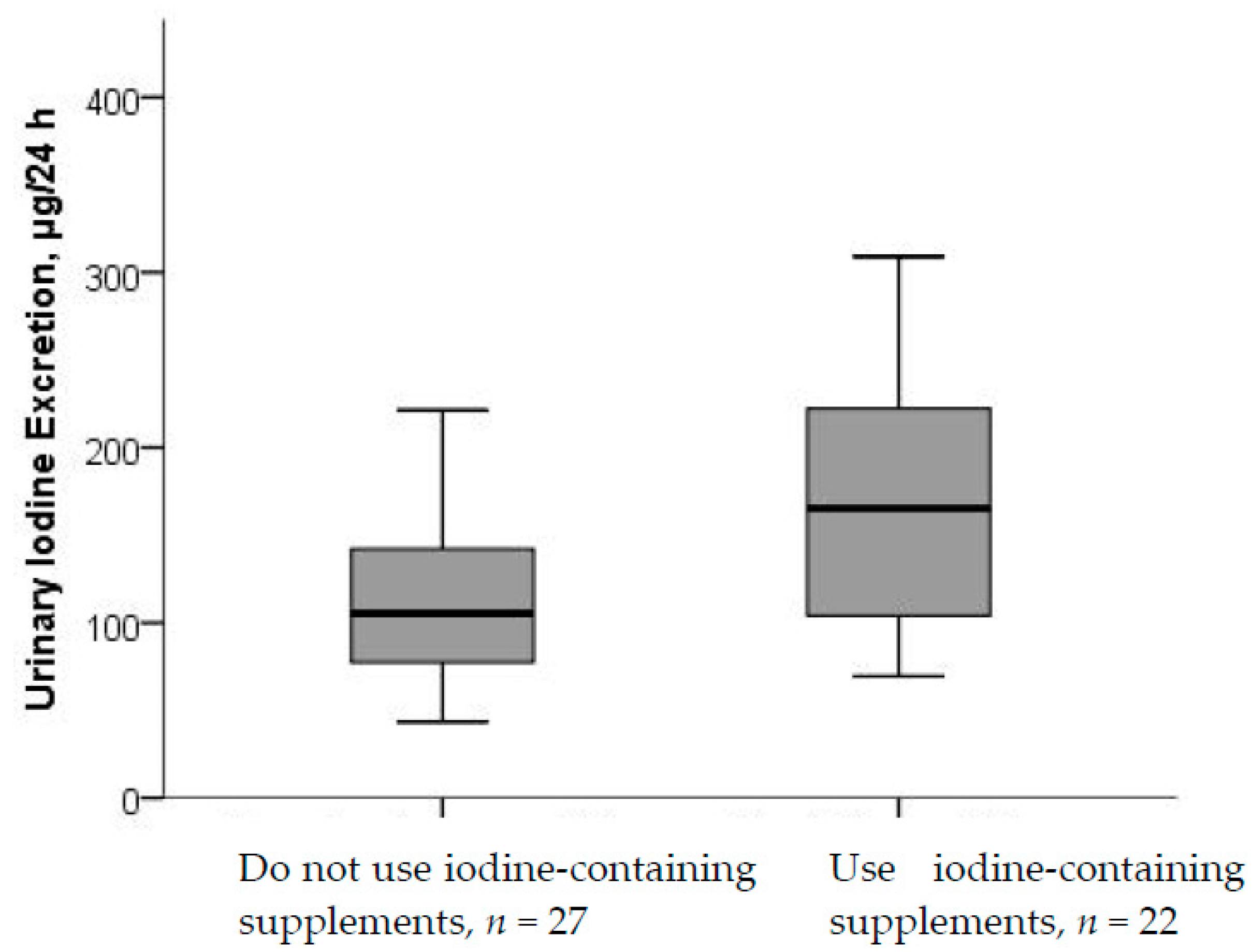
| Iodine supplement use | 263 (32.7) | 241 (31.9) | 22 (44.9) |
| Smoking during pregnancy | 10 (1.2) d | 10 (1.3) | 0 |
| Self-reported use of dry snuff | 10 (1.2) d | 10 (1.3) | 0 |
| Thyroid disease (self-reported) | 38 (4.7) | 34 (4.5) | 4 (8.1) |
| Hypothyroidism e | 32 (4.0) | 29 (3.8) | 3 (6.1) |
| Hyperthyroidism | 6 (0.7) | 5 (0.7) | 1 (2.0) |
| UIC (n = 777) | |||||
|---|---|---|---|---|---|
| UIC (μg/L) | Median | p25–p75 | Mean | SD | Min, Max |
| All trimesters (n = 777) | 92 | 59–140 | 114 | 86 | 11, 860 |
| 1st Trimester (n = 26) | 92 | 43–173 | 115 | 75 | 23, 280 |
| 2nd Trimester (n = 332) | 96 | 64–140 | 119 | 94 | 14, 860 |
| 3rd Trimester (n = 413) | 91 | 58–130 | 110 | 80 | 11, 660 |
| UIE (n = 49) | |||||
| UIC in 24-h urine (µg/L) | 91 | 61–140 | 103 | 54 | 24, 250 |
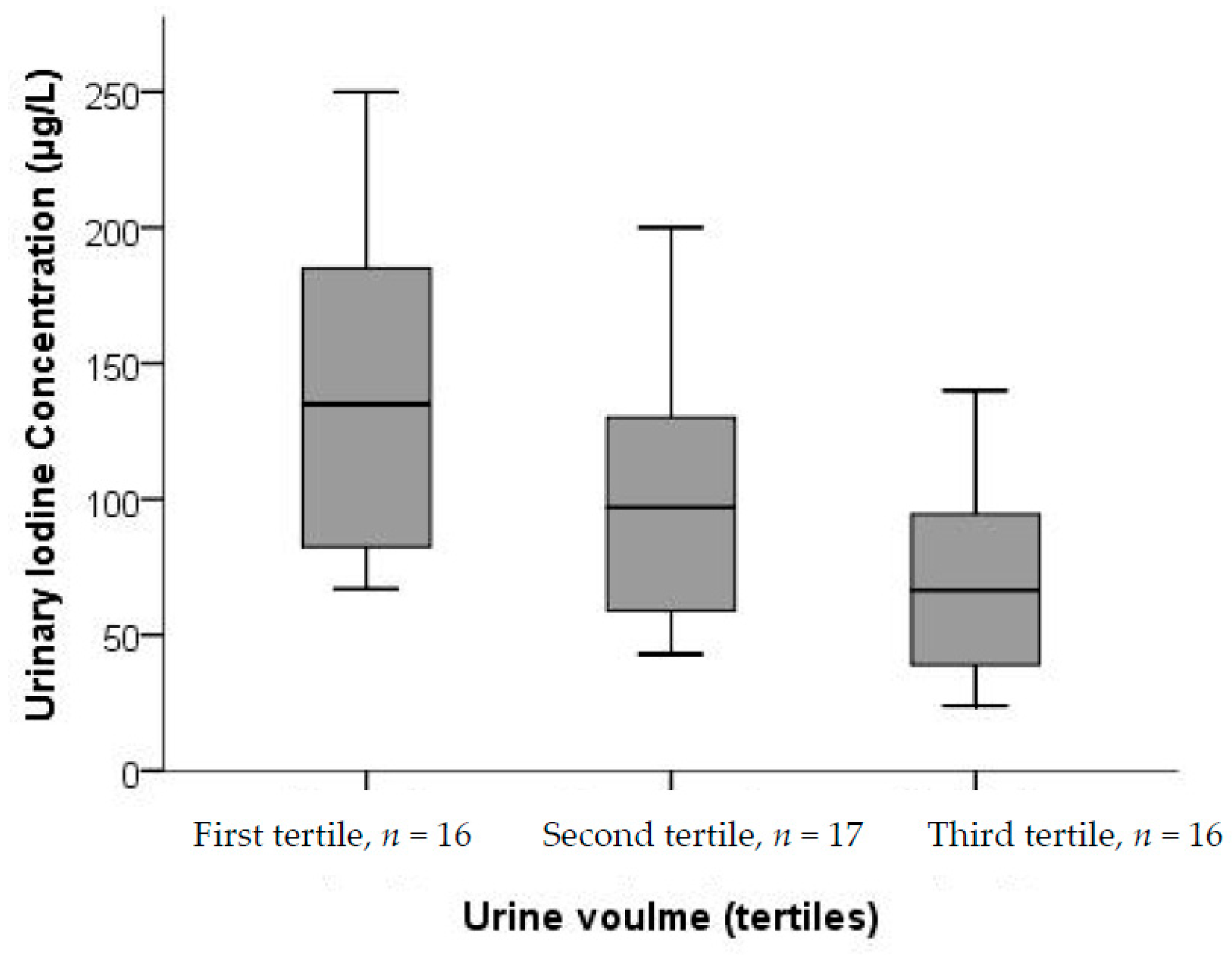
| Urine volume (L/24 h) | 1.4 | 1.1–1.8 | 1.5 | 0.5 | 0.5, 3.2 |
| UIE (µg/24 h) | 120 | 83–181 | 136 | 64 | 43, 309 |
| Main Study (n = 755) | |||||
|---|---|---|---|---|---|
| Iodine Intake (µg/day) | Median | p25–p75 | Mean | SD | Min, Max |
| 24-h intake from food a | 110 | 70–150 | 121 | 67 | 30, 667 |
| 24-h total intake b,§ | 148 | 86–251 | 175 | 105 | 30, 689 |
| Estimated intake from UIC | 145 | 89–214 | 176 | 133 | 16, 1183 |
| Sub-Study (n = 49) | |||||
| 24-h intake from food | 114 | 78–149 | 128 | 75 | 18, 403 |
| 24-h total intake c,§§ | 143 | 101–289 | 188 | 106 | 18, 403 |
| Habitual intake from food | 117 | 95–147 | 122 | 37 | 50, 206 |
| Habitual total intake d,§§ | 149 | 109–268 | 182 | 90 | 56, 361 |
| Estimated intake from UIC e | 157 | 103–257 | 193 | 122 | 103, 257 |
| Estimated intake from UIE e,f | 133 | 92–201 | 151 | 71 | 48, 343 |
| Predictor Variables | Unadjusted Coefficient (95% CI) | p | Adjusted Coefficient (95% CI) | p | Stand Beta |
|---|---|---|---|---|---|
| Constant | 4.181 (3.849, 4.513) | <0.001 | |||
| Maternal age | 0.015 (0.005, 0.025) | 0.004 | 0.013 (0.003, 0.022) | 0.011 | 0.088 |
| Gestational weeks | −0.004 (−0.010, 0.001) | 0.139 | −0.007 (−0.012, −0.001) | 0.019 | −0.081 |
| Hypothyroidism b | 0.291 (0.057, 0.525) | 0.015 | 0.313 (0.090, 0.536) | <0.001 | 0.289 |
| 24-h iodine Suppl c | 0.002 (0.001, 0.002) | <0.001 | 0.002 (0.002, 0.003) | 0.006 | 0.094 |
| Smoking d | −0.529 (−0.951, −0.108) | 0.014 | −0.442 (−0.869, −0.016) | 0.042 | −0.070 |
| R2 | 0.105 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henjum, S.; Aakre, I.; Lilleengen, A.M.; Garnweidner-Holme, L.; Borthne, S.; Pajalic, Z.; Blix, E.; Gjengedal, E.L.F.; Brantsæter, A.L. Suboptimal Iodine Status among Pregnant Women in the Oslo Area, Norway. Nutrients 2018, 10, 280. https://doi.org/10.3390/nu10030280
Henjum S, Aakre I, Lilleengen AM, Garnweidner-Holme L, Borthne S, Pajalic Z, Blix E, Gjengedal ELF, Brantsæter AL. Suboptimal Iodine Status among Pregnant Women in the Oslo Area, Norway. Nutrients. 2018; 10(3):280. https://doi.org/10.3390/nu10030280
Chicago/Turabian StyleHenjum, Sigrun, Inger Aakre, Anne Marie Lilleengen, Lisa Garnweidner-Holme, Sandra Borthne, Zada Pajalic, Ellen Blix, Elin Lovise Folven Gjengedal, and Anne Lise Brantsæter. 2018. "Suboptimal Iodine Status among Pregnant Women in the Oslo Area, Norway" Nutrients 10, no. 3: 280. https://doi.org/10.3390/nu10030280
APA StyleHenjum, S., Aakre, I., Lilleengen, A. M., Garnweidner-Holme, L., Borthne, S., Pajalic, Z., Blix, E., Gjengedal, E. L. F., & Brantsæter, A. L. (2018). Suboptimal Iodine Status among Pregnant Women in the Oslo Area, Norway. Nutrients, 10(3), 280. https://doi.org/10.3390/nu10030280