Evaluation of UR-UVGI System for Sterilization Effect on Microorganism Contamination in Negative Pressure Isolation Ward

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
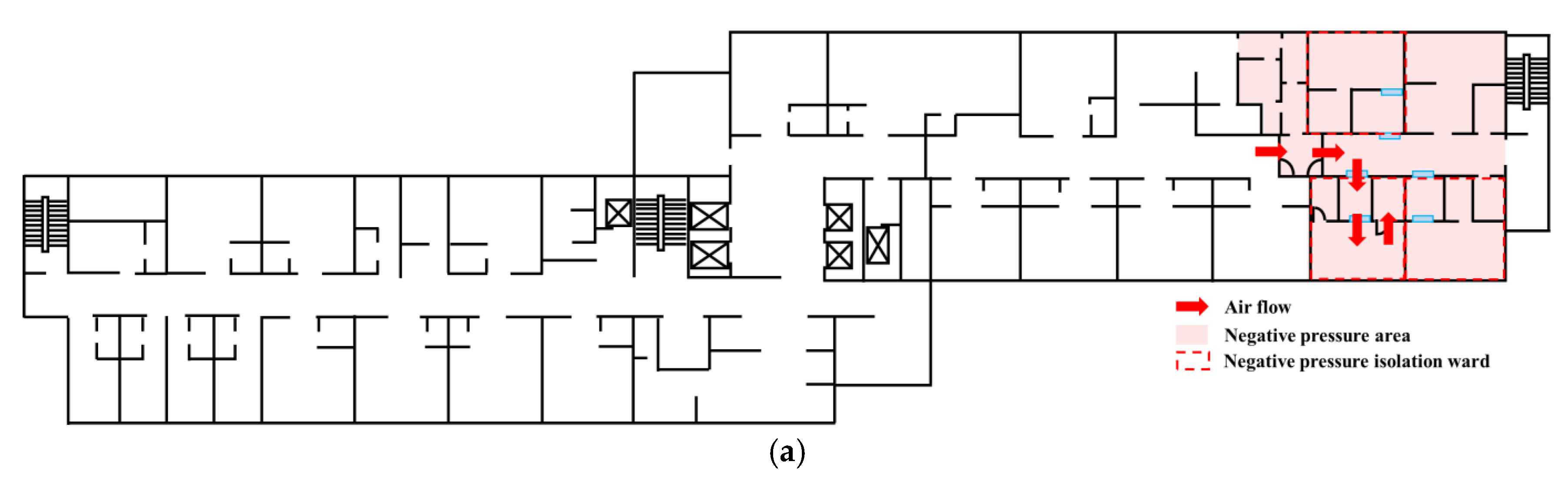
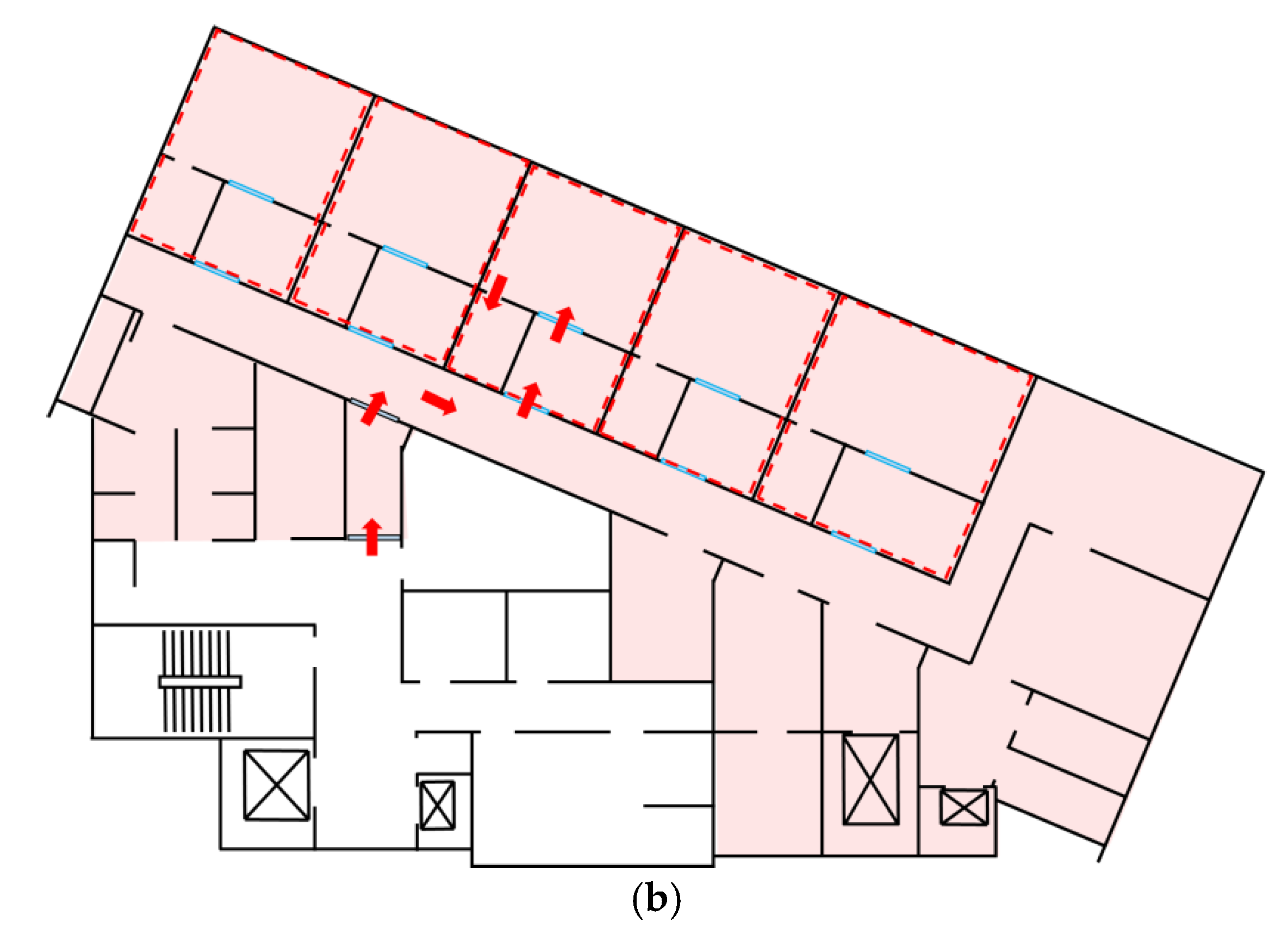
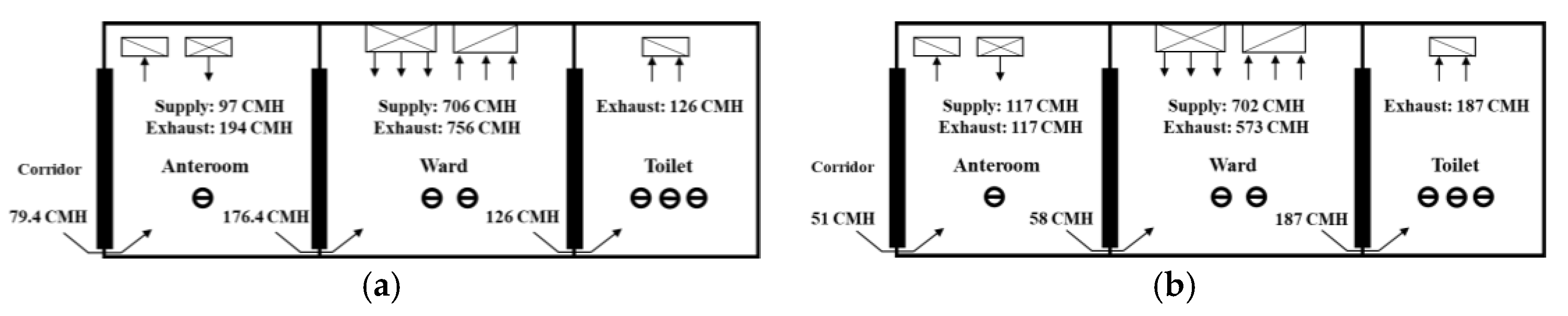
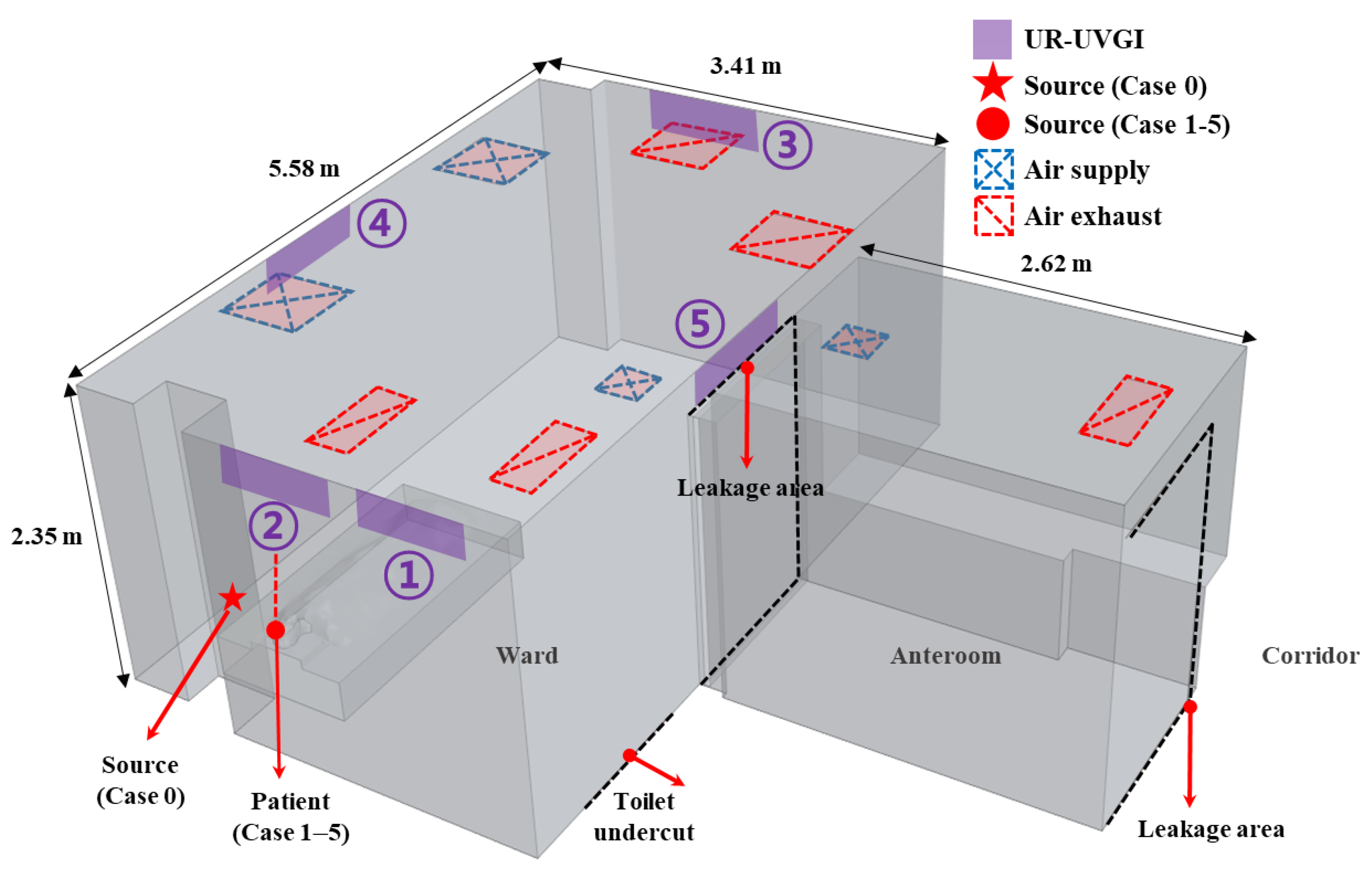
2.1. Study Subject: Negative Pressure Isolation Facility
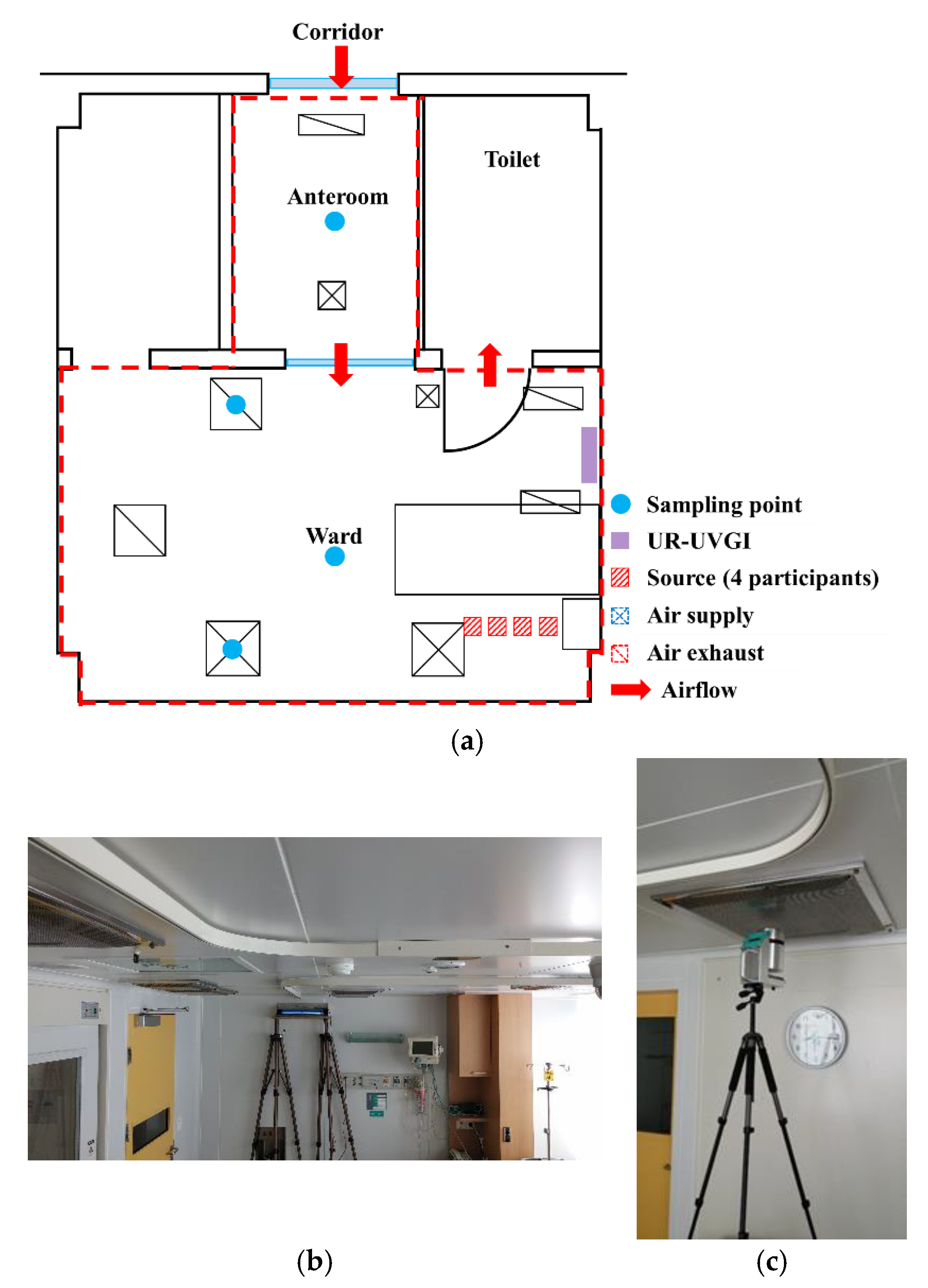
2.2. Experimental Setup
2.3. Numerical Simulation
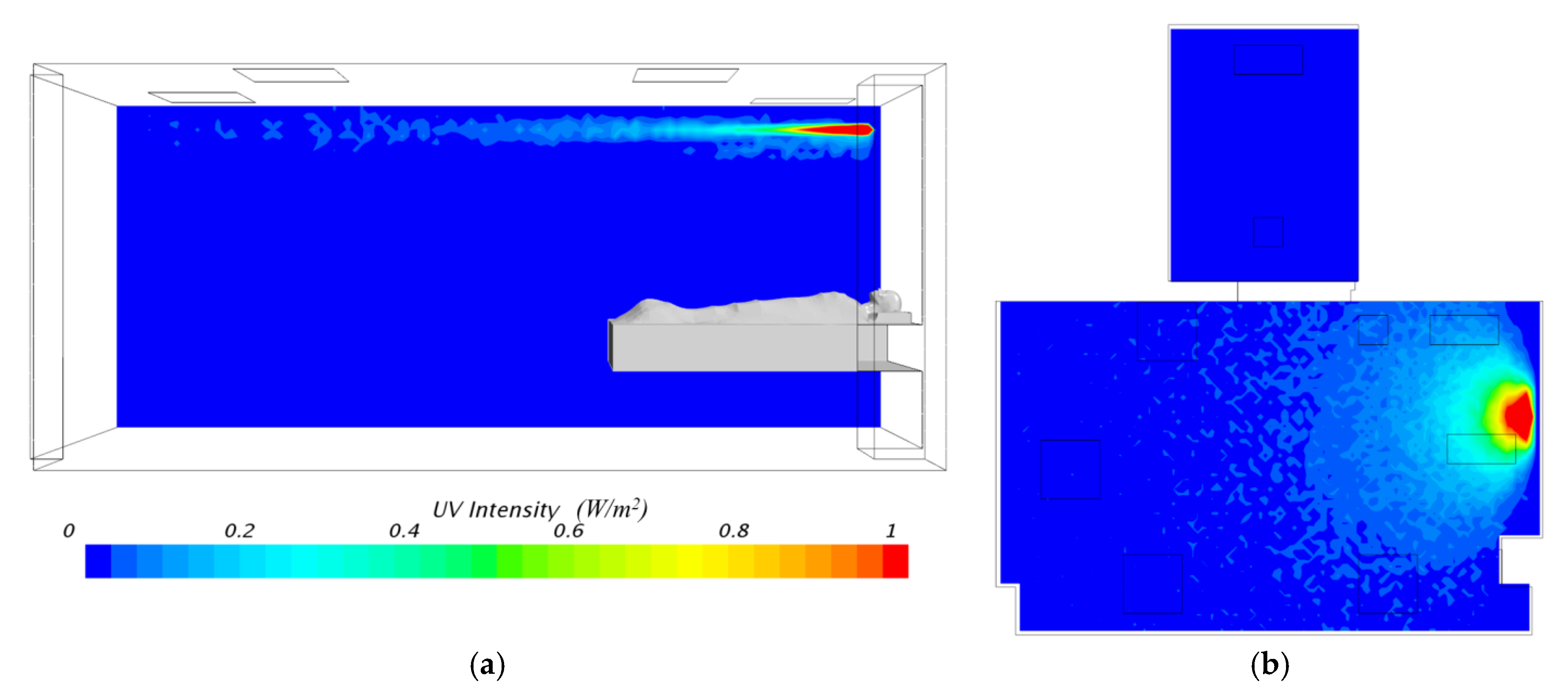
2.3.1. UV Intensity Distribution
2.3.2. CFD Simulation
3. Results
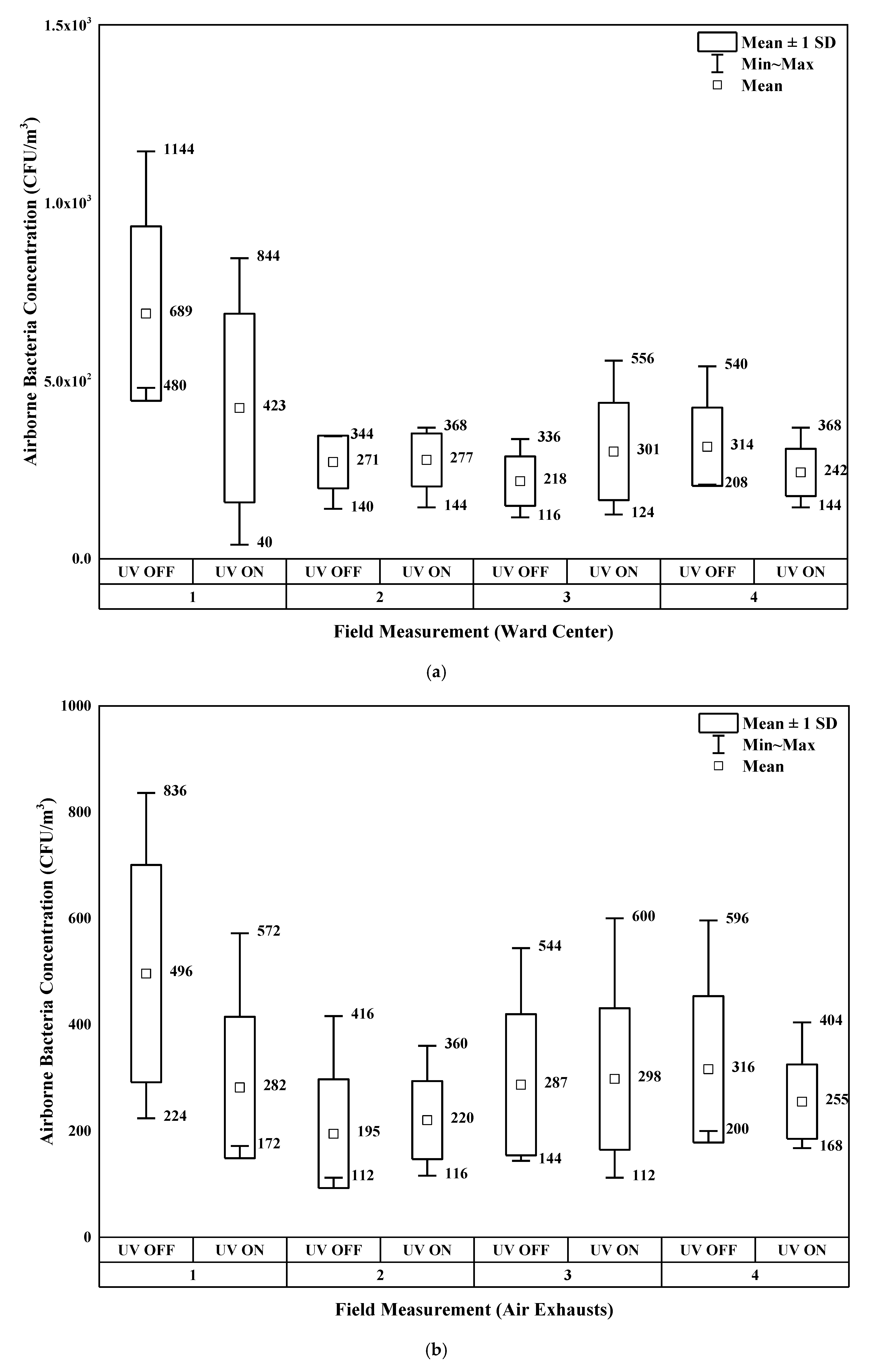
3.1. Experimental Results
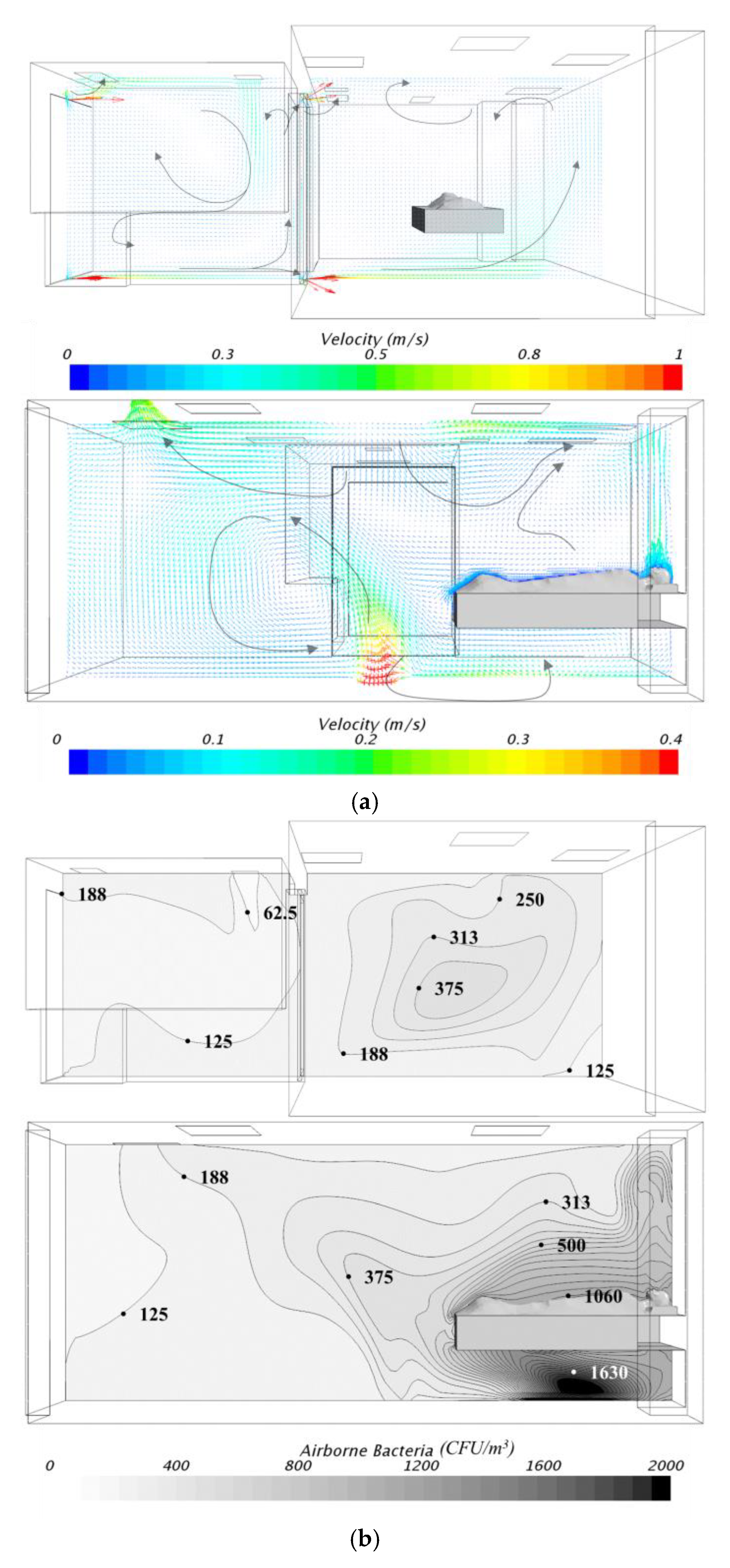
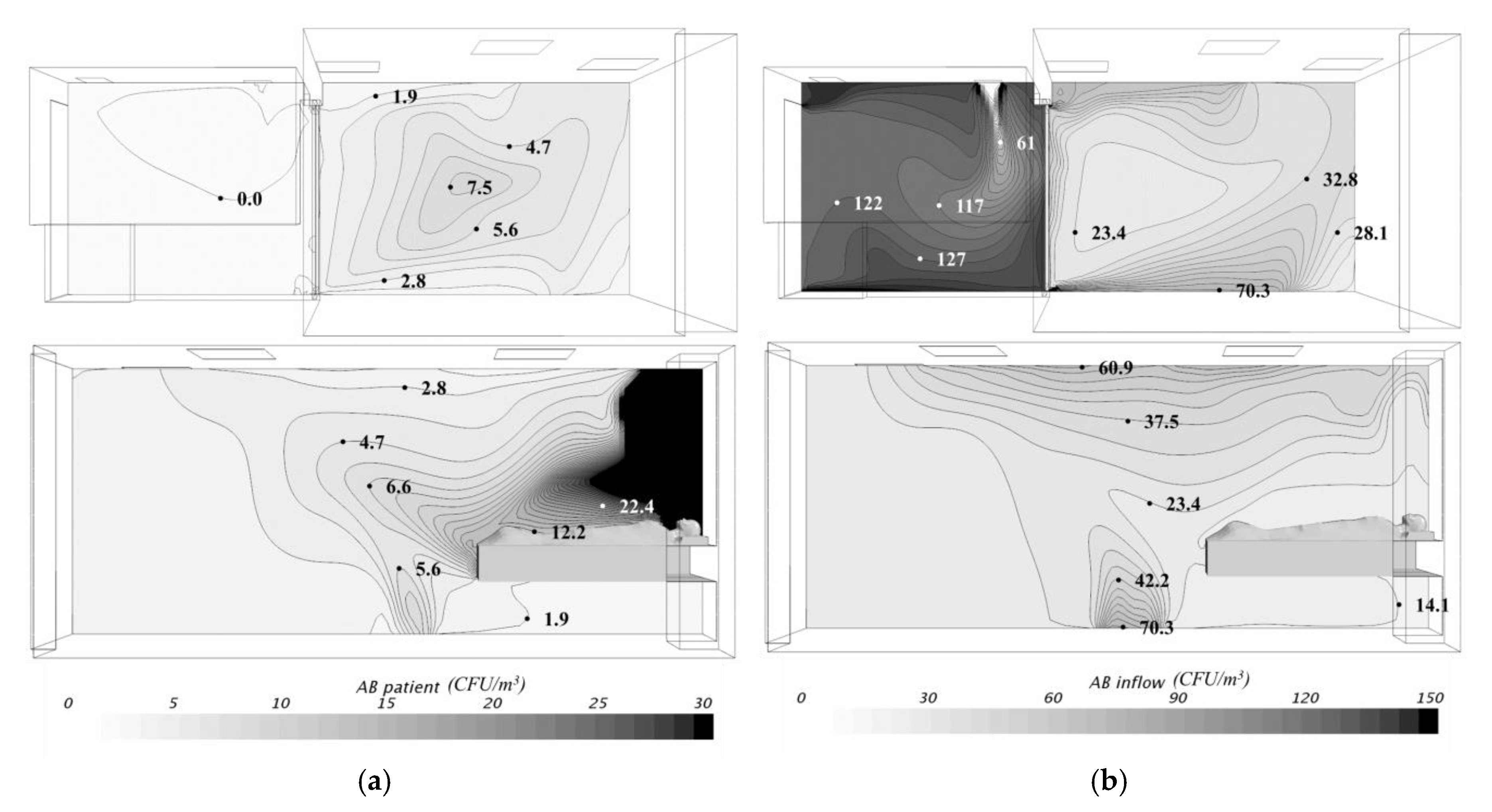
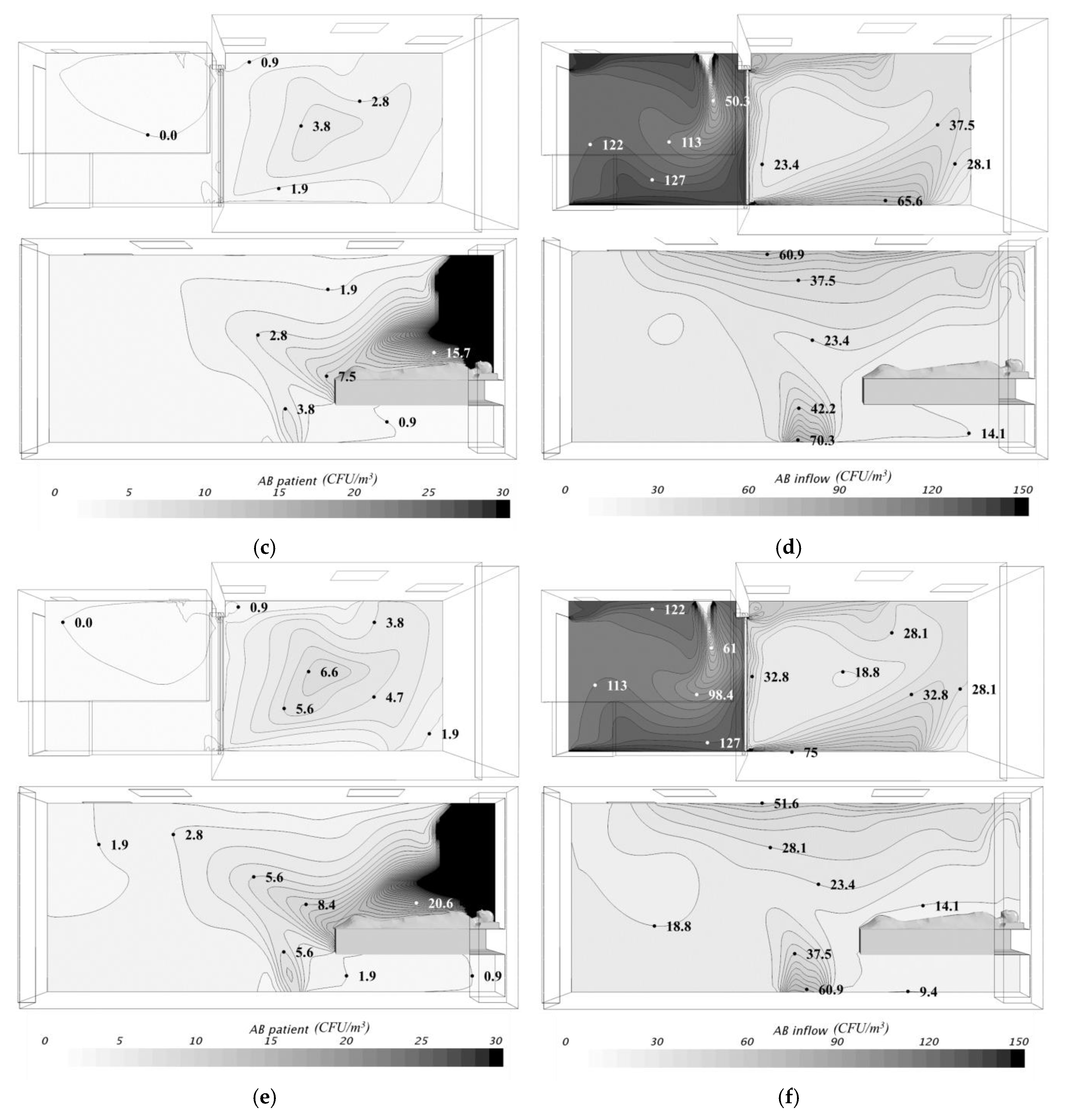
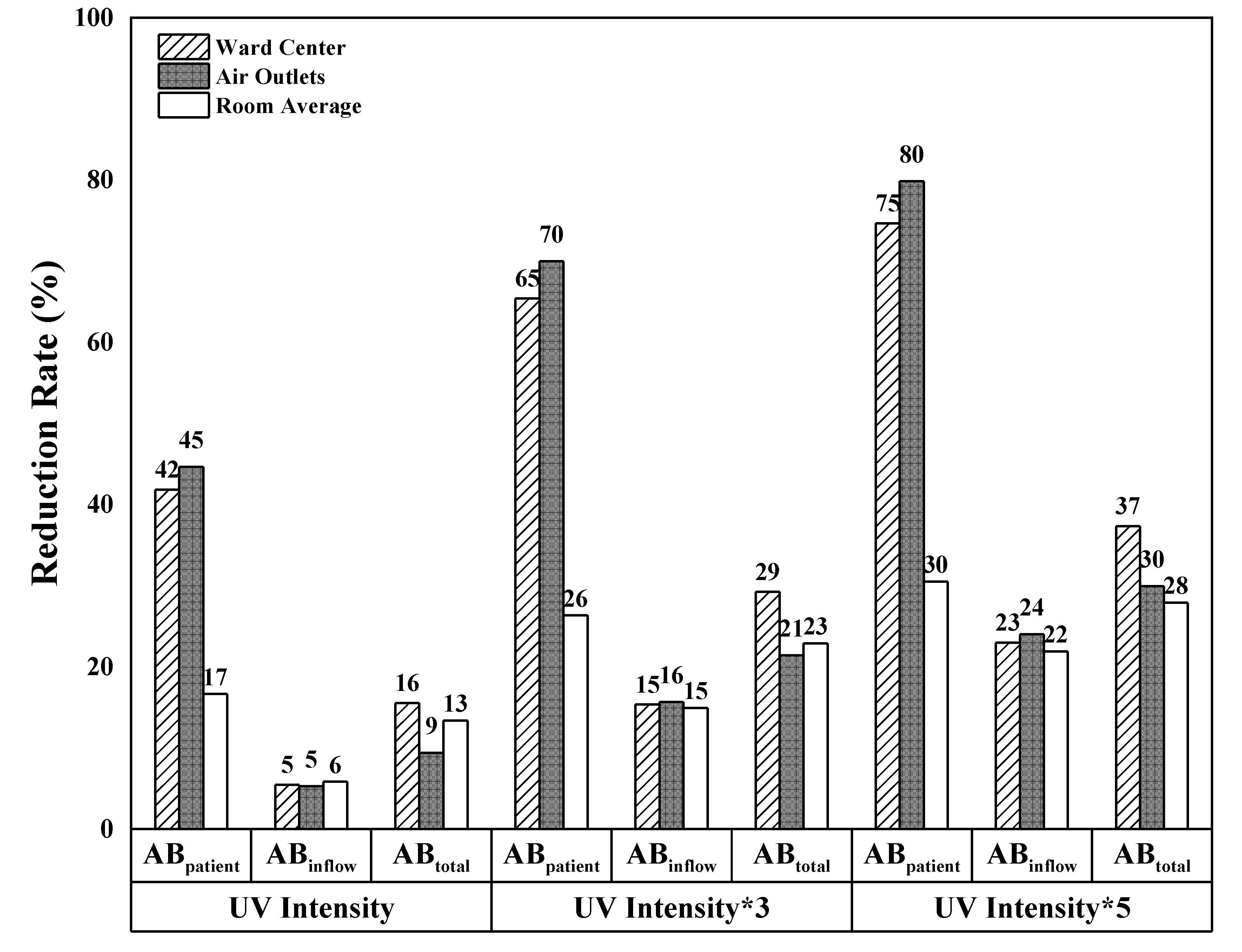
3.2. Numerical Simulation Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Korea Center for Disease Control and Prevention. Guidelines for Operation and Management of Nationally Designed Hospital Beds; Ministry for Health and Welfare: Cheongju-si, Korea, 2017.
- Interim Infection Prevention and Control Recommendations for Hospitalized Patients with Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Available online: https://www.cdc.gov/coronavirus/mers/infection-prevention-control.html (accessed on 6 August 2018).
- Frequently Asked Questions on Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Available online: http://www.who.int/csr/disease/coronavirus_infections/faq/en/ (accessed on 6 August 2018).
- Sehulster, L.; Chinn, R.Y.; Arduino, M.J.; Carpenter, J.; Donlan, R.; Ashford, D.; Besser, R.; Fields, B.; McNeil, M.M.; Whitney, C. Guidelines for environmental infection control in health-care facilities. MMWR Recomm. Rep. 2003, 52, 1–42. [Google Scholar] [PubMed]
- Jensen, P.A.; Lambert, L.A.; Iademarco, M.F.; Ridzon, R. Guidelines for Preventing the Transmission of Mycobacterium Tuberculosis in Health-Care Settings; Center for Disease Control and Prevention: Atlanta, GA, USA, 2005.
- Yanagi, U.; Kagi, N.; Ikeda, K.; Nishimura, N.; Yoshino, H.; Obata, M.; Saito, H.; Saito, K.; Kamakura, R. A Study on the Way of Maintenance of Sanitary Environment in Medical Facilities: Part2-The actual status and countermeasures of airborne microbe contamination in waiting rooms. Trans. Soc. Heat. Air Condit. Sanit. Eng. Jpn. 2008, 33, 9–17. [Google Scholar] [CrossRef]
- Siegel, J.D.; Rhinehart, E.; Jackson, M.; Chiarello, L.; Health Care Infection Control Practices Advisory Committee. 2007 guideline for isolation precautions: Preventing transmission of infectious agents in health care settings. Am. J. Infect. Control 2007, 35, S65–S164. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Interim WHO Infection Control Guidelines for Health Care Facilities: AI, including Influenza A (H5N1) in Humans. Available online: http://www.wpro.who.int/emerging_diseases/documents/AI_Inf_Control_Guide_10May2007/en/ (accessed on 6 August 2018).
- Schoen, L.J.; Hodgson, M.J.; McCoy, W.F.; Miller, S.L.; Li, Y.; Olmsted, R.N.; Sekhar, C. ASHRAE Position Document on Airborne Infectious Diseases; ASHRAE: Atlanta, GA, USA, 2009. [Google Scholar]
- Rutala, W.A.; Weber, D.J. Guideline for Disinfection and Sterilization in Healthcare Facilities; Center for Disease Control and Prevention: Atlanta, GA, USA, 2008.
- Lindsley, W.G.; Blachere, F.M.; Davis, K.A.; Pearce, T.A.; Fisher, M.A.; Khakoo, R.; Davis, S.M.; Rogers, M.E.; Thewlis, R.E.; Posada, J.A.; et al. Distribution of airborne influenza virus and respiratory syncytial virus in an urgent care medical clinic. Clin. Infect. Dis. 2010, 50, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Gilkeson, C.A.; Noakes, C.J.; Khan, M.A.I. Computational fluid dynamics modelling and optimisation of an upper-room ultraviolet germicidal irradiation system in a naturally ventilated hospital ward. Indoor Built Environ. 2014, 23, 449–466. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.-M.; Cheng, H.-T. The influence of the bed with a semiopen hood on bacteria removal in a negative-pressure isolation room. Adv. Mech. Eng. 2014, 6, 468232. [Google Scholar] [CrossRef]
- Fletcher, L.A.; Noakes, C.J.; Beggs, C.B.; Sleigh, P.A. The importance of bioaerosols in hospital infections and the potential for control using germicidal ultraviolet irradiation. In Proceedings of the First Seminar on Applied Aerobiology, Murcia, Spain, 20 May 2004. [Google Scholar]
- Hollaender, A.; Oliphant, J.W. The inactivating effect of monochromatic ultraviolet radiation on influenza virus. J. Bacteriol. 1944, 48, 447–454. [Google Scholar] [PubMed]
- Macher, J.M.; Alevantis, L.E.; Chang, Y.-L.; Liu, K.-S. Effect of ultraviolet germicidal lamps on airborne microorganisms in an outpatient waiting room. Appl. Occup. Environ. Hyg. 1992, 7, 505–513. [Google Scholar] [CrossRef]
- Memarzadeh, F.; Jiang, J. Methodology for minimizing risk from airborne organisms in hospital isolation rooms. ASHRAE Trans. 2000, 106, 731–747. [Google Scholar]
- Ko, G.; First, M.W.; Burge, H.A. The characterization of upper-room ultraviolet germicidal irradiation in inactivating airborne microorganisms. Environ. Health Perspect. 2002, 110, 95–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, P.; Peccia, J.; Fabian, P.; Martyny, J.W.; Fennelly, K.P.; Hernandez, M.; Miller, S.L. Efficacy of ultraviolet germicidal irradiation of upper-room air in inactivating airborne bacterial spores and mycobacteria in full-scale studies. Atmos. Environ. 2003, 37, 405–419. [Google Scholar] [CrossRef]
- Menzies, D.; Popa, J.; Hanley, J.A.; Rand, T.; Milton, D.K. Effect of ultraviolet germicidal lights installed in office ventilation systems on workers’ health and wellbeing: Double-blind multiple crossover trial. Lancet 2003, 362, 1785–1791. [Google Scholar] [CrossRef]
- Brickner, P.W.; Vincent, R.L. Ultraviolet germicidal irradiation safety concerns: A lesson from the tuberculosis ultraviolet shelter study: Murphy’s law affirmed. Photochem. Photobiol. 2003, 89, 819–821. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-W.; Li, S.-Y.; Huang, S.-H.; Huang, C.-K.; Chen, Y.-Y.; Chen, C.-C. Effects of ultraviolet germicidal irradiation and swirling motion on airborne Staphylococcus aureus, Pseudomonas aeruginosa and Legionella pneumophila under various relative humidities. Indoor Air 2013, 23, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Kanaan, M.; Ghaddar, N.; Ghali, K.; Araj, G. New airborne pathogen transport model for upper-room UVGI spaces conditioned by chilled ceiling and mixed displacement ventilation: Enhancing air quality and energy performance. Energy Convers. Manag. 2014, 85, 50–61. [Google Scholar] [CrossRef]
- Memarzadeh, F.; Olmsted, R.N.; Bartley, J.M. Applications of ultraviolet germicidal irradiation disinfection in health care facilities: Effective adjunct, but not stand-alone technology. Am. J. Infect. Control 2010, 38, S13–S24. [Google Scholar] [CrossRef] [PubMed]
- Gilkeson, C.A.; Noakes, C. Application of CFD simulation to predicting upper-room UVGI effectiveness. Photochem. Photobiol. 2013, 89, 799–810. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Fisher, N.; Miller, S.L. Using computational fluid dynamics modeling to evaluate the design of hospital ultraviolet germicidal irradiation systems for inactivating airborne mycobacteria. Photochem. Photobiol. 2013, 89, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Noakes, C.J.; Sleigh, P.A.; Fletcher, L.A.; Beggs, C.B. Use of CFD modelling to optimise the design of upper-room UVGI disinfection systems for ventilated rooms. Indoor Built Environ. 2006, 15, 347–356. [Google Scholar] [CrossRef]
- Sung, M.; Kato, S. Method to evaluate UV dose of upper-room UVGI system using the concept of ventilation efficiency. Build. Environ. 2010, 45, 1626–1631. [Google Scholar] [CrossRef]
- Sung, M.; Kato, S. Estimating the germicidal effect of upper-room UVGI system on exhaled air of patients based on ventilation efficiency. Build. Environ. 2011, 46, 2326–2332. [Google Scholar] [CrossRef]
- Kowalski, W. Ultraviolet Germicidal Irradiation Handbook: UVGI for Air and Surface Disinfection; Springer Science & Business Media: Berlin, Germany, 2010. [Google Scholar]
- Rohdin, P.; Moshfegh, B. Numerical modelling of industrial indoor environments: A comparison between different turbulence models and supply systems supported by field measurements. Build. Environ. 2011, 46, 2365–2374. [Google Scholar] [CrossRef]
- Noakes, C.J.; Fletcher, L.A.; Beggs, C.B.; Sleigh, P.A.; Kerr, K.G. Development of a numerical model to simulate the biological inactivation of airborne microorganisms in the presence of ultraviolet light. J. Aerosol Sci. 2004, 35, 489–507. [Google Scholar] [CrossRef] [Green Version]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Details |
|---|---|
| Pressure difference | Maintenance of negative pressure between rooms (adjusted by setting exhaust air volume at a greater value than supply air volume) |
| 2.5 Pa or higher (0.01 mmAq) | |
| Ventilation rate | 6 ACH or higher (12 ACH recommended) |
| Airflow | Inflow of air into ward for infected patients |
| Others | Installation of HEPA filters that can eliminate 99.97% of particles of size 0.3-μm or greater passing through the air exhaust |
| If the leakage area is 0.5 ft2, the difference in volume of supply and exhaust air is 125 cfm or higher |
| Component | UV-C Reflectivity (%) | Visible Light Reflectivity (%) |
|---|---|---|
| Aluminum, etched | 88 | 90 |
| Black lacquer paint | 5 | 9 |
| CFU/m3) | Remodeled Facility | Stand-Alone Facility | ||||||
|---|---|---|---|---|---|---|---|---|
| Ante-Room | Ward | Ante-Room | Ward | |||||
| Center | Air Supply | Air Exhaust | Center | Air Supply | Air Exhaust | |||
| Average (±standard deviation) | 110.4 (±57) | 102.4 (±79) | 3.2 (±4.7) | 97.6 (±61) | 22.5 (±17) | 2.5 (±3) | 1.3 (±2) | 5 (±4) |
| CFU/m3 | UR-UVGI OFF | UR-UVGI ON | Reduction Rate (%) | |||
|---|---|---|---|---|---|---|
| Ward-Center | Ward-Exhaust | Ward-Center | Ward-Exhaust | Ward-Center | Ward-Exhaust | |
| Experiment | 373 ± 232 * | 312 ± 179 | 310 ± 165 | 263 ± 103 | 16.9 | 15.7 |
| Simulation (Case 0) | 392 | 162 | 382 | 150 | 2.6 | 7.4 |
| Airborne Bacteria Concentration (CFU/m3) | Anteroom Center | Ward | Room Average (Ward) | ||
|---|---|---|---|---|---|
| Center | Air exhausts | ||||
| Control case (UV off) | ABPatient | - | 8.5 | 2.8 | 57.3 |
| ABInflow | 117.1 | 22.1 | 23.3 | 24.8 | |
| AB | 117.1 | 30.7 | 26.1 | 82.1 | |
| Case 1 | ABPatient | - | 4.9 (41.8%) | 1.5 (44.6) | 47.8 (16.6) |
| ABInflow | 117.2 | 20.9 (5.4) | 22.1 (5.2) | 23.3 (5.8) | |
| AB | 117.2 | 25.9 (15.5) | 23.7 (9.4) | 71.1 (13.4) | |
| Case 2 | ABPatient | - | 6.4 (24.2) | 2.0 (28.1) | 50.5 (11.9) |
| ABInflow | 117.2 | 20.8 (6.1) | 22.1 (5.5) | 23.1 (6.6) | |
| AB | 117.2 | 27.3 (11.1) | 24.0 (7.9) | 73.7 (10.3) | |
| Case 3 | ABPatient | - | 8.4 (1.2) | 2.5 (9.9) | 57.2 (0.2) |
| ABInflow | 117.2 | 21.5 (3.0) | 21.8 (6.8) | 23.8 (3.8) | |
| AB | 117.2 | 29.9 (2.5) | 24.3 (7.1) | 81.1 (1.3) | |
| Case 4 | ABPatient | - | 7.2 (15.5) | 2.1 (22.4) | 55.3 (3.6) |
| ABInflow | 117.2 | 20.2 (8.9) | 21.4 (8.4) | 22.8 (7.9) | |
| AB | 117.2 | 27.4 (10.7) | 23.5 (9.9) | 78.1 (4.9) | |
| Case 5 | ABPatient | - | 8.0 (6.3) | 2.4 (11.7) | 56.4 (1.7) |
| ABInflow | 117.2 | 18.9 (14.6) | 20.3 (13.3) | 21.2 (14.2) | |
| AB | 117.2 | 26.9 (12.3) | 22.7 (13.1) | 77.6 (5.5) | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bang, J.-I.; Park, J.; Choi, A.; Jeong, J.-W.; Kim, J.Y.; Sung, M. Evaluation of UR-UVGI System for Sterilization Effect on Microorganism Contamination in Negative Pressure Isolation Ward. Sustainability 2018, 10, 3192. https://doi.org/10.3390/su10093192
Bang J-I, Park J, Choi A, Jeong J-W, Kim JY, Sung M. Evaluation of UR-UVGI System for Sterilization Effect on Microorganism Contamination in Negative Pressure Isolation Ward. Sustainability. 2018; 10(9):3192. https://doi.org/10.3390/su10093192
Chicago/Turabian StyleBang, Jong-Il, Jeongyeon Park, Anseop Choi, Jae-Weon Jeong, Jin Yong Kim, and Minki Sung. 2018. "Evaluation of UR-UVGI System for Sterilization Effect on Microorganism Contamination in Negative Pressure Isolation Ward" Sustainability 10, no. 9: 3192. https://doi.org/10.3390/su10093192