A Combined Dietary and Cognitive Intervention in 3–5-Year-Old Children in Indonesia: A Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
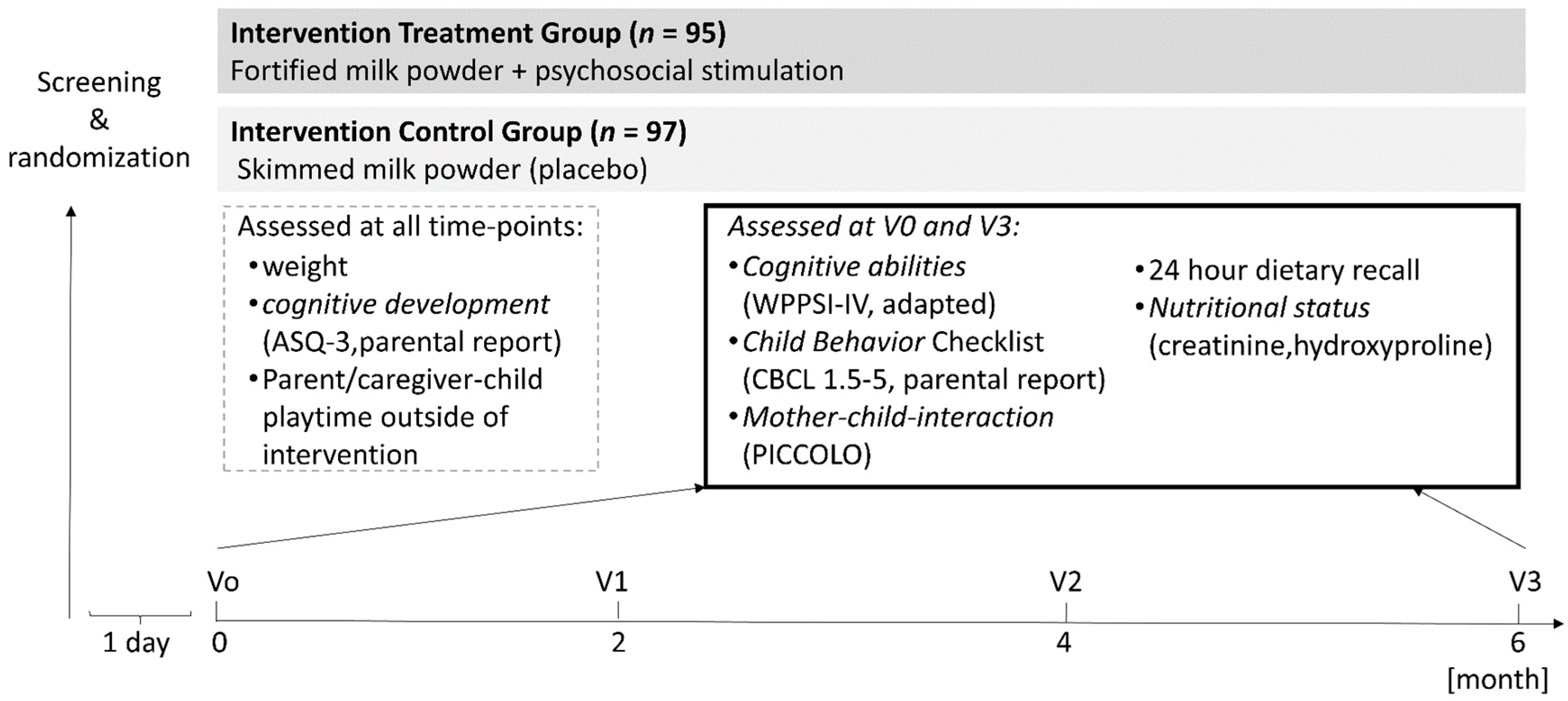
2.2. Experimental Design and Procedure
2.3. Psychosocial Stimulation
2.4. Cognitive, Behavioral, and Nutritional Assessments
2.5. Analysis
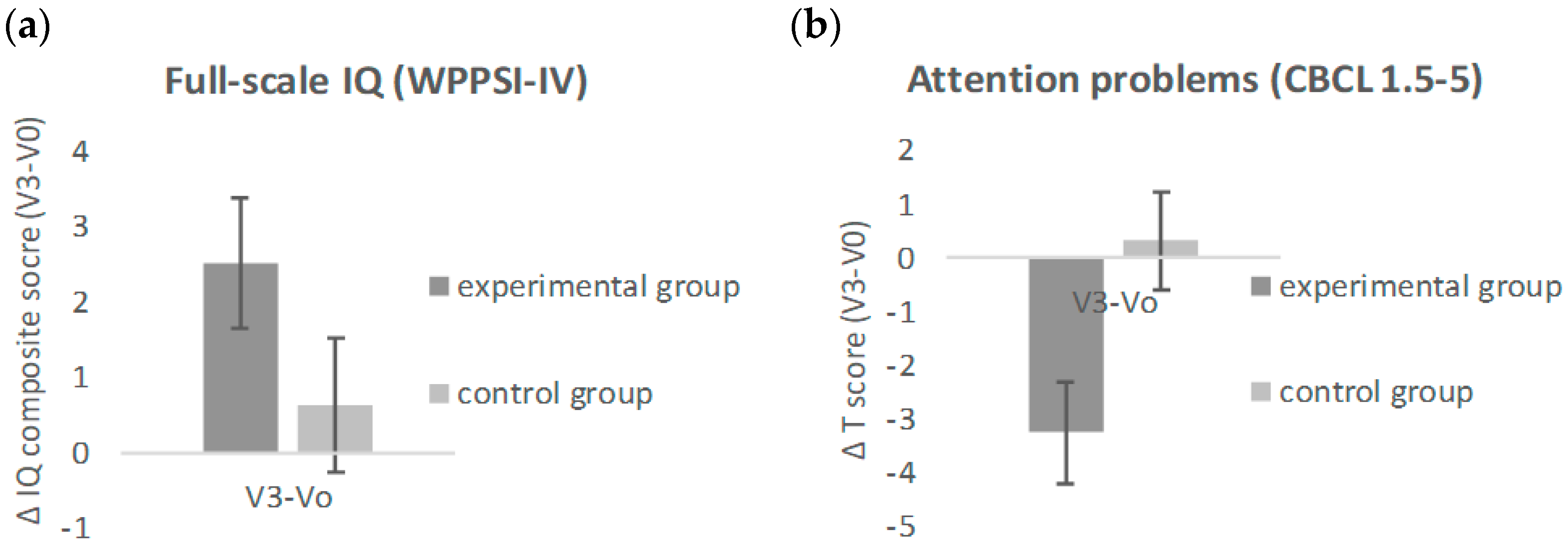
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Black, M.M.; Perez-Escamilla, R.; Rao, S.F. Integrating nutrition and child development interventions: Scientific basis, evidence of impact, and implementation considerations. Adv. Nutr. 2015, 6, 852–859. [Google Scholar] [CrossRef] [PubMed]
- Warsito, O.; Khomsan, A.; Hernawati, N.; Anwar, F. Relationship between nutritional status, psychosocial stimulation, and cognitive development in preschool children in Indonesia. Nutr. Res. Pract. 2012, 6, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Engle, P.L.; Black, M.M.; Behrman, J.R.; Cabral de Mello, M.; Gertler, P.J.; Kapiriri, L.; Martorell, R.; Eming Young, M. Child development in developing countries 3—Strategies to avoid the loss of developmental potential in more than 200 million children in the developing world. Lancet 2007, 369, 229–242. [Google Scholar] [CrossRef]
- Walker, S.P.; Grantham-McGregor, S.M.; Powell, C.A.; Chang, S.M. Effects of growth restriction in early childhood on growth, IQ, and cognition at age 11 to 12 years and the benefits of nutritional supplementation and psychosocial stimulation. J. Pediatr. 2000, 137, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Palmer, C.F.; Barba, C.V.C. Mental-development after dietary intervention—A study of Philippine children. J. Cross-Cult. Psychol. 1981, 12, 480–488. [Google Scholar] [CrossRef]
- Nores, M.; Barnett, W.S. Benefits of early childhood interventions across the world: (Under) Investing in the very young. Econ. Educ. Rev. 2010, 29, 271–282. [Google Scholar] [CrossRef]
- Yousafzai, A.K.; Aboud, F. Review of implementation processes for integrated nutrition and psychosocial stimulation interventions. Ann. N. Y. Acad. Sci. 2014, 1308, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Grantham-McGregor, S.M.; Fernald, L.C.H.; Kagawa, R.M.C.; Walker, S. Effects of integrated child development and nutrition interventions on child development and nutritional status. Ann. N. Y. Acad. Sci. 2014, 1308, 11–32. [Google Scholar] [CrossRef] [PubMed]
- Hertzman, C.; Wiens, M. Development and long-term outcomes: A population health perspective and summary of successful interventions. Soc. Sci. Med. 1996, 43, 1083–1095. [Google Scholar] [CrossRef]
- Hamadani, J.D.; Huda, S.N.; Khatun, F.; Grantham-McGregor, S.M. Psychosocial stimulation improves the development of undernourished children in rural Bangladesh. J. Nutr. 2006, 136, 2645–2652. [Google Scholar] [CrossRef] [PubMed]
- Martinez, S.; Naudeau, S.; Pereira, V. The promise of preschool in Africa: A randomised impact evaluation of early childhood development in rural Mozambique. J. Dev. Eff. 2012, 4, 580–581. [Google Scholar]
- Behrman, J.R.; Cheng, Y.M.; Todd, P.E. Evaluating preschool programs when length of exposure to the program varies: A nonparametric approach. Rev. Econ. Stat. 2004, 86, 108–132. [Google Scholar] [CrossRef]
- McKay, H.; Sinisterra, L.; McKay, A.; Gomez, H.; Lloreda, P. Improving cognitive ability in chronically deprived children. Science 1978, 200, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Perez Escamilla, R.; Pollitt, E. Growth improvements in children above 3 years of age—The Cali study. J. Nutr. 1995, 125, 885–893. [Google Scholar] [PubMed]
- Bernal, R.; Fernandez, C. Subsidized childcare and child development in Colombia: Effects of Hogares Comunitarios de Bienestar as a function of timing and length of exposure. Soc. Sci. Med. 2013, 97, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Grantham-McGregor, S.; Powell, C.; Walker, S.; Himes, J. Nutritional supplementation, psychosocial stimulation, and mental development of stunted children—The Jamaican study. Lancet 1991, 338, 1–5. [Google Scholar] [CrossRef]
- Grantham-McGregor, S.M.; Walker, S.P.; Chang, S.M.; Powell, C.A. Effects of early childhood supplementation with and without stimulation on later development in stunted Jamaican children. Am. J. Clin. Nutr. 1997, 66, 247–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, K.; Flores, R.; Fujiwara, J.; Lien, T.H.T. Early childhood development interventions and cognitive development of young children in rural Vietnam. J. Nutr. 2005, 135, 1918–1925. [Google Scholar] [CrossRef] [PubMed]
- Yousafzai, A.K.; Obradovic, J.; Rasheed, M.A.; Rizvi, A.; Portilla, X.A.; Tirado-Strayer, N.; Siyal, S.; Memon, U. Effects of responsive stimulation and nutrition interventions on children’s development and growth at age 4 years in a disadvantaged population in Pakistan: A longitudinal follow-up of a cluster-randomised factorial effectiveness trial. Lancet Glob. Health 2016, 4, E548–E558. [Google Scholar] [CrossRef]
- Magwaza, A.S.; Edwards, S.D. An evaluation of an integrated parent-effectiveness training and children’s enrichment programme for disadvantaged families. S. Afr. J. Psychol. 1999, 21, 21–25. [Google Scholar] [CrossRef]
- Kagitcibasi, C.; Sunar, D.; Bekman, S. Long-term effects of early intervention: Turkish low-income mothers and children. J. Appl. Dev. Psychol. 2001, 22, 333–361. [Google Scholar] [CrossRef]
- Bradley, R.H. The Home Inventory: Review and reflections. Adv. Child Dev. Behav. 1994, 25, 241–288. [Google Scholar] [PubMed]
- Clark, C.; Wiebe, S.; Sheffield, T.; Chevalier, N.; Nelson, J.; Espy, K. Charting Early Trajectories of Executive Control With the Shape School. Dev. Psychol. 2013, 49, 1481–1493. [Google Scholar] [CrossRef] [PubMed]
- Mezzacappa, E.; Buckner, J.; Felton, E. Prenatal cigarette exposure and infant learning stimulation as predictors of cognitive control in childhood. Dev. Sci. 2011, 14, 881–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackman, D.; Gallop, R.; Evans, G.; Farah, M. Socioeconomic status and executive function: Developmental trajectories and mediation. Dev. Sci. 2015, 18, 686–712. [Google Scholar] [CrossRef] [PubMed]
- Bradley, R.H.; Caldwell, B.M.; Rock, S.L.; Hamrick, H.M.; Harris, P. Home observation for measurement of the environment: Development of a home inventory for use with families having children 6 to 10 years old. Contemp. Educ. Psychol. 1988, 13, 58–71. [Google Scholar] [CrossRef]
- Nahar, B.; Hossain, M.I.; Hamadani, J.D.; Ahmed, T.; Grantham-McGregor, S.; Persson, L.-A. Effects of psychosocial stimulation on improving home environment and child-rearing practices: Results from a community-based trial among severely malnourished children in Bangladesh. BMC Public Health 2012, 12, 622. [Google Scholar] [CrossRef] [PubMed]
- McNamara, R.K.; Able, J.; Jandacek, R.; Rider, T.; Tso, P.; Eliassen, J.C.; Alfieri, D.; Weber, W.; Jarvis, K.; DelBello, M.P.; et al. Docosahexaenoic acid supplementation increases prefrontal cortex activation during sustained attention in healthy boys: A placebo-controlled, dose-ranging, functional magnetic resonance imaging study. Am. J. Clin. Nutr. 2010, 91, 1060–1067. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.S.; Nelson, E.B. Assessing the effect of docosahexaenoic acid on cognitive functions in healthy, preschool children: A randomized, placebo-controlled, double-blind study. Clin. Pediatr. 2008, 47, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Ivanovic, D.M.; Perez, H.T.; Olivares, M.G.; Diaz, N.S.; Leyton, B.D.; Ivanovic, R.M. Scholastic achievement: A multivariate analysis of nutritional, intellectual, socioeconomic, sociocultural, familial, and demographic variables in Chilean school-age children. Nutrition 2004, 20, 878–889. [Google Scholar] [CrossRef] [PubMed]
- Hubbs-Tait, L.; Kennedy, T.S.; Droke, E.A.; Belanger, D.M.; Parker, J.R. Zinc, iron, and lead: Relations to head start children’s cognitive scores and teachers’ ratings of behavior. J. Am. Diet. Assoc. 2007, 107, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Taves, D. Minimization: A new method of assigning patients to treatment and control groups. Clin. Pharmacol. Ther. 1974, 15, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Twombly, E.; Fink, G. ASQ-3 Learning Activities; Brooks Publishing: Baltimore, MD, USA, 2012; ISBN 978-1-59857-246-9. [Google Scholar]
- Osendarp, S.J.M.; Baghurst, K.I.; Bryan, J.; Calvaresi, E.; Hughes, D.; Hussaini, M.; Karyadi, S.J.M.; van Klinken, B.J.-W.; van der Knaap, H.C.M.; Lukito, W.; et al. Effect of a 12-mo micronutrient intervention on learning and memory in well-nourished and marginally nourished school-aged children: 2 parallel, randomized, placebo-controlled studies in Australia and Indonesia. Am. J. Clin. Nutr. 2007, 86, 1082–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malda, M.; Transler, C.; Van de Vijver, F.J.R.; Srinivas, K.; Sukumar, P.; Rao, K. Adapting a cognitive test for a different culture: An illustration of qualitative procedures. Psychol. Sci. Q. 2008, 50, 451–468. [Google Scholar]
- Jakob, L.; Bojanic, L.; Tsvetanova, D.D.; Buabang, E.K.; de Bles, N.J.; Sarafoglou, A.; Dijkzeul, A.; Del Pino, R. Study Protocol on Cognitive Performance in Bulgaria, Croatia, and the Netherlands: The Normacog Brief Battery. Front. Psychol. 2016, 7, 1658. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, R.G. Hydroxyproline creatinine ratio as an index of nutritional status and rate of growth. Lancet 1965, 2, 567–570. [Google Scholar] [CrossRef]
- Ackerman, P.L.; Beier, M.E.; Boyle, M.O. Working memory and intelligence: The same or different constructs? Psychol. Bull. 2005, 131, 30–60. [Google Scholar] [CrossRef] [PubMed]
- Ginsburg, K.R. The importance of play in promoting healthy child development and maintaining strong parent-child bonds. Pediatrics 2007, 119, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.N.; West, A.F.; Stein, A.; Malmberg, L.-E.; Bethell, K.; Barnes, J.; Sylva, K.; Leach, P. A comparison of father-infant interaction between primary and non-primary care giving fathers. Child Care Health Dev. 2009, 35, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Yiengprugsawan, V.; Banwell, C.; Takeda, W.; Dixon, J.; Seubsman, S.-A.; Sleigh, A.C. Health, happiness and eating together: What can a large Thai cohort study tell us? Glob. J. Health Sci. 2015, 7, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Cohn, D. Child-mother attachment of 6-year-olds and social competence at school. Child Dev. 1990, 61, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Henry, M. More than just play: The significance of mutually directed adult-child activity. Early Child Dev. Care 1990, 60, 35–51. [Google Scholar] [CrossRef]
- Bernier, A.; Carlson, S.; Deschêne, M.; Matt-Gagné, C. Social factors in the development of early executive functioning: A closer look at the caregiving environment. Dev. Sci. 2012, 15, 12–24. [Google Scholar] [CrossRef] [PubMed]
- French, J.R.P. Experiments in field settings. In Research Methods in the Behavioral Sciences; Festinger, L., Katz, D., Eds.; Holt, Rinehart & Winston: New York, NY, USA, 1953. [Google Scholar]
- Bramel, D.; Friend, R. Hawthorne, the myth of the docile worker and class bias in psychology. Am. Psychol. 1981, 36, 867–878. [Google Scholar] [CrossRef]
- Holden, J.D. Hawthorne effects and research into professional practice. J. Eval. Clin. Pract. 2001, 7, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Chiesa, M.; Hobbs, S. Making sense of social research: How useful is the Hawthorne effect? Eur. J. Soc. Psychol. 2008, 38, 67–74. [Google Scholar] [CrossRef]
- Tomopoulos, S.; Tomopoulos, S.; Dreyer, B.; Berkule, S.; Fierman, A.; Brockmeyer, C.; Mendelsohn, A. Infant Media Exposure and Toddler Development. Arch. Pediatr. Adolesc. Med. 2010, 164, 1105–1111. [Google Scholar] [CrossRef] [PubMed]
- Pagani, L.S.; Fitzpatrick, C.; Barnett, T.A.; Dubow, E. Prospective associations between early childhood television exposure and academic, psychosocial, and physical well-being by middle childhood. Arch. Pediatr. Adolesc. Med. 2010, 164, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, F.J.; Christakis, D.A. Children’s television viewing and cognitive outcomes—A longitudinal analysis of national data. Arch. Pediatr. Adolesc. Med. 2005, 159, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Reich, S.M.; Yau, J.C.; Warschauer, M. Tablet-based eBooks for young children: What does the research say? J. Dev. Behav. Pediatr. 2016, 37, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Carabin, H.; Gyorkos, T.W.; Soto, J.C.; Joseph, L.; Payment, P.; Collet, J.P. Effectiveness of a training program in reducing infections in toddlers attending day care centers. Epidemiology 1999, 10, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Ball, T.M.; Castro-Rodriguez, J.A.; Griffith, K.A.; Holberg, C.J.; Martinez, F.D.; Wright, A.L. Siblings, daycare attendance and the risk of asthma and wheezing during childhood. N. Engl. J. Med. 2000, 343, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Huskins, W.C. Transmission and control of infections in out-of-home child care. Pediatr. Infect. Dis. J. 2000, 19, S106–S110. [Google Scholar] [CrossRef] [PubMed]
- Hagerhed-Engman, L.; Bornehag, C.-G.; Sundell, J.; Sundell, J.; Aberg, N. Day-care attendance and increased risk for respiratory and allergic symptoms in preschool age. Allergy 2006, 61, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. (Eds.) Chapter 8. In Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration: Hoboken, NJ, USA, 2018. [Google Scholar]



{kind=link}
{kind=link}
| Macronutrients | Unit | Control Product (Skimmed Milk Powder) | Fortified Milk Powder |
|---|---|---|---|
| Energy | kcal/100 g | 467.8 | 477.7 |
| kcal/serving | 168.4 | 172 | |
| Fat | g/100 g | 17.8 | 21.4 |
| g/serving | 6.4 | 7.7 | |
| Alpha-linolenic acid | mg/100 g | 60.9 | 556.6 |
| mg/serving | 28.1 | 200.4 | |
| Protein | g/100 g | 14.8 | 16.3 |
| g/serving | 5.3 | 5.9 | |
| Fortification | mg/100 g | none | Zinc (8), Iron (11.4), Magnesium (141.7), Thiamin (1.05), Niacin (11), Pyridoxine (1.77), Biotin (0.0177), Vitamin C (97.3), and Alpha-linolenic acid (ALA, 556.6) |
| Baseline Measure | Experimental Group (n = 95) | Control Group (n = 97) |
|---|---|---|
| Age (years) | 3.90 ± 0.57 | 3.93 ± 0.57 |
| Sex (f/m) | 45/60 | 45/52 |
| HOME Inventory (score) | 21.14 ± 3.34 | 21.15 ± 3.25 |
| WPPSI (full-scale IQ score) | 81.64 ± 9.937 | 80.51 ± 10.294 |
| Ages and Stages (above/within normal) | 93/2 | 92/5 |
| Treatment Group | Control Group | |||||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | |||||
| V0 | V3 | V0 | V3 | V0 | V3 | Vo | V3 | |
| Height (cm) | 99.05 ± 6.332 | 102.11 ± 6.429 | 99.54 ± 5.733 | 103.32 ± 5.593 | 100.05 ± 5.151 | 103.67 ± 5.203 | 98.30 ± 5.572 | 101.56 ± 5.400 |
| Weight (kg) | 14.84 ± 2.212 | 15.83 ± 2.797 | 14.92 ± 2.664 | 16.48 ± 2.969 | 15.35 ± 2.047 | 16.39 ± 2.406 | 14.21 ± 2.034 | 15.49 ± 2.231 |
| Experimental Group | Control Group | |||
|---|---|---|---|---|
| V0 | V3 | V0 | V3 | |
| Hydroxyproline (ug/uL) | 0.1629 ± 0.09821 | 0.6146 ± 0.29840 | 0.1572 ± 0.07314 | 0.6446 ± 0.31704 |
| Creatinine (mg/dL) | 87.49 ± 53.575 | 98.29 ± 46.407 | 86.34 ± 46.975 | 99.30 ± 50.867 |
| Hydroxyproline Index: Hydroxyproline/creatinine (nmol/mg) | 1.48 | 5.0 | 1.51 | 5.2 |
| Experimental Group | Control Group | p-Value (Diff. between Groups) | ||
|---|---|---|---|---|
| V0 to V1 | 32.9 | - | - |
| V1 to V2 | 34.8 | - | - | |
| V2 to V3 | 29.9 | - | - | |
| V0 to V1 | 1.26 (0.09) | - | - |
| V1 to V2 | 1.08 (0.07) | - | - | |
| V2 to V3 | 1.43 (1.11) | - | - | |
| V0 to V1 | 2.26 (0.16) | 2.89 (0.21) | p < 0.05 * |
| V1 to V2 | 1.95 (0.28) | 2.56 (0.21) | p = 0.08 | |
| V2 to V3 | 1.54 (0.13) | 2.19 (0.21) | p < 0.05 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schneider, N.; Geiser, E.; Gosoniu, L.M.; Wibowo, Y.; Gentile-Rapinett, G.; Tedjasaputra, M.S.; Sastroasmoro, S. A Combined Dietary and Cognitive Intervention in 3–5-Year-Old Children in Indonesia: A Randomized Controlled Trial. Nutrients 2018, 10, 1394. https://doi.org/10.3390/nu10101394
Schneider N, Geiser E, Gosoniu LM, Wibowo Y, Gentile-Rapinett G, Tedjasaputra MS, Sastroasmoro S. A Combined Dietary and Cognitive Intervention in 3–5-Year-Old Children in Indonesia: A Randomized Controlled Trial. Nutrients. 2018; 10(10):1394. https://doi.org/10.3390/nu10101394
Chicago/Turabian StyleSchneider, Nora, Eveline Geiser, Laura M. Gosoniu, Yulianti Wibowo, Gertrude Gentile-Rapinett, Mayke S. Tedjasaputra, and Sudigdo Sastroasmoro. 2018. "A Combined Dietary and Cognitive Intervention in 3–5-Year-Old Children in Indonesia: A Randomized Controlled Trial" Nutrients 10, no. 10: 1394. https://doi.org/10.3390/nu10101394