Association between Spatial Access to Food Outlets, Frequency of Grocery Shopping, and Objectively-Assessed and Self-Reported Fruit and Vegetable Consumption


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Settings and Participants
2.2. Food Access Variables
2.3. Food Outlet Shopping
2.4. Fruit and Vegetable Consumption
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
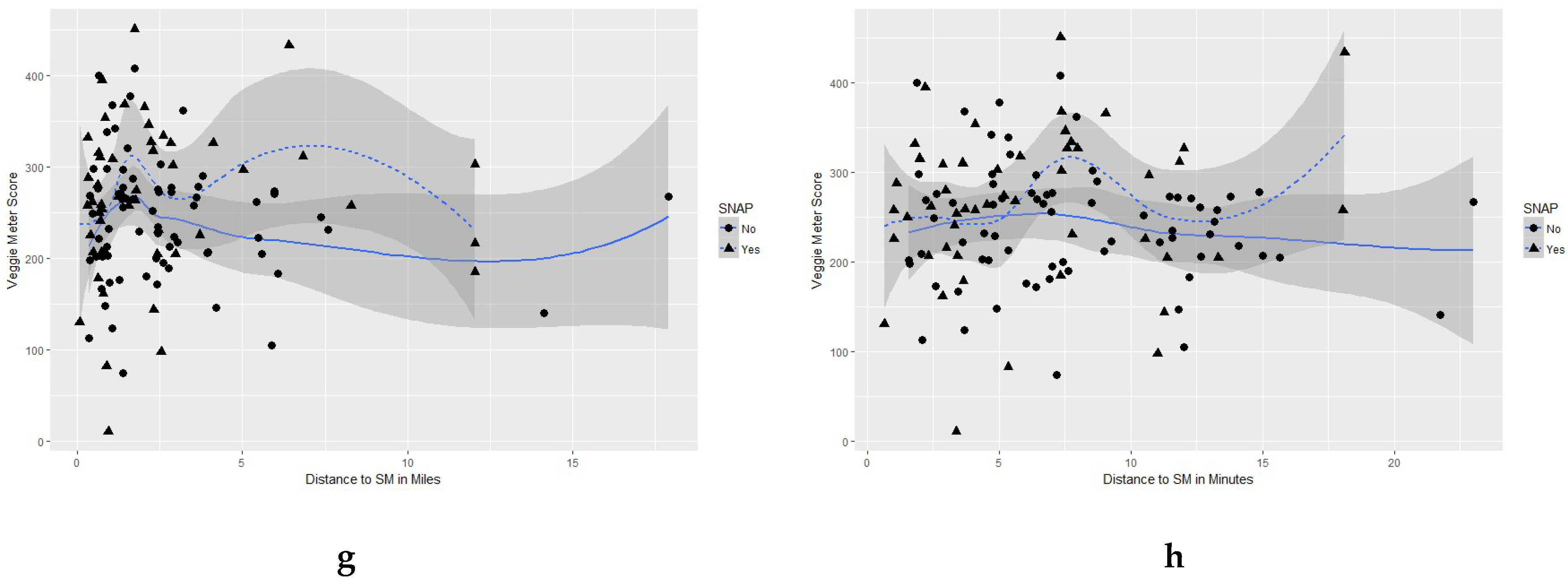
3.2. Association between Distance to Supermarket and Dietary Consumption
3.3. Association between Skin Carotenoids and Accessibility to Healthy Food Outlets.
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. 8th Edition; December 2015. Available online: https://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 3 December 2018).
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality—A systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Chan, D.S.; Vieira, A.R.; Rosenblatt, D.A.N.; Vieira, R.; Greenwood, D.C.; Norat, T. Dietary compared with blood concentrations of carotenoids and breast cancer risk: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2012, 96, 356–373. [Google Scholar] [CrossRef] [PubMed]
- Bertoia, M.L.; Mukamal, K.J.; Cahill, L.E.; Hou, T.; Ludwig, D.S.; Mozaffarian, D.; Willett, W.C.; Hu, F.B.; Rimm, E.B. Changes in Intake of Fruits Vegetables Weight Change in United States Men Women Followed for Up to 24 Years: Analysis from Three Prospective Cohort Studies. PLoS Med. 2015, 12, e1001878. [Google Scholar] [CrossRef] [PubMed]
- Ledoux, T.; Hingle, M.D.; Baranowski, T. Relationship of fruit and vegetable intake with adiposity: A systematic review. Obes. Rev. 2011, 12, e143–e150. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ouyang, Y.; Liu, J.; Zhu, M.; Zhao, G.; Bao, W.; Hu, F.B. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2014, 349, 4490. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.M.; Reedy, J.; KrebsSmith, S.M. American diet quality: Where it is, where it is heading, and what it could be. J. Acad. Nutr. Diet. 2016, 116, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Krebs-Smith, S.M.; Guenther, P.M.; Subar, A.F.; Kirkpatrick, S.I.; Dodd, K.W. Americans do not meet federal dietary recommendations. J. Nutr. 2010, 140, 1832–1838. [Google Scholar] [CrossRef] [PubMed]
- Banfield, E.C.; Liu, Y.; Davis, J.S.; Chang, S.; Frazier-Wood, A.C. Poor adherence to US dietary guidelines for children and adolescents in the national health and nutrition examination survey population. J. Acad. Nutr. Diet. 2016, 116, 21–27. [Google Scholar] [CrossRef]
- Kimmons, J.; Gillespie, C.; Seymour, J.; Serdula, M.; Blanck, H.M. Fruit and vegetable intake among adolescents and adults in the United States: Percentage meeting individualized recommendations. Medscape J. Med. 2009, 11, 26. [Google Scholar]
- Lutfiyya, M.N.; Chang, L.F.; Lipsky, M.S. A cross-sectional study of US rural adults’ consumption of fruits and vegetables: Do they consume at least five servings daily? BMC Public Health 2012, 12, 1. [Google Scholar] [CrossRef] [PubMed]
- Kamphuis, C.B.; Giskes, K.; de Bruijn, G.J.; Wendel-Vos, W.; Brug, J.; van Lenthe, F.J. Environmental determinants of fruit and vegetable consumption among adults: A systematic review. Br. J. Nutr. 2006, 96, 620–635. [Google Scholar] [PubMed]
- Savoie-Roskos, M.; Durward, C.; Jeweks, M.; Blanck, H.M. Reducing food insecurity and improving fruit and vegetable intake among farmers’ market incentive program participants. J. Nutr. Educ. Behav. 2016, 48, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Bowling, A.B.; Moretti, M.; Ringelheim, K.; Tran, A.; Davison, K. Healthy Foods, Healthy Families: Combining incentives and exposure interventions at urban farmers’ markets to improve nutrition among recipients of US federal food assistance. Health Promot. Perspect. 2016, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, S.; Bost, A.; McGonigle, M.; Rosen, L.; Peterson-Kosecki, A.; Colon-Ramos, U.; Robien, K. Fruit and vegetable intake among participants in a District of Columbia farmers’ market incentive programme. Public Health Nutr. 2018, 21, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Almaguer, S.B.; Law, Y.; Young, C. Healthier Corner Stores: Positive Impacts and Profitable Changes. Available online: http://thefoodtrust.org/uploads/media_items/healthier-corner-stores-positive-impacts-and-profitable-changes.original.pdf (accessed on 3 December 2018).
- Langellier, B.A.; Garza, J.R.; Prelip, M.L.; Glik, D.; Brookmeyer, R.; Ortega, A.N. Corner Store Inventories, Purchases, and Strategies for Intervention: A Review of the Literature. Calif. J. Health Promot. 2013, 11, 1–13. [Google Scholar] [PubMed]
- Ortega, A.N.; Albert, S.L.; Chan-Golston, A.M.; Langellier, B.A.; Glik, D.C.; Belin, T.R.; Garcia, R.E.; Brookmeyer, R.; Sharif, M.Z.; Prelip, M.L. Substantial improvements not seen in health behaviors following corner store conversions in two Latino food swamps. BMC Public Health 2016, 16, 389. [Google Scholar] [CrossRef] [PubMed]
- Lawman, H.G.; Vander Veur, S.; Mallya, G.; McCoy, T.A.; Wojtanowski, A.; Colby, L.; Sanders, T.A.; Lent, M.R.; Sandoval, B.A.; Sherman, S.; et al. Changes in quantity, spending, and nutritional characteristics of adult, adolescent and child urban corner store purchases after an environmental intervention. Prev. Med. 2015, 74, 81–85. [Google Scholar] [CrossRef]
- Song, H.; Gittelsohn, J.; Kim, M.; Suratkar, S.; Sharma, S.; Anliker, J. A corner store intervention in a low-income urban community is associated with increased availability and sales of some healthy foods. Public Health Nutr. 2009, 12, 2060–2067. [Google Scholar] [CrossRef] [PubMed]
- Adam, A.; Jensen, J.D. What is the effectiveness of obesity related interventions at retail grocery stores and Supermarkets?—A systematic review. BMC Public Health 2016, 16, 1247. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.H.; Finkelstein, E.A.; Katz, D.L.; Jankowiak, N.; Pudlewski, C.; Paluch, R.A. Effects of nutrient profiling and price changes based on NuVal® scores on food purchasing in an online experimental Supermarket. Public Health Nutr. 2015, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Surkan, P.J.; Tabrizi, M.J.; Lee, R.M.; Palmer, A.M.; Frick, K.D. Eat Right—Live Well! Supermarket Intervention Impact on Sales of Healthy Foods in a Low-Income Neighborhood. J. Nutr. Educ. Behav. 2016, 48, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Foster, G.D.; Karpyn, A.; Wojtanowsk, A.C.; Davis, E.; Weiss, S.; Brensinger, C.; Tierney, A.; Guo, W.; Brown, J.; Spross, C.; et al. Placement and promotion strategies to increase sales of healthier products in supermarkets in low-income, ethnically diverse neighborhoods: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 99, 1359–1368. [Google Scholar] [CrossRef]
- Drewnowski, A.; Rehm, C.D. Consumption of added sugars among US children and adults by food purchase location and food source. Am. J. Clin. Nutr. 2014, 100, 901–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drewnowski, A.; Rehm, C.D. Energy intakes of US children and adults by food purchase location and by specific food source. Nutr. J. 2013, 12, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivlin, G. Rigged: Supermarket Shelves for Sale. Center for Science in the Public Interest: Washington, DC, USA, 2016. Available online: https://www.thefreelibrary.com/Rigged!+Supermarket+shelves+for+sale.-a0469848741 (accessed on 3 December 2018).
- Cohen, D.A.; Collins, R.; Hunter, G.; Ghosh-Dastidar, B.; Dubowitz, T. Store Impulse Marketing Strategies and Body Mass Index. Am. J. Public Health 2014, 105, 1446–1452. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.A.; Babey, S.H. Contextual influences on eating behaviours: Heuristic processing and dietary choices. Obes. Rev. 2012, 13, 766–779. [Google Scholar] [CrossRef] [PubMed]
- Escaron, A.L.; Meinen, A.M.; Nitzke, S.A.; Martinez-Donate, A.P. Supermarket and grocery store-based interventions to promote healthful food choices and eating practices: A. systematic review. Prev. Chronic Dis. 2013, 10, E50. [Google Scholar] [CrossRef] [PubMed]
- Hartmann-Boyce, J.; Bianchi, F.; Piernas, C.; Riches, S.P.; Frie, K.; Nourse, R.; Jebb, S.A. Grocery store interventions to change food purchasing behaviors: A systematic review of randomized controlled trials. Am. J. Clin. Nutr. 2018, 107, 1004–1016. [Google Scholar] [CrossRef] [PubMed]
- Johnson III, J.A.; Johnson, A.M. Urban-rural differences in childhood and adolescent obesity in the United States: A systematic review and meta-analysis. Child. Obes. 2015, 11, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Befort, C.A.; Nazir, N.; Perri, M.G. Prevalence of obesity among adults from rural and urban areas of the United States: Findings from NHANES (2005–2008). J. Rural Health 2012, 28, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Jones, S.J.; Sun, H.; Merchant, A.T.; Cavicchia, P. Diet, physical activity, and sedentary behaviors as risk factors for childhood obesity: An urban and rural comparison. Child. Obes. 2012, 8, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Sallis, J.F.; Saelens, B.E.; Frank, L.D. Healthy nutrition environments: Concepts and measures. Am. J. Health Promot. 2005, 19, 330–343. [Google Scholar] [CrossRef] [PubMed]
- Caspi, C.E.; Sorensen, G.; Subramanian, S.; Kawachi, I. The local food environment and diet: A systematic review. Health Place 2012, 18, 1172–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marsh, M.; Alagona, P.S. (Eds.) AP Human Geography 2008; Barron’s Educational Series: Hauppauge, NY, USA, 2008. [Google Scholar]
- Zenk, S.N.; Lachance, L.L.; Schulz, A.J.; Mentz, G.; Kannan, S.; Ridella, W. Neighborhood retail food environment and fruit and vegetable intake in a multiethnic urban population. Am. J. Health Promot. 2009, 23, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Laraia, B.A.; Siega-Riz, A.M.; Kaufman, J.S.; Jones, S.J. Proximity of supermarkets is positively associated with diet quality index for pregnancy. Prev. Med. 2004, 39, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Michimi, A.; Wimberly, M.C. Associations of supermarket accessibility with obesity and fruit and vegetable consumption in the conterminous United States. Int. J. Health Geogr. 2010, 9, 49. [Google Scholar] [CrossRef] [PubMed]
- Morland, K.; Wing, S.; Diez Roux, A. The contextual effect of the local food environment on residents’ diets: The atherosclerosis risk in communities study. Am. J. Public Health 2002, 92, 1761–1767. [Google Scholar] [CrossRef]
- Thornton, L.E.; Crawford, D.; Ball, K. Neighbourhood-socioeconomic variation in women’s diet: The role of nutrition environments. Eur. J. Clin. Nutr. 2010, 64, 1423. [Google Scholar] [CrossRef]
- Aggarwal, A.; Cook, A.J.; Jiao, J.; Seguin, R.A.; Vernez Moudon, A.; Hurvitz, P.M.; Drewnowski, A. Access to supermarkets and fruit and vegetable consumption. Am. J. Public Health 2014, 104, 917–923. [Google Scholar] [CrossRef]
- Caspi, C.E.; Kawachi, I.; Subramanian, S.; Adamkiewicz, G.; Sorensen, G. The relationship between diet and perceived and objective access to supermarkets among low-income housing residents. Soc. Sci. Med. 2012, 75, 1254–1262. [Google Scholar] [CrossRef] [Green Version]
- An, R.; Sturm, R. School and residential neighborhood food environment and diet among California youth. Am. J. Prev. Med. 2012, 42, 129–135. [Google Scholar] [CrossRef]
- Boone-Heinonen, J.; Gordon-Larsen, P.; Kiefe, C.I.; Shikany, J.M.; Lewis, C.E.; Popkin, B.M. Fast food restaurants and food stores: Longitudinal associations with diet in young to middle-aged adults: The CARDIA study. Arch. Intern. Med. 2011, 171, 1162–1170. [Google Scholar] [CrossRef] [PubMed]
- Abeykoon, A.H.; Engler-Stringer, R.; Muhajarine, N. Health-related outcomes of new grocery store interventions: A systematic review. Public Health Nutr. 2017, 20, 2236–2248. [Google Scholar] [CrossRef] [PubMed]
- Harnack, L.; Himes, J.H.; Anliker, J.; Clay, T.; Gittelsohn, J.; Jobe, J.B.; Ring, K.; Snyder, P.; Thompson, J.; Weber, J.L. Intervention-related bias in reporting of food intake by fifth-grade children participating in an obesity prevention study. Am. J. Epidemiol. 2004, 160, 1117–1121. [Google Scholar] [CrossRef] [PubMed]
- Miller, T.M.; Abdel-Maksoud, M.F.; Crane, L.A.; Marcus, A.C.; Byers, T.E. Effects of social approval bias on self-reported fruit and vegetable consumption: A randomized controlled trial. Nutr. J. 2008, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Kristal, A.R.; Andrilla, C.; Koepsell, T.; Diehr, P.H.; Cheadle, A. Dietary assessment instruments are susceptible to intervention-associated response set bias. J. Am. Diet. Assoc. 1998, 98, 40–43. [Google Scholar] [CrossRef]
- Thornton, L.E.; Pearce, J.R.; Macdonald, L.; Lamb, K.E.; Ellaway, A. Does the choice of neighbourhood supermarket access measure influence associations with individual-level fruit and vegetable consumption? A case study from Glasgow. Int. J. Health Geogr. 2012, 11, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogus, S.; Athens, J.; Cantor, J.; Elbel, B. Measuring micro-level effects of a new supermarket: Do residents within 0.5 mile have improved dietary behaviors? J. Acad. Nutr. Diet. 2018, 118, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Cobb, L.K.; Appel, L.J.; Franco, M.; Jones-Smith, J.C.; Nur, A.; Anderson, C.A.M. The relationship of the local food environment with obesity: A systematic review of methods, study quality, and results. Obesity 2015, 23, 1331–1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- County Health Rankings and Roadmaps, 2018. University of Wisconsin Population Health Institute, Robert Wood Johnson Foundation, and Burness. Available online: http://www.countyhealthrankings.org/ (accessed on 3 December 2018).
- Census Tract Level State Maps of the Modified Retail Food Environment Index (mRFEI). National Center for Chronic Disease Prevention and Health Promotion. Division of Nutrition, Physical Activity, and Obesity. Available online: ftp://ftp.cdc.gov/pub/Publications/dnpao/census-tract-level-state-maps-mrfei_TAG508.pdf (accessed on 3 December 2018).
- World Traffic Service. ESRI. 2018. Available online: https://www.arcgis.com/home/item.html?id = ff11eb5b930b4fabba15c47feb130de4 (accessed on 3 December 2018).
- Greene, G.W.; Resnicow, K.; Thompson, F.E.; Peterson, K.E.; Hurley, T.G.; Hebert, J.R.; Toobert, D.J.; Williams, G.C.; Elliot, D.L.; Goldman Sher, T.; et al. Correspondence of the NCI Fruit and Vegetable Screener to repeat 24-H recalls and serum carotenoids in behavioral intervention trials. J. Nutr. 2008, 138, 200S–204S. [Google Scholar] [CrossRef] [PubMed]
- Ermakov, I.V.; Whigham, L.D.; Redelfs, A.H.; Stookey, L.J.; Bernstein, P.S.; Gellermann, W. Skin carotenoids as biomarker for vegetable and fruit intake: Validation of the reflection-spectroscopy based “Veggie Meter”. FASEB J. 2016, 30, 409.3. [Google Scholar]
- Ermakov, I.V.; Gellermann, W. Dermal carotenoid measurements via pressure mediated reflection spectroscopy. J. Biophotonics 2012, 5, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Jilcott Pitts, S.B.; Jahns, L.; Wu, Q.; Moran, N.E.; Bell, R.A.; Truesdale, K.P.; Laska, M.N. A non-invasive assessment of skin carotenoid status through reflection spectroscopy is a feasible, reliable and potentially valid measure of fruit and vegetable consumption in a diverse community sample. Public Health Nutr. 2018, 21, 1664–1670. [Google Scholar] [CrossRef] [PubMed]
- Cooksey-Stowers, K.; Schwartz, M.B.; Brownell, K.D. Food swamps predict obesity rates better than food deserts in the United States. Int. J. Environ. Res. Public Health 2017, 14, 1366. [Google Scholar] [CrossRef] [PubMed]
- Spence, C.; Okajima, K.; Cheok, A.D.; Petit, O.; Michel, C. Eating with our eyes: From visual hunger to digital satiation. Brain Cogn. 2016, 110, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Paeratakul, S.; Ferdinand, D.P.; Champagne, C.M.; Ryan, D.H.; Bray, G.A. Fast-food consumption among US adults and children: Dietary and nutrient intake profile. J. Am. Diet. Assoc. 2003, 103, 1332–1338. [Google Scholar] [CrossRef]
- Bowman, S.A.; Vinyard, B.T. Fast food consumption of US adults: Impact on energy and nutrient intakes and overweight status. J. Am. Coll. Nutr. 2004, 23, 163–168. [Google Scholar] [CrossRef]
- Jago, R.; Baranowski, T.; Baranowski, J.C. Fruit and vegetable availability: A micro environmental mediating variable? Public Health Nutr. 2007, 10, 681–689. [Google Scholar] [CrossRef]
- Basiotis, P.P.; Kramer-LeBlanc, C.S.; Kennedy, E.T. Maintaining nutrition security and diet quality: The role of the Food Stamp Program and WIC. Fam. Econ. Nutr. Rev. 1998, 11, 4. [Google Scholar]
- Rose, D.; Habicht, J.; Devaney, B. Household participation in the Food Stamp and WIC programs increases the nutrient intakes of preschool children. J. Nutr. 1998, 128, 548–555. [Google Scholar] [CrossRef]
- Pomeranz, J.L.; Chriqui, J.F. The Supplemental Nutrition Assistance Program: Analysis of program administration and food law definitions. Am. J. Prev. Med. 2015, 49, 428–436. [Google Scholar] [CrossRef]
- Zhang, F.F.; Liu, J.; Rehm, C.; Wilde, P.; Mande, J.; Mozaffarian, D. Trends and Disparities in Diet Quality Among US Adults by Supplemental Nutrition Assistance Program Participation Status. JAMA Network Open 2018, E180237. [Google Scholar] [CrossRef]
- Ludwig, J.; Sanbonmatsu, L.; Gennetian, L.; Adam, E.; Duncan, G.J.; Katz, L.F.; Kessler, R.C.; Kling, J.R.; Lindau, S.T.; Whitaker, R.C.; et al. Neighborhoods, obesity, and diabetes—A randomized social experiment. N. Engl. J. Med. 2011, 365, 1509–1519. [Google Scholar] [CrossRef]
- Drewnowski, A.; Aggarwal, A.; Hurvitz, P.M.; Monsivais, P.; Moudon, A.V. Obesity and supermarket access: Proximity or price? Am. J. Public Health 2012, 102, e74–e80. [Google Scholar] [CrossRef]
- Gustafson, A.; Christian, J.W.; Lewis, S.; Moore, K.; Jilcott, S. Food outlet choice, consumer food environment, but not food outlet availability within daily travel patterns are associated with dietary intake among adults, Lexington Kentucky 2011. Nutr. J. 2013, 12, 17. [Google Scholar] [CrossRef]
- Wiig, K.; Smith, C. The art of grocery shopping on a food stamp budget: Factors influencing the food choices of low-income women as they try to make ends meet. Public Health Nutr. 2009, 12, 1726–1734. [Google Scholar] [CrossRef]
- Dammann, K.W.; Smith, C. Factors affecting low-income women’s food choices and the perceived impact of dietary intake and socioeconomic status on their health and weight. J. Nutr. Educ. Behav. 2009, 41, 242–253. [Google Scholar] [CrossRef]
- McGuirt, J.T.; Jilcott Pitts, S.B.; Ward, R.; Crawford, T.W.; Keyserling, T.C.; Ammerman, A.S. Examining the influence of price and accessibility on willingness to shop at farmers’ markets among low-income eastern North Carolina women. J. Nutr. Educ. Behav. 2014, 46, 26–33. [Google Scholar] [CrossRef]
- Jackson, P.; Del Aguila, R.P.; Clarke, I.; Hallsworth, A.; De Kervenoael, R.; Kirkup, M. Retail restructuring and consumer choice 2. Understanding consumer choice at the household level. Environ. Plan. A 2006, 38, 47–67. [Google Scholar] [CrossRef]
- Jackson, P.A.; Rowlands, M.; Miller, D. Shopping, Place and Identity; Routledge: London, UK, 21 May 1998. [Google Scholar]
- Longevity Link Corporation. The VEGGIE METER®-Skin Carotenoids as Indicator of Fruit and Vegetable Intake and Biomarker Associated with Better Health. Available online: http://www.longevitylinkcorporation.com/products.html (accessed on 3 December 2018).
- Couillard, C.; Lemieux, S.; Vohl, M.C.; Couture, P.; Lamarche, B. Carotenoids as biomarkers of fruit and vegetable intake in men and women. Br. J. Nutr. 2016, 116, 1206–1215. [Google Scholar] [CrossRef] [Green Version]
- El-Sohemy, A.; Baylin, A.; Kabagambe, E.; Ascherio, A.; Spiegelman, D.; Campos, H. Individual carotenoid concentrations in adipose tissue and plasma as biomarkers of dietary intake. Am. J. Clin. Nutr. 2002, 76, 172–179. [Google Scholar] [CrossRef]
- Mayne, S.T.; Cartmel, B.; Scarmo, S.; Jahns, L.; Ermakov, I.V.; Gellermann, W. Resonance Raman spectroscopic evaluation of skin carotenoids as a biomarker of carotenoid status for human studies. Arch. Biochem. Biophys. 2013, 539, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Jilcott Pitts, S.B.; Wu, Q.; McGuirt, J.T.; Crawford, T.W.; Keyserling, T.C.; Ammerman, A.S. Associations between access to farmers’ markets and supermarkets, shopping patterns, fruit and vegetable consumption and health indicators among women of reproductive age in eastern North Carolina, USA. Public Health Nutr. 2013, 16, 1944–1952. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Mean (SD) or Number (%) |
|---|---|
| Sex | |
| Males | 33 (24.2%) |
| Females | 103 (75.7%) |
| Age (years) | 46.4 (15.0) |
| Race | |
| Black/African American | 117 (86.0%) |
| White | 14 (10.3%) |
| Other | 5 (3.7%) |
| Receive SNAP | 53 (39.0%) |
| Receive WIC | 12 (9.0%) |
| Education High School or less | 51 (37.5%) |
| Annual Income (<$40,000) | 101 (74.2%) |
| Children in Household | 1.2 (1.6) |
| Frequency of Shopping at outlet (once per week or more) | 114 (84.4%) |
| NCI Fruit, servings per day | 1.5 (2.1) |
| NCI Vegetables, servings per day | 1.8 (1.9) |
| BMI (kg/m2) | 32.8 (7.9) |
| Skin Carotenoids, RS Device | 250.5 (75.4) |
| GIS distance to supermarket from home to supermarket surveyed (miles) | 4.0 (7.7) |
| GIS distance to supermarket from home to supermarket surveyed (min) | 9.0 (9.7) |
| GIS distance to closest supermarket (miles) | 1.2 (3.3) |
| GIS distance to closest supermarket (min) | 4.6 (5.2) |
| mRFEI | 9.9 (12.4) |
| mRFEI healthy stores | 3 (2.9) |
| mRFEI less healthy stores | 21 (12.0) |
| Food Environment Measure | RS Device Fruit and Vegetable Consumption | Mean Vegetable Consumption Self-Reported | Mean Vegetable Consumption-(Minus Fried Potatoes) Self-Reported | Mean Fruit Consumption, Self-Reported |
|---|---|---|---|---|
| Distance to supermarket where surveyed (miles) | 0.01; p = 0.89 | −0.17; p = 0.12 | −0.15; p = 0.14 | −0.30; p = 0.002 |
| Time to supermarket shopped (min) | −0.007; p = 0.94 | −0.16; p = 0.13 | −0.15; p = 0.15 | −0.30; p = .004 |
| Distance to closest supermarket | −0.01; p = 0.87 | 0.07; p = 0.51 | 0.09; p = 0.39 | −0.13; p = 0.19 |
| Distance to closest supercenter | 0.07; p = 0.43 | −0.10; p = 0.34 | −0.09; p = 0.43 | −0.20; p = 0.06 |
| mRFEI | 0.13; p = 0.15 | −0.09; p = 0.38 | −0.12; p = 0.25 | −0.05; p = 0.64 |
| mRFEI Healthy Outlets | 0.02; p = 0.76 | −0.02; p = 0.89 | −0.05; p = 0.66 | 0.0007; p = 0.99 |
| mRFEI Unhealthy Outlets | −0.07; p = 0.43 | 0.11; p = 0.29 | 0.11; p = 0.29 | 0.08; p = 0.45 |
| mRFEI Service Area 1 mile | −0.11; p = 0.24 | −0.05; p = 0.67 | −0.06; p = 0.61 | 0.07; p = 0.48 |
| mRFEI Service Area 3 mile | −0.09; p = 0.33 | 0.002; p = 0.98 | 0.01; p = 0.89 | 0.03; p = 0.79 |
| mRFEI Service Area 5 mile | −0.06; p = 0.50 | 0.02; p = 0.80 | 0.04; p = 0.75 | 0.04; p = 0.72 |
| Supermarket Density 1 mile | −0.02; p = 0.83 | −0.03; p = 0.80 | −0.03; p = 0.75 | 0.11; p = 0.26 |
| Supermarket Density 3 mile | −0.07; p = 0.41 | 0.17; p = 0.11 | 0.14; p = 0.16 | 0.23; p = .02 |
| Supermarket Density 5 mile | −0.01; p = 0.94 | 0.09; p = 0.39 | 0.07; p = 0.52 | 0.15; p = 0.15 |
| Dependent Variable | Independent Variable | Parameter Estimate | Standard Error | t-Value | p-Value | r-Squared |
|---|---|---|---|---|---|---|
| Carotenoids (RS Device) | Distance to supermarket where surveyed (inverse) | −7.6 | 4.9 | −1.53 | 0.13 | 0.2 |
| Carotenoids (RS Device) | mRFEI (linear) | 1.26 | 0.53 | 2.38 | 0.02 * | 0.05 |
| Carotenoids (RS Device) | mRFEI Healthy Outlets (cubic) | 0.55 | 0.30 | 1.82 | 0.07 | 0.04 |
| Carotenoids (RS Device) | mRFEI Unhealthy Outlets (cubic) | −0.005 | 0.003 | −1.651 | 0.10 | 0.04 |
| Carotenoids (RS Device) | mRFEI Local Service Area 1 mile (quadratic) | 2.21 × 10−2 | 7.23 × 10−3 | 3.05 | 0.003 ** | 0.12 |
| Carotenoids (RS Device) | mRFEI Local Service Area 3 mile (quadratic) | 0.04 | 0.02 | 1.971 | 0.05 * | 0.06 |
| Carotenoids (RS Device) | mRFEI Local Service Area 5 mile (cubic) | −0.01 | 0.02 | −0.618 | 0.54 | 0.04 |
| Carotenoids (RS Device) | Supermarket Density 1 mile (quad) | 1.596 × 10−6 | 2.272 × 10−6 | 0.703 | 0.49 | 0.009 |
| Carotenoids (RS Device) | Supermarket Density 3 mile (cubic) | 0.2396 | 0.2189 | 1.095 | 0.276 | 0.03 |
| Carotenoids (RS Device) | Supermarket Density 5 mile (cubic) | −0.005455 | 0.025213 | −0.216 | 0.829 | 0.01417 |
| * p-value ≤ 0.05; ** p-value ≤ 0.01 | ||||||
| Independent Variables | Estimate | Standard Error | t-Value | p-Value |
|---|---|---|---|---|
| Intercept | 266.5 | 30.5 | 8.75 | 2.68 × 10−14 |
| Age | −0.26 | 0.60 | −0.44 | 0.66 |
| Gender | −46.3 | 19.2 | −2.4 | 0.01 ** |
| Race | −34.5 | 41.7 | −0.83 | 0.41 |
| Outlet | −19.02 | 16.9 | −1.13 | 0.26 |
| WIC | 55.4 | 25.3 | 2.19 | 0.03 * |
| SNAP | −13.24 | 17.5 | −0.76 | 0.45 |
| Reasons for Shopping: Near Home excluding near Work | 2.9 | 16.7 | 0.18 | 0.86 |
| mRFEI Local Service Area 1 mile | −6.02 | 173.28 | −0.04 | 0.97 |
| mRFEI Local Service Area 3 mile | 2.4 | 0.79 | 3.08 | 0.003 ** |
| Supermarket Distance (miles) (inverse) | −5.34 | 4.91 | −1.09 | 0.28 |
| (F = 2.186, p = 0.03), with an R2 of 0.26 * p-value ≤ 0.05; ** p-value ≤ 0.01 | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McGuirt, J.T.; Jilcott Pitts, S.B.; Gustafson, A. Association between Spatial Access to Food Outlets, Frequency of Grocery Shopping, and Objectively-Assessed and Self-Reported Fruit and Vegetable Consumption. Nutrients 2018, 10, 1974. https://doi.org/10.3390/nu10121974
McGuirt JT, Jilcott Pitts SB, Gustafson A. Association between Spatial Access to Food Outlets, Frequency of Grocery Shopping, and Objectively-Assessed and Self-Reported Fruit and Vegetable Consumption. Nutrients. 2018; 10(12):1974. https://doi.org/10.3390/nu10121974
Chicago/Turabian StyleMcGuirt, Jared T., Stephanie B. Jilcott Pitts, and Alison Gustafson. 2018. "Association between Spatial Access to Food Outlets, Frequency of Grocery Shopping, and Objectively-Assessed and Self-Reported Fruit and Vegetable Consumption" Nutrients 10, no. 12: 1974. https://doi.org/10.3390/nu10121974