Empowering Patients to Co-Create a Sustainable Healthcare Value

Department of Economics and Law, University of Cassino and Southern Lazio, 03043 Cassino, Italy
*
Author to whom correspondence should be addressed.
Sustainability 2019, 11(5), 1315; https://doi.org/10.3390/su11051315
Submission received: 31 December 2018
/
Revised: 21 February 2019
/
Accepted: 23 February 2019
/
Published: 2 March 2019
(This article belongs to the Special Issue Sustainability for Healthcare)
Abstract
:Extensive literature suggests that a solution to the current problems of healthcare sustainability is the active involvement of patients in health management through the empowerment of their abilities. Latest marketing frameworks suggest that patients are important resources for co-creating health value together with operators. This research aims to analyze the effects of patient empowerment on patients’ value co-creation behaviors. An empirical survey was conducted on 250 patients with chronic diseases in Italy. The results, analyzed using the structural equation modeling, showed that their empowerment enhanced value co-creation behaviors. Patients apply their health competencies and resources in their co-creation of health service with operators. It is, therefore, important to empower patients in their transformation from passive to active stakeholders, working with providers for the most optimal health outcomes. This research provides practitioners with suggestions for patient involvement which utilizes their knowledge, capabilities and responsibility to improving healthcare services.
1. Introduction
Healthcare sustainability refers to the capacity of healthcare systems to ensure the long-term health and well-being of communities [1]. It is threatened, in several countries, by factors such as aging populations [2], increases in multiple-chronic diseases [3], scarcity of financial resources [4] and an increasing distrust and dissatisfaction by citizens. These challenges require the allocation of enormous financial resources to the prevention, assistance, care, research and technologies that are necessary to ensure the continued health of the population. However, after the economic and financial crisis of 2008, many countries—especially within the European community—have been affected by austerity policies and public spending cuts, shifting the focus from the ethical-value dimension [5] and humanization of the service [1] to the rationalization of resources and technical/economic performance [1,6]. In view of these problems, new strategic and organizational guidelines are required to ensure the sustainability of healthcare.
Whereas, in the past, scholars and professionals have focused on healthcare organizations’ improvements in effectiveness and efficiency [7,8,9,10,11], in recent years the importance of the patient’s active role as a fundamental resource for healthcare sustainability has been re-evaluated [12,13,14].
The World Health Organization’s (WHO) program “Health 2020” [3] sets patient empowerment as the main goal for achieving better results in healthcare. Patient empowerment can be defined as the patient’s health education, responsibility and active participation in managing healthcare [15,16,17,18]. Several authors agree that the empowerment of patients is a necessary prerequisite for achieving important goals towards healthcare sustainability, including cost reduction, better health outcomes, fewer resources wasted, more prevention, improved service quality and patient satisfaction [19,20,21,22,23,24,25]. These authors explain empowerment as a set of competencies in patients which improve their health literacy [18,21,26], control [27,28,29], participation [15,26,27] and communications capacities [15,26,29]. However, this level of analysis does not reveal how such competencies determine behaviors aimed at improving healthcare value. This research thus applies the paradigm of value co-creation which has been introduced by recent service marketing theories (service-dominant logic [30,31]; service logic [32,33]; service science [34,35,36]) to explain how customers participate with providers in service delivery through the integration of resources and the utilization of competencies to improve the value created [30,37]. By introducing the concepts of co-creation and resource integration, service research supports a key requirement in sustainable development, which is the multi-stakeholder engagement and participatory process [38]. According to a value co-creation view, organizations create value not only for themselves but also for all the actors involved in the process and for the whole ecosystem in which they operate, thus sustaining social development and sustainability [39]. Compared with theories on patient empowerment, those on value co-creation focus on the service delivery process and on customers’ behaviors rather than just on their competencies [40]. Yi and Gong [40] identify two categories of co-creative behaviors: (1) participation behaviors, which include, among others, the search for information, information-exchange, responsible actions and positive attitude during personal interactions; (2) citizenship behaviors, which include, among others, the provision of feedback, service promotion to other people, helping other customers and tolerance towards service failures.
Patients have developed in recent years from subjects who passively received instructions and treatment from professionals to subjects who actively gather information and manage their own state of health [41,42]. They may thus be considered as customers [43,44] and the basic axioms of value co-creation theories can be applied to them [44,45,46,47]. Hence, patients can be considered as active individuals who participate in the creation of “health” value by sharing their information, competencies and resources with health professionals [43,48,49,50]. A sustainable health value can be created when the needs and objectives of organizations and patients fit thanks to a deeper understanding of patients and their participation in the value creation process [51].
Integrating theories of patient empowerment with those of value co-creation allows an analysis of patient’s contributions to health sustainability on a higher level, one that includes both the competencies of patients—expressed by their empowerment—and their co-creation behaviors. However, the links between these constructs need to be investigated. The aim of this work is to analyze, first theoretically and then empirically, how the empowerment of patients influences their value co-creation behaviors, thus answering the following research questions:
RQ1: What are the characteristics of patients that determine their co-creation behaviors to health value, together with the operators?
RQ2: Is it possible to stimulate patient participation in the co-creation of better health value by increasing their level of empowerment?
Through a literature revision, this paper highlights how the health service can be improved becoming more sustainable by transforming the competencies of patients in participation behaviors of health value co-creation. Based on the literature, a theoretical model was constructed to investigate the links between the patients’ competencies and their participatory behaviors. The constructs analyzed are those of patient empowerment and value co-creation and have been operationalized on the basis of models validated in the literature. The investigation was carried out by administering the questionnaire to 250 patients with chronic diseases and data have been analyzed using structural equation modeling. The results are discussed and conclusions, theoretical and practical implications are provided.
2. Literature Review
2.1. Patient Empowerment and Healthcare Sustainability
Patient empowerment is a concept studied by different scientific disciplines from medicine to public administration, from marketing to human sciences. This has not allowed the emergence of a univocal, common definition. Despite the confusion about this concept’s meaning, it can be generally defined as a social process of recognition, promotion and improvement of patients’ abilities to meet their needs, solve their problems and feel in control of their lives [19,20,26,52,53].
Regardless of any definition of patient empowerment adopted, the different authors agree by recognizing it as a multidimensional construct. Some authors focus on patient characteristics such as self-management [19,54], self-efficacy [20,26], self-care [15] and control over the health status [16,41,52]. Others focus on the relationships between patients and healthcare professionals in terms of the communicative process [26,29], a model of partnership [17,55], collaboration [54,56] patient-centered care [57], and egalitarian and equitable relationships [41].
All these dimensions can be traced back to the four main dimensions of patient empowerment described by the SUSTAINS project of the European community [58]:
- -
- -
- -
- -
- Communication with healthcare professionals: patients’ ability to effectively and efficiently communicate with healthcare professionals [15,26,29]. This is a reciprocal process where patients must be able to make detailed explanations of their symptoms, express considerations and preferences, and ask for more information; clinicians must encourage dialogue, mutual listening and comprehension.
With regard to health literacy, it is necessary to specify that there are different views in the literature about the links between health literacy and patient empowerment. Some authors sustain that the two concepts are distinct but closely interwoven [61,62,63] and that health literacy does not automatically lead to empowerment [64]. However, we agree with the SUSTAIN project in including health literacy as a dimension of patient empowerment and with a consistent part of the literature claiming that patient empowerment begins with knowledge [65] and health literacy is critical to the empowerment of patients [66,67,68,69,70,71,72,73,74] showing in some cases a direct relationship between the two concepts [22,75,76]. Moreover, some authors highlight that low health literacy creates difficulties in interacting with the healthcare professionals and understanding health information available [77,78,79,80], thus discouraging the patients’ participation in the delivery of health services [81,82] and in decision-making [83].
Healthcare sustainability can be defined as the capacity of the health system to constantly maintain or improve the health of the population as a whole and of each individual by adapting itself to economic, socio-demographic changes [1]. The sustainability of the health systems faces two risks: economic sustainability, or the system’s capacity to find necessary financial resources; and social sustainability, or the system’s capacity to guarantee accessible and adequate care for all citizens and satisfy their needs. Saviano et al. [84] highlight an increasing risk of dissonance in the relationship provider-patients because the current governance model in healthcare is focused primarily on the relationships provider-authorities while often neglecting the human, emotional and ethical aspects of the relationship with patients. In a general context of scarce resources and a growing demand for healthcare, the goal of sustainability should not be based on political or ideological solutions but rather on the ethical ones. These critical issues stimulate governments and organizations to locate new organizational and management models to enable their health systems to remain sustainable. WHO’s program “Health 2020” [3] thus nominates patient empowerment as the main objective for improving health outcomes. According to WHO, patient empowerment could help solve some of the most demanding problems in modern healthcare, improve the quality of healthcare services [22] and reduce their costs [85], thus contributing to the sustainability of healthcare systems [23]. The contributions of patient empowerment to better healthcare sustainability and value are described in Table 1 [18,19,20,21,22,23,24,25,86,87].
2.2. Value Co-Creation and Patient Empowerment
During the last decade, several works in the marketing literature have highlighted the complexity and importance of patients’ involvement as "operating" resources in value-creation [43,44,45,46,47,48,49,50]. These contributions arise from two principal scientific frameworks: Service-Dominant logic [32,33] and Service Science [34,35,36].
According to Service-Dominant logic, patients have fundamental resources for value creation [88]—such as information. Professionals, in turn, are responsible for effectively educating and managing patients [48], collecting and analyzing patients’ necessary information [45], listening to patients’ opinions about their satisfaction with the service and interpreting this feedback [13]. Such moments of interaction enhance the experiential value perceived by the patient [32] and his/her assessment of satisfaction [89].
According to Service Science, the evolution of information and communication technologies—with the emergence of health platforms and online communities—provided new sources of information to patients and new modes of interaction, which allowed delivering service continuously [46]. New technologies add the type of value that traditional healthcare systems, based on occasional encounters between practitioners and patients, could not [49]; thus stimulating value co-creation paths [46,49,90,91]. The value co-creation process can enable more agile and integrated healthcare delivery with better outcomes and less error, focusing on preventative intervention, and facilitating increased agency and responsibility in patients [34,42]. In this new vision, the customer must share the responsibility of achieving the sustainability objective together with all the other entities involved in the system [84]. It is, therefore, becoming increasingly necessary for health organizations and policymakers to understand how individuals can be involved in value co-creation to better manage their healthcare experience [50]. The literature indicates that individuals can participate in the creation of healthcare through different behaviors, mental attitudes and models of co-creation [45,50,92,93].
This research considers the value co-creation behaviors described by Yi and Gong [40], as they have been operationalized:
Participation behavior: it includes several in-role behaviors that are necessary for the success of value co-creation such as the search for information, information-exchange, responsible actions and positive attitude during personal interactions [40];
Citizenship behavior: it includes voluntary extra-role behaviors that are not necessary for value co-creation but provide an unexpected value to the organization [40] such as the provision of feedback, service promotion to other people, helping other customers and tolerance towards service failures [94,95,96,97].
Service-Dominant logic defines value co-creation as the “…integration of resources and application of competencies during the interactions among providers and customers” [35]; thus, in order to co-create value with health professionals, patients must be able to integrate their resources in this process and bring their own competencies to these interactions. The more the resources and competencies of patients, the more they can contribute to creating value.
Patient empowerment can be defined as how people gain the information and abilities to actively partner with healthcare professionals to decide and choose their own treatment and care [55,98] and identify and apply the resources that can give them a sense of control over own lives [17]. Patient empowerment can equip patients with the resources and competencies required to co-create value with healthcare professionals. Therefore, empowerment concerns a set of competencies and resources that the patient can apply and exchange with service providers during interactions to co-create value [35]. We can thus hypothesize that patient empowerment enables the value co-creation behaviors.
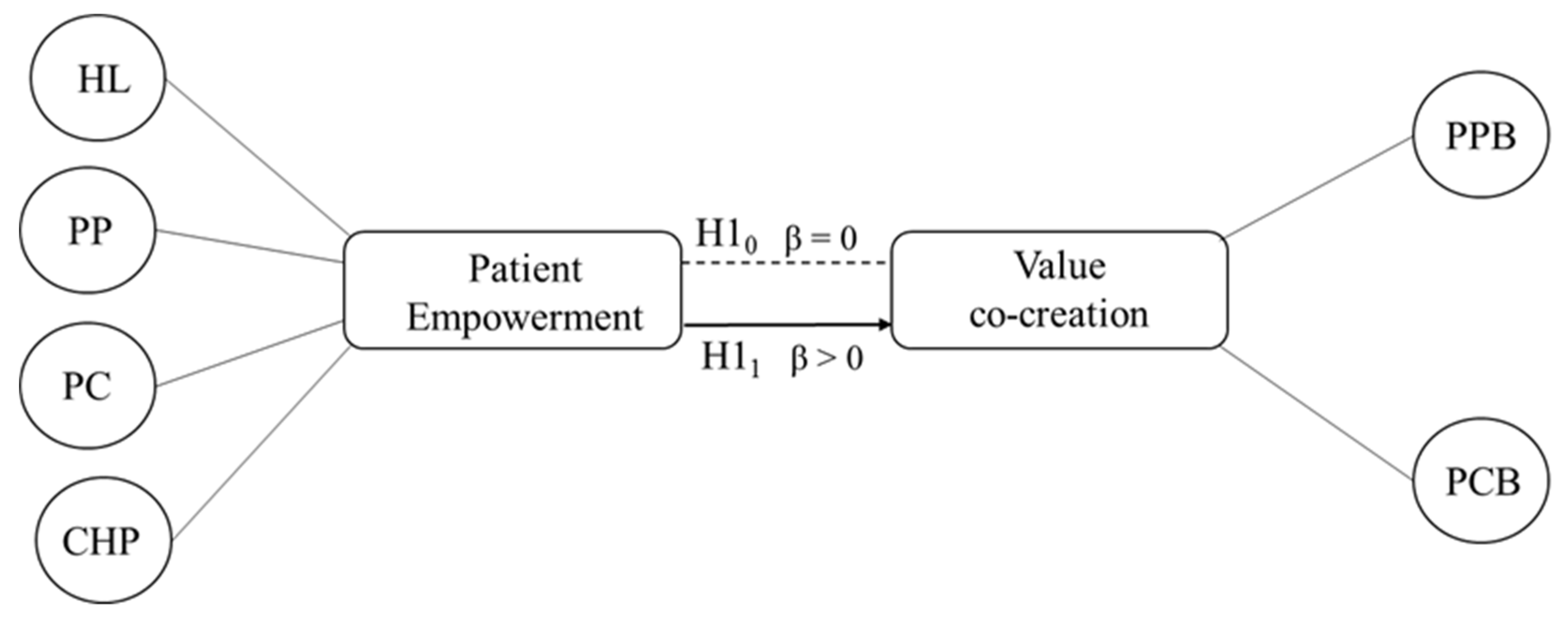
Based on these considerations, we formulated the following research hypotheses using the hypotheses test H0: β = 0 null hypothesis, H1: β > 0 alternative hypothesis:
H10: The level of patient empowerment does not affect (β = 0) the patient’s value co-creation behaviors.
H11: The level of patient empowerment positively affects (β > 0) the patient’s value co-creation behaviors.
3. Materials and Method
An empirical investigation was conducted to test the research hypotheses. The research model is composed of two second order-constructs (Figure 1). The patient empowerment construct is explained by the dimensions health literacy (HL), patient participation (PP), patient control (PC), communication with healthcare professionals (CHP); the value co-creation construct is explained by the dimensions patient participation behavior (PPB), patient citizenship behavior (PCB).
A cross-sectional research design was applied to test the correlations between patient empowerment and value co-creation. The four dimensions recognized by the European community [57] were considered for the operationalization of the patient empowerment construct (see Section 2.1). The literature does not provide a common definition of empowerment and its dimensions [20] thus leading to the proliferation of different measurement models [99,100]. We constructed the patient empowerment scale on the basis of two recent literature reviews [99,100] which, in addition to identifying the existing empowerment scales, also evaluate their validity. From these reviews, 35 measurement scales of patient empowerment were identified. By eliminating models for measuring the empowerment of pediatric patients or patients with psychological or very specific conditions, 14 measurement models were selected for generic patients or patients with chronic diseases. These models were examined and those including the dimensions of empowerment considered in this study [57] were selected to derive the items for each dimension. In particular, the items for measuring health literacy were selected from the model [72], those for the patient participation from references [26,60], for patient control from [20,21] and for the communication with health professionals from [25]. The items selected were translated into Italian and adapted in the form with the help of a physician. After collecting data, a principal component analysis was conducted and only the items with a factor loading higher than 0.6 were retained for subsequent analyses [101].
Several studies in the marketing literature have highlighted problems in measuring value co-creation [50,53,102,103,104,105]. Only three relevant empirical studies about value co-creation have yet been detected [50,53,102]. We chose the model of Yi and Gong [40] for this research because it is the only one in which validity has been tested. This model measures value co-creation through its two dimensions of customer participation behavior and customer citizenship behavior. The items were adapted to the healthcare context with the help of a physician and those presenting a high factor loading in the model were used for the analyses.
The final model is shown in Table 2.
All items were measured on five-point Likert scales where 1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, and 5 = strongly agree.
Sample
The questionnaire was administered in the waiting rooms of the local health units of the Lazio region, during the period from July 2017 to March 2018, to 340 patients with chronic diseases. This category of patients was chosen because, according to the European patients forum [106], chronic diseases represent the major sustainability challenge for politicians and policymakers who represent European health systems which are unable to cope well with chronic conditions because they do not meet patients’ needs. The convenience sampling method was used to select the sample. Although it is a non-probability sampling method, it is the most applicable and widely used method in clinical research and healthcare setting [107,108] as it allows selecting the sample elements according to their convenient accessibility and proximity [109]. To reduce bias, the questionnaire was administered directly by the health operators in the absence of the researchers and the validity and reliability were assessed to estimate the size of the error in the sample and calculating the significance of findings [110]. At the beginning of the questionnaire, a privacy note was reported informing respondents that the questionnaire was completely anonymous and the data would be treated in an aggregate form exclusively for statistical purposes and in compliance with the Italian law on privacy (D.Lgs. n. 196/2003). 250 valid questionnaires were collected with a response rate of 73.5%, satisfying the sample size of 200 cases suggested for the application of the structural equation modeling [111]. The characteristics of the sample are described in Table 3.
Data were analyzed through covariance-based structural equation modelling [112].
4. Results
A set of fit indices were used to evaluate the model fit as recommended by Chin et al. [113] and Hooper et al. [114]. The measurement model shows an overall acceptable fit [115] with χ2 = 1334.56, df = 601 (p < 0.01), and χ2/df = 2.22 satisfying the recommendations for a relative/normed chi-square range from as high as 5.0 [116] to as low as 2.0 [117].
According to Hair et al. [112] and Awang [118], CFI = 0.92 shows a satisfactory fit by in overcoming the cut-off criterion of CFI ≥ 0.90. A value greater than 0.90 ensures that wrongly specified models are not accepted [119].
According to Awang [118], RMSEA = 0.07 shows an acceptable fit, being below 0.08. The general consensus among scholars in this area is a cut-off value close to 0.06 [119] or a stringent upper limit of 0.07 [120]; however, some authors state that an RMSEA below 0.08 shows a good fit [114,121].
The composite reliability shows the measurement model reliability cause values ranged from 0.816 to 0.951, thus exceeding the recommended threshold of 0.6 [115].
All standardized factor loadings for each first-order and second-order construct varied from 0.697 to 0.98, exceeding the recommended threshold of 0.6 [113]. The square roots of AVEs for each latent construct was higher than the construct’s highest squared correlation with any other construct and over the 0.50 that would guarantee good discriminant validity [124]. Thus, reliability, convergent validity and discriminant validity were met [125].
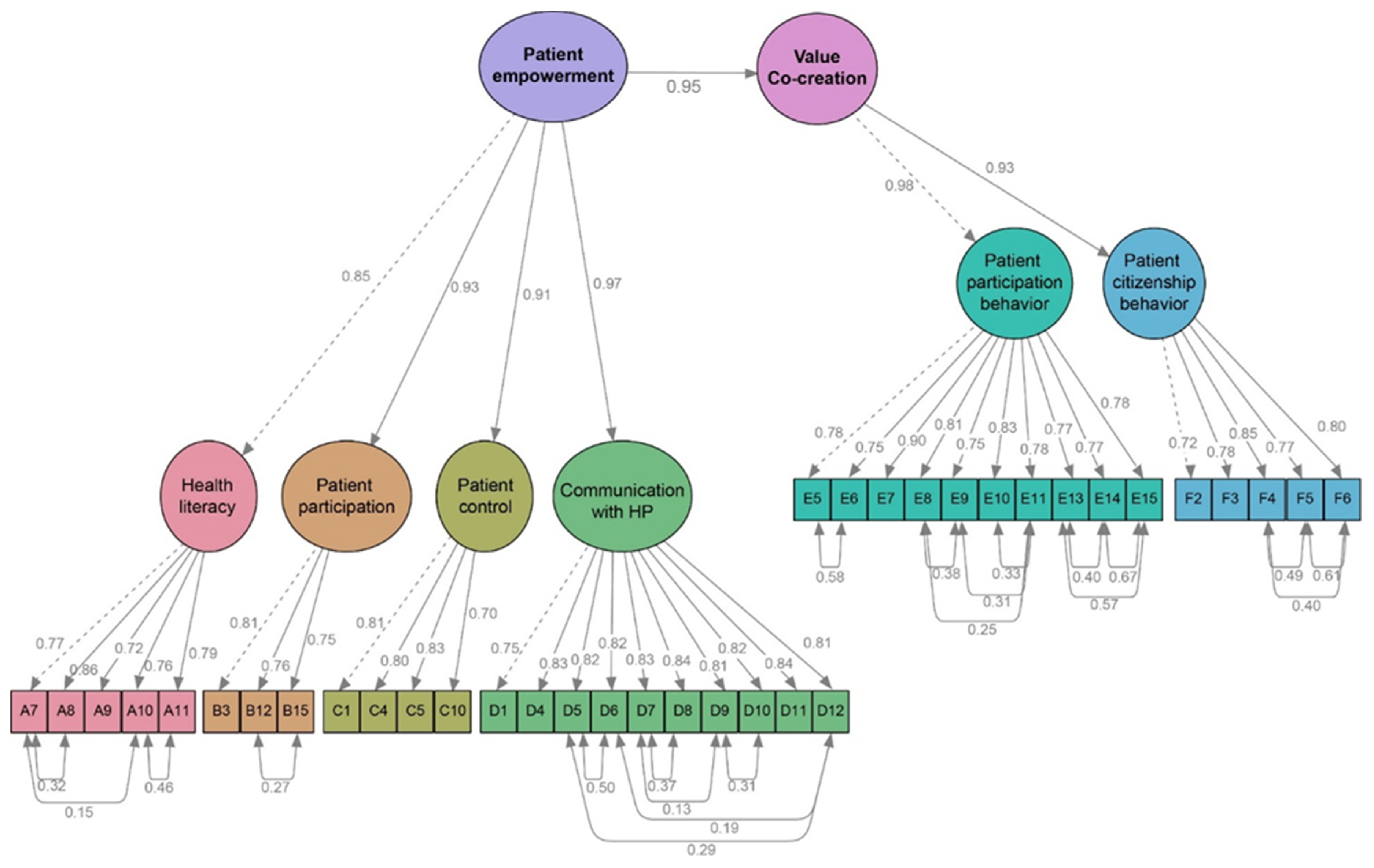
We arrived at the structural model after ensuring the measurement model’s validity. The model was a good fit, according to the results (Table 6 and Figure 2).
Table 6 shows the validity of the structural model: χ2 was 1334.56 with df = 601, χ2/df had a value of 2.22 and below the threshold of 3 [111], CFI was 0.921, greater than the cutoff of 0.92 [115]. In addition, the RMSEA was 0.069 and SRMR was 0.04, thereby lower than the threshold of 0.07 [115].
Figure 2 illustrates the results of the structural model. Latent variables are drawn as ovals and manifest or measured variables (items) are shown as squares. The straight line pointing from a latent variable to the observed variables indicates the causal effect of the latent variable on the observed variables. The figure provides numerical estimates for each of the parameters (arrows) in the model and indicates that all the observed variables are good indicators of the latent variables with high covariation that ranges from 0.70 to 0.90. The curved arrows at the bottom are the measurement errors (unreliability) in the items. Moreover, results show that all the dimensions are correlated with high values, which range from 0.85 to 0.98, to the second order constructs (Patient empowerment and Value co-creation). Finally, the arrow between patient empowerment and value co-creation indicates a direct and positive relationship between the two latent variables with a standard regression estimate (β = 0.95, p < 0.01) that detect a strong and positive effect of one construct over the other. These results validate H11, showing that patient empowerment directly and positively affects value co-creation behaviors.
5. Discussion
The results of this research offer interesting opportunities for understanding of the role of patients in improving health value by integrating two actual and debated theories in the healthcare management and service marketing fields: patient empowerment and value co-creation.
In line with the relevant literature on patient empowerment, this analysis shows that it can be explained by the four dimensions of health literacy, patient control, and participation and communication abilities [15,18,21,26,27,28,59,60]. However, while previous works were limited to measuring these dimensions in patients with different conditions [26,40,60,80,94,126], this research adds value by showing some possible consequences of patient empowerment in terms of value co-creation behaviors. The consequences of empowerment had previously been investigated mainly in terms of improving health and well-being [86,87,127,128] and in terms of patient satisfaction [129,130,131], which can be considered a measure of service quality in healthcare [132,133]. According to the results of this research, patient empowerment should positively influence co-creation behaviors because from the analysis it emerges that the dimensions of empowerment have direct and positive effects on the patient’s predisposition to implement behaviors of participation in health management and citizenship behaviors with health organizations. For example, if we take diabetic patients into consideration, their empowerment is reflected in a greater knowledge of the pathology, symptoms, and treatment alternatives; a greater participation with physicians in making decisions about the most appropriate diet or treatment according to the patient’s lifestyle and preferences; a greater capacity to control the pathology that would allow patients to manage it autonomously, for example by learning how to check insulin levels in the blood and to calibrate and administer the amount of insulin needed from time to time; an increased ability to communicate efficiently and effectively with doctors to describe all the relevant factors that allow evaluating the evolution of the disease. The results of this study suggest that these empowered diabetic patients should be more likely to activate co-creative behaviors like information seeking and sharing, responsible behaviors towards health providers, positive personal interactions, feedback, advocacy, tolerance for service failures and helping other patients.
The application of value co-creation theories to the study of patient empowerment allows a focus on the patient as an operant resource in the value-creating process [30]. The focus is shifted from the service provider to the patient because, as stated by Service-Dominant logic, the service provider “…cannot deliver value, but only offer value propositions” and “…value is always uniquely and phenomenologically determined by the beneficiary” [31]. Consequently, the value co-creation view also changes the analysis from output to outcome.
The results of this study offer interesting suggestions for theories of value co-creation about creating the necessary conditions for activating the path of co-creation between patients and providers. According to Berry and Bendapudi [13], understating how to stimulate participation in value creation is a critical issue in the health field: patients are often unwilling to do so, although the health policies of west countries increasingly promote the active participation of the patients in health services. They do this both for the effects that patient participation has on health outcomes (especially for chronic disease) and on cost savings.
The literature on the value co-creation makes several attempts to identify the drivers of co-creation [50,53,105]. The main problems seem to be related to the understanding of the dimensions behind customers’ co-creation behaviors [102,103,126]. This conceptual ambiguity is also reflected in the terminology used to describe the facets of customers’ co-creation. Terms such as “involvement”, “engagement” and “self-engagement” are often used, sometimes synonymously, although they express different levels of commitment and intensity of interaction by customers, as well as different roles in actual interactions [37,94]. “Involvement” is generally used to emphasize the proactive role of providers in facilitating and promoting the active participation of clients [130,134,135,136,137,138,139,140,141,142,143,144]; the service provider takes the initiative and the customer’s role requires less effort/intensity. “Engagement” is often used to indicate the active, equal and reciprocal participation of the customer and the supplier in the value co-creation [104,137,138,139]; both the customer and the supplier, with equal effort or intensity, initiate participation. ”Self-engagement” is generally used when individuals feel a sense of responsibility and commitment to certain services that they consider important [140]; the initiative to participate is taken directly by the customer, compared to other forms of participation, there is a greater intensity of commitment from the customer compared to the provider. ”Empowerment”, on the other hand, encompasses all these concepts. Demonstrating a positive correlation between empowerment and co-creation helps to define the consumer’s dimensions necessary for co-creation. According to this research, the dimensions that explain the customers’ co-creation behaviors in the healthcare context can be identified in health literacy, the capacity to control health status, ability to make decisions about health with professionals and actively participate in its management, and the capacity to effectively communicate with operators.
The explanation of value co-creation through the dimensions of the patient empowerment also provides a better understanding of the problem of information asymmetry in the patient-professional relationship. Several studies state that the information asymmetry in healthcare creates an unequal power relationship between experts and patients [141,142], which does not allow the exploitation of the value co-creation opportunities [143]. Patient empowerment, particularly through its dimension of health literacy, reduces the information gap of patients thus enabling their involvement in value co-creation.
6. Conclusions, Practical and Theoretical Implications
Due to the economic crisis of 2008 and the increased need for care and assistance in the population, health systems in many countries currently see their sustainability compromised, especially from economic and social points of view. The empowerment of patients has been identified as a possible way of improving several aspects of healthcare management. This study contributes by integrating value co-creation theories with the study of patient empowerment, showing that, by empowering patients, it is possible to activate value co-creation paths between them and health providers. Value co-creation is recognized in marketing as a process of interaction and exchange between customers and providers able to create higher value.
On a theoretical level, this paper offers a contribution to addressing the challenge of sustainability by integrating different perspectives and research areas. The links between patient empowerment and value co-creation highlight the role of “people, technology and governance for sustainability” which represent the pillars of sustainable development according to the systems perspective [144]. People possess fundamental resources for the sustainability of healthcare systems such as information, knowledge and competencies. These resources must be applied and shared during the interactions with professionals in order to create a sustainable health value. Technology provides the right tools and environments to support this process. Governments are responsible for educating both patients and professionals to a logic of mutual and sustainable benefit and investing time and capital in the introduction of stronger mechanisms of integration. The literature on healthcare sustainability at first focused on the effectiveness and efficiency of health organizations and then moved the focus on the resources and competencies of patients in conjunction with the development of theories on patient empowerment. This work supports previous studies [5,37,143,144] aimed at shifting the focus on the relational approach as a possible way to activate the principles of value co-creation in order to consider both patients and professionals and the relationships between them as fundamental elements for sustainability in healthcare, according to a win-win logic [145].
From a managerial point of view, this implies that policies aimed at sustainability must not only consider the performance of organizations but also the role of patients and better management of the interactions with them. Governments and health organizations are responsible for considering patients as operant resources, to be involved in health management for better results. According to this study, two main actions should be implemented to improve health outcomes: policies aimed at increasing citizen empowerment, and the creation of fertile contexts for value co-creation between patients and practitioners. These objectives could be achieved by providing citizens’ education and training programs, making information and educational material accessible, educating health professionals to greater sharing and dialogue with patients, improving the digitalization of health to allow citizens to access some services autonomously, and exploiting social media through the creation of health communities where patients can share information, opinions and experiences with other patients and professionals. Service Science suggests that these processes could be supported by the latest technology platforms and ICT solutions. This would represent an important vehicle for value co-creation, facilitating interaction and information sharing between the various stakeholders [36]. For example, e-health introduced several tools and services that use ICTs to improve prevention, diagnosis, treatment, monitoring and management of health and lifestyle. Among these tools we find the electronic health record allows patients to manage their health information; e-reservation and e-prescription platforms that allow patients to independently manage appointments, medical prescriptions and get medical reports; mobile applications for the self-monitoring of various physiological parameters; telemedicine techniques that allow the treatment of a patient, or more generally to provide health services, at a distance; online communities where patients can gather useful information, share their experience, communicate with other patients or professionals. In particular, the latter has spread a lot in recent years. For example, MyHealthTeams reached 1.75 million members from 13 countries, and Carenity more than 600.000 members in the European area. These communities represent virtual places able to foster patients’ co-creative behaviors because patients accept the usage of their data and of their conversations for research and medical aims and often participate actively in investigations related to their pathology. In Carenity, more than 500.000 people co-operated with professionals to the scientific research by answering questionnaires.
7. Research Limitations and Future Research
The principal limitation of this paper concerns the method used to measure the patient empowerment construct. This limitation derives by the great uncertainty in the literature about the best way to define and measure it [20,26,99,146]. From the review of Barr et al. [99], it emerges that the available measures of patient empowerment have been developed independently, with scale content informed by different theoretical frameworks and no clear consensus about what patient empowerment comprises. Each existing measure captures a different conceptualization leading to distinct constructs. Moreover, a number of patient empowerment measures are condition or specialty-specific making their generalization or application in different contexts difficult. These measures also present several problems in their methodological quality assessed in terms of reproducibility, responsiveness, internal consistency, content and construct validity. For example, reliability was assessed only in a few studies, either resulting in poor or fair ratings, and measurement error was not reported in any study. For these reasons, we were not able to identify a specific model to use in our work, but we had to select the items appropriate to measure the dimensions of the empowerment that we considered of interest for our research from different models. This methodological approach, in addition to the convenience sampling method used, certainly exposes the research to different critical issues as the researchers’ bias and limited replicability of the research design. However, these limitations are very frequent in empirical works about patient empowerment where only a few studies used randomized sampling [147,148], while the most common sampling method is convenience sampling [16,53,69,146,147,148,149,150,151] and some studies did not report the sampling method at all [53,80,152,153,154]. Moreover, the psychometric property reproducibility is generally not assessed [99]. Further research about the operationalization of patient empowerment is thus required.
Another limitation concerns the model used to measure value co-creation. As explained above, there are not many empirical studies in this area; thus, the only model for which validity has been demonstrated in the literature was chosen. The results of the survey show satisfactory values of the psychometric properties of this scale, which can be applied to the health context. However, originally this model was created to detect the behaviors of the employees within organizations and then was adapted by Yi and Gong [40] for consumers’ behaviors. Although it represents an interesting first attempt to measure the co-creation of value, it does not fully represent the construct as defined by the service research. We believe that the work of McColl Kennedy et al. [50], which identifies the mental behaviors and attitudes of patients in the processes of value co-creation and uses S-D logic as a scientific basis, should be more interesting for measuring value co-creation. However, the internal composition by sub-dimensions has not yet been studied, despite the intention expressed by the authors to provide it in future research; this has not allowed the operationalization of the theoretical construct. Future research could elaborate on a model based on this study and test it. It would also be interesting for future research to reverse the analysis and investigate how participation in the value co-creation processes affects patient empowerment.
Author Contributions
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Aquino, R.P.; Barile, S.; Grasso, A.; Saviano, M. Envisioning smart and sustainable healthcare: 3D Printing technologies for personalized medication. Futures 2018, 103, 35–50. [Google Scholar] [CrossRef]
- ISTAT. Rapporto Annuale 2018—La Situazione del Paese. 2018. Available online: https://www.istat.it/it/archivio/214230 (accessed on 25 September 2018).
- World Health Organization, Regional Office for Europe. Health 2020 Policy Framework and Strategy Document; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- AGI. Tumori: Oncologi, in Italia Costano 19 mld l’Anno. 2018. Available online: http://www.regioni.it/sanita/2018/06/01/tumori-oncologi-in-italia-costano-19-mld-lanno-564182/ (accessed on 1 October 2018).
- Barile, S. Introduzione. In Condizioni di Efficacia Relazionale e di Performance Nell’Azienda Sanitaria; Saviano, M., Ed.; Giappichelli: Torino, Italy, 2012. [Google Scholar]
- Saviano, M.; Bassano, C.; Piciocchi, P.; Di Nauta, P.; Lettieri, M. Monitoring Viability and Sustainability in Healthcare Organizations. Sustainability 2018, 10, 3548. [Google Scholar] [CrossRef]
- Zuckerman, S.; Hadley, J.; Iezzoni, L. Measuring Hospital Efficiency with Frontier Cost Functions. J. Health Econ. 1994, 13, 255–280. [Google Scholar] [CrossRef]
- Conrad, D.; Wickizer, T.; Maynard, C.; Klastorin, T.; Lessler, D.; Ross, A.; Soderstrom, N.; Sullivan, S.; Alexander, J.; Travis, K. Managing Care, Incentives, and Information: An Exploratory Look Inside the ‘Black Box’ of Hospital Efficiency. Health Serv. Res. 1996, 31, 235–259. [Google Scholar] [PubMed]
- Carman, J.M.; Shortell, S.M.; Foster, R.W.; Hughes, E.F.; Boerstler, H.; O’Brien, J.L.; O’Conner, E.J. Keys for successful implementation of total quality management in hospitals. Health Care Manag. Rev. 1996, 21, 48–60. [Google Scholar] [CrossRef]
- Bretthauer, K.M.; Côté, M.J. A model for planning resource requirements in health care organizations. Decis. Sci. 1998, 29, 243–270. [Google Scholar] [CrossRef]
- Arah, O.A.; Klazinga, N.S.; Delnoij, D.M.J.; Ten Asbroek, A.H.A.; Custers, T. Conceptual frameworks for health systems performance: A quest for effectiveness, quality, and improvement. Int. J. Qual. Health Care 2003, 15, 377–398. [Google Scholar] [CrossRef] [PubMed]
- Coulter, A.; Jenkinson, J. European patients’ views on the responsiveness of health systems and healthcare providers. Eur. J. Public Health 2005, 15, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Berry, L.L.; Bendapudi, N. Health care: A fertile field for service research. J. Serv. Res. 2007, 10, 111–122. [Google Scholar] [CrossRef]
- Akaka, M.A.; Vargo, S.L.; Lusch, R.F. The complexity of context: A service ecosystems approach for international marketing. J. Mark. Res. 2013, 21, 1–20. [Google Scholar] [CrossRef]
- Fotoukian, Z.; Shahboulaghi, F.M.; Khoshknab, M.F.; Mohammadi, E. Concept analysis of empowerment in old people with chronic diseases using a hybrid model. Asian Nurs. Res. 2014, 8, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; Funnell, M.M. Patient empowerment: Myths and misconceptions. Patient Educ. Couns. 2010, 79, 277–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodwell, C.M. An analysis of the concept of empowerment. J. Adv. Nurs. 1996, 23, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Ouschan, R.; Sweeney, J.C.; Johnson, L.W. Dimensions of patient empowerment: Implications for professional services marketing. Heal. Mark. Q. 2000, 18, 99–114. [Google Scholar] [CrossRef] [PubMed]
- Bann, C.M.; Sirois, F.M.; Walsh, E.G. Provider support in complementary and alternative medicine: Exploring the role of patient empowerment. J. Altern. Complement. Med. 2010, 16, 745–752. [Google Scholar] [CrossRef] [PubMed]
- McAllister, M.; Dunn, G.; Payne, K.; Davies, L.; Todd, C. Patient empowerment: The need to consider it as a measurable patient-reported outcome for chronic conditions. BMC Health Serv. Res. 2012, 12, 157. [Google Scholar] [CrossRef] [PubMed]
- Aujoulat, I.; Deccache, A.; Marcolongo, R.; Bonadiman, L. Reconsidering patient empowerment in chronic illness: A critique of models of self-efficacy and bodily control. Soc. Sci. Med. 2008, 66, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Moretta Tartaglione, A.; Cavacece, Y.; Cassia, F.; Russo, G. The excellence of patient-centered healthcare: Investigating the links between empowerment, cocreation and satisfaction. TQM J. 2018, 30, 153–167. [Google Scholar] [CrossRef]
- Polese, F.; Moretta Tartaglione, A.; Cavacece, Y. Patient empowerment for healthcare service quality improvements: A value co-creation view. In Proceedings of the 19th Toulon-Verona International Conference Excellence in Services, Huelva, Spain, 5–6 September 2016; pp. 385–397. [Google Scholar]
- Seiders, K.; Flynn, A.G.; Berry, L.L.; Haws, K.L. Motivating customers to adhere to expert advice in professional services a medical service context. J. Serv. Res. 2015, 18, 39–58. [Google Scholar] [CrossRef]
- Hibbard, J.H.; Stockard, J.; Mahoney, E.R.; Tusler, M. Development of the Patient Activation Measure (PAM): Conceptualizing and measuring activation in patients and consumers. Health Serv. Res. 2004, 39, 1005–1026. [Google Scholar] [CrossRef] [PubMed]
- Small, N.; Bower, P.; Chew-Graham, C.; Whalley, D.; Protheroe, J. Patient empowerment in long-term conditions: Development and preliminary testing of a new measure. BMC Heal. Serv. Res. 2013, 13, 263. [Google Scholar] [CrossRef] [PubMed]
- Salmon, P.; Hall, G.M. Patient empowerment or the emperor’s new clothes. J. R. Soc. Med. 2004, 97, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.J.; Lee, B. The Effect of computer-mediated social support in online communities on patient empowerment and doctor-patient communication. Health Commun. 2012, 27, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Aujoulat, I.; D’Hoore, W.; Deccache, A. Patient empowerment in theory and practice: Polysemy or cacophony? Patient Educ. Couns. 2007, 66, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Vargo, S.L.; Lusch, R.F. Evolving to a New Dominant Logic for Marketing. J. Mark. 2004, 68, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Vargo, S.L.; Lusch, R.F. Service-dominant logic: Continuing the evolution. J. Acad. Mark. Sci. 2008, 36, 1–10. [Google Scholar] [CrossRef]
- Grönroos, C. Service logic revisited: Who creates value? And who co-creates? Eur. Bus. Rev. 2008, 20, 298–314. [Google Scholar] [CrossRef]
- Grönroos, C. Service Management and Marketing. A Customer Relationship Management Approach; John Wiley: Chichester, UK, 2000. [Google Scholar]
- Maglio, P.; Spohrer, J. Fundamentals of service science. J. Acad. Mark. Sci. 2008, 36, 18–20. [Google Scholar] [CrossRef]
- Vargo, S.L.; Maglio, P.P.; Akaka, M.A. On value and value co-creation: A service systems and service logic perspective. Eur. Manag. J. 2008, 26, 145–152. [Google Scholar] [CrossRef]
- Spohrer, J.; Maglio, P.P.; Bailey, J.; Gruhl, D. Steps toward a science of service systems. Computer 2007, 40, 71–77. [Google Scholar] [CrossRef]
- Vargo, S.L. Customer Integration and Value Creation: Paradigmatic Traps and Perspectives. J. Serv. Res. 2008, 11, 211–215. [Google Scholar] [CrossRef]
- Saviano, M.; Barile, S.; Spohrer, J.C.; Caputo, F. A service research contribution to the global challenge of sustainability. J. Serv. Theory Pract. 2017, 27, 951–976. [Google Scholar] [CrossRef]
- Aquilani, B.; Silvestri, C.; Ruggieri, A. Sustainability, TQM and Value Co-Creation Processes: The Role of Critical Success Factors. Sustainability 2016, 8, 995. [Google Scholar] [CrossRef]
- Yi, Y.; Gong, T. Customer value co-creation behavior: Scale development and validation. J. Bus. Res. 2013, 66, 1279–1284. [Google Scholar] [CrossRef] [Green Version]
- McWilliam, C.L. Patients, persons or partners? Involving those with chronic disease in their care. Chronic Illn. 2009, 5, 277–292. [Google Scholar] [CrossRef] [PubMed]
- Carrubbo, L.; Bruni, R.; Cavacece, Y.; Moretta Tartaglione, A. Service System Platforms to Improve Value Co-Creation: Insights for Translational Medicine. In Service Dominant Logic, Network and Systems Theory and Service Science: Integrating Three Perspectives for a New Service Agenda; Gummesson, E., Mele, C., Polese, F., Eds.; Giannini Editore: Napoli, Italy, 2015. [Google Scholar]
- Nordgren, L. The performativity of the service management discourse: “Value creating customers” in health care”. J. Health Organ. Manag. 2008, 22, 510–528. [Google Scholar] [CrossRef] [PubMed]
- Shackley, P.; Ryan, M. What is the Role of the Consumer in Health Care? J. Soc. Policy 1994, 23, 517–541. [Google Scholar] [CrossRef]
- Elg, M.; Engström, J.; Witell, L.; Poksinska, B. Co-creation and learning in health-care service development. J. Serv. Manag. 2012, 23, 328–343. [Google Scholar] [CrossRef]
- Rantala, K.; Karjaluoto, H. Co-creation in health care: Insights into the transformation from value creation to value co-creation through digitization. In Proceedings of the 20th International Academic Mindtrek Conference, Tampere, Finland, 17–18 October 2016; pp. 34–41. [Google Scholar]
- Nambisan, P.; Nambisan, S. Models of consumer value cocreation in health care. Health Care Manag. Rev. 2009, 47, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Gill, L.; White, L.; Cameron, I.D. Service co-creation in community-based aged healthcare. Manag. Serv. Qual. Int. J. 2011, 21, 152–177. [Google Scholar] [CrossRef]
- Van Oerle, S.; Mahr, D.; Lievens, A. Coordinating online health communities for cognitive and affective value creation. J. Serv. Manag. 2016, 27, 481–506. [Google Scholar] [CrossRef]
- McColl-Kennedy, J.R.; Vargo, S.L.; Dagger, T.S.; Sweeney, J.C.; van Kasteren, Y. Health Care Customer Value Cocreation Practice Styles. J. Serv. Res. 2012, 12, 370–389. [Google Scholar] [CrossRef]
- Casali, G.L.; Perano, M.; Moretta Tartaglione, A.; Zolin, R. How Business Idea Fit Affects Sustainability and Creates Opportunities for Value Co-Creation in Nascent Firms. Sustainability 2018, 10, 189. [Google Scholar] [CrossRef]
- Aslani, P. Patient empowerment and informed decision-making. Int. J. Pharm. Pract. 2013, 21, 347–348. [Google Scholar] [CrossRef] [PubMed]
- Bulsara, C.; Styles, I.; Ward, A.M.; Bulsara, M. The psychometrics of developing the patient empowerment scale. J. Psychosoc. Oncol. 2006, 24, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Shearer, N.; Cisar, N.; Greenberg, E.A. A telephone-delivered empowerment intervention with patients diagnosed with heart failure. Hearung 2007, 36, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Boudioni, M.; McLaren, S.M.; Lister, G. Cross-national diagnostic analysis of patient empowerment in England and Greece. Int. J. Caring Sci. 2012, 5, 246–264. [Google Scholar]
- Wentzer, H.S.; Bygholm, A. Narratives of empowerment and compliance: Studies of communication in online patient support groups. Int. J. Med. Inform. 2013, 82, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Jerofke, T.A. Concept analysis of empowerment from survivor and nurse perspectives within the context of cancer survivorship. Res. Theory Nurs. Pract. 2013, 27, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Ünver, Ö.; Atzori, W. Document D3.2—Questionnaire for Patient Empowerment Measurement Version 1.0; ICT PSP—Empowering Patients: Bruxelles, Belgium, 2013. [Google Scholar]
- Sheridan, S.L. Shared decision making about screening and chemoprevention: A suggested approach from the U.S. preventive service task force. Am. J. Prev. Med. 2004, 26, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Aghili, R.; Khamseh, M.E.; Malek, M.; Banikarimi, A.S.; Baradaran, H.R.; Ebrahim Valojerdi, A. Development and validation of diabetes empowerment questionnaire in Iranian people with type 2 diabetes. Int. Nurs. Rev. 2013, 60, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Schulz, P.J.; Nakamoto, K. Patient behavior and the benefits of artificial intelligence: The perils of “dangerous” literacy and illusory patient empowerment. Patient Educ. Couns. 2013, 92, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Camerini, A.L.; Schulz, P.J. Health literacy and patient empowerment: Separating con-joined twins in the context of chronic low back pain. PLoS ONE 2015, 10, e0118032. [Google Scholar] [CrossRef] [PubMed]
- Eyüboğlu, E.; Schulz, P.J. Do health literacy and patient empowerment affect self-care behaviour? A survey study among Turkish patients with diabetes. BMJ Open 2016, 6, e010186. [Google Scholar] [CrossRef] [PubMed]
- Porr, C.; Drummond, J.; Richter, S. Health literacy as an empowerment tool for low-income mothers. Fam. Community Health 2006, 29, 328–335. [Google Scholar] [CrossRef] [PubMed]
- McGuckin, M.; Govednik, J. Patient empowerment begins with knowledge: Consumer perceptions and knowledge sources for hand hygiene compliance rates. Am. J. Infect. Control 2014, 42, 1106–1108. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.; Wood, F.; Davies, M.; Edwards, A. The development of health literacy in patients with a long-term health condition: The health literacy pathway model. BMC Public Health 2012, 12, 130. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, H.; Kiuchi, T. Health literacy and health communication. Biopsychosoc. Med. 2010, 4, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stiles, E. Promoting health literacy in patients with diabetes. Nurs. Stand. 2011, 26, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.O.; Rose, C.D.; Dilworth, S.E.; Neilands, T.B. Advances in the conceptualization and measurement of health care development and validation of the health care empowerment inventory. PLoS ONE 2012, 7, e45692. [Google Scholar] [CrossRef] [PubMed]
- Topac, V.; Stoicu-Tivadar, V. Patient empowerment by increasing the understanding of medical language for lay users. Methods Inf. Med. 2013, 52, 454–462. [Google Scholar] [PubMed]
- Smith, S.G.; Curtis, L.M.; Wardle, J.; von Wagner, C.; Wolf, M.S. Skill set or mind set? Associations between health literacy. Patient Activation and Health. PLoS ONE 2013, 8, e74373. [Google Scholar] [CrossRef] [PubMed]
- Heijmans, M.; Waverijn, G.; Rademakers, J.; van der Vaart, R.; Rijkena, M. Functional, communicative and critical health literacy of chronic disease patients and their importance for self-management. Patient Educ. Couns. 2015, 98, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Erlen, J.A. Functional health illiteracy. Ethical concerns. Orthop. Nurs. 2004, 23, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, R. The Bright Side and the Dark Side of Patient Empowerment. Co-Creation and Co-Destruction of Value in the Healthcare Environment; Springer: New York, NY, USA, 2017. [Google Scholar]
- Wang, R.H.; Hsu, H.C.; Lee, Y.J.; Shin, S.J.; Lin, K.D.; An, L.W. Patient empowerment interacts with health literacy to associate with subsequent self-management behaviors in patients with type 2 diabetes: A prospective study in Taiwan. Patient Educ. Couns. 2016, 99, 1626–1631. [Google Scholar] [CrossRef] [PubMed]
- Shin, K.S.; Lee, E.H. Relationships of health literacy to self-care behaviors in people with diabetes aged 60 and above: Empowerment as a mediator. J. Adv. Nurs. 2018, 74, 2363–2372. [Google Scholar] [CrossRef] [PubMed]
- Halbach, S.M.; Ernstmann, N.; Kowalski, C.; Pfaff, H.; Pförtner, T.K.; Wesselmannc, S. Unmet information needs and limited health literacy in newly diagnosed breast cancer patients over the course of cancer treatment. Patient Educ. Couns. 2016, 99, 1511–1518. [Google Scholar] [CrossRef] [PubMed]
- Gazmararian, J.A.; Williams, M.V.; Peel, J.; Baker, D.W. Health literacy and knowledge of chronic disease. Patient Educ. Couns. 2003, 51, 267–275. [Google Scholar] [CrossRef]
- Federman, A.D.; Wisnivesky, J.P.; Wolf, M.S.; Leventhal, H.; Halm, E.A. Inadequate health literacy is associated with suboptimal health beliefs in older asthmatics. J. Asthma 2010, 47, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.C.; Boren, D.; Solem, S.L. The Kim Alliance Scale: Development and preliminary testing. Clin. Nurs. Res. 2001, 10, 314–331. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, R.; Annarumma, C.; Adinolfi, P.; Musella, M. The missing link to patient engagement in Italy. The role of health literacy in enabling patients. J. Health Organ. Manag. 2016, 30, 1183–1203. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, C.A.; Rincon, M. Asthma patients’ assessments of health care and medical decision making: The role of health care. J. Asthma 2006, 43, 41–44. [Google Scholar] [CrossRef] [PubMed]
- McCaffery, K.J.; Holmes-Rovner, M.; Smith, S.K.; Rovner, D.; Nutbeam, D.; Clayman, M.L. Addressing health literacy in patient decision aids. BMC Med. Inform. Decis. 2013, 13, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Saviano, M.; Bassano, C.; Calabrese, M. A VSA-SS Approach to Healthcare Service System. The Triple Target of Effectiveness, Efficiency and Sustainability. Serv. Sci. 2010, 2, 41–61. [Google Scholar] [CrossRef]
- Ippolito, A.; Zoccoli, P. Theoretical Contribution to Develop the Classical BSC to Health Care Needs. Int. J. Healthc. Manag. 2013, 6, 37–44. [Google Scholar] [CrossRef]
- Adinolfi, P.; Starace, F.; Palumbo, R. Health Outcomes and Patient Empowerment: The Case of Health Budgets in Italy. J. Health Manag. 2016, 18, 117–133. [Google Scholar] [CrossRef]
- Powers, T.L.; Bendall, D. Improving Health Outcomes Through Patient Empowerment. J. Hosp. Mark. Public Relat. 2004, 15, 45–59. [Google Scholar] [CrossRef]
- Zainuddin, N.; Russell-Bennett, R.; Previte, J. The value of health and wellbeing: An empirical model of value creation in social marketing. Eur. J. Mark. 2013, 47, 1504–1524. [Google Scholar] [CrossRef]
- Osei-Frimpong, K. Examining the effects of patient characteristics and prior value needs on the patient-doctor encounter process in healthcare service delivery. Int. J. Pharm. Healthc. Mark. 2006, 10, 192–213. [Google Scholar] [CrossRef]
- Loane, S.S.; Webster, C.M. Consumer-to-consumer value within social networks. Mark. Rev. 2014, 14, 447–462. [Google Scholar] [CrossRef]
- Buranarach, M.; Thatphithakkul, N.; Kawtrakul, A.; Wongrochananan, S.; Kulnawan, N.; Jiamjarasrangsi, W. Development of service systems to support diabetes patient self-management using a personalized service framework. In Proceedings of the 2011 Annual SRII Global Conference, San Jose, CA, USA, 29 March–2 April 2011; pp. 363–370. [Google Scholar]
- McColl-Kennedy, J.R.; Vargo, S.L.; Dagger, T.S.; Sweeney, J.C. Customers as Resource Integrators: Styles of Customer Co-creation. In Service Science, S-D Logic and Network Theory; Gummesson, E., Mele, C., Polese, F., Eds.; Giannini Editore: Napoli, Italy, 2009. [Google Scholar]
- Lusch, R.F.; Vargo, S.L. Service-dominant logic: Reactions, reflections and refinements. Mark. Theory 2006, 6, 281–288. [Google Scholar] [CrossRef]
- Bove, L.L.; Pervan, S.J.; Beatty, S.E.; Shiu, E. Service worker role in encouraging customer organizational citizenship behaviors. J. Bus. Res. 2008, 62, 698–705. [Google Scholar] [CrossRef]
- Groth, M. Customers as good soldiers: Examining citizenship behaviors in internet service deliveries. J. Manag. 2005, 31, 7–27. [Google Scholar] [CrossRef]
- Yi, Y.; Gong, T. If employees “go the extra mile”, do customers reciprocate with similar behavior? Psychol. Mark. 2008, 25, 961–986. [Google Scholar] [CrossRef]
- Yi, Y.; Nataraajanb, R.; Gong, T. Customer participation and citizenship behavioural influences on employee performance, satisfaction, commitment, and turnover intention. J. Bus. Res. 2011, 64, 87–95. [Google Scholar] [CrossRef]
- Fumagalli, L.; Radaelli, G.; Emanuele, L.; Bertele’, P.; Masella, C. Patient Empowerment and its neighbours: Clarifying the boundaries and their mutual relationships. Health Policy 2015, 119, 384–394. [Google Scholar] [CrossRef] [PubMed]
- Barr, P.J.; Scholl, I.; Bravo, P.; Faber, M.J.; Elwyn, G.; McAllister, M. Assessment of patient empowerment: A systematic review of measures. PLoS ONE 2015, 10, e0126553. [Google Scholar] [CrossRef] [PubMed]
- Cerezo, P.G.; Juvé-Udina, M.E.; Delgado-Hito, P. Concepts and measures of patient empowerment: A comprehensive review. Revista da Escola de Enfermagem da USP 2016, 50, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Defrère, D.; Hinz, P.M.; Mennesson, B.; Hoffmann, W.F.; Millan-Gabet, R.; Skemer, A.J.; Grenz, P. Nulling data reduction and on-sky performance of the Large Binocular Telescope Interferometer. Astrophys. J. 2016, 824, 66. [Google Scholar] [CrossRef]
- Randall, W.S.; Gravier, M.J.; Prybutok, V.R. Connection, trust, and commitment: Dimensions of co-creation? J. Strateg. Mark. 2011, 19, 3–24. [Google Scholar] [CrossRef]
- Xie, C.; Bagozzi, R.P.; Troye, S.V. Trying to prosume: Toward a theory of consumers as co-creators of value. J. Acad. Mark. Sci. 2008, 36, 109–122. [Google Scholar] [CrossRef]
- Payne, A.F.; Storbacka, K.; Frow, P. Managing the co-creation of valu. J. Acad. Mark. Sci. 2008, 36, 83–96. [Google Scholar] [CrossRef]
- Neghina, C.; Caniëls, M.C.J.; Bloemer, J.M.M.; Van Birgelen, M.J.H. Value co-creation in service interactions: Dimensions and antecedents. Mark. Theory 2014, 10, 1–22. [Google Scholar]
- European Patients Forum. Empowered Patients Are an Asset to Society; Conference Report; European Patients Forum: Brussels, Belgium, 2015. [Google Scholar]
- Elfil, M.; Negida, A. Sampling methods in Clinical Research; an Educational Review. Emergency 2017, 5, e52. [Google Scholar] [PubMed]
- Lloyd, R. Quality Health Care: A Guide to Developing and Using Indicators; Jones & Bartlett Publishers: Burlington, MA, USA, 2004. [Google Scholar]
- Gravetter, F.; Forzano, L. Research Methods for the Behavioral Sciences, 4th ed.; Wadsworth: Belmont, CA, USA, 2012. [Google Scholar]
- Smith, J.; Noble, H. Bias in research. Evid.-Based Nurs. 2014, 17, 100–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kline, R.B. Principles and Practice of Structural Equation Modelling, 3rd ed.; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Hair, J.F.; Ringle, C.M.; Sarstedt, M. PLS-SEM: Indeed a silver bullet. J. Mark. Theory Pract. 2011, 19, 139–151. [Google Scholar] [CrossRef]
- Chin, W.W.; Peterson, R.A.; Brown, S.P. Structural equation modeling in marketing: Some practical reminders. J. Mark. Theory Pract. 2008, 16, 287–298. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural equation modelling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Bagozzi, R.P.; Yi, Y. Specification, evaluation, and interpretation of structural equation models. J. Acad. Mark. Sci. 2012, 40, 8–34. [Google Scholar] [CrossRef]
- Wheaton, B.; Muthen, B.; Alwin, D.F.; Summers, G. Assessing Reliability and Stability in Panel Models. Sociol. Methodol. 1977, 8, 84–136. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 5th ed.; Allyn and Bacon: New York, NY, USA, 2007. [Google Scholar]
- Awang, Z. Structural Equation Modeling Using Amos Graphic; UiTM Press: Shah Alam, Malaysia, 2012. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria Versus New Alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Steiger, J.H. Understanding the limitations of global fit assessment in structural equation modeling. Personal. Individ. Differ. 2007, 42, 893–898. [Google Scholar] [CrossRef]
- MacCallum, R.C.; Browne, M.W.; Sugawara, H.M. Power analysis and determination of sample size for covariance structure modeling. Psychol. Methods 1996, 1, 130. [Google Scholar] [CrossRef]
- Byrne, B.M. Structural Equation Modeling with LISREL, PRELIS and SIMPLIS: Basic Concepts, Applications and Programming; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1998. [Google Scholar]
- Diamantopoulos, A.; Siguaw, J.A. Introducing LISREL; Sage Publications: London, UK, 2000. [Google Scholar]
- Chin, W.W. The partial least squares approach to structural equation modeling. Mod. Methods Bus. Res. 1998, 2, 295–336. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Kim, S.C.; Kim, S.; Boren, D. The quality of therapeutic alliance between patient and provider predicts general satisfaction. Mil. Med. 2008, 173, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Wensing, M. Evidence-based patient empowerment. BMJ Qual. Saf. 2000, 9, 200–201. [Google Scholar] [CrossRef] [Green Version]
- Bridges, J.F.P.; Loukanova, S.; Carrera, P. Patient empowerment in health care. In International Encyclopedia of Public Health; Elsevier: San Diego, CA, USA, 2008; pp. 17–28. [Google Scholar]
- Friedman, B.; Wamsley, B.R.; Liebel, D.V.; Saad, Z.B.; Eggert, G.M. Patient satisfaction, empowerment, and health and disability status effects of a disease management-health promotion nurse intervention among Medicare beneficiaries with disabilities. Gerontologist 2009, 49, 778–792. [Google Scholar] [CrossRef] [PubMed]
- Rakhonde, A.K.; Seth, A.; Rakhonde, N.; Chanchlani, R. A prospective study of level of satisfaction among surgical patients in a tertiary care hospital of central India. Int. Surg. J. 2015, 2, 499–504. [Google Scholar] [CrossRef]
- Yeh, M.Y.; Wu, S.C.; Tung, T.H. The relation between patient education, patient empowerment and patient satisfaction: A cross-sectional-comparison study. Appl. Nurs. Res. 2018, 39, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Prakash, B. Patient satisfaction. J. Cutan. Aesthetic Surg. 2010, 3, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Reichheld, F.F. The one number you need to grow. Harv. Bus. Rev. 2003, 81, 46–54. [Google Scholar] [PubMed]
- Prahalad, C.K.; Ramaswamy, V. Co-opting Customer Competence. Harv. Bus. Rev. 2000, 78, 79–87. [Google Scholar]
- Lusch, R.F.; Vargo, S.L.; O’Brien, M. Competing through service: Insights from service-dominant logic. J. Retail. 2007, 83, 5–18. [Google Scholar] [CrossRef]
- Kohler, T.; Fueller, J.; Matzler, K.; Stieger, D. Cocreation in virtual worlds: The design of the user experience. MIS Q. 2011, 35, 773–788. [Google Scholar] [CrossRef]
- Sweeney, J.C.; Danaher, T.S.; McColl-Kennedy, J.R. Customer effort in value cocreation activities improving quality of life and behavioral intentions of health care customers. J. Serv. Res. 2015, 18, 318–335. [Google Scholar] [CrossRef]
- Shaw, G.; Bailey, A.; Williams, A. Aspects of service-dominant logic and its implications for tourism management: Examples from the hotel industry. Tour. Manag. 2011, 32, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Hardyman, W.; Daunt, K.L.; Kitchener, M. Value co-creation through patient engagement in health care: A micro-level approach and research agenda. Public Manag. Rev. 2015, 17, 90–107. [Google Scholar] [CrossRef]
- Britt, T.W.; Castro, C.A.; Adler, A.B. Self-engagement, stressors, and health: A longitudinal study. Personal. Soc. Psychol. Bull. 2005, 31, 1475–1486. [Google Scholar] [CrossRef] [PubMed]
- Bloom, G.; Standing, H.; Lloyd, R. Markets, information asymmetry and health care: Towards new social contracts. Soc. Sci. Med. 2008, 66, 2076–2087. [Google Scholar] [CrossRef] [PubMed]
- Engström, J. Co-Creation in Health Care Service Development—A Diary-Based approach. Linköping Studies in Science and Technology. Ph.D. Thesis, Linköping University, Linköping, Sweden, 2012. [Google Scholar]
- Barile, S.; Saviano, M.; Polese, F. Information asymmetry and co-creation in health care services. Australas. Mark. J. 2014, 22, 205–217. [Google Scholar] [CrossRef]
- Barile, S.; Orecchini, F.; Saviano, M.; Farioli, F. People, technology, and governance for sustainability: The contribution of systems and cyber-systemic thinking. Sustain. Sci. 2018, 13, 1197–1208. [Google Scholar] [CrossRef]
- Caputo, F. Approccio Sistemico e Co-Creazione di Valore in Sanità; Edizioni Nuova Cultura: Rome, Italy, 2018. [Google Scholar]
- Faulkner, M. A measure of patient empowerment in hospital environments catering for older people. J. Adv. Nurs. 2001, 34, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Shiu, A.T.; Wong, R.Y.; Thompson, D.R. Development of a reliable and valid Chinese version of the diabetes empowerment scale. Diabetes Care 2003, 26, 2817–2821. [Google Scholar] [CrossRef] [PubMed]
- Tol, A.; Sharifirad, G.R.; Pourreza, A.G.; Rahimi, A.; Shojaeezadeh, D.; Mohrajeritehrani, M.R.; Alhani, F. Development of a valid and reliable diabetes empowerment scale: An Iranian version. Iran. Red. Crescent Med. J. 2012, 14, 305–308. [Google Scholar] [PubMed]
- Leksell, J.; Funnell, M.; Sandberg, G.; Smide, B.; Wiklund, G.; Wikblad, K. Psychometric properties of the Swedish Diabetes Empowerment Scale. Scand. J. Caring Sci. 2007, 21, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.F.; Wang, R.H.; Cheng, C.P.; Chin, C.C.; Stocker, J.; Tang, S.M.; Chen, S.W. Diabetes Empowerment Process Scale: Development and psychometric testing of the Chinese version. J. Adv. Nurs. 2011, 67, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Arvidsson, S.; Bergman, S.; Arvidsson, B.; Fridlund, B.; Tingstrom, P. Psychometric properties of the Swedish Rheumatic Disease Empowerment Scale, SWE-RES-23. Musculoskelet. Care 2012, 10, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Hansson, L.; Bjorkman, T. Empowerment in people with a mental illness: Reliability and validity of the Swedish version of an empowerment scale. Scand. J. Caring Sci. 2005, 19, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Suzuki, K. Application of Empowerment Scale to patients with schizophrenia: Japanese experience. Psychiatry Clin. Neurosci. 2007, 61, 594–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrigan, P.W.; Faber, D.; Rashid, F.; Leary, M. The construct validity of empowerment among consumers of mental health services. Schizophr. Res. 1999, 38, 77–84. [Google Scholar] [CrossRef]
Figure 1.
Research model.

Figure 2.
The structural model.


{kind=link}
{kind=link}
Table 1.
Contributions of patient empowerment to health value sustainability.
| PE Dimension. | Value for Organizations | Value for the Community |
|---|---|---|
| Health literacy |
|
|
| Patient participation |
|
|
| Patient control |
|
|
| Communication with healthcare professionals |
|
|
Table 2.
The measurement scales.
| Main Constructs | Scales | Items | Sources |
|---|---|---|---|
| Patient empowerment | Health Literacy (HL) | 5 | [72] |
| Patient Participation (PP) | 3 | [26,60] | |
| Patient Control (PC) | 4 | [20,21] | |
| Communication with Healthcare Professionals (CHP) | 10 | [25] | |
| Value co-creation | Patient Participation Behavior (PPB) | 10 | [40] |
| Patient Citizenship Behavior (PCB) | 5 |
Table 3.
Characteristics of the sample.
| Variable | n (%) |
|---|---|
| Age | |
| 18–30 | 33 (13.2%) |
| 31–50 | 86 (34.4%) |
| 51–70 | 101 (40.4%) |
| >70 | 30 (12.0%) |
| Levels of education | |
| Primary education | 29 (11.6%) |
| Lower secondary education | 49 (19.6%) |
| Upper secondary education | 82 (32.8%) |
| First stage of tertiary education | 55 (22.0%) |
| Second stage of tertiary education | 35 (14.0%) |
| Chronic diseases * | |
| Diabetes | 48 (19.2%) |
| Hypertension | 35 (14.0%) |
| Cardiac decompensation/cardiovascular diseases | 50 (20.0%) |
| Arthrosis | 28 (11.2%) |
| Arthritis | 25 (10.0%) |
| Muscle-degenerative diseases | 21 (8.4%) |
| Chronic respiratory diseases/COPD | 20 (8.0%) |
| Others | 23 (9.2%) |
* in the case of multiple diseases, it was indicated in the questionnaire to indicate the disease that the patient considered to be the main one.
Table 4.
The measurement model.
| Construct | Item | Composite Reliability | Factor loading |
|---|---|---|---|
| Second-order construct | |||
| Patient empowerment | HL | - | 0.85 |
| PP | 10.901 | 0.928 | |
| PC | 10.797 | 0.905 | |
| CHP | 10.61 | 0.964 | |
| Value co-creation | PPB | - | 0.98 |
| PCB | 10.989 | 0.931 | |
| First-order constructs | |||
| HL | I collect additional information on my disease from various sources | - | 0.771 |
| I select the most relevant information for my specific case | 16.954 | 0.859 | |
| I understand the information obtained | 11.334 | 0.723 | |
| I ensure that the information obtained is appropriate for my disease | 12.784 | 0.759 | |
| I check the validity, reliability and credibility of the information obtained | 12.346 | 0.787 | |
| PP | I look for information about possible treatment alternatives | 0.815 | |
| I talk to my doctor if I change idea about my treatment | 12.736 | 0.756 | |
| When treatment goals are not met, I discuss any remedies with my doctor | 12.552 | 0.748 | |
| PC | I am committed to keeping my health status as best I can | - | 0.815 |
| I recognize when my lifestyle is worsening my health | 14.256 | 0.802 | |
| I take the commitment to my treatment seriously | 14.863 | 0.827 | |
| I maintain lifestyle changes that are necessary for my health | 11.848 | 0.697 | |
| CHP | I always express my opinion to professionals | 0.751 | |
| I provide all the information my doctors need | 13.784 | 0.826 | |
| I ask all the questions necessary to get the answers I need | 13.574 | 0.816 | |
| I ask for further explanation of what I do not understand | 13.696 | 0.822 | |
| I describe my symptoms in detail | 13.794 | 0.827 | |
| I describe in detail my clinical history and allergies | 13.964 | 0.835 | |
| I am honest about my habits and lifestyle even when they are damaging to health | 13.374 | 0.805 | |
| I admit when I do not follow the directions or the treatment as prescribed | 13.633 | 0.818 | |
| I can easily dialogue with professionals | 14.102 | 0.842 | |
| I always ask for additional information | 13.421 | 0.808 | |
| PPB | I gave the professional proper information | - | 0.781 |
| I provided necessary information so that the professional could perform his or her duties | 19.695 | 0.748 | |
| I answered all the professional’s service-related questions | 16.268 | 0.899 | |
| I performed all the tasks that are required | 14.088 | 0.807 | |
| I adequately completed all the expected behaviors | 12.932 | 0.755 | |
| I behaved responsibly towards health professionals | 14.73 | 0.835 | |
| I followed the professional’s directives or orders | 13.526 | 0.783 | |
| I was friendly to the professional | 13.298 | 0.771 | |
| I was kind to the professional | 13.194 | 0.767 | |
| I was polite to the professional | 13.478 | 0.779 | |
| PCB | When I receive good service from the professional, I comment about it | - | 0.716 |
| When I experience a problem, I let the professional know about it | 11.787 | 0.784 | |
| I said positive things about the service and the professionals to others | 12.687 | 0.85 | |
| I recommended the service and the professionals to others | 11.444 | 0.769 | |
| I encouraged friends and relatives to use the same service | 11.855 | 0.796 | |
Table 5.
Correlations, Average Variance Extracted (AVE) and reliability.
| Measure | HL | PP | PC | CHP | PPB | PCB | AVE | Composite Reliability |
|---|---|---|---|---|---|---|---|---|
| HL | 1.00 | 0.61 | 0.886 | |||||
| PP | 0.676 | 1.00 | 0.598 | 0.816 | ||||
| PC | 0.677 | 0.744 | 1.00 | 0.619 | 0.866 | |||
| CHP | 0.712 | 0.768 | 0.763 | 1.00 | 0.664 | 0.951 | ||
| PPB | 0.686 | 0.663 | 0.762 | 0.840 | 1.00 | 0.629 | 0.944 | |
| PCB | 0.621 | 0.655 | 0.664 | 0.761 | 0.803 | 1.00 | 0.614 | 0.888 |
Notes: All correlations were significant at the 0.01 level; model measurement fit: χ2 = 1334.56 (df = 601, p < 0.01); comparative fit index (CFI) = 0.92; root mean square error of approximation (RMSEA) = 0.07; standardized root mean square residual (SRMR) = 0.04.
Table 6.
The structural model.
| Unst. Coeff. | SE | Std. Coeff. | |
|---|---|---|---|
| Structural effects | |||
| Patient empowerment → Value Co-creation | 0.95 ** | 0.092 | 0.950 |
| Model fit | |||
| χ2 | 1334.56, df = 601, p < 0.01 | ||
| RMSEA | 0.069 | ||
| CFI | 0.921 | ||
| SRMR | 0.04 | ||
Notes: * p < 0.05; ** p < 0.01.
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Russo, G.; Moretta Tartaglione, A.; Cavacece, Y. Empowering Patients to Co-Create a Sustainable Healthcare Value. Sustainability 2019, 11, 1315. https://doi.org/10.3390/su11051315
AMA Style
Russo G, Moretta Tartaglione A, Cavacece Y. Empowering Patients to Co-Create a Sustainable Healthcare Value. Sustainability. 2019; 11(5):1315. https://doi.org/10.3390/su11051315
Chicago/Turabian StyleRusso, Giuseppe, Andrea Moretta Tartaglione, and Ylenia Cavacece. 2019. "Empowering Patients to Co-Create a Sustainable Healthcare Value" Sustainability 11, no. 5: 1315. https://doi.org/10.3390/su11051315
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.