Changes in Dietary Intake and Adherence to the NU-AGE Diet Following a One-Year Dietary Intervention among European Older Adults—Results of the NU-AGE Randomized Trial

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
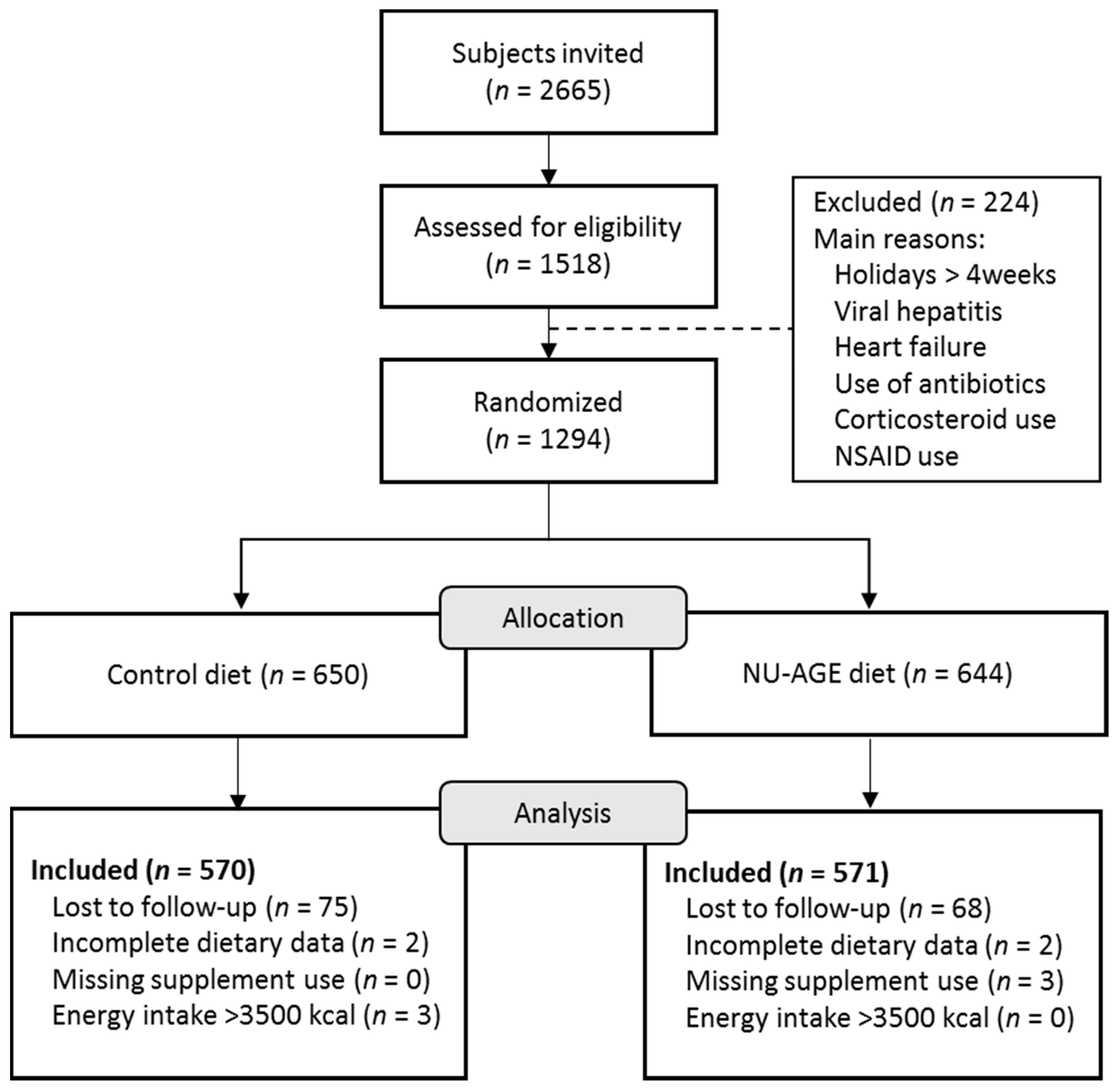
2.1. Study Design
2.2. Dietary Intervention
2.3. Dietary Assessment
2.4. Other Variables
2.5. NU-AGE Index
2.5.1. Food Based Dietary Guidelines for the Elderly Population
2.5.2. Definition of Food Groups
2.5.3. Choice of Cut-Offs and Scoring
2.6. Statistical Analyses
3. Results
3.1. General Characteristics
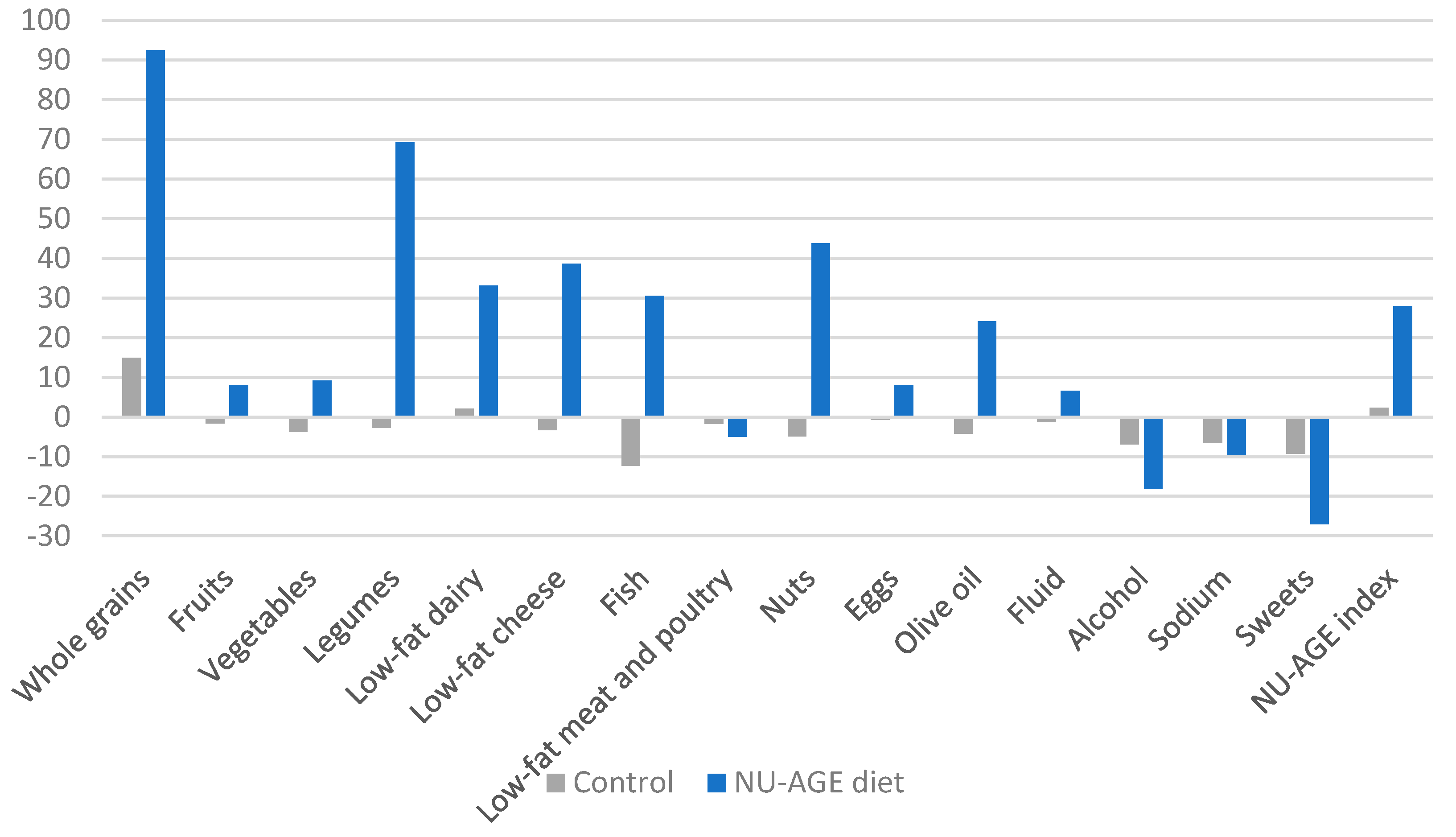
3.2. Changes in Dietary Intake by Intervention Group
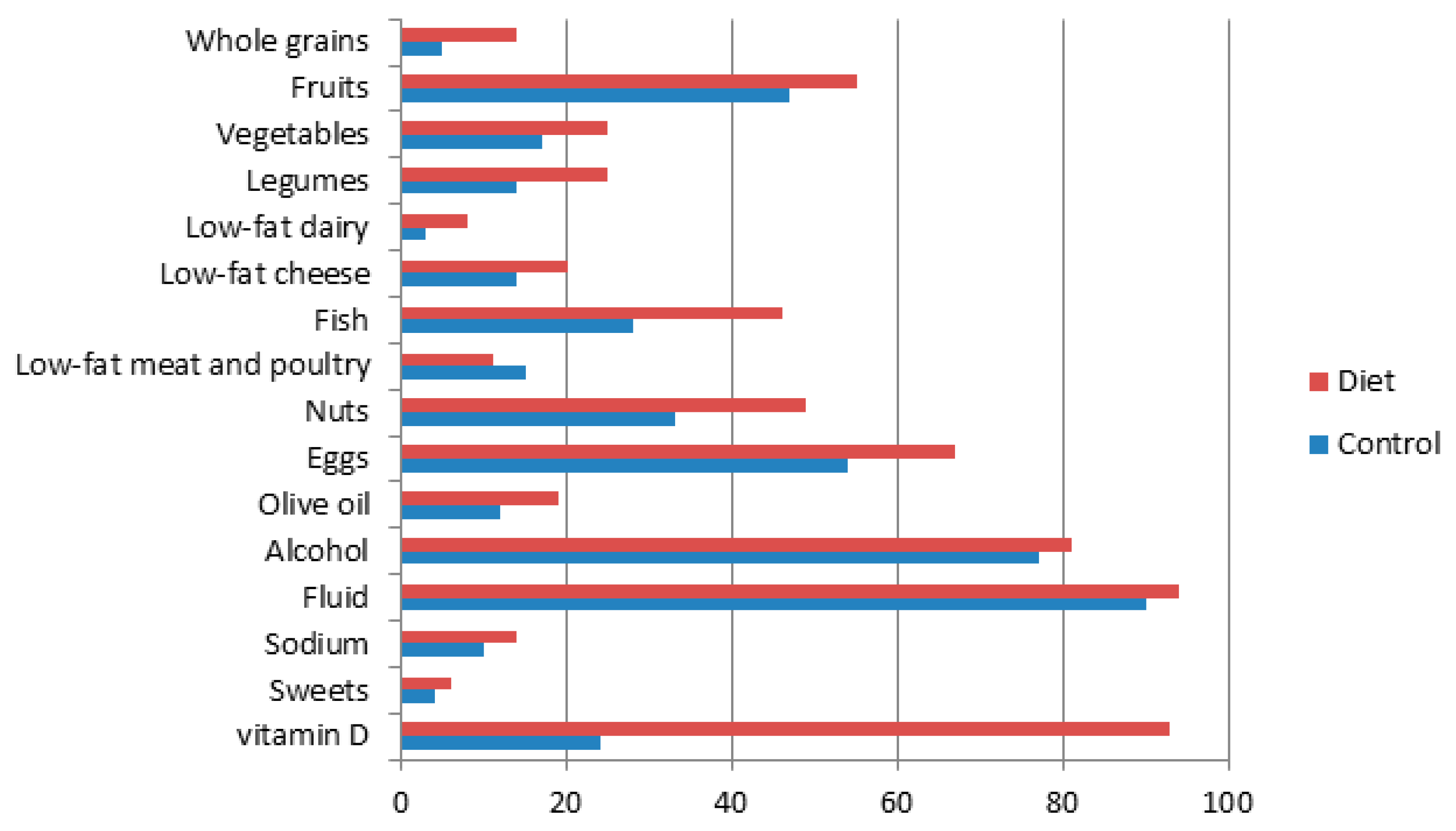
3.3. Achievement of the NU-AGE Guidelines by Intervention Group
3.4. Country Specific Changes in Dietary Intake
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Eurostat. Europop2010—Convergence Scenario, National Level—Assumptions. Available online: http://epp.eurostat.ec.europa.eu/portal/page/portal/population/data/database (accessed on 25 September 2013).
- Cevenini, E.; Monti, D.; Franceschi, C. Inflamm-ageing. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 14–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franceschi, C.; Bonafè, M.; Valensin, S.; Olivieri, F.; De Luca, M.; Ottaviani, E.; De Benedictis, G. Inflamm-aging: An evolutionary perspective on immunosenescence. Ann. N. Y. Acad. Sci. 2000, 908, 244–254. [Google Scholar] [CrossRef]
- Franceschi, C.; Capri, M.; Monti, D.; Giunta, S.; Olivieri, F.; Sevini, F.; Panourgia, M.P.; Invidia, L.; Celani, L.; Scurti, M.; et al. Inflammaging and anti-inflammaging: A systemic perspective on aging and longevity emerged from studies in humans. Mech. Ageing Dev. 2007, 128, 92–105. [Google Scholar] [CrossRef] [PubMed]
- Bouwens, M.; van de Rest, O.; Dellschaft, N.; Bromhaar, M.G.; de Groot, L.C.; Geleijnse, J.M.; Muller, M.; Afman, L.A. Fish-oil supplementation induces antiinflammatory gene expression profiles in human blood mononuclear cells. Am. J. Clin. Nutr. 2009, 90, 415–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraguljac, N.V.; Montori, V.M.; Pavuluri, M.; Chai, H.S.; Wilson, B.S.; Unal, S.S. Efficacy of omega-3 fatty acids in mood disorders—A systematic review and metaanalysis. Psychopharmacol. Bull. 2009, 42, 39–54. [Google Scholar] [PubMed]
- Paddon-Jones, D.; Rasmussen, B.B. Dietary protein recommendations and the prevention of sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Staehelin, H.B.; Orav, J.E.; Stuck, A.E.; Theiler, R.; Wong, J.B.; Egli, A.; Kiel, D.P.; Henschkowski, J. Fall prevention with supplemental and active forms of vitamin d: A meta-analysis of randomised controlled trials. BMJ 2009, 339, b3692. [Google Scholar] [CrossRef] [Green Version]
- Hin, H.; Clarke, R.; Sherliker, P.; Atoyebi, W.; Emmens, K.; Birks, J.; Schneede, J.; Ueland, P.M.; Nexo, E.; Scott, J.; et al. Clinical relevance of low serum vitamin b12 concentrations in older people: The banbury b12 study. Age Ageing 2006, 35, 416–422. [Google Scholar] [CrossRef]
- Sato, Y.; Honda, Y.; Iwamoto, J.; Kanoko, T.; Satoh, K. Effect of folate and mecobalamin on hip fractures in patients with stroke: A randomized controlled trial. JAMA 2005, 293, 1082–1088. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Lowe, G.D.; Rumley, A.; Bruckdorfer, K.R.; Whincup, P.H. Associations of vitamin c status, fruit and vegetable intakes, and markers of inflammation and hemostasis. Am. J. Clin. Nutr. 2006, 83, 567–574; quiz 726-567. [Google Scholar] [CrossRef]
- Vinas, B.R.; Barba, L.R.; Ngo, J.; Gurinovic, M.; Novakovic, R.; Cavelaars, A.; de Groot, L.C.; van’t Veer, P.; Matthys, C.; Majem, L.S. Projected prevalence of inadequate nutrient intakes in Europe. Ann. Nutr. Metab. 2011, 59, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Ocke, M.C.; Buurma-Rethans, E.J.; De Boer, E.J.; Wilson-Van den Hooven, C.; Etemad-Ghameslou, Z.; Drijvers, J.J.; Van Rossum, C.T. Diet of Community-Dwelling Older Adults: Dutch National Food Consumption Survey Older Adults 2010–2012; RIVM: Bilthoven, The Netherlands, 2013; p. 127. [Google Scholar]
- Jacobs, D.R., Jr.; Steffen, L.M. Nutrients, foods, and dietary patterns as exposures in research: A framework for food synergy. Am. J. Clin. Nutr. 2003, 78, 508S–513S. [Google Scholar] [CrossRef] [PubMed]
- Jacques, P.F.; Tucker, K.L. Are dietary patterns useful for understanding the role of diet in chronic disease? Am. J. Clin. Nutr. 2001, 73, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Alles, B.; Samieri, C.; Feart, C.; Jutand, M.A.; Laurin, D.; Barberger-Gateau, P. Dietary patterns: A novel approach to examine the link between nutrition and cognitive function in older individuals. Nutr. Res. Rev. 2012, 25, 207–222. [Google Scholar] [CrossRef] [PubMed]
- De Lorgeril, M.; Renaud, S.; Mamelle, N.; Salen, P.; Martin, J.L.; Monjaud, I.; Guidollet, J.; Touboul, P.; Delaye, J. Mediterranean alpha-linolenic acid-rich diet in secondary prevention of coronary heart disease. Lancet 1994, 343, 1454–1459. [Google Scholar] [CrossRef]
- Estruch, R.; Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Ruiz-Gutierrez, V.; Covas, M.I.; Fiol, M.; Gomez-Gracia, E.; Lopez-Sabater, M.C.; Vinyoles, E.; et al. Effects of a mediterranean-style diet on cardiovascular risk factors: A randomized trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, S.A.; Bates, C.J.; Mishra, G.D. Diet quality is associated with all-cause mortality in adults aged 65 years and older. J. Nutr. 2012, 142, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Panunzio, M.F.; Caporizzi, R.; Antoniciello, A.; Cela, E.P.; Ferguson, L.R.; D’Ambrosio, P. Randomized, controlled nutrition education trial promotes a mediterranean diet and improves anthropometric, dietary, and metabolic parameters in adults. Ann. Ig. 2011, 23, 13–25. [Google Scholar]
- Trichopoulou, A.; Orfanos, P.; Norat, T.; Bueno-de-Mesquita, B.; Ocke, M.C.; Peeters, P.H.; van der Schouw, Y.T.; Boeing, H.; Hoffmann, K.; Boffetta, P.; et al. Modified mediterranean diet and survival: Epic-elderly prospective cohort study. BMJ 2005, 330, 991. [Google Scholar] [CrossRef]
- Talegawkar, S.A.; Bandinelli, S.; Bandeen-Roche, K.; Chen, P.; Milaneschi, Y.; Tanaka, T.; Semba, R.D.; Guralnik, J.M.; Ferrucci, L. A higher adherence to a mediterranean-style diet is inversely associated with the development of frailty in community-dwelling elderly men and women. J. Nutr. 2012, 142, 2161–2166. [Google Scholar] [CrossRef]
- Valls-Pedret, C.; Sala-Vila, A.; Serra-Mir, M.; Corella, D.; de la Torre, R.; Martinez-Gonzalez, M.A.; Martinez-Lapiscina, E.H.; Fito, M.; Perez-Heras, A.; Salas-Salvado, J.; et al. Mediterranean diet and age-related cognitive decline: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to mediterranean diet and health status: Meta-analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef] [PubMed]
- De Lorgeril, M.; Salen, P. New insights into the health effects of dietary saturated and omega-6 and omega-3 polyunsaturated fatty acids. BMC Med. 2012, 10, 50. [Google Scholar] [CrossRef] [PubMed]
- Martucci, M.; Ostan, R.; Biondi, F.; Bellavista, E.; Fabbri, C.; Bertarelli, C.; Salvioli, S.; Capri, M.; Franceschi, C.; Santoro, A. Mediterranean diet and inflammaging within the hormesis paradigm. Nutr. Rev. 2017, 75, 442–455. [Google Scholar] [CrossRef] [PubMed]
- Berendsen, A.M.; Santoro, A.; Pini, E.; Cevenini, E.; Ostan, R.; Pietruszka, B.; Rolf, K.; Cano, N.; Caille, A.; Lyon-Belgy, N.; et al. Reprint of: A parallel randomized trial on the effect of a healthful diet on inflammageing and its consequences in European elderly people: Design of the nu-age dietary intervention study. Mech. Ageing Dev. 2014, 136–137, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Pini, E.; Scurti, M.; Palmas, G.; Berendsen, A.; Brzozowska, A.; Pietruszka, B.; Szczecinska, A.; Cano, N.; Meunier, N.; et al. Combating inflammaging through a mediterranean whole diet approach: The nu-age project’s conceptual framework and design. Mech. Ageing Dev. 2014, 136–137, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Rollnick, S. Motivational Interviewing: Preparing People for Change; The Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Prochaska, J.O.; DiClemente, C.C. Transtheoretical therapy: Toward a more integrative model of change. Psychother. Theory Res. Pract. 1982, 19, 276–288. [Google Scholar] [CrossRef]
- Health Council of the Netherlands. Dietary Reference Intakes: Calcium, Vitamin D, Thiamin, Riboflavin, Niacin, Pantothenic Acid, and Biotin; Health Council of the Netherlands: The Hague, The Netherlands, 2000; p. 180.
- Health Council of the Netherlands. Towards an Adequate Intake of Vitamin D; Health Council of the Netherlands: The Hague, The Netherlands, 2008; p. 172.
- Istituto Nazionale di Ricerca per gli Alimenti e la Nutrizione. Istituto Nazionale di Ricerca per gli Alimenti e la Nutrizione. Available online: http://www.inran.it/ (accessed on 3 August 2011).
- Department of Health. Report on Health & Social Subjects 41 Dietary Reference Values for Food Energy and Nutrients for the United Kingdom; Health Council of the Netherlands: London, UK, 1991.
- Health Council of the Netherlands. Guidelines for a Healthy Diet 2006; Health Council of the Netherlands: The Hague, The Netherlands, 2006.
- Jarosz, M.; Bulhak-Jachymczyk, B. Normy Zywienia Czlowieka. Podstawy Prewencji Otylosci i Chorob Niezakaznych/Nutrition Recommendations. Basis for the Prevention of Obesity and Non-Communicable Dieseases; Wydawnictwo Lekarskie PZWL/National Food and Nutrition Institute: Warsaw, Poland, 2008. [Google Scholar]
- Ministère du Travail, de l’Emploi et de la Santé, French National Nutrition and Health Program 2011–2015. Available online: http://www.sante.gouv.fr/IMG/pdf/French_National_Nutrition_and_Health_Program_2011-2015.pdf (accessed on 3 August 2011).
- Rhee, J.J.; Sampson, L.; Cho, E.; Hughes, M.D.; Hu, F.B.; Willett, W.C. Comparison of methods to account for implausible reporting of energy intake in epidemiologic studies. Am. J. Epidemiol. 2015, 181, 225–233. [Google Scholar] [CrossRef]
- Coulston, A.M.; Boushey, C.J. Nutrition in the Prevention and Treatment of Disease, 2nd ed.; Elsevier Academie Press: Burlington, VT, USA, 2008. [Google Scholar]
- Willett, W.C. Nutritional Epidemiology, 3rd ed.; Oxford University Press: Oxford, UK, 2013; Volume IX, p. 529. [Google Scholar]
- RIVM/Voedingscentrum. Nevo-Tabel; Nederlands Voedingsstoffenbestand 2011; RIVM/Voedingscentrum: Den Haag, The Netherlands, 2011. [Google Scholar]
- Food Standards Agency. Mccance and Widdowson’s the Composition of Foods; The Royal Society of Chemistry: Cambridge, UK, 2002.
- Tabelle INRAN di Composizione degli Alimenti. Banca dati di Composizione degli Alimenti per Studi Epidemiologici in Italia (bda). Available online: http://online.scuola.zanichelli.it/cappellivannucchi/tabelle-inran-di-composizione-degli-alimenti/ (accessed on 3 August 2011).
- Food Composition Database for Epidemiological Studies in Italy (Banca Dati di Composizione degli Alimenti per Studi Epidemiologici in Italia–BDA). Available online: http://www.bda-ieo.it/wordpress/?page_id=146 (accessed on 3 August 2011).
- Kunachowicz, H.; Przygoda, B.; Nadolna, I.; Iwanow, K. Tabele Skladu i Wartosci Odzywczej Zywnosci/Food Composition Tables; Wydawnictwo Lekarskie PZWL/National Food and Nutrition Institute: Warsaw, Poland, 2005. [Google Scholar]
- ANSES. Ciqual French Food Composition Table Version 2016; French Agency for Food Environmental and Occupational Health Safety: Maisons-Alfort, France, 2016.
- Washburn, R.A.; Smith, K.W.; Jette, A.M.; Janney, C.A. The physical activity scale for the elderly (pase): Development and evaluation. J. Clin. Epidemiol. 1993, 46, 153–162. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Food and Nutrition Council. Nederlandse Normen 1989/Dutch Dietary Reference Values 1989; Health Council of the Netherlands: The Hague, The Netherlands, 1992.
- Health Council of the Netherlands. Dietary Reference Intakes: Energy, Proteins, Fats and Digestible Carbohydrates; Health Council of the Netherlands: The Hague, The Netherlands, 2001.
- Health Council of the Netherlands. Dietary Reference Intakes: Vitamin B6, Folic Acid, and Vitamin B12; Health Council of the Netherlands: The Hague, The Netherlands, 2003.
- Health Council of the Netherlands. Guideline for Dietary Fiber Intake; Health Council of the Netherlands: The Hague, The Netherlands, 2006.
- AFSSA; CNERNA-CNRS. Apports Nutritionnels Conseillés pour la Population Française, 3rd ed.; Tec et Doc Lavoisier: Paris, France, 2001; p. 608. [Google Scholar]
- Peregrin, T. Getting to know the modified mypyramid for older adults. J. Am. Diet. Assoc. 2008, 108, 937–938. [Google Scholar] [CrossRef] [PubMed]
- Shelnutt, K.P.; Bobroff, L.B.; Diehl, D.C. Mypyramid for older adults. J. Nutr. Educ. Behav. 2009, 41, 300–302. [Google Scholar] [CrossRef] [PubMed]
- Commission of the European Communities. Nutrient and Energy Intakes for the European Community; European Food Safety Authority (EFSA), Scientific Committee for Food: Luxembourg, 1993. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes. The Essential Guide to Nutrient Requirements; The National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- NetWISP v4.0. Tinuviel Software. Vol. 4.0. Available online: http://www.tinuvielsoftware.co.uk/ (accessed on 3 August 2011).
- Wajszczyk, B.; Chwojnowska, Z.; Chabros, E.; Nasiadko, D.; Rybaczuk, M. Instrukcja Programu Dieta-5 do Planowania i Bieżącej Oceny Żywienia Indywidualnego/Dieta-5 Manual for Planning and Dietary Assessment of Individuals; National Food and Nutrition Institute: Warsaw, Poland, 2011. [Google Scholar]
- Van Lee, L.; Geelen, A.; van Huysduynen, E.J.; de Vries, J.H.; van’t Veer, P.; Feskens, E.J. The Dutch healthy diet index (dhd-index): An instrument to measure adherence to the Dutch guidelines for a healthy diet. Nutr. J. 2012, 11, 49. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, A.; Nelson, M.E.; Tucker, K.L.; Layne, J.; Johnson, E.; Nuernberger, A.; Castaneda, C.; Judge, J.O.; Buchner, D.; Singh, M.F. A home-based nutrition intervention to increase consumption of fruits, vegetables, and calcium-rich foods in community dwelling elders. J. Am. Diet. Assoc. 2002, 102, 1421–1427. [Google Scholar] [CrossRef]
- Zazpe, I.; Sanchez-Tainta, A.; Estruch, R.; Lamuela-Raventos, R.M.; Schroder, H.; Salas-Salvado, J.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; Aros, F.; et al. A large randomized individual and group intervention conducted by registered dietitians increased adherence to mediterranean-type diets: The predimed study. J. Am. Diet. Assoc. 2008, 108, 1134–1144. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Polyunsaturated fatty acids, inflammatory processes and inflammatory bowel diseases. Mol. Nutr. Food Res. 2008, 52, 885–897. [Google Scholar] [CrossRef] [PubMed]
- De Munter, J.S.; Hu, F.B.; Spiegelman, D.; Franz, M.; van Dam, R.M. Whole grain, bran, and germ intake and risk of type 2 diabetes: A prospective cohort study and systematic review. PLoS Med. 2007, 4, e261. [Google Scholar] [CrossRef] [Green Version]
- Mellen, P.B.; Walsh, T.F.; Herrington, D.M. Whole grain intake and cardiovascular disease: A meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 283–290. [Google Scholar] [CrossRef]
- Gaesser, G.A. Carbohydrate quantity and quality in relation to body mass index. J. Am. Diet. Assoc. 2007, 107, 1768–1780. [Google Scholar] [CrossRef]
- Pan, A.; Yu, D.; Demark-Wahnefried, W.; Franco, O.H.; Lin, X. Meta-analysis of the effects of flaxseed interventions on blood lipids. Am. J. Clin. Nutr. 2009, 90, 288–297. [Google Scholar] [CrossRef] [Green Version]
- Maillot, M.; Issa, C.; Vieux, F.; Lairon, D.; Darmon, N. The shortest way to reach nutritional goals is to adopt mediterranean food choices: Evidence from computer-generated personalized diets. Am. J. Clin. Nutr. 2011, 94, 1127–1137. [Google Scholar] [CrossRef] [PubMed]
- Wibisono, C.; Probst, Y.; Neale, E.; Tapsell, L. Impact of food supplementation on weight loss in randomised-controlled dietary intervention trials: A systematic review and meta-analysis. Br. J. Nutr. 2016, 115, 1406–1414. [Google Scholar] [CrossRef] [PubMed]
- Lara, J.; Evans, E.H.; O’Brien, N.; Moynihan, P.J.; Meyer, T.D.; Adamson, A.J.; Errington, L.; Sniehotta, F.F.; White, M.; Mathers, J.C. Association of behaviour change techniques with effectiveness of dietary interventions among adults of retirement age: A systematic review and meta-analysis of randomised controlled trials. BMC Med. 2014, 12, 177. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Ros, E.; Covas, M.I.; Fiol, M.; Warnberg, J.; Aros, F.; Ruiz-Gutierrez, V.; Lamuela-Raventos, R.M.; et al. Cohort profile: Design and methods of the predimed study. Int. J. Epidemiol. 2010, 41, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Troyer, J.L.; Racine, E.F.; Ngugi, G.W.; McAuley, W.J. The effect of home-delivered dietary approach to stop hypertension (dash) meals on the diets of older adults with cardiovascular disease. Am. J. Clin. Nutr. 2010, 91, 1204–1212. [Google Scholar] [CrossRef] [PubMed]
- Ostan, R.; Guidarelli, G.; Giampieri, E.; Lanzarini, C.; Berendsen, A.A.M.; Januszko, O.; Jennings, A.; Lyon, N.; Caumon, E.; Gillings, R.; et al. Cross-Sectional Analysis of the Correlation Between Daily Nutrient Intake Assessed by 7-Day Food Records and Biomarkers of Dietary Intake Among Participants of the NU-AGE Study. Front. Physiol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Bowman, G.L.; Shannon, J.; Ho, E.; Traber, M.G.; Frei, B.; Oken, B.S.; Kaye, J.A.; Quinn, J.F. Reliability and validity of food frequency questionnaire and nutrient biomarkers in elders with and without mild cognitive impairment. Alzheimer Dis. Assoc. Disord. 2011, 25, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Bazzocchi, A.; Guidarelli, G.; Ostan, R.; Giampieri, E.; Mercatelli, D.; Scurti, M.; Berendsen, A.; Surala, O.; Jennings, A.; et al. A cross-sectional analysis of body composition among healthy elderly from the European NU-AGE study: sex and country specific features. Front. Physiol. 2018, 9, 1693. [Google Scholar] [CrossRef]
- Jeruszka-Bielak, M.; Kollajtis-Dolowy, A.; Santoro, A.; Ostan, R.; Berendsen, A.A.M.; Jennings, A.; Meunier, N.; Marseglia, A.; Caumon, E.; Gillings, R.; et al. Are Nutrition-Related Knowledge and Attitudes Reflected in Lifestyle and Health Among Elderly People? A Study Across Five European Countries. Front. Physiol. 2018. [Google Scholar] [CrossRef]
- Jennings, A.; Cashman, K.D.; Gillings, R.; Cassidy, A.; Tang, J.; Fraser, W.; Dowling, K.G.; Hull, G.L.J.; Berendsen, A.A.M.; de Groot, L.C.P.G.M.; et al. A Mediterranean-like dietary pattern with vitamin D3 (10 µg/d) supplements reduced the rate of bone loss in older Europeans with osteoporosis at baseline: results of a 1-y randomized controlled trial. Am. J. Clin. Nutr. 2018. [Google Scholar] [CrossRef]
- Marseglia, A.; Xu, W.; Fratiglioni, L.; Fabbri, C.; Berendsen, A.A.M.; Bialecka-Debek, A.; Jennings, A.; Gillings, R.; Meunier, N.; Caumon, E.; et al. Effect of the NU-AGE Diet on Cognitive Functioning in Older Adults: A Randomized Controlled Trial. Front. Physiol. 2018. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Component | Servings | Scoring | |||
|---|---|---|---|---|---|
| Minimum Score (0) | Lower Range b (1–10) | Maximum Score (10) | Upper Range c (10–1) | ||
| Wholemeal bread and wholegrain pasta or rice a | Bread 4–6 servings/day (140–210 g/day) Pasta/rice 2 × 80 g/week (23 g/day) | Max | 1–163g | 163–233 g | 233-max |
| Fruits | 2 servings/day (240 g/day) | 0 g | 0–240 g | ≥240 g | |
| Vegetables | 300 g/day | 0 g | 0–300 g | ≥300 g | |
| Legumes | 200 g/week (29 g/day) | 0 g | 0–29 g | ≥29 g | |
| Low-fat dairy | 500 mL/day | 0 g | 0–500 g | ≥500 g | |
| Low-fat cheese | 30 g/day | 0 g | 0–30 g | ≥30 g | |
| Fish | 2 times 125 g/week (36 g/day) | 0 g | 0–36 g | ≥36 g | |
| Low-fat meat and poultry a | 4 times 125 g/week (71 g/day) | Max | 0–71 g | 71–125 g | 125-max |
| Nuts | 2 times 20g/week (6 g/day) | 0 g | 0–6 g | >6 g | |
| Eggs | 2–4 eggs/week (14–28 g/day) | 0 g | 0–14 g | >14g | |
| Olive oil | 20 g/day | 0 mL | 0–20 mL | ≥20 mL | |
| Fluid | 1500 mL/day | <1000 mL | 1000–1500 mL | >1500 mL | |
| vitamin D | Use supplement (10 µg/day) | No | Yes | ||
| Alcohol | Max 2 servings/day for men and 1 serving/day for women | >10 g for women >20 g for men | ≤10 g for women ≤20 g for men | ||
| Salt a | 5 g/day (2000 mg/day sodium) | ≥85th | 0–1500 mg | 1500–2000 mg | 2000–85th |
| Sweets a | Limited use | ≥85th | 0 | 0–85th | |
| Control (n = 570) | NU-AGE Diet (n = 571) | p | |
|---|---|---|---|
| Men | 262 (46) | 248 (43) | 0.39 |
| Age | 71.1 ± 3.9 | 70.7 ± 4.0 | 0.11 |
| Current occupation a | 0.23 | ||
| Employed | 19 (3.4) | 24 (4.2) | |
| Retired | 540 (94.7) | 541 (94.7) | |
| Other | 11 (2.1) | 6 (1.1) | |
| Education (years) | 12.6 ± 3.6 | 12.7 ± 3.6 | 0.62 |
| BMI (kg/m2) | 26.7 ± 3.7 | 26.7 ± 4.1 | 0.89 |
| Physical activity (MET score) | 135.1 ± 57.4 | 132.5 ± 54.9 | 0.43 |
| Multivitamin use | 67 (11.8) | 86 (15.1) | 0.10 |
| Nutrient intake | |||
| Energy, Kcal | 1899 ± 448 | 1854 ± 432 | 0.08 |
| Carbohydrates, EN% | 46.9 ± 7.9 | 47.3 ± 7.2 | 0.29 |
| Carbohydrates, g | 221.9 ± 62.6 | 218.8 ± 60.2 | 0.41 |
| Protein, EN% | 16.3 ± 2.4 | 16.5 ± 2.8 | 0.14 |
| Protein, g | 76.3 ± 17.8 | 75.3 ± 17.7 | 0.36 |
| Fat, EN% | 34.3 ± 5.4 | 34.1 ± 5.5 | 0.56 |
| Fat, g | 72.6 ± 21.8 | 70.4 ± 20.8 | 0.08 |
| Current smokers | 21 (7.9) | 26 (9.7) | 0.46 |
| Pre-frail | 101 (17.8) | 137 (24.0) | 0.01 |
| Prevalence of diseases | |||
| Hypertension | 222 (39.0) | 242 (42.4) | 0.25 |
| Heart disease | 97 (17.0) | 94 (16.5) | 0.58 |
| Diabetes Mellitus type 2 | 26 (4.6) | 29 (5.1) | 0.69 |
| Hypercholesterolemia | 142 (24.9) | 154 (27.0) | 0.43 |
| Neurological disease | 12 (2.1) | 17 (3.0) | 0.39 |
| Osteoporosis | 59 (10.4) | 70 (12.3) | 0.25 |
| Control Group(n = 570) | NU-AGE Diet Group (n = 571) | Difference in Change between Groups | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NU-AGE Components | Baseline | Follow-Up | Change | p | Baseline | Follow-Up | Change | p | p | |
| Whole grains (g/day) | 54.4 ± 53.9 | 62.6 ± 60.7 | 8.1 ± 57.4 | 0.02 | 55.7 ± 58.3 | 107.2 ± 66.4 | 51.5 ± 62.5 | <0.01 | 43.3 ± 64.7 | <0.01 |
| Fruits (g/day) | 260.0 ± 158.7 | 255.7 ± 154.0 | −4.3 ± 156.3 | 0.64 | 248.2 ± 140.2 | 268.2 ± 140.0 | 20.1 ± 140.1 | 0.02 | 24.4 ± 127.3 | <0.01 |
| Vegetables (g/day) | 221.4 ± 120.7 | 213.2 ± 125.7 | −8.2 ± 123.2 | 0.26 | 214.5 ± 110.8 | 234.2 ± 103.7 | 19.7 ± 107.3 | <0.01 | 27.9 ± 110.6 | <0.01 |
| Legumes (g/day) | 11.1 ± 20.0 | 10.8 ± 19.2 | −0.3 ± 19.6 | 0.77 | 10.4 ± 20.9 | 17.6 ± 21.9 | 7.2 ± 21.5 | <0.01 | 7.5 ± 25.6 | <0.01 |
| Low-fat dairy (g/day) | 155.0 ± 154.6 | 158.2 ± 177.5 | 3.2 ± 166.4 | 0.74 | 173.0 ± 163.2 | 230.3 ± 174.4 | 57.3 ± 168.9 | <.001 | 54.1 ± 131.8 | <0.01 |
| Low-fat cheese (g/day) | 11.9 ± 21.9 | 11.6 ± 19.6 | −0.39 ± 20.8 | 0.75 | 12.7 ± 26.6 | 17.6 ± 24.9 | 4.9 ± 25.8 | <0.01 | 5.3 ± 23.1 | <0.01 |
| Fish (g/day) | 28.4 ± 29.3 | 24.9 ± 23.2 | −3.5 ± 26.4 | 0.02 | 28.4 ± 25.3 | 37.1 ± 28.1 | 8.7 ± 26.7 | <0.01 | 12.3 ± 32.4 | <0.01 |
| Low-fat meat and poultry (g/day) | 41.2 ± 33.4 | 40.5 ± 31.4 | −0.71 ± 32.4 | 0.71 | 40.5 ± 31.6 | 38.5 ± 27.9 | −2.0 ± 29.8 | 0.26 | −1.3 ± 34.7 | 0.53 |
| Nuts (g/day) | 6.4 ± 12.8 | 6.1 ± 9.9 | −0.31 ± 11.4 | 0.65 | 5.7 ± 10.7 | 8.3 ± 9.4 | 2.5 ± 10.1 | <0.01 | 2.8 ± 11.1 | <0.01 |
| Eggs (g/day) | 17.5 ± 17.0 | 17.3 ± 17.2 | −0.13 ± 17.1 | 0.90 | 17.3 ± 17.6 | 18.7 ± 13.9 | 1.4 ± 15.9 | 0.13 | 1.5 ± 18.4 | 0.16 |
| Olive oil (g/day) | 9.4 ± 9.9 | 8.9 ± 9.9 | −0.39 ± 9.9 | 0.50 | 9.1 ± 9.2 | 11.3 ± 8.9 | 2.2 ± 9.1 | <0.01 | 2.6 ± 8.0 | <0.01 |
| Fluid (mL/day) | 2311 ± 654 | 2282 ± 651 | −28.8 ± 652 | 0.46 | 2329 ± 671 | 2482 ± 657 | 154 ± 664 | <0.01 | 182 ± 469 | <0.01 |
| Vitamin D, n (%) | 81 (14.2) | 138 (24.2) | 75 (10) | <0.01 | 84 (14.7) | 529 (92.6) | 445 (77.9) | <0.01 | 370 (67.9) | <0.01 |
| Alcohol (g/day) | 9.6 ± 10.9 | 8.9 ± 10.9 | −0.66 ± 10.9 | 0.31 | 8.8 ± 10.3 | 7.2 ± 9.1 | −1.6 ± 9.7 | <0.01 | −0.92 ± 6.6 | 0.02 |
| Sodium (mg/day) | 2628 ± 1365 | 2455 ± 965 | −173 ± 1182 | <0.01 | 2554 ± 1500 | 2309 ± 946 | −245 ± 1254 | <0.01 | −72.1 ± 1271 | 0.34 |
| Sweets (g/day) | 84.1 ± 113.7 | 76.3 ± 102.3 | −7.8 ± 108.1 | 0.22 | 87.2 ± 103.5 | 63.6 ± 82.8 | −23.6 ± 93.7 | <0.01 | 15.8 ± 91.7 | <0.01 |
| NU-AGE index | 82.6 ± 16.5 | 84.6 ± 16.1 | 1.9 ± 16.3 | 0.05 | 82.6 ± 15.3 | 105.7 ± 17.6 | 23.1 ± 16.2 | <0.01 | 21.3 ± 15.9 | <0.01 |
| Italy (n = 114 Control, 127 Diet) | UK (n = 126 Control, 126 Diet) | The Netherlands (n = 124 Control, 117 Diet) | Poland (n = 106 Control, 114 Diet) | France (n = 100 Control, 87 Diet) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| NU-AGE Components | Group | Baseline | Change | Baseline | Change | Baseline | Change | Baseline | Change | Baseline | Change |
| Whole grains (g/day) | Control | 30.8 ± 42.9 | 0.52 ± 39.4 | 60.3 ± 41.1 | 23.5 ± 54.4 2 | 71.4 ± 61.7 | 12.7 ± 60.2 | 74.2 ± 61.1 | 2.2 ± 64.4 | 31.8 ± 42.4 | −1.7 ± 41.9 |
| Diet | 23.1 ± 32.3 | 60.4 ± 41.5 2,b | 61.9 ± 46.4 | 34.2 ± 54.5 2 | 82.5 ± 64.2 | 34.1 ± 67.2 2,b | 78.9 ± 70.0 | 38.3 ± 73.2 2,b | 28.2 ± 42.3 | 104 ± 54.1 2,b | |
| Fruits (g/day) | Control | 293 ± 177 | 18.3 ± 182 | 259 ± 137 | −2.2 ± 136 | 234 ± 146 | 6.8 ± 145 | 228 ± 159 | −24.4 ± 152 | 290 ± 167 | −25.4 ± 153 |
| Diet | 278 ± 149 | 14.0 ± 144 | 259 ± 139 | 2.4 ± 140 | 235 ± 127 | 43.2 ± 129 2,a | 198 ± 121 | 9.5 ± 129 a | 273 ± 151 | 37.2 ± 142 b | |
| Vegetables (g/day) | Control | 216 ± 113 | −6.7 ± 112 | 208 ± 91.6 | 15.0 ± 97.2 | 165 ± 83.9 | −6.9 ± 80.9 | 282 ± 170 | −17.6 ± 183 | 249 ± 101 | −30.9 ± 97.6 1 |
| Diet | 216 ± 101 | 23.2 ± 96.3 a | 218 ± 105 | 10.1 ± 106 | 162 ± 77.9 | 25.5 ± 78.1 2,b | 261 ± 146 | 11.3 ± 137 | 217 ± 87.6 | 31.6 ± 84.2 2,b | |
| Legumes (g/day) | Control | 16.5 ± 23.1 | −2.3 ± 21.9 | 17.4 ± 22.4 | 2.2 ± 20.9 | 3.8 ± 12.6 | 1.5 ± 12.1 | 4.8 ± 14.1 | 0.3 ± 18.0 | 12.9 ± 21.3 | −4.2 ± 19.6 |
| Diet | 8.7 ± 10.9 | 2.7 ± 13.2 b | 19.9 ± 25.9 | 3.9 ± 25.4 | 3.4 ± 11.9 | 6.5 ± 17.2 2,a | 10.2 ± 29.5 | 8.4 ± 26.1 1,a | 8.6 ± 15.1 | 17.9 ± 18.1 2,b | |
| Low-fat dairy (g/day) | Control | 89.7 ± 103 | 1.1 ± 108 | 264 ± 162 | 31.2 ± 175 | 196 ± 166 | 8.0 ± 177 | 74.0 ± 93.1 | −20.9 ± 110 | 127 ± 138 | −10.0 ± 134 |
| Diet | 87.6 ± 93.7 | 45.8 ± 99.9 2,b | 278 ± 165 | 31.4 ± 168 | 256 ± 183 | 40.9 ± 183 a | 96.5 ± 102 | 61.3 ± 1312 2,b | 134 ± 140 | 128 ± 156 2,b | |
| Low-fat cheese (g/day) | Control | 0.17 ± 1.0 | 0.18 ± 2.15 | 2.2 ± 6.5 | 1.3 ± 8.2 | 9.6 ± 21.6 | −0.6 ± 19.2 | 30.2 ± 32.9 | −4.6 ± 30.6 | 21.3 ± 15.9 | 1.5 ± 17.3 |
| Diet | 1.46 ± 4.87 | 0.93 ± 5.27 | 2.76 ± 6.65 | 1.42 ± 7.5 | 6.5 ± 10.6 | 7.7 ± 11.9 2,b | 38.8 ± 46.8 | 10.0 ± 41.6 a | 17.5 ± 15.4 | 5.0 ± 14.3 1 | |
| Fish (g/day) | Control | 29.9 ± 28.8 | −2.2 ± 26.3 | 24.7 ± 23.5 | 5.2 ± 22.3 | 22.3 ± 26.2 | −3.0 ± 25.5 | 31.4 ± 40.7 | −8.9 ± 33.4 | 35.8 ± 23.3 | −11.0 ± 22.2 2 |
| Diet | 27.1 ± 23.1 | 17.1 ± 27.5 2,b | 29.5 ± 24.3 | 2.3 ± 23.4 a | 23.9 ± 24.9 | 5.3 ± 22.9 a | 31.0 ± 31.2 | 12.2 ± 33.1 2,b | 31.0 ± 21.2 | 12.5 ± 21.5 2,b | |
| Low-fat meat and poultry (g/day) | Control | 49.8 ± 35.9 | −2.6 ± 34.8 | 33.7 ± 26.6 | −0.83 ± 26.3 | 32.5 ± 25.4 | −0.7 ± 24.8 | 33.3 ± 36.2 | −0.36 ± 33.4 | 60.3 ± 34.1 | 1.3 ± 33.4 |
| Diet | 51.4 ± 28.9 | −2.1 ± 27.4 | 33.4 ± 31.8 | −1.7 ± 28.6 | 31.2 ± 24.3 | −1.66 ± 23.3 | 34.2 ± 32.3 | −3.7 ± 31.6 | 56.1 ± 33.2 | 0.45 ± 29.4 | |
| Nuts (g/day) | Control | 8.1 ± 14.4 | −0.14 ± 12.6 | 6.1 ± 11.8 | −0.19 ± 11.2 | 6.3 ± 11.6 | 0.2 ± 10.8 | 4.1 ± 8.4 | 0.9 ± 8.2 | 7.6 ± 16.7 | −2.7 ± 13.8 |
| Diet | 4.3 ± 10.7 | 0.00 ± 9.2 | 5.3 ± 8.3 | 4.1 ± 8.7 2,b | 6.8 ± 11.0 | 3.6 ± 11.1 1,a | 4.6 ± 8.2 | 3.3 ± 8.6 2,a | 8.4 ± 14.9 | 1.5 ± 12.3 a | |
| Eggs (g/day) | Control | 7.3 ± 8.7 | 1.7 ± 10.2 | 16.6 ± 15.5 | −0.64 ± 15.2 | 16.8 ± 17.3 | 0.86 ± 17.4 | 30.7 ± 20.3 | −2.8 ± 21.0 | 16.9 ± 12.9 | −0.1 ± 13.5 |
| Diet | 7.8 ± 7.7 | 1.5 ± 7.9 | 17.2 ± 15.4 | 6.7 ± 15.1 2,b | 14.8 ± 15.2 | 2.9 ± 14.4 | 28.4 ± 22.9 | −4.9 ± 19.2 | 20.2 ± 17.7 | 0.0 ± 15.3 | |
| Olive oil (g/day) | Control | 16.8 ± 8.5 | 1.0 ± 8.3 | 2.85 ± 2.97 | −0.16 ± 2.73 | 2.4 ± 3.5 | 0.19 ± 3.6 | 11.9 ± 10.7 | 0.13 ± 11.9 | 14.9 ± 10.8 | −3.6 ± 9.6 2 |
| Diet | 17.1 ± 6.7 | 1.2 ± 6.6 | 2.5 ± 2.5 | 2.0 ± 3.9 2,b | 3.2 ± 3.9 | 1.9 ± 4.5 2,b | 10.4 ± 8.9 | 2.1 ± 8.7 | 13.2 ± 11.8 | 4.2 ± 10.2 2,b | |
| Fluid (mL/day) | Control | 1756 ± 542 | 64.9 ± 552 | 2565 ± 623 | −80.5 ± 633 | 2438 ± 614 | −71.7 ± 607 | 2405 ± 605 | −68.9 ± 603 | 2367 ± 553 | 25.3 ± 595 |
| Diet | 1901 ± 588 | 144 ± 584 1 | 2721 ± 732 | 66.7 ± 719 b | 2356 ± 561 | 116 ± 574 b | 2451 ± 593 | 127 ± 580 b | 2189 ± 529 | 378 ± 546 2,b | |
| Alcohol (g/day) | Control | 8.1 ± 9.9 | −1.1 ± 9.6 | 10.9 ± 10.8 | −1.4 ± 10.7 | 13.4 ± 12.5 | 0.0 ± 12.8 | 3.9 ± 6.4 | −0.7 ± 6.1 | 10.6 ± 11.7 | −0.1 ± 11.7 |
| Diet | 9.0 ± 9.9 | −2.6 ± 8.8 1 | 9.6 ± 10.1 | −1.6 ± 9.4 | 11.9 ± 11.2 | 0.8 ± 11.5 | 3.7 ± 5.8 | −1.7 ± 4.9 1 | 9.5 ± 12.1 | −3.1 ± 10.4 b | |
| Salt (mg/day) | Control | 1731 ± 545 | −3.2 ± 543 | 2376 ± 879 | −162 ± 801 | 2435 ± 670 | −175 ± 677 1 | 3495 ± 1118 | −68.5 ± 1110 | 3289 ± 2282 | −489 ± 1711 1 |
| Diet | 1809 ± 698 | −173 ± 615 1,a | 2357 ± 679 | −295 ± 669 2 | 2323 ± 618 | −54.5 ± 577 | 3523 ± 1143 | −122 ± 1144 | 2968 ± 2988 | −695 ± 2166 1 | |
| Sweets (g/day) | Control | 43.6 ± 51.2 | 2.3 ± 56.7 | 137 ± 166 | −11.7 ± 156 | 83.6 ± 93.5 | −16.8 ± 82.4 | 96.3 ± 111 | −10.6 ± 97.7 | 51.1 ± 77.9 | 0.4 ± 91.8 |
| Diet | 55.5 ± 67.7 | −16.6 ± 61.7 1,a | 132 ± 129 | −49.8 ± 107 2,b | 79.5 ± 102 | −5.3 ± 106 | 104 ± 113 | −21.6 ± 102 | 56.4 ± 58.2 | −23.2 ± 51.6 2,a | |
| Vitamin D, n (%) | Control | 25 (21.9) | 17 (14.9) 1 | 12 (9.5) | 7 (5.6) | 15 (12) | 8 (6.6) | 22 (20.8) | 17 (16.0) 2 | 7 (7.0) | 8 (8.0) |
| Diet | 22 (17.3) | 83 (65.4) 2,b | 11 (8.7) | 108 (85.7) 2,b | 16 (13.7) | 88 (75.2) 2,b | 22 (19.3) | 83 (72.7) 2,b | 13 (14.9) | 68 (78.2) 2,b | |
| NU-AGE index | Control | 86.9 ± 14.9 | 2.5 ± 14.7 | 79.9 ± 15.2 | 6.7 ± 15.5 2 | 72.9 ± 15.8 | 3.6 ± 16.6 | 84.7 ± 17.2 | 0.53 ± 16.5 | 91.2 ± 12.9 | −5.4 ± 13.4 2 |
| Diet | 82.5 ± 15.4 | 21.2 ± 14.4 2,b | 81.5 ± 12.7 | 20.8 ± 13.9 2,b | 76.1 ± 15.4 | 20.3 ± 15.5 2,b | 86.1 ± 14.8 | 21.4 ± 15.2 2,b | 88.2 ± 15.8 | 35.6 ± 16.0 2,b | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berendsen, A.A.M.; Van de Rest, O.; Feskens, E.J.M.; Santoro, A.; Ostan, R.; Pietruszka, B.; Brzozowska, A.; Stelmaszczyk-Kusz, A.; Jennings, A.; Gillings, R.; et al. Changes in Dietary Intake and Adherence to the NU-AGE Diet Following a One-Year Dietary Intervention among European Older Adults—Results of the NU-AGE Randomized Trial. Nutrients 2018, 10, 1905. https://doi.org/10.3390/nu10121905
Berendsen AAM, Van de Rest O, Feskens EJM, Santoro A, Ostan R, Pietruszka B, Brzozowska A, Stelmaszczyk-Kusz A, Jennings A, Gillings R, et al. Changes in Dietary Intake and Adherence to the NU-AGE Diet Following a One-Year Dietary Intervention among European Older Adults—Results of the NU-AGE Randomized Trial. Nutrients. 2018; 10(12):1905. https://doi.org/10.3390/nu10121905
Chicago/Turabian StyleBerendsen, Agnes A. M., Ondine Van de Rest, Edith J. M. Feskens, Aurelia Santoro, Rita Ostan, Barbara Pietruszka, Anna Brzozowska, Agnieszka Stelmaszczyk-Kusz, Amy Jennings, Rachel Gillings, and et al. 2018. "Changes in Dietary Intake and Adherence to the NU-AGE Diet Following a One-Year Dietary Intervention among European Older Adults—Results of the NU-AGE Randomized Trial" Nutrients 10, no. 12: 1905. https://doi.org/10.3390/nu10121905