The Dietary Intake and Practices of Adolescent Girls in Low- and Middle-Income Countries: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
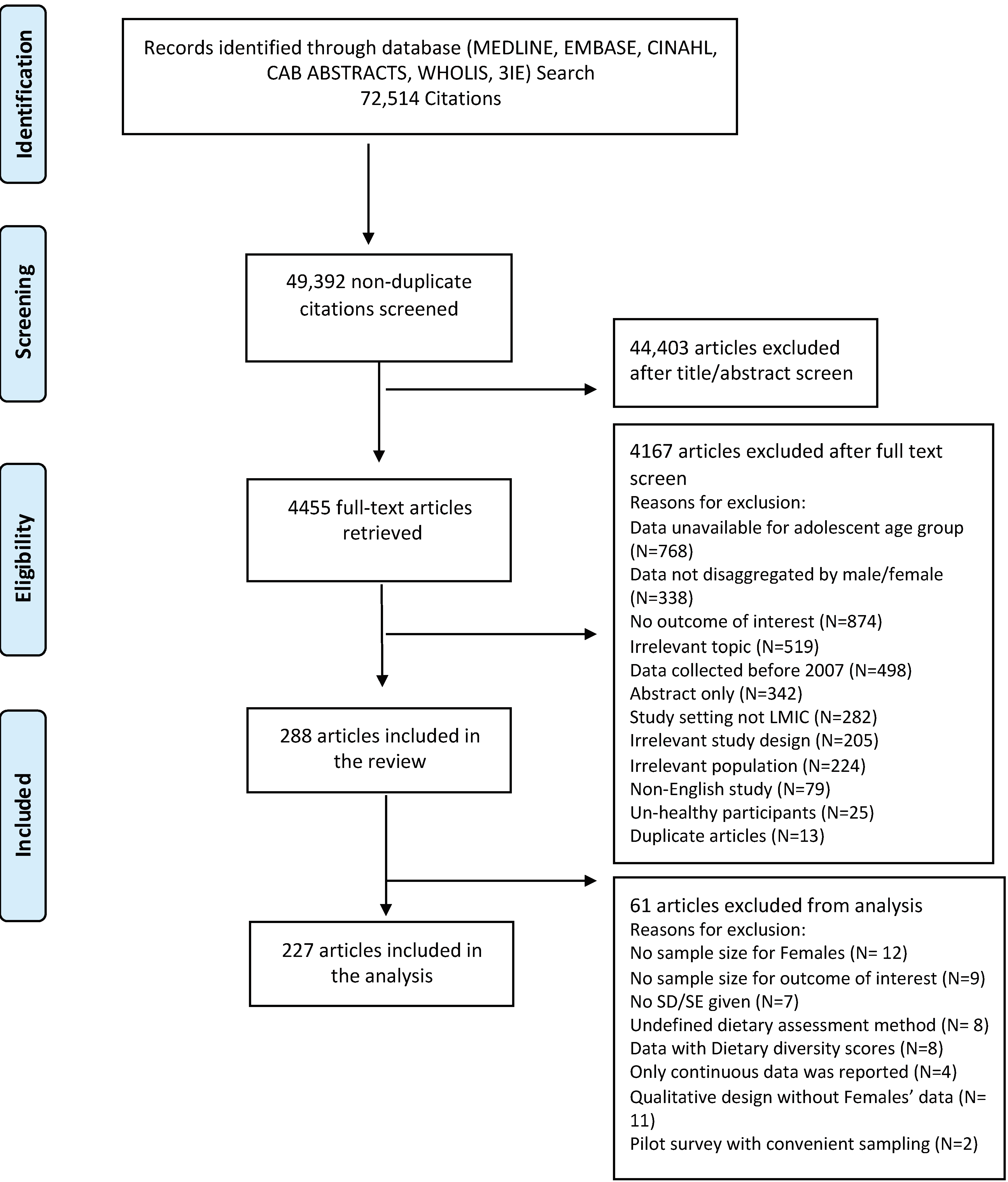
2.2. Study Selection and Data Abstraction
2.3. Quality Assessment
2.4. Data Synthesis
2.4.1. Dietary Intake
2.4.2. Adequate Consumption of Fruits and Vegetables
2.4.3. Macronutrient and Energy Intake
2.4.4. Meal Patterns
3. Results
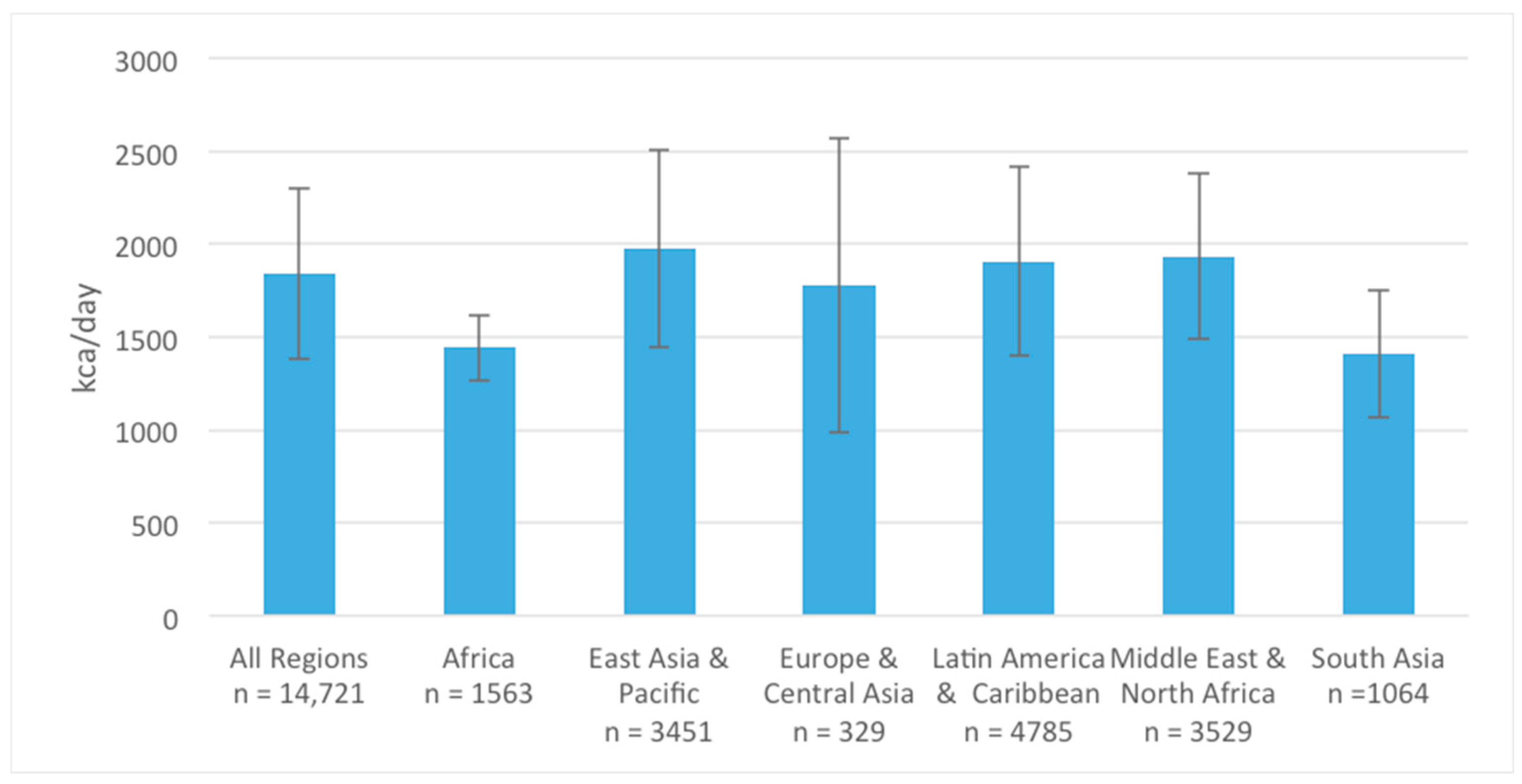
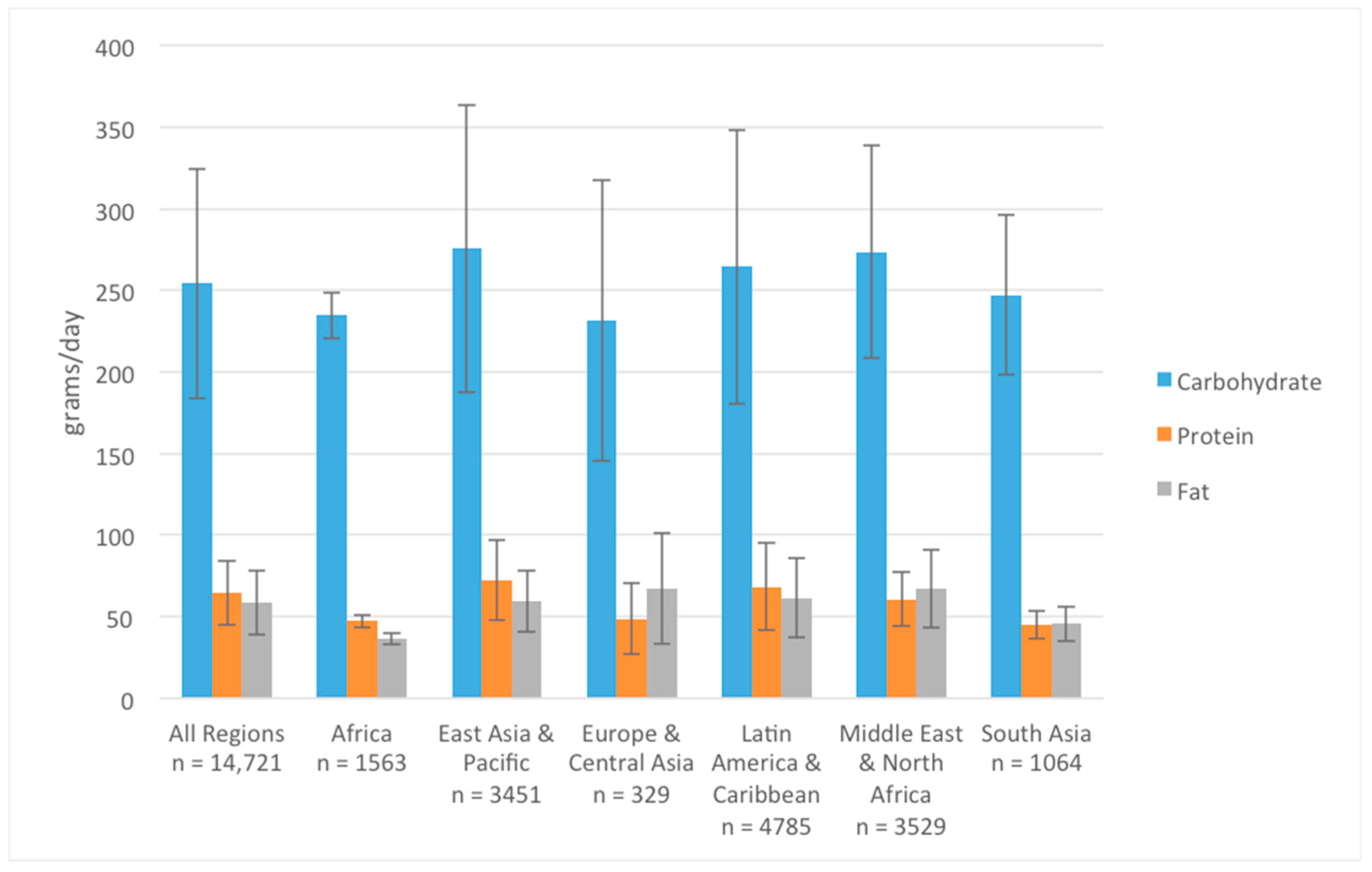
3.1. Energy and Macronutrient Intake
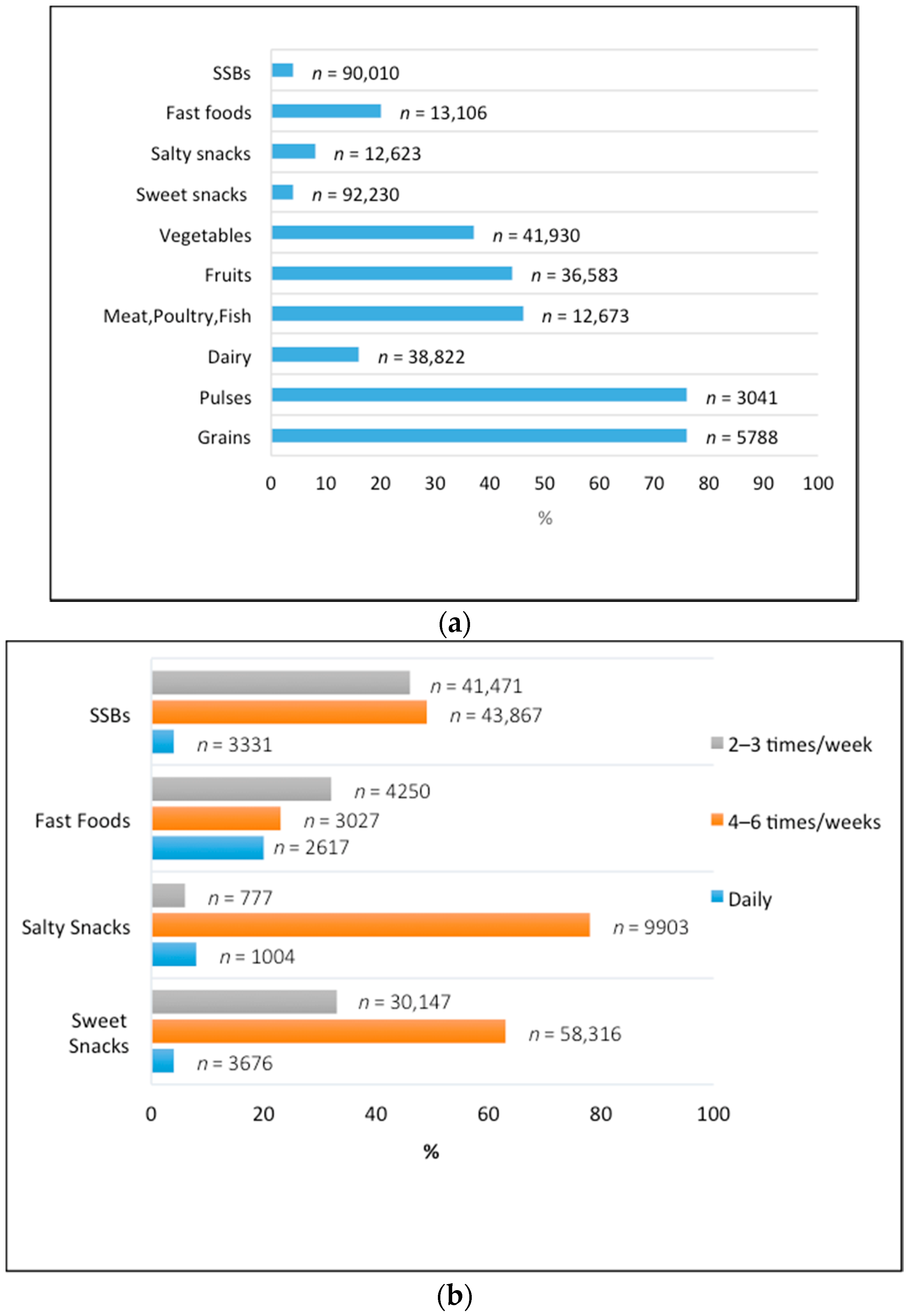
3.2. Dietary Intake
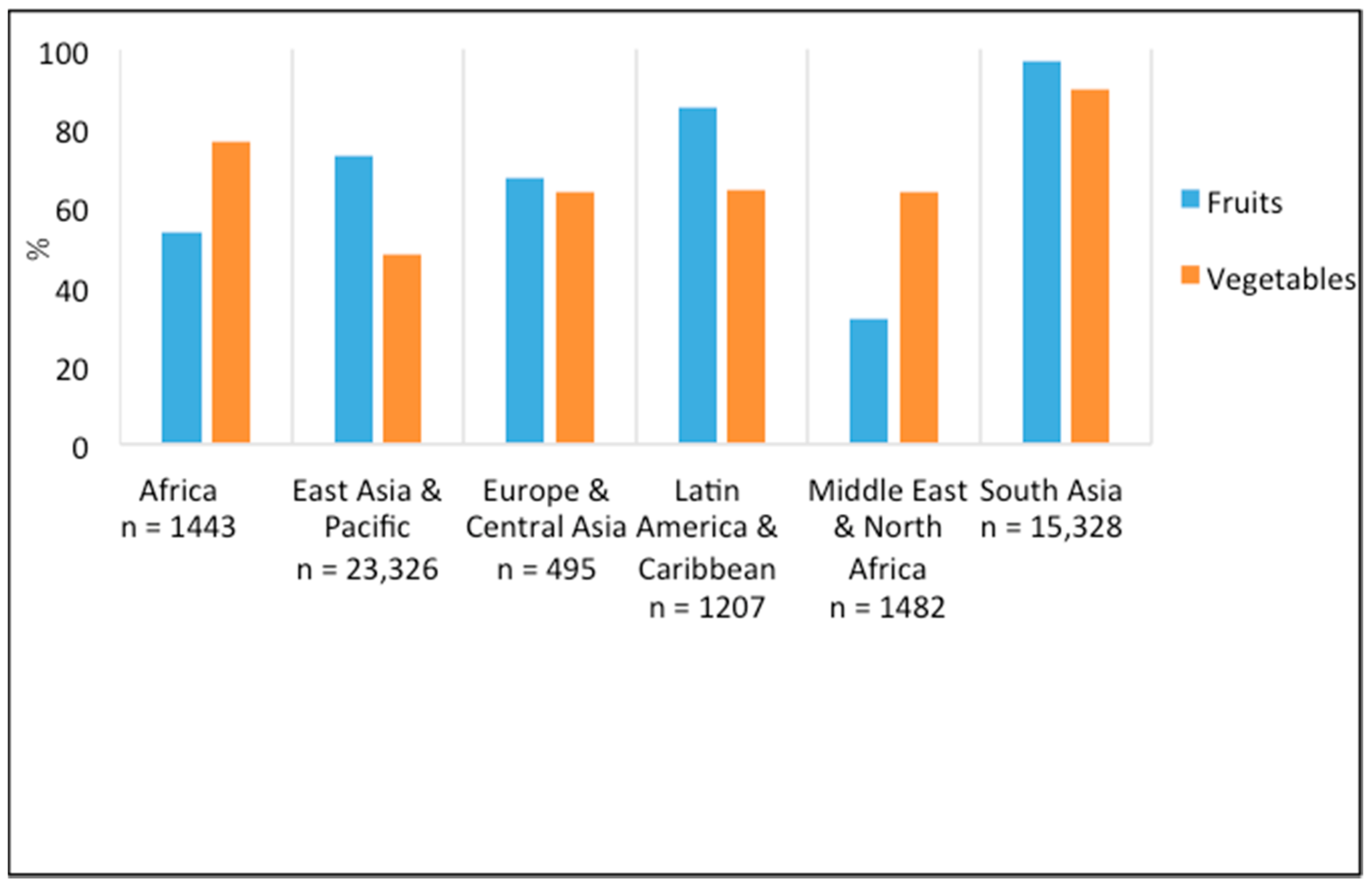
3.3. Adequate Fruit and Vegetable Consumption
3.4. Meal Patterns
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sheehan, P.; Sweeny, K.; Rasmussen, B.; Wils, A.; Friedman, H.S.; Mahon, J.; Patton, G.C.; Sawyer, S.M.; Howard, E.; Symons, J.; et al. Building the foundations for sustainable development: A case for global investment in the capabilities of adolescents. Lancet 2017, 390, 1792–1806. [Google Scholar] [CrossRef]
- United Nations. World Population Prospects. 2017. Available online: https://population.un.org/wpp/ (accessed on 17 May 2018).
- United Nations, Youth Population Trends and Sustainable Development. 2015. Available online: http://203.187.160.132:9011/www.un.org/c3pr90ntc0td/en/development/desa/population/publications/pdf/popfacts/PopFacts_2015-1.pdf (accessed on 17 May 2018).
- Patton, G.C.; Sawyer, S.M.; Santelli, J.S.; Ross, D.A.; Afifi, R.; Allen, N.B.; Arora, M.; Azzopardi, P.; Baldwin, W.; Bonell, C.; et al. Our future: A Lancet commission on adolescent health and wellbeing. Lancet 2016, 387, 2423–2478. [Google Scholar] [CrossRef]
- Akseer, N.; Al-Gashm, S.; Mehta, S.; Mokdad, A.; Bhutta, Z.A. Global and regional trends in the nutritional status of young people: A critical and neglected age group. Ann. N. Y. Acad. Sci. 2017, 1393, 3–20. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Stevens, G.A.; Finucane, M.M.; De-Regil, L.M.; Paciorek, C.J.; Flaxman, S.R.; Branca, F.; Peña-Rosas, J.P.; Bhutta, Z.A.; Ezzati, M.; Nutrition Impact Model Study Group (Anaemia). Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: A systematic analysis of population-representative data. Lancet Glob. Health 2013, 1, e16–e25. [Google Scholar]
- Christian, P.; Smith, E.R. Adolescent undernutrition: Global burden, physiology, and nutritional risks. Ann. Nutr. Metab. 2018, 72, 316–328. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Lassi, Z.S.; Bergeron, G.; Koletzko, B.; Salam, R.; Diaz, A.; McLean, M.; Black, R.E.; De-Regil, L.M.; Christian, P.; et al. Delivering an action agenda for nutrition interventions addressing adolescent girls and young women: Priorities for implementation and research. Ann. N. Y. Acad. Sci. 2017, 1393, 61–71. [Google Scholar] [CrossRef]
- WHO. Global Health Estimates 2015: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2015; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Ochola, S.; Masibo, P.K. Dietary intake of schoolchildren and adolescents in developing countries. Ann. Nutr. Metab. 2014, 64, 24–40. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0: The Cochrane Collaboration 2011. Available online: http://handbook.cochrane.org (accessed on 5 February 2017).
- National Institute of Health. Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 5 February 2017).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- FAO and FHI 360. Minimum Dietary Diversity for Women: A Guide for Measurement; Food and Agriculture Organization of the United Nations: Rome, NY, USA, 2016. [Google Scholar]
- Friel, S.; Hattersley, L.; Snowdon, W.; Thow, A.M.; Lobstein, T.; Sanders, D.; Barquera, S.; Mohan, S.; Hawkes, C.; Kelly, B.; et al. Monitoring the impacts of trade agreements on food environments. Obes. Rev. 2013, 1, 120–134. [Google Scholar] [CrossRef] [PubMed]
- WHO. Diet, Nutrition and the Prevention of Chronic Diseases: Report of A Joint WHO/FAO Expert Consultation; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes (DRIs): Estimated Average Requirements. 2018. Available online: http://www.nationalacademies.org/hmd/~/media/Files/Activity Files/Nutrition/DRI-Tables/5Summary TableTables 14.pdf?la=en (accessed on 16 May 2017).
- Popkin, B.M. The nutrition transition and its health implications in lower-income countries. Public Health Nutr. 1998, 1, 5–21. [Google Scholar] [CrossRef] [Green Version]
- Abdul Majid, H.; Ramli, L.; Ying, S.P.; Su, T.T.; Jalaludin, M.Y.; Abdul Mohsein, N.A. Dietary intake among adolescents in a middle-income country: An outcome from the Malaysian health and adolescents longitudinal research team study (the MyHeARTs Study). PLoS ONE 2016, 11, e0155447. [Google Scholar] [CrossRef] [PubMed]
- Jaacks, L.M.; Slining, M.M.; Popkin, B.M. Recent trends in the prevalence of under- and overweight among adolescent girls in low- and middle-income countries. Pediatr. Obes. 2015, 10, 428–435. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, L.A.; Mundo-Rosas, V.; Mendez-Gomez-Humaran, I.; Perez-Escamilla, R.; Shamah-Levy, T. Dietary quality and household food insecurity among Mexican children and adolescents. Matern. Child Nutr. 2017, 13. [Google Scholar] [CrossRef]
- Aurino, E.; Fernandes, M.; Penny, M.E. The nutrition transition and adolescents’ diets in low- and middle-income countries: A cross-cohort comparison. Public Health Nutr. 2017, 20, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Collaborators GBDRF. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef]
- Miller, V.; Mente, A.; Dehghan, M.; Rangarajan, S.; Zhang, X.; Swaminathan, S.; Dagenais, G.; Gupta, R.; Mohan, V.; Lear, S.; et al. Fruit, vegetable, and legume intake, and cardiovascular disease and deaths in 18 countries (PURE): A prospective cohort study. Lancet 2017, 390, 2037–2049. [Google Scholar] [CrossRef]
- Lassi, Z.S.; Mansoor, T.; Salam, R.A.; Bhutta, S.Z.; Das, J.K.; Bhutta, Z.A. Review of nutrition guidelines relevant for adolescents in low- and middle-income countries. Ann. N. Y. Acad. Sci. 2017, 1393, 51–60. [Google Scholar] [CrossRef] [Green Version]
- De la Hunty, A.; Gibson, S.; Ashwell, M. Does regular breakfast cereal consumption help children and adolescents stay slimmer? A systematic review and meta-analysis. Obes. Facts 2013, 6, 70–85. [Google Scholar] [CrossRef]
- Szajewska, H.; Ruszczynski, M. Systematic review demonstrating that breakfast consumption influences body weight outcomes in children and adolescents in Europe. Crit. Rev. Food Sci. Nutr. 2010, 50, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Hoyland, A.; Dye, L.; Lawton, C.L. A systematic review of the effect of breakfast on the cognitive performance of children and adolescents. Nutr. Res. Rev. 2009, 22, 220–243. [Google Scholar] [CrossRef] [PubMed]
- Benedict, R.K.; Schmale, A.; Namaste, S. Adolescent Nutrition 2000–2017: DHS Data on Adolescents Age 15–19; USAID: Rockville, MD, USA, 2018.
- SPRING. Stakeholders Consultation on Adolescent Girls’ Nutrition: Evidence, Guidance, and Gaps Arlington, VA Strengthening Partnerthips, Results, and Innovations in Nutrition Globally (SPRING) Project. 2017. Available online: http://www.spring-nutrition.org/events/stakeholders-consultation-adolescent-girls-nutrition-evidence-guidance-and-gaps (accessed on 21 September 2018).
- SPRING. Adolescent Nutrition CALL TO ACTION: Better Data Now to Drive Bettern Policies and Programs in the Future Arlington, VA Stregthening Parternships, Results, and Innovations in Nutrition Globally (SPRING) Project. 2018. Available online: https://www.spring-nutrition.org/about-us/news/adolescent-nutrition-call-action-better-data-now-drive-better-policies-and-programs (accessed on 22 September 2018).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Demographics | |||
|---|---|---|---|
| World Regions | Study Design | Urban/Rural Setting | Study Setting |
| Africa (N = 36) | Cohort: N = 3 Cross Sectional: N = 33 | Urban: N = 16 Rural: N = 6 Mixed: N = 11 Peri-Urban: N = 1 NR: N = 2 | Community: N = 7 Regional: N = 4 School: N = 25 |
| East Asia and Pacific (N = 47) | Cohort: N = 5 Cross Sectional: N = 39 Mixed Design: N = 1 RCT: N = 1 Twin Study: N = 1 | Urban: N= 24 Rural: N = 6 Mixed: N = 14 Peri-Urban: N = 1 NR: N = 2 | Community: N = 2 National: N = 4 Regional: N = 4 School: N = 37 |
| Europe and Central Asia (N = 9) | Cross Sectional: N = 9 | Urban: N = 8 Mixed: N = 1 | Community: N = 1 School: N = 8 |
| Latin America and the Caribbean (N = 35) | Case Study: N = 1 Cohort: N = 2 Cross Sectional: N = 26 Longitudinal: N = 1 Qualitative: N = 2 RCT: N = 3 | Urban: N = 18 Rural: N = 1 Mixed: N = 11 Peri-Urban: N = 2 NR: N = 3 | Community: N = 2 National: N = 5 Regional: N = 4 School: N = 24 |
| Middle East and North Africa (N = 46) | Cross Sectional: N = 42 Qualitative: N = 1 Quasi-Experimental: N = 3 | Urban: N = 33 Rural: N = 1 Mixed: N = 10 NR: N = 2 | National: N = 1 Regional: N = 2 School: N = 43 |
| South Asia (N = 54) | Case Control: N = 2 Cross Sectional: N = 50 RCT: N = 2 | Urban: N = 35 Rural: N = 7 Mixed: N = 8 NR: N = 4 | Community: N = 10 Regional: N = 3 School: N = 41 |
| All Regions (N = 227) | Cohort: N= 10 Case Study: N = 1 Case Control: N = 2 Cross Sectional: N = 199 Mixed Design: N = 1 Longitudinal: N = 1 Qualitative: N = 3 Quasi-Experimental: N = 3 RCT: N = 6 Twin Study: N = 1 | Community: N = 22 National: N = 10 Regional: N = 17 School: N = 178 | Community: N = 22 National: N = 10 Regional: N = 17 School: N = 178 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keats, E.C.; Rappaport, A.I.; Shah, S.; Oh, C.; Jain, R.; Bhutta, Z.A. The Dietary Intake and Practices of Adolescent Girls in Low- and Middle-Income Countries: A Systematic Review. Nutrients 2018, 10, 1978. https://doi.org/10.3390/nu10121978
Keats EC, Rappaport AI, Shah S, Oh C, Jain R, Bhutta ZA. The Dietary Intake and Practices of Adolescent Girls in Low- and Middle-Income Countries: A Systematic Review. Nutrients. 2018; 10(12):1978. https://doi.org/10.3390/nu10121978
Chicago/Turabian StyleKeats, Emily C., Aviva I. Rappaport, Shailja Shah, Christina Oh, Reena Jain, and Zulfiqar A. Bhutta. 2018. "The Dietary Intake and Practices of Adolescent Girls in Low- and Middle-Income Countries: A Systematic Review" Nutrients 10, no. 12: 1978. https://doi.org/10.3390/nu10121978