Serum Carotenoids Are Inversely Associated with RBP4 and Other Inflammatory Markers in Middle-Aged and Elderly Adults




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
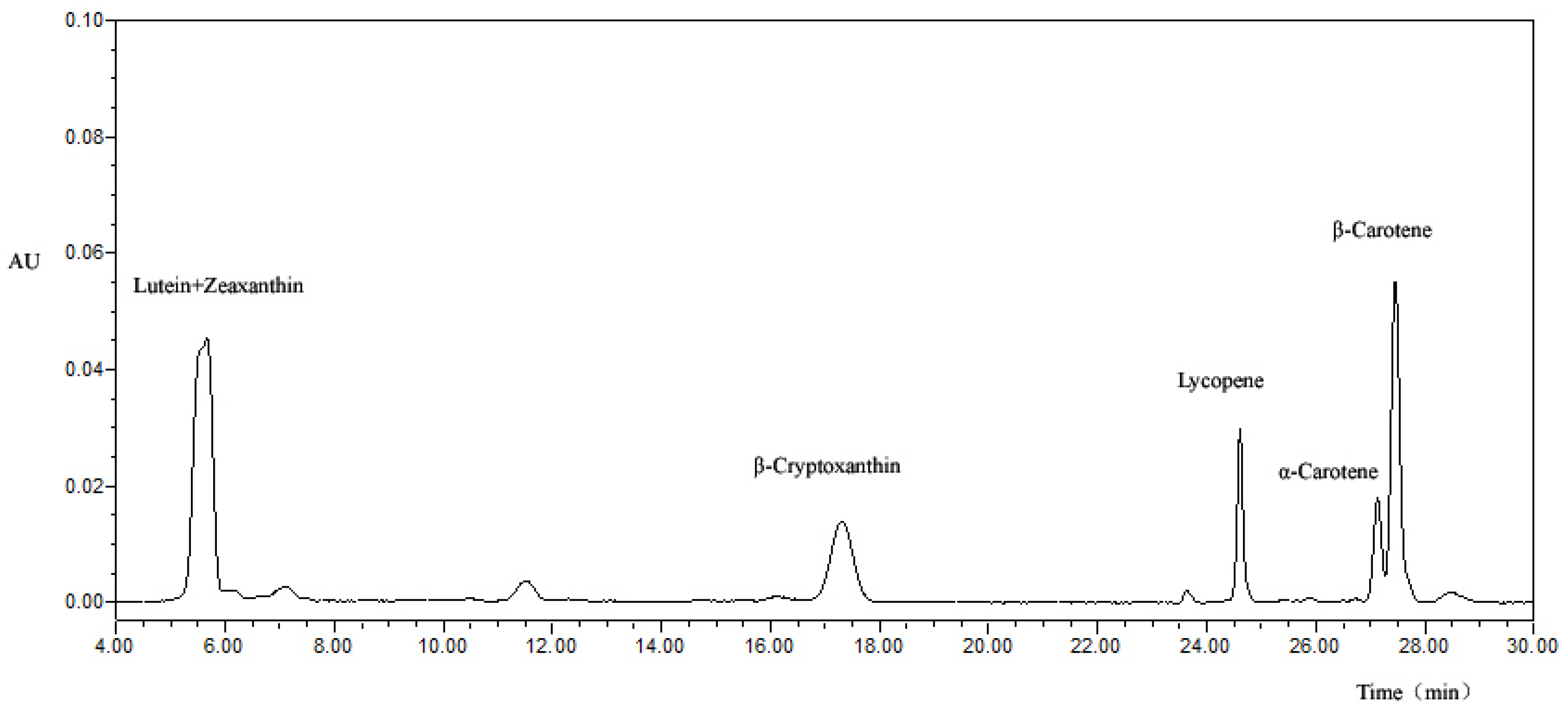
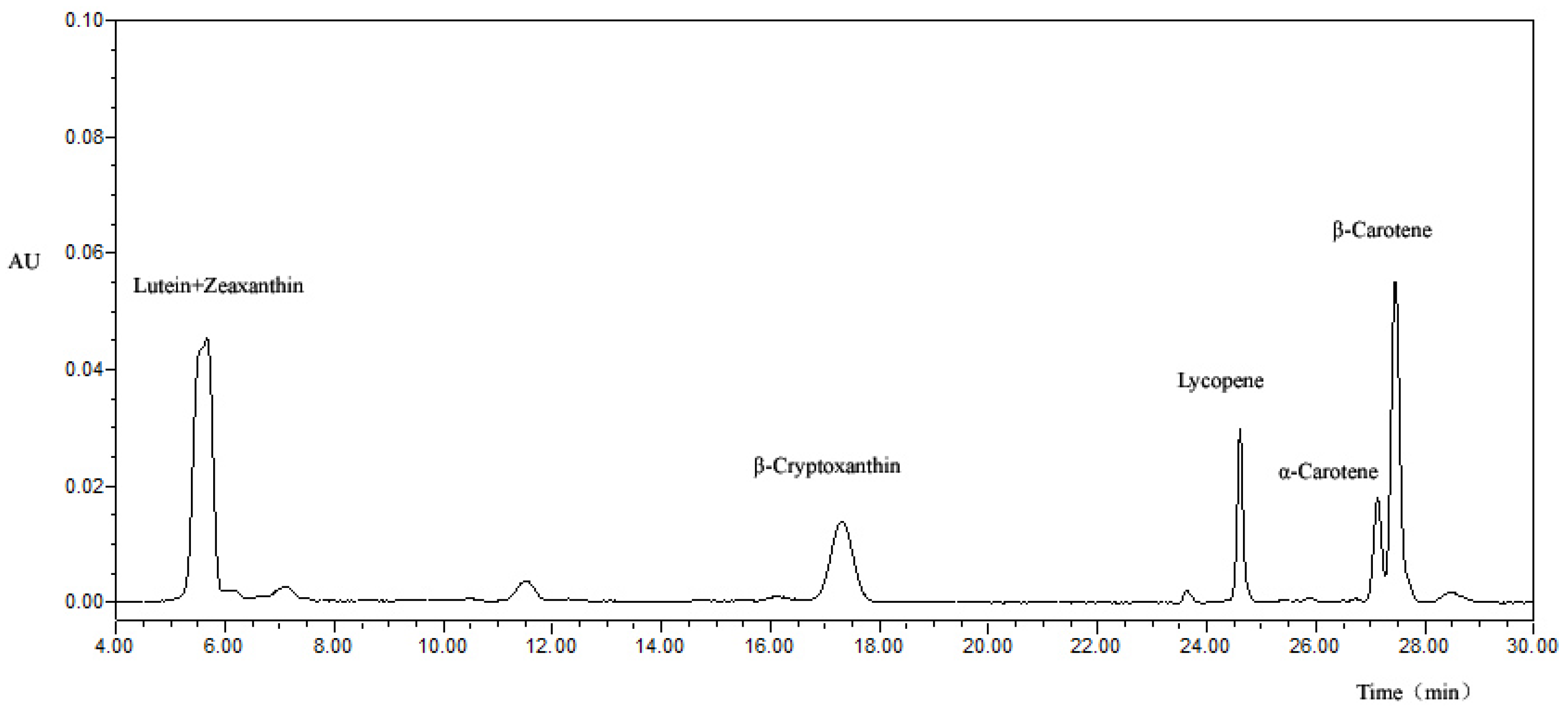
2.3. Measurement of Serum Carotenoids
2.4. Measurement of RBP4 and Inflammatory Markers
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Carotenoids, Other Dietary Factors and Blood RBP4
4.2. Carotenoids and Blood Inflammatory Markers
4.3. Relationship between RBP4 and Inflammatory Markers
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix

{kind=link}
| Age, Sex Adjusted M1 | Multivariate-Adjusted M2 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| aRBP4 d | RBP4 | hsCRP | MCP1 | IL6 | IL-1β | TNF-α | aRBP4 d | RBP4 | hsCRP | MCP1 | IL-6 | IL-1β | TNF-α | |
| Women | 1866 | 1866 | 1989 | 894 | 879 | 880 | 883 | 1866 | 1866 | 1989 | 894 | 879 | 880 | 883 |
| Total carotenoids e | −0.143 c | −0.112 c | −0.155 c | −0.043 | 0.035 | −0.002 | 0.001 | −0.111 c | −0.091 c | −0.107 c | −0.048 | 0.032 | −0.036 | −0.037 |
| Log total carotenoids | −0.146 c | −0.111 c | −0.146 c | −0.045 | 0.057 | 0.037 | 0.027 | −0.115 c | −0.093 c | −0.097 c | −0.052 | 0.051 | −0.010 | −0.026 |
| α-Carotene | −0.071 b | −0.058 a | −0.140 c | −0.068 a | −0.027 | −0.074 a | −0.075 a | −0.039 | −0.030 | −0.086 c | −0.054 | −0.009 | −0.055 | −0.053 |
| β-Carotene | −0.116 c | −0.095 c | −0.171 c | −0.064 | 0.039 | 0.039 | 0.028 | −0.079 c | −0.068 b | −0.110 c | −0.066 | 0.040 | 0.016 | −0.004 |
| β-Cryptoxanthin | −0.090 c | −0.073 b | −0.055 a | 0.014 | 0.091 b | 0.021 | 0.055 | −0.077 c | −0.069 b | −0.051 a | −0.005 | 0.072 a | −0.017 | 0.009 |
| Lycopene | −0.109 c | −0.088 c | −0.127 c | −0.002 | −0.009 | −0.023 | −0.017 | −0.082 c | −0.069 b | −0.086 c | −0.0004 | −0.011 | −0.033 | −0.028 |
| Lutein + zeaxanthin | −0.149 c | −0.106 c | −0.086 c | −0.042 | 0.035 | 0.028 | 0.012 | −0.130 c | −0.098 c | −0.056 b | −0.050 | 0.025 | −0.041 | −0.065 |
| Men | 866 | 866 | 930 | 414 | 411 | 410 | 412 | 866 | 866 | 930 | 414 | 411 | 410 | 412 |
| Total carotenoids e | −0.096 b | −0.059 | −0.165 c | −0.148 b | −0.06 | 0.013 | −0.041 | −0.068 | −0.043 | −0.123 c | −0.156 b | −0.087 | −0.029 | −0.099 a |
| Log total carotenoids | −0.105 b | −0.063 | −0.124 c | −0.121 a | −0.046 | 0.007 | −0.035 | −0.078 a | −0.047 | −0.088 b | −0.127 b | −0.072 | −0.042 | −0.100 a |
| α-Carotene | −0.076 a | −0.068 a | −0.206 c | −0.126 b | −0.074 | −0.029 | −0.088 | −0.052 | −0.049 | −0.160 c | −0.125 b | −0.076 | −0.015 | −0.079 |
| β-Carotene | −0.072 a | −0.062 | −0.134 c | −0.091 | −0.027 | −0.025 | −0.034 | −0.038 | −0.037 | −0.090 b | −0.096 | −0.051 | −0.074 | −0.089 |
| β-Cryptoxanthin | −0.055 | −0.019 | −0.067 a | −0.119 a | −0.061 | 0.038 | 0.048 | −0.040 | −0.016 | −0.044 | −0.126 a | −0.095 | −0.024 | −0.017 |
| Lycopene | −0.032 | −0.005 | −0.154 c | −0.128 b | −0.021 | 0.056 | −0.062 | −0.013 | 0.003 | −0.117 c | −0.125 b | −0.028 | 0.041 | −0.096 |
| Lutein + zeaxanthin | −0.121 c | −0.065 | −0.055 | −0.093 | −0.045 | 0.011 | −0.011 | −0.104 b | −0.057 | −0.036 | −0.098 a | −0.070 | −0.036 | −0.074 |
| Carotenoids (μmol/L) b | hsCRP (mg/L) | RBP4 (μg/mL) | ||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Total carotenoids | 0.31 (0.22–0.45) | <0.001 | 0.42 (0.29–0.61) | <0.001 | 0.42 (0.27–0.64) | <0.001 | 0.43 (0.27–0.67) | <0.001 |
| α-Carotene | 0.38 (0.29–0.49) | <0.001 | 0.48 (0.37–0.63) | <0.001 | 0.60 (0.43–0.82) | <0.001 | 0.64 (0.46–0.90) | 0.009 |
| β-Carotene | 0.39 (0.30–0.49) | <0.001 | 0.51 (0.40–0.67) | <0.001 | 0.64 (0.48–0.85) | <0.001 | 0.68 (0.50–0.93) | 0.015 |
| β-Cryptoxanthin | 0.72 (0.57–0.91) | 0.006 | 0.76 (0.59–0.97) | 0.029 | 0.70 (0.52–0.95) | <0.001 | 0.75 (0.55–1.01) | 0.060 |
| Lycopene | 0.38 (0.28–0.50) | <0.001 | 0.46 (0.34–0.62) | <0.001 | 0.54 (0.38–0.76) | <0.001 | 0.54 (0.38–0.77) | 0.001 |
| Lutein + zeaxanthin | 0.60 (0.43–0.83) | 0.002 | 0.73 (0.52–1.04) | 0.085 | 0.44 (0.29–0.65) | <0.001 | 0.44 (0.29–0.68) | <0.001 |
References
- Feghali, C.A.; Wright, T.M. Cytokines in acute and chronic inflammation. Front. Biosci. 1997, 2, 12–26. [Google Scholar]
- Abraham, G.; Sundaram, V.; Sundaram, V.; Mathew, M.; Leslie, N.; Sathiah, V. C-Reactive protein, a valuable predictive marker in chronic kidney disease. Saudi J. Kidney Dis. Transplant. 2009, 20, 811–815. [Google Scholar]
- Vermeire, S.; Van Assche, G.; Rutgeerts, P. C-reactive protein as a marker for inflammatory bowel disease. Inflamm. Bowel Dis. 2004, 10, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Libby, P. Inflammation in atherosclerosis. Nature 2002, 420, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Coyne, T.; Ibiebele, T.I.; Baade, P.D.; Dobson, A.; McClintock, C.; Dunn, S.; Leonard, D.; Shaw, J. Diabetes mellitus and serum carotenoids: Findings of a population-based study in Queensland, Australia. Am. J. Clin. Nutr. 2005, 82, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Hozawa, A.; Jacobs, D.R., Jr.; Steffes, M.W.; Gross, M.D.; Steffen, L.M.; Lee, D.H. Associations of serum carotenoid concentrations with the development of diabetes and with insulin concentration: Interaction with smoking: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Am. J. Epidemiol. 2006, 163, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, M.; Nakamura, M.; Ogawa, K.; Ikoma, Y.; Yano, M. High-serum carotenoids associated with lower risk for developing type 2 diabetes among Japanese subjects: Mikkabi cohort study. BMJ Open Diabetes Res. Care 2015, 3, e000147. [Google Scholar] [CrossRef] [PubMed]
- Riccioni, G.; D’Orazio, N.; Speranza, L.; Di Ilio, E.; Glade, M.; Bucciarelli, V.; Scotti, L.; Martini, F.; Pennelli, A.; Bucciarelli, T. Carotenoids and asymptomatic carotid atherosclerosis. J. Biol. Regul. Homeost. Agents 2010, 24, 447–452. [Google Scholar] [PubMed]
- Leermakers, E.T.; Darweesh, S.K.; Baena, C.P.; Moreira, E.M.; Melo van Lent, D.; Tielemans, M.J.; Muka, T.; Vitezova, A.; Chowdhury, R.; Bramer, W.M.; et al. The effects of lutein on cardiometabolic health across the life course: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2016, 103, 481–494. [Google Scholar] [CrossRef] [PubMed]
- Petyaev, I.M. Lycopene Deficiency in Ageing and Cardiovascular Disease. Oxid. Med. Cell. Longev. 2016, 2016, 3218605. [Google Scholar] [CrossRef] [PubMed]
- Baena Ruiz, R.; Salinas Hernández, P. Cancer chemoprevention by dietary phytochemicals: Epidemiological evidence. Maturitas 2016, 94, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Kaulmann, A.; Bohn, T. Carotenoids, inflammation, and oxidative stress—Implications of cellular signaling pathways and relation to chronic disease prevention. Nutr. Res. 2014, 34, 907–929. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chung, S.J.; McCullough, M.L.; Song, W.O.; Fernandez, M.L.; Koo, S.I.; Chun, O.K. Dietary carotenoids are associated with cardiovascular disease risk biomarkers mediated by serum carotenoid concentrations. J. Nutr. 2014, 144, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Gaziano, J.M.; Norkus, E.P.; Buring, J.E.; Sesso, H.D. Associations of plasma carotenoids with risk factors and biomarkers related to cardiovascular disease in middle-aged and older women. Am. J. Clin. Nutr. 2008, 88, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Inoue, T.; Hashimoto, S.; Ochiai, J.; Kusuhara, Y.; Ito, Y.; Hamajima, N. Association of serum carotenoids with high molecular weight adiponectin and inflammation markers among Japanese subjects. Clin. Chim. Acta 2010, 411, 1330–1334. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.D.; Strachan, A.A.; Thies, F.; Aucott, L.S.; Reid, D.M.; Hardcastle, A.C.; Mavroeidi, A.; Simpson, W.G.; Duthie, G.G.; Macdonald, H.M. Patterns of dietary intake and serum carotenoid and tocopherol status are associated with biomarkers of chronic low-grade systemic inflammation and cardiovascular risk. Br. J. Nutr. 2014, 112, 1341–1352. [Google Scholar] [CrossRef] [PubMed]
- Hozawa, A.; Jacobs, D.R.; Steffes, M.W.; Gross, M.D.; Steffen, L.M.; Lee, D.H. Relationships of circulating carotenoid concentrations with several markers of inflammation, oxidative stress, and endothelial dysfunction: The Coronary Artery Risk Development in Young Adults (CARDIA)/Young Adult Longitudinal Trends in Antioxidants (YALTA) study. Clin. Chem. 2007, 53, 447–455. [Google Scholar] [PubMed]
- Akdis, M.; Aab, A.; Altunbulakli, C.; Azkur, K.; Costa, R.A.; Crameri, R.; Duan, S.; Eiwegger, T.; Eljaszewicz, A.; Ferstl, R.; et al. Interleukins (from IL-1 to IL-38), interferons, transforming growth factor β, and TNF-α: Receptors, functions, and roles in diseases. J. Allergy Clin. Immunol. 2016, 138, 984–1010. [Google Scholar] [CrossRef] [PubMed]
- Norseen, J.; Hosooka, T.; Hammarstedt, A.; Yore, M.M.; Kant, S.; Aryal, P.; Kiernan, U.A.; Phillips, D.A.; Maruyama, H.; Kraus, B.J.; et al. Retinol-Binding Protein 4 Inhibits Insulin Signaling in Adipocytes by Inducing Proinflammatory Cytokines in Macrophages through a c-Jun N-Terminal Kinase- and Toll-Like Receptor 4-Dependent and Retinol-Independent Mechanism. Mol. Cell. Biol. 2012, 32, 2010–2019. [Google Scholar] [CrossRef] [PubMed]
- Du, M.; Martin, A.; Hays, F.; Johnson, J.; Farjo, R.A.; Farjo, K.M. Serum retinol-binding protein-induced endothelial inflammation is mediated through the activation of toll-like receptor 4. Mol. Vis. 2017, 23, 185–197. [Google Scholar] [PubMed]
- Farjo, K.M.; Farjo, R.A.; Halsey, S.; Moiseyev, G.; Ma, J.X. Retinol-binding protein 4 induces inflammation in human endothelial cells by an NADPH oxidase- and nuclear factor kappa B-dependent and retinol-independent mechanism. Mol. Cell. Biol. 2012, 32, 5103–5115. [Google Scholar] [CrossRef] [PubMed]
- Moraes-Vieira, P.M.; Yore, M.M.; Dwyer, P.M.; Syed, I.; Aryal, P.; Kahn, B.B. RBP4 activates antigen-presenting cells leading to adipose tissue inflammation and systemic insulin resistance. Cell Metab. 2014, 19, 512–526. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Graham, T.E.; Mody, N.; Preitner, F.; Peroni, O.D.; Zabolotny, J.M.; Kotani, K.; Quadro, L.; Kahn, B.B. Serum retinol binding protein 4 contributes to insulin resistance in obesity and type 2 diabetes. Nature 2005, 436, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Meisinger, C.; Ruckert, I.M.; Rathmann, W.; Doring, A.; Thorand, B.; Huth, C.; Kowall, B.; Koenig, W. Retinol-binding protein 4 is associated with prediabetes in adults from the general population: The Cooperative Health Research in the Region of Augsburg (KORA) F4 Study. Diabetes Care 2011, 34, 1648–1650. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Kiernan, U.A.; Shi, L.; Phillips, D.A.; Kahn, B.B.; Hu, F.B.; Manson, J.E.; Albert, C.M.; Rexrode, K.M. Plasma retinol-binding protein 4 (RBP4) levels and risk of coronary heart disease: A prospective analysis among women in the nurses’ health study. Circulation 2013, 127, 1938–1947. [Google Scholar] [CrossRef] [PubMed]
- Qi, Q.; Yu, Z.; Ye, X.; Zhao, F.; Huang, P.; Hu, F.B.; Franco, O.H.; Wang, J.; Li, H.; Liu, Y.; et al. Elevated retinol-binding protein 4 levels are associated with metabolic syndrome in Chinese people. J. Clin. Endocrinol. Metab. 2007, 92, 4827–4834. [Google Scholar] [CrossRef] [PubMed]
- Mercader, J.; Palou, A.; Bonet, M.L. Resveratrol enhances fatty acid oxidation capacity and reduces resistin and Retinol-Binding Protein 4 expression in white adipocytes. J. Nutr. Biochem. 2011, 22, 828–834. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, R.; Nishimura, N.; Hoshino, H.; Isa, Y.; Kadowaki, M.; Ichi, T.; Tanaka, A.; Nishiumi, S.; Fukuda, I.; Ashida, H.; et al. Cyanidin 3-glucoside ameliorates hyperglycemia and insulin sensitivity due to downregulation of retinol binding protein 4 expression in diabetic mice. Biochem. Pharmacol. 2007, 74, 1619–1627. [Google Scholar] [CrossRef] [PubMed]
- Qin, B.; Polansky, M.M.; Harry, D.; Anderson, R.A. Green tea polyphenols improve cardiac muscle mRNA and protein levels of signal pathways related to insulin and lipid metabolism and inflammation in insulin-resistant rats. Mol. Nutr. Food Res. 2010, 54, S14–S23. [Google Scholar] [CrossRef] [PubMed]
- Canas, J.A.; Damaso, L.; Altomare, A.; Killen, K.; Hossain, J.; Balagopal, P.B. Insulin resistance and adiposity in relation to serum beta-carotene levels. J. Pediatr. 2012, 161, 58.e2–64.e2. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Burri, B.J.; Dopler-Nelson, M.; Neidllinger, T.R. Measurements of the major isoforms of vitamins A and E and carotenoids in the blood of people with spinal-cord injuries. J. Chromatogr. A 2003, 987, 359–366. [Google Scholar] [CrossRef]
- Liu, J.; Shi, W.Q.; Cao, Y.; He, L.P.; Guan, K.; Ling, W.H.; Chen, Y.M. Higher serum carotenoid concentrations associated with a lower prevalence of the metabolic syndrome in middle-aged and elderly Chinese adults. Br. J. Nutr. 2014, 112, 2041–2048. [Google Scholar] [CrossRef] [PubMed]
- Feng, D.; Liu, T.; Su, D.F.; Wang, H.; Ding, P.; He, Y.H.; Deng, X.Q.; Hou, M.J.; Ling, W.H.; Chen, W.Q. The association between smoking quantity and hypertension mediated by inflammation in Chinese current smokers. J. Hypertens. 2013, 31, 1798–1805. [Google Scholar] [CrossRef] [PubMed]
- Erikstrup, C.; Mortensen, O.H.; Nielsen, A.R.; Fischer, C.P.; Plomgaard, P.; Petersen, A.M.; Krogh-Madsen, R.; Lindegaard, B.; Erhardt, J.G.; Ullum, H.; et al. RBP-to-retinol ratio, but not total RBP, is elevated in patients with type 2 diabetes. Diabetes Obes. Metab. 2009, 11, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O., III; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Zabetian-Targhi, F.; Mahmoudi, M.J.; Rezaei, N.; Mahmoudi, M. Retinol binding protein 4 in relation to diet, inflammation, immunity, and cardiovascular diseases. Adv. Nutr. 2015, 6, 748–762. [Google Scholar] [CrossRef] [PubMed]
- Balagopal, P.; Graham, T.E.; Kahn, B.B.; Altomare, A.; Funanage, V.; George, D. Reduction of elevated serum retinol binding protein in obese children by lifestyle intervention: Association with subclinical inflammation. J. Clin. Endocrinol. Metab. 2007, 92, 1971–1974. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Kang, S. Effects of regular exercise on obesity and type 2 diabete mellitus in Korean children: Improvements glycemic control and serum adipokines level. J. Phys. Ther. Sci. 2015, 27, 1903–1907. [Google Scholar] [CrossRef] [PubMed]
- Christou, G.A.; Tellis, C.C.; Elisaf, M.S.; Tselepis, A.D.; Kiortsis, D.N. The changes in plasma retinol-binding protein 4 levels are associated with those of the apolipoprotein B-containing lipoproteins during dietary and drug treatment. Angiology 2012, 63, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Hermsdorff, H.H.; Zulet, M.A.; Abete, I.; Martinez, J.A. Discriminated benefits of a Mediterranean dietary pattern within a hypocaloric diet program on plasma RBP4 concentrations and other inflammatory markers in obese subjects. Endocrine 2009, 36, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Neyestani, T.R.; Nikooyeh, B.; Alavi-Majd, H.; Shariatzadeh, N.; Kalayi, A.; Tayebinejad, N.; Heravifard, S.; Salekzamani, S.; Zahedirad, M. Improvement of vitamin D status via daily intake of fortified yogurt drink either with or without extra calcium ameliorates systemic inflammatory biomarkers, including adipokines, in the subjects with type 2 diabetes. J. Clin. Endocrinol. Metab. 2012, 97, 2005–2011. [Google Scholar] [CrossRef] [PubMed]
- Van Herpen-Broekmans, W.M.; Klopping-Ketelaars, I.A.; Bots, M.L.; Kluft, C.; Princen, H.; Hendriks, H.F.; Tijburg, L.B.; van Poppel, G.; Kardinaal, A.F. Serum carotenoids and vitamins in relation to markers of endothelial function and inflammation. Eur. J. Epidemiol. 2004, 19, 915–921. [Google Scholar] [CrossRef] [PubMed]
- Kritchevsky, S.B.; Bush, A.J.; Pahor, M.; Gross, M.D. Serum carotenoids and markers of inflammation in nonsmokers. Am. J. Epidemiol. 2000, 152, 1065–1071. [Google Scholar] [CrossRef] [PubMed]
- Walston, J.; Xue, Q.; Semba, R.D.; Ferrucci, L.; Cappola, A.R.; Ricks, M.; Guralnik, J.; Fried, L.P. Serum antioxidants, inflammation, and total mortality in older women. Am. J. Epidemiol. 2006, 163, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Palozza, P.; Calviello, G.; Serini, S.; Maggiano, N.; Lanza, P.; Ranelletti, F.O.; Bartoli, G.M. β-carotene at high concentrations induces apoptosis by enhancing oxy-radical production in human adenocarcinoma cells. Free Radic. Biol. Med. 2001, 30, 1000–1007. [Google Scholar] [CrossRef]
- Liu, D.; Shi, J.; Ibarra, CA.; Kakuda, Y.; Xue, S.J. The scavenging capacity and synergistic effects of lycopene, vitamin E, vitamin C, and β-carotene mixtures on the DPPH free radical. LWT Food Sci. Technol. 2008, 41, 1344–1349. [Google Scholar] [CrossRef]
- Shi, J.; Kakuda, Y.; Yeung, D. Antioxidative properties of lycopene and other carotenoids from tomatoes: Synergistic effects. BioFactors 2004, 21, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Vallabhapurapu, S.; Karin, M. Regulation and Function of NF-kappa B Transcription Factors in the Immune System. Annu. Rev. Immunol. 2009, 27, 693–733. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Zanetti, M.; Semolic, A.; Pirulli, A.; Cattin, M.R.; Biolo, G.; Bosutti, A.; Panzetta, G.; Bernardi, A.; Guarnieri, G. High plasma retinol binding protein 4 (RBP4) is associated with systemic inflammation independently of low RBP4 adipose expression and is normalized by transplantation in nonobese, nondiabetic patients with chronic kidney disease. Clin. Endocrinol. 2011, 75, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, D.; Li, D.; Sun, R.; Xia, M. Associations of retinol-binding protein 4 with oxidative stress, inflammatory markers, and metabolic syndrome in a middle-aged and elderly Chinese population. Diabetol. Metab. Syndr. 2014, 6, 25. [Google Scholar] [CrossRef] [PubMed]
- Bobbert, P.; Weithauser, A.; Andres, J.; Bobbert, T.; Kuhl, U.; Schultheiss, H.P.; Rauch, U.; Skurk, C. Increased plasma retinol binding protein 4 levels in patients with inflammatory cardiomyopathy. Eur. J. Heart Fail. 2009, 11, 1163–1168. [Google Scholar] [CrossRef] [PubMed]
- Kotnik, P.; Keuper, M.; Wabitsch, M.; Fischer-Posovszky, P. Interleukin-1beta downregulates RBP4 secretion in human adipocytes. PLoS ONE 2013, 8, e57796. [Google Scholar] [CrossRef] [PubMed]
- Kiernan, U.A.; Phillips, D.A.; Trenchevska, O.; Nedelkov, D. Quantitative mass spectrometry evaluation of human retinol binding protein 4 and related variants. PLoS ONE 2011, 6, e17282. [Google Scholar] [CrossRef] [PubMed]
| n | Total (n = 3031) | Female (n = 2063) | Male (n = 968) | p Value | |
|---|---|---|---|---|---|
| Age (years) | 3031 | 58.6 ± 6.24 | 57.6 ± 5.8 | 60.7 ± 6.7 | <0.001 |
| BMI (kg/m2) | 3031 | 23.3 ± 3.06 | 23.1 ± 3.11 | 23.8 ± 2.90 | <0.001 |
| Waist circumference (cm) | 3031 | 83.3 ± 8.95 | 81.9 ± 8.90 | 86.2 ± 8.35 | <0.001 |
| Education (n (%)) | 0.211 | ||||
| Secondary school or below | 869 | 869 (28.7) | 606 (29.4) | 263 (27.2) | |
| High school or above | 2162 | 2162 (71.3) | 1457 (70.6) | 705 (72.8) | |
| Married (n (%)) | 2730 | 2730 (90.1) | 1790 (86.8) | 940 (97.1) | <0.001 |
| Household income (Yuan/month/person), (n (%)) | <0.001 | ||||
| ≤500 | 57 | 57 (1.9) | 31 (1.5) | 26 (2.7) | |
| 501–1500 | 790 | 790 (26.1) | 572 (27.7) | 218 (22.5) | |
| 1501–3000 | 1327 | 1327 (43.8) | 922 (44.7) | 405 (41.8) | |
| >3000 | 857 | 857 (28.3) | 538 (26.1) | 319 (33.0) | |
| Smokers (n (%)) a | 489 | 489 (16.1) | 6 (0.3) | 483 (49.9) | <0.001 |
| Alcohol drinkers (n (%)) b | 215 | 215 (7.1) | 50 (2.4) | 165 (17.1) | <0.001 |
| Vitamin supplement users (n (%)) | 662 | 662 (21.8) | 520 (25.2) | 142 (14.7) | <0.001 |
| Calcium supplement users (n (%)) | 951 | 951 (31.4) | 757 (36.7) | 194 (20.0) | <0.001 |
| Physical activity (MET·h/day) c | 3031 | 25.8 ± 6.67 | 26.1 ± 6.48 | 25.3 ± 7.09 | 0.001 |
| Serum fasting glucose (mmol/L) | 2892 | 5.02 ± 1.16 | 4.97 ± 1.13 | 5.14 ± 1.22 | <0.001 |
| Serum fasting insulin (mU/L) | 2901 | 9.06 ± 5.57 | 9.29 ± 5.73 | 8.58 ± 5.19 | 0.001 |
| Serum TC (mmol/L) | 3024 | 5.52 ± 1.10 | 5.66 ± 1.11 | 5.24 ± 1.03 | <0.001 |
| Serum retinol (μmol/L) | 3031 | 1.58 (1.35, 1.86) | 1.54 (1.32, 1.80) | 1.68 (1.42, 1.99) | <0.001 |
| Serum carotenoids (μmol/L) | |||||
| α-Carotene | 3031 | 0.06 (0.04, 0.09) | 0.06 (0.04, 0.10) | 0.05 (0.03, 0.08) | <0.001 |
| β-Carotene | 3031 | 0.44 (0.25, 0.70) | 0.50 (0.30, 0.77) | 0.33 (0.19, 0.52) | <0.001 |
| β-Cryptoxanthin | 3031 | 0.12 (0.07, 0.20) | 0.13 (0.08, 0.23) | 0.09 (0.06, 0.16) | <0.001 |
| Lycopene | 3031 | 0.16 (0.10, 0.23) | 0.17 (0.12, 0.25) | 0.13 (0.08, 0.20) | <0.001 |
| Lutein + zeaxanthin | 3031 | 0.62 (0.44, 0.86) | 0.64 (0.45, 0.89) | 0.58 (0.41, 0.79) | <0.001 |
| Total carotenoids | 3031 | 1.63 (1.04, 2.08) | 1.64 (1.13, 2.20) | 1.28 (0.90, 1.74) | <0.001 |
| Inflammatory marker | |||||
| MCP1 (pg/mL) | 1314 | 454 (334, 609) | 460 (339, 623) | 442 (326, 575) | 0.016 |
| Interleukin-6 (pg/mL) | 1312 | 1.31 (0.77, 2.44) | 1.21 (0.73, 2.28) | 1.48 (0.87, 2.63) | 0.001 |
| Interleukin-1β (pg/mL) | 1313 | 3.88 (1.50, 17.87) | 3.51 (1.40, 13.79) | 6.05 (1.76, 24.20) | <0.001 |
| TNF-α (pg/mL) | 1313 | 6.84 (1.66, 62.43) | 5.69 (1.60, 48.87) | 11.44 (1.72, 71.35) | 0.001 |
| hsCRP (mg/L) | 2925 | 0.95 (0.56, 1.93) | 0.98 (0.58, 1.99) | 0.86 (0.52, 1.77) | 0.001 |
| RBP4 (μg/mL) | 2738 | 36.48 ± 6.92 | 35.36 ± 6.49 | 38.91 ± 7.19 | <0.001 |
| aRBP4 a | RBP4 | hsCRP | MCP1 | IL-6 | IL-1β | TNF-α | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | r | p | r | p | r | p | |
| n | 2734 | 2734 | 2921 | 1310 | 1292 | 1292 | 1297 | |||||||
| Age, sex adjusted M1 | ||||||||||||||
| Total carotenoids b | −0.129 | <0.001 | −0.097 | <0.001 | −0.159 | <0.001 | −0.079 | 0.004 | 0.002 | 0.933 | 0.002 | 0.944 | −0.014 | 0.608 |
| Log total carotenoids | −0.134 | <0.001 | −0.098 | <0.001 | −0.140 | <0.001 | −0.071 | 0.010 | 0.022 | 0.438 | 0.026 | 0.345 | 0.006 | 0.835 |
| α-Carotene | −0.073 | <0.001 | −0.062 | 0.001 | −0.161 | <0.001 | −0.088 | 0.001 | −0.044 | 0.117 | −0.059 | 0.033 | −0.080 | 0.004 |
| β-Carotene | −0.103 | <0.001 | −0.087 | <0.001 | −0.161 | <0.001 | −0.075 | 0.006 | 0.015 | 0.582 | 0.016 | 0.553 | 0.006 | 0.838 |
| β-Cryptoxanthin | −0.080 | <0.001 | −0.057 | 0.003 | −0.060 | 0.001 | −0.028 | 0.305 | 0.043 | 0.120 | 0.025 | 0.369 | 0.051 | 0.064 |
| Lycopene | −0.086 | <0.001 | −0.063 | 0.001 | −0.136 | <0.001 | −0.046 | 0.099 | −0.014 | 0.610 | 0.003 | 0.926 | −0.033 | 0.231 |
| Lutein + zeaxanthin | −0.140 | <0.001 | −0.093 | <0.001 | −0.076 | <0.001 | −0.059 | 0.033 | 0.009 | 0.758 | 0.022 | 0.424 | 0.004 | 0.890 |
| Multivariate-adjusted M2 | ||||||||||||||
| Total carotenoids b | −0.098 | <0.001 | −0.079 | <0.001 | −0.114 | <0.001 | −0.090 | 0.001 | −0.014 | 0.616 | −0.055 | 0.050 | −0.079 | 0.005 |
| Log total carotenoids | −0.103 | <0.001 | −0.080 | <0.001 | −0.097 | <0.001 | −0.081 | 0.004 | 0.007 | 0.793 | −0.033 | 0.242 | −0.062 | 0.027 |
| α-Carotene | −0.044 | 0.023 | −0.037 | 0.052 | −0.112 | <0.001 | −0.090 | 0.001 | −0.046 | 0.096 | −0.072 | 0.010 | −0.096 | 0.001 |
| β-Carotene | −0.067 | <0.001 | −0.061 | 0.001 | −0.105 | <0.001 | −0.081 | 0.004 | 0.009 | 0.744 | −0.020 | 0.474 | −0.034 | 0.222 |
| β-Cryptoxanthin | −0.067 | <0.001 | −0.056 | 0.004 | −0.048 | 0.009 | −0.036 | 0.200 | 0.026 | 0.350 | −0.025 | 0.368 | −0.003 | 0.923 |
| Lycopene | −0.062 | 0.001 | −0.050 | 0.009 | −0.100 | <0.001 | −0.054 | 0.050 | −0.033 | 0.233 | −0.044 | 0.115 | −0.089 | 0.001 |
| Lutein + zeaxanthin | −0.120 | <0.001 | −0.084 | <0.001 | −0.051 | 0.005 | −0.067 | 0.016 | −0.006 | 0.834 | −0.039 | 0.163 | −0.066 | 0.018 |
| Age, Sex Adjusted M1 | Multivariate-Adjusted M2 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| aRBP4 d | RBP4 | hsCRP | MCP1 | IL6 | IL-1β | TNF-α | aRBP4 d | RBP4 | hsCRP | MCP1 | IL-6 | IL-1β | TNF-α | |
| Women | ||||||||||||||
| n | 1866 | 1866 | 1989 | 894 | 879 | 880 | 883 | 1866 | 1866 | 1989 | 894 | 879 | 880 | 883 |
| Total carotenoids e | −0.143 c | −0.112 c | −0.155 c | −0.043 | 0.035 | −0.002 | 0.001 | −0.111 c | −0.091 c | −0.110 c | −0.053 | 0.029 | −0.059 | −0.061 |
| Log total carotenoids | −0.146 c | −0.111 c | −0.146 c | −0.045 | 0.057 | 0.037 | 0.027 | −0.115 c | −0.093 c | −0.101 c | −0.054 | 0.052 | −0.022 | −0.036 |
| α-Carotene | −0.071 b | −0.058 a | −0.140 c | −0.068 a | −0.027 | −0.074 a | −0.075 a | −0.039 | −0.03 | −0.088 | −0.069 a | −0.025 | −0.091 b | −0.094 b |
| β-Carotene | −0.116 c | −0.095 c | −0.171 c | −0.064 | 0.039 | 0.039 | 0.028 | −0.079 c | −0.068 b | −0.113 c | −0.068 a | 0.041 | 0.003 | −0.008 |
| β-Cryptoxanthin | −0.090 c | −0.073 b | −0.055 a | 0.014 | 0.091 b | 0.021 | 0.055 | −0.078 c | −0.070 b | −0.052 a | 0.001 | 0.079 a | −0.025 | 0.002 |
| Lycopene | −0.109 c | −0.088 c | −0.127 c | −0.002 | −0.009 | −0.023 | −0.017 | −0.082 c | −0.071 b | −0.089 c | −0.01 | −0.020 | −0.069 a | −0.068 a |
| Lutein + zeaxanthin | −0.149 c | −0.106 c | −0.086 c | −0.042 | 0.035 | 0.028 | 0.012 | −0.129 c | −0.097 c | −0.059 b | −0.05 | 0.029 | −0.035 | −0.056 |
| Men | ||||||||||||||
| n | 866 | 866 | 930 | 414 | 411 | 410 | 412 | 866 | 866 | 930 | 414 | 411 | 410 | 412 |
| Total carotenoids e | −0.096 b | −0.059 | −0.165 c | −0.148 b | −0.06 | 0.013 | −0.041 | −0.066 | −0.043 | −0.124 c | −0.160 c | −0.096 | −0.042 | −0.109 a |
| Log total carotenoids | −0.105 b | −0.063 | −0.124 c | −0.121 a | −0.046 | 0.007 | −0.035 | −0.075 a | −0.047 | −0.089 b | −0.131 b | −0.082 | −0.049 | −0.105 a |
| α-Carotene | −0.076 a | −0.068 a | −0.206 c | −0.126 b | −0.074 | −0.029 | −0.088 | −0.051 | −0.048 | −0.160 c | −0.131 b | −0.082 | −0.033 | −0.095 |
| β-Carotene | −0.072 a | −0.062 | −0.134 c | −0.091 | −0.027 | −0.025 | −0.034 | −0.036 | −0.038 | −0.090 b | −0.099 a | −0.05 | −0.061 | −0.076 |
| β-Cryptoxanthin | −0.055 | −0.019 | −0.067 a | −0.119 a | −0.061 | 0.038 | 0.048 | −0.04 | −0.017 | −0.046 | −0.123 a | −0.094 | −0.023 | −0.016 |
| Lycopene | −0.032 | −0.005 | −0.154 c | −0.128 b | −0.021 | 0.056 | −0.062 | −0.012 | 0.003 | −0.117 c | −0.136 b | −0.049 | 0.007 | −0.127 b |
| Lutein + zeaxanthin | −0.121 c | −0.065 | −0.055 | −0.093 | −0.045 | 0.011 | −0.011 | −0.100 b | −0.055 | −0.038 | −0.098 a | −0.077 | −0.04 | −0.077 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jing, L.; Xiao, M.; Dong, H.; Lin, J.; Chen, G.; Ling, W.; Chen, Y. Serum Carotenoids Are Inversely Associated with RBP4 and Other Inflammatory Markers in Middle-Aged and Elderly Adults. Nutrients 2018, 10, 260. https://doi.org/10.3390/nu10030260
Jing L, Xiao M, Dong H, Lin J, Chen G, Ling W, Chen Y. Serum Carotenoids Are Inversely Associated with RBP4 and Other Inflammatory Markers in Middle-Aged and Elderly Adults. Nutrients. 2018; 10(3):260. https://doi.org/10.3390/nu10030260
Chicago/Turabian StyleJing, Lipeng, Mianli Xiao, Hongli Dong, Jiesheng Lin, Gengdong Chen, Wenhua Ling, and Yuming Chen. 2018. "Serum Carotenoids Are Inversely Associated with RBP4 and Other Inflammatory Markers in Middle-Aged and Elderly Adults" Nutrients 10, no. 3: 260. https://doi.org/10.3390/nu10030260
APA StyleJing, L., Xiao, M., Dong, H., Lin, J., Chen, G., Ling, W., & Chen, Y. (2018). Serum Carotenoids Are Inversely Associated with RBP4 and Other Inflammatory Markers in Middle-Aged and Elderly Adults. Nutrients, 10(3), 260. https://doi.org/10.3390/nu10030260