
Why Certain Repurposed Drugs Are Unlikely to Be Effective Antivirals to Treat SARS-CoV-2 Infections
 , , , , and
, , , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Drug Candidates
2.2. Cells and Viruses
2.3. In Vitro Evaluation of Compounds versus SARS-CoV-2
2.3.1. Measurement of Half Maximal Cytotoxic Concentration (CC50)
2.3.2. Measurement of In Vitro Anti-SARS-CoV-2 Activity (EC50 and EC90)
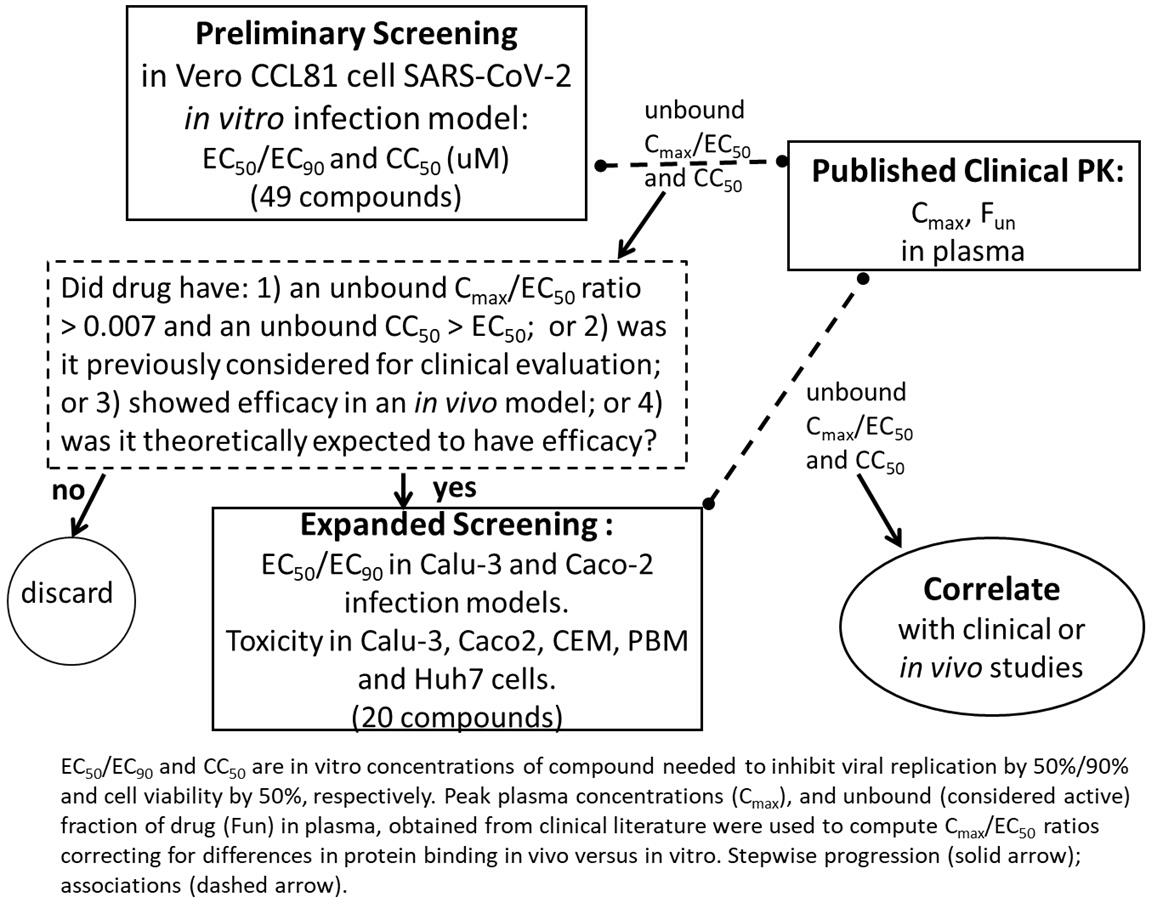
2.4. Pharmacokinetics (PK) and Assessment of the Relative Clinical Potential of Compounds

{kind=link}
| Cmax (μM) | Calu-3 SARS-CoV-2 | Caco-2 SARS-CoV-2 | Vero CCL-81 SARS-CoV-2 | Therapeutic Category | Refs | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Drug Typical dose | (% CV or range) {unbound} | Fun | EC50/EC90 (μM) | Unbound Cmax/EC50 | EC50/EC90 (μM) | Unbound Cmax/EC50 | EC50/EC90 (μM) | unbound Cmax/EC50 | NA | |
| * VV116 300 mg bid | 10.6 (25%) {8.37} | --- | --- | 34 | --- | 105 | --- | 10.5 | NA | [89] |
| ** Molnupiravir (NHC) 800 mg bid | 8.99 (37%) {7.10} | 1 | 0.4/1.8 | 22 | 1.7/12.2 | 5.3 | 0.6/1.4 | 4.58 | NA | [17] |
| * Obeldesivir 350 mg bid | 7.33 (32%) {5.79} | --- | --- | 19 | --- | 72 | --- | 7.2 | NA | [28] |
| GS-441524 750 mg/d | 3.05 (23%) {2.41} | 0.79 | 0.3/2.34 | 8.03 | 0.08/1.4 | 30 | 0.8/1.4 | 3.0 | NA | [90,91] |
| Remdesivir 200 mg d1, 100 mg qd | 3.70 (19%) {0.44} | 0.12 | 0.2/0.7 | 2.2 | 0.02/0.1 | 22 | 3.2/4.7 | 0.14 | NA | [10] |
| Nirmatrelvir 300 mg + 100 mg ritonavir bid. | 6.86 (33%) {2.13} | 0.31 | 1.8/8.8 | 0.4 | 0.1/0.3 | 6.8 | 3.7/5.6 | 0.21 | NNAV | [92] |
| Nitazoxanide | 1.4 (19%) {0.014} | 0.01 | 22.8/42.9 | 0.015 | 4.4/11.1 | 0.078 | 1.4/3.9 | 0.25 | APA | [93,94] |
| Ivermectin 390–470 μg/kg qd | 0.30 (66%) {0.28} | 0.07 | 6.2/9.3 | 0.003 | 4.5/8.9 | 0.005 | 2.1/4.5 | 0.010 | APA | [71,95,96,97] |
| Imatinib 400 mg qd | 5.17 (30.3%) {0.26} | 0.05 | 77.9/95.8 | 0.003 | 37.9/88 | 0.006 | 4.6/14.5 | 0.056 | ONC | [98] |
|
Apilimod mesylate 150 mg qd | 0.54 {0.043} | 0.08 | >100/NE | NE | 85/>100 | 0.0005 | 0.7/7.4 | * 0.062 | ILi | [99,100] |
| Celecoxib 200 mg bid | 1.85 (38%) {0.056} | 0.03 | 3.0/6.3 | 0.019 | 0.7/1.2 | 0.08 | 7.2/14.6 | 0.008 | NSAID | [101] |
| Zileuton 600 m qd | 2.29 {0.16} | 0.07 | >100/NE | NE | >100 | 0.003 | 6.7/35.8 | 0.02 | LM | [102] |
| Daclatasvir 60 mg qd | 1.91 (13%) {0.02} | 0.01 | >100/NE | NE | 44.7/89.4 | 0.0005 | 0.7/3.5 | 0.03 | NNAV | [103] |
| Fenofibrate 200 mg qd (micronized form) | 28.36 (19%) {0.28} | 0.01 | >100/NE | NE | >100/NE | NE | 42.7/88.7 | 0.007 | LL | [104] |
| Ebselen 800 mg qd | 0.256 (47%) {0.013} | 0.05 | 6.5/>10 | 0.002 | >100/NE | NE | 1.1/2.7 | 0.012 | AO | [105] |
| Favipiravir | 411 (45%) {193} | 0.46 | >300/NE | NE | 256/>300 | 0.74 | 90.6/234.1 | 2.1 | NA | [85] |
| Fluvoxamine (maleate) 100 mg qd | 0.039 (0.02–0.06) {0.003} | 0.23 | >100/NE | 0.005 | 17.9/47.5 | 0.0017 | >100/NE | NE | SSUi | [106,107] |
|
Honokiol not approved | NE | 0.36 | 69.2/94.0 | 69.2/94 | 9.6/80.4 | NE | 20.1/84 | NE | NP | [108] |
| Iota-Carrageenan (topical) | --- | --- | 0.5/1.9 | --- | 59.2/93.3 | --- | 0.7/1.6 | --- | DS | |
| Mefenamic acid 500 mg day 1, 250 mg qid | 15.83 (11–22) {1.58} | 0.1 | > 100/NE | NE | >100/NE | NE | 87.6/>100 | 0.018 | NSA | [109,110] |
3. Results
4. Discussion
4.1. Relevance of Cell Lines and SARS-CoV-2 Variants
4.2. Potent Antivirals: Unbound Cmax/EC50 Ratios > 1 in Calu-3, Caco-2, and Vero CCL-81 Cells
4.3. Drugs with Moderate Unbound Cmax/EC50 Ratios in Calu-3 and/or Caco-2, and Vero CCL-81 Cells
4.4. Drugs with Measurable EC50 in Caco-2 Cells and EC50 > 100 μM in Calu-3 and Vero CCL-81 Cells
4.5. Drugs with Measurable Unbound Cmax/EC50 Ratios in Vero Cells Only
4.6. Drugs with EC50 > 100 μM in Calu-3, Caco-2, and Vero CCL-81 Cells
4.7. Drugs with EC50 < 100 μM in Vero-CCL-81, Calu-3, and Caco-2 Cells but without Published Human PK Data
4.8. Compounds for Intranasal Administration to Protect against SARS-CoV-2 Infection
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Bid | twice per day |
| Cmax | peak concentration of drug observed in plasma |
| CC50 | drug concentration that inhibits cell division by 50% in vitro |
| DMEM | Dulbecco’s Modified Eagle Medium |
| EC50/EC90 | median/90th percentile effective antiviral concentration measured in cell culture |
| FBS | fetal bovine serum |
| FDA | US Federal Drug administration |
| Fun | unbound fraction of drug in plasma |
| H | Hour |
| LC-MS-MS | chemical analysis which couples liquid chromatography with mass spectrometry |
| MEM | Minimum Essential Media |
| MOI | multiplicity of infection (MOI) |
| MTS | 3-(4,5-Dimethylthiazol-2-yl)-5-(3-carboxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium |
| NA | nucleoside analog |
| NE | not estimated |
| NIH | US National Institutes of Health |
| PD | Pharmacodynamics |
| PK | pharmacokinetics |
| Qd | once per day |
| t1/2 | elimination half-life |
| Tid | three times per day |
| qRT-PCR | quantitative real-time PCR |
| RPMI | Roswell Park Memorial Institute 1640 Media |
| unbound Cmax/EC50 | ratio of Cmax/EC50 normalized for protein binding. |
References
- U.S. Centers for Disease Control and Prevention. Overview of COVID-19 Vaccines. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/overview-COVID-19-vaccines.html (accessed on 28 November 2023).
- Yap, C.; Ali, A.; Prabhakar, A.; Prabhakar, A.; Pal, A.; Lim, Y.Y.; Kakodkar, P. Comprehensive literature review on COVID-19 vaccines and role of SARS-CoV-2 variants in the pandemic. Ther. Adv. Vaccines Immunother. 2021, 9, 25151355211059791. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.J.; Chan, K.H.; Hung, I.F. Safety and efficacy of COVID-19 vaccines: A systematic review and meta-analysis of different vaccines at phase 3. Vaccines 2021, 9, 989. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, A.; Narwal, M.; Majowicz, S.A.; Varricchio, C.; Toner, S.A.; Ballatore, C.; Brancale, A.; Murakami, K.S.; Jose, J. Identification of SARS-CoV-2 inhibitors targeting Mpro and PLpro using in-cell-protease assay. Commun. Biol. 2022, 5, 169. [Google Scholar] [CrossRef]
- Malin, J.J.; Suarez, I.; Priesner, V.; Fatkenheuer, G.; Rybniker, J. Remdesivir against COVID-19 and other viral diseases. Clin. Microbiol. Rev. 2020, 34, e00162-20. [Google Scholar] [CrossRef] [PubMed]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Chokkalingam, A.P.; Hayden, J.; Goldman, J.D.; Li, H.; Asubonteng, J.; Mozaffari, E.; Bush, C.; Wang, J.R.; Kong, A.; Osinusi, A.O.; et al. Association of remdesivir treatment with mortality among hospitalized adults with COVID-19 in the United States. JAMA Netw. Open 2022, 5, e2244505. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari, E.; Chandak, A.; Zhang, Z.; Liang, S.; Thrun, M.; Gottlieb, R.L.; Kuritzkes, D.R.; Sax, P.E.; Wohl, D.A.; Casciano, R.; et al. Remdesivir treatment in hospitalized patients with coronavirus disease 2019 (COVID-19): A comparative analysis of in-hospital all-cause mortality in a large multicenter observational cohort. Clin. Infect. Dis. 2022, 75, e450–e458. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early remdesivir to prevent progression to severe COVID-19 in outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Gilead Sciences, Inc. VEKLURY® (Remdesivir) for Injection, for Intravenous Use: Highlights of Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/214787Orig1s015lbl.pdf (accessed on 18 December 2022).
- U.S. National Institutes of Health. COVID-19 Treatment Guidelines. Remdesivir. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/antivirals-including-antibody-products/remdesivir/ (accessed on 29 February 2024).
- Pfizer Inc. FDA Advisory Committee Votes in Support of Favorable Benefit-Risk Profile for Pfizer’s Paxlovid™. Available online: https://www.pfizer.com/news/press-release/press-release-detail/fda-advisory-committee-votes-support-favorable-benefit-risk (accessed on 28 March 2023).
- Parums, D.V. Editorial: Current status of oral antiviral drug treatments for SARS-CoV-2 infection in non-hospitalized patients. Med. Sci. Monit. 2022, 28, e935952. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. COVID-19 Treatment Guidelines—Ritonavir -Boosted Nirmatrelvir. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/antivirals-including-antibody-products/ritonavir-boosted-nirmatrelvir--paxlovid-/ (accessed on 5 April 2024).
- Pfizer Inc. Pfizer Announces Additional Phase 2/3 Study Results Confirming Robust Efficacy of Novel COVID-19 Oral Antiviral Treatment Candidate in Reducing Risk of Hospitalization or Death. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-additional-phase-23-study-results (accessed on 15 December 2021).
- U.S. Centers for Disease Control and Prevention. Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19: Information for Healthcare Professionals. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingconditions.html (accessed on 28 November 2023).
- Merck & Co. Inc. Fact Sheet for Healthcare Providers: Emergency Use Authorization for Lagevrio™ (Molnupiravir) Capsules. Available online: https://www.merck.com/eua/molnupiravir-hcp-fact-sheet.pdf (accessed on 6 March 2023).
- Stuyver, L.J.; Whitaker, T.; McBrayer, T.R.; Hernandez-Santiago, B.I.; Lostia, S.; Tharnish, P.M.; Ramesh, M.; Chu, C.K.; Jordan, R.; Shi, J.; et al. Ribonucleoside analogue that blocks replication of bovine viral diarrhea and hepatitis C viruses in culture. Antimicrob. Agents Chemother. 2003, 47, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Hollecker, L.; Choo, H.; Chong, Y.; Chu, C.K.; Lostia, S.; McBrayer, T.R.; Stuyver, L.J.; Mason, J.C.; Du, J.; Rachakonda, S.; et al. Synthesis of beta-enantiomers of N4-hydroxy-3′-deoxypyrimidine nucleosides and their evaluation against bovine viral diarrhoea virus and hepatitis C virus in cell culture. Antivir. Chem. Chemother. 2004, 15, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Costantini, V.P.; Whitaker, T.; Barclay, L.; Lee, D.; McBrayer, T.R.; Schinazi, R.F.; Vinjé, J. Antiviral activity of nucleoside analogues against norovirus. Antivir. Ther. 2012, 17, 981–991. [Google Scholar] [CrossRef] [PubMed]
- Ehteshami, M.; Tao, S.; Zandi, K.; Hsiao, H.M.; Jiang, Y.; Hammond, E.; Amblard, F.; Russell, O.O.; Merits, A.; Schinazi, R.F. Characterization of β-d-N(4)-hydroxycytidine as a novel inhibitor of Chikungunya virus. Antimicrob. Agents Chemother. 2017, 61, e02395-16. [Google Scholar] [CrossRef] [PubMed]
- Painter, G.R.; Natchus, M.G.; Cohen, O.; Holman, W.; Painter, W.P. Developing a direct acting, orally available antiviral agent in a pandemic: The evolution of molnupiravir as a potential treatment for COVID-19. Curr. Opin. Virol. 2021, 50, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Swanstrom, R.; Schinazi, R.F. Lethal mutagenesis as an antiviral strategy. Science 2022, 375, 497–498. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Hill, C.S.; Sarkar, S.; Tse, L.V.; Woodburn, B.M.D.; Schinazi, R.F.; Sheahan, T.P.; Baric, R.S.; Heise, M.T.; Swanstrom, R. β-d-N4-hydroxycytidine inhibits SARS-CoV-2 through lethal mutagenesis but is also mutagenic to mammalian cells. J. Infect. Dis. 2021, 224, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Troth, S.; Butterton, J.; DeAnda, C.S.; Escobar, P.; Grobler, J.; Hazuda, D.; Painter, G. Letter to the editor in response to zhou et al. J. Infect. Dis. 2021, 224, 1442–1443. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Institutes of Health. COVID-19 Treatment Guidelines—Molnupiravir. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/antivirals-including-antibody-products/molnupiravir/ (accessed on 26 June 2023).
- Mackman, R.L.; Kalla, R.; Babusis, D.; Pitts, J.; Barrett, K.T.; Chun, K.; Pont, V.D.; Rodriguez, L.; Moshiri, J.; Xu, Y.; et al. Discovery of GS-5245 (Obeldesivir), an oral prodrug of nucleoside GS-441524 that exhibits antiviral efficacy in SARS-CoV-2 infected african green monkeys. J. Med. Chem. 2023, 66, 11701–11717. [Google Scholar] [CrossRef] [PubMed]
- Anoshchenko, O.; Abdelghany, M.; Hyland, R.H.; Davies, S.; Mkay, C.; Shen, G.; Xiao, D.; Winter, H.; Llewellyn, J.; Humeniuk, R. Pharmacokinetics, safety, and tolerability of obeldesivir (OBV; GS-5245) in healthy participants. Poster # P260 Presented at the 33rd European Congress of Clinical Microbiology and Infectious Diseases (ECCMID), 15–18 April 2023. Available online: https://www.natap.org/2023/HIV/092523_03.htm (accessed on 5 April 2024).
- Stevens, L.J.; Pruijssers, A.J.; Lee, H.W.; Gordon, C.J.; Tchesnokov, E.P.; Gribble, J.; George, A.S.; Hughes, T.M.; Lu, X.; Li, J.; et al. Mutations in the SARS-CoV-2 RNA-dependent RNA polymerase confer resistance to remdesivir by distinct mechanisms. Sci. Transl. Med. 2022, 14, eabo0718. [Google Scholar] [CrossRef] [PubMed]
- Costacurta, F.; Dodaro, A.; Bante, D.; Schöppe, H.; Sprenger, B.; Moghadasi, S.A.; Fleischmann, J.; Pavan, M.; Bassani, D.; Menin, S.; et al. A comprehensive study of SARS-CoV-2 main protease (M(pro)) inhibitor-resistant mutants selected in a VSV-based system. bioRxiv 2023. [Google Scholar] [CrossRef]
- Gandhi, S.; Klein, J.; Robertson, A.J.; Peña-Hernández, M.A.; Lin, M.J.; Roychoudhury, P.; Lu, P.; Fournier, J.; Ferguson, D.; Mohamed Bakhash, S.A.K.; et al. De novo emergence of a remdesivir resistance mutation during treatment of persistent SARS-CoV-2 infection in an immunocompromised patient: A case report. Nat. Commun. 2022, 13, 1547. [Google Scholar] [CrossRef] [PubMed]
- Focosi, D.; Maggi, F.; McConnell, S.; Casadevall, A. Very low levels of remdesivir resistance in SARS-COV-2 genomes after 18 months of massive usage during the COVID19 pandemic: A GISAID exploratory analysis. Antivir. Res. 2022, 198, 105247. [Google Scholar] [CrossRef] [PubMed]
- Ip, J.D.; Wing-Ho Chu, A.; Chan, W.M.; Cheuk-Ying Leung, R.; Umer Abdullah, S.M.; Sun, Y.; Kai-Wang To, K. Global prevalence of SARS-CoV-2 3CL protease mutations associated with nirmatrelvir or ensitrelvir resistance. EBioMedicine 2023, 91, 104559. [Google Scholar] [CrossRef] [PubMed]
- Strizki, J.M.; Gaspar, J.M.; Howe, J.A.; Hutchins, B.; Mohri, H.; Nair, M.S.; Kinek, K.C.; McKenna, P.; Goh, S.L.; Murgolo, N. Molnupiravir maintains antiviral activity against SARS-CoV-2 variants and exhibits a high barrier to the development of resistance. Antimicrob. Agents Chemother. 2024, 68, e0095323. [Google Scholar] [CrossRef]
- Sanderson, T.; Hisner, R.; Donovan-Banfield, I.; Hartman, H.; Løchen, A.; Peacock, T.P.; Ruis, C. A molnupiravir-associated mutational signature in global SARS-CoV-2 genomes. Nature 2023, 623, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Alavian, G.; Kolahdouzan, K.; Mortezazadeh, M.; Torabi, Z.S. Antiretrovirals for prophylaxis against COVID-19: A comprehensive literature review. J. Clin. Pharmacol. 2021, 61, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Grieb, P.; Swiatkiewicz, M.; Prus, K.; Rejdak, K. Amantadine for COVID-19. J. Clin. Pharmacol. 2021, 61, 412–413. [Google Scholar] [CrossRef] [PubMed]
- Sharun, K.; Tiwari, R.; Dhama, K. Protease inhibitor GC376 for COVID-19: Lessons learned from feline infectious peritonitis. Ann. Med. Surg. 2021, 61, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.K.; Chen, C.Y.; Chen, W.C.; Lai, C.C.; Hung, S.H.; Lin, W.T. The effect of sofosbuvir-based treatment on the clinical outcomes of patients with COVID-19: A systematic review and meta-analysis of randomized controlled trials. Int. J. Antimicrob. Agents 2022, 59, 106545. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Li, M.; Zhou, L.; Liu, D.; He, W.; Liang, W.; Sun, Q.; Sun, H.; Li, Y.; Liu, X. Ribavirin treatment for critically Ill COVID-19 patients: An observational study. Infect. Drug Resist. 2021, 14, 5287–5291. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group. Lopinavir-ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2020, 396, 1345–1352. [Google Scholar] [CrossRef] [PubMed]
- Aherfi, S.; Pradines, B.; Devaux, C.; Honore, S.; Colson, P.; Scola, B.; Raoult, D. Drug repurposing against SARS-CoV-1, SARS-CoV-2 and MERS-CoV. Future Microbiol. 2021, 16, 1341–1370. [Google Scholar] [CrossRef] [PubMed]
- Baghaki, S.; Yalcin, C.E.; Baghaki, H.S.; Aydin, S.Y.; Daghan, B.; Yavuz, E. COX2 inhibition in the treatment of COVID-19: Review of literature to propose repositioning of celecoxib for randomized controlled studies. Int. J. Infect. Dis. 2020, 101, 29–32. [Google Scholar] [CrossRef]
- Ghaznavi, H.; Mohammadghasemipour, Z.; Shirvaliloo, M.; Momeni, M.K.; Metanat, M.; Gorgani, F.; Abedipour, F.; Mohammadi, M.; Sartipi, M.; Khorashad, A.R.S.; et al. Short-term celecoxib (celebrex) adjuvant therapy: A clinical trial study on COVID-19 patients. Inflammopharmacology 2022, 30, 1645–1657. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, L.P.; Linhares, E.; Nogueira, F.G.O.; Moreira-Silva, D.; Medeiros-Lima, D.J.M. Perspectives on glucocorticoid treatment for COVID-19: A systematic review. Pharmacol. Rep. 2021, 73, 728–735. [Google Scholar] [CrossRef] [PubMed]
- GómezMoore, N.; Bosco-Levy, P.; Thurin, N.; Blin, P.; Droz-Perroteau, C. NSAIDs and COVID-19: A Systematic Review and Meta-analysis. Drug Saf. 2021, 44, 929–938. [Google Scholar] [CrossRef]
- Kelleni, M.T. NSAIDs/nitazoxanide/azithromycin repurposed for COVID-19: Potential mitigation of the cytokine storm interleukin-6 amplifier via immunomodulatory effects. Expert. Rev. Anti Infect. Ther. 2022, 20, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Vaja, R.; Chan, J.S.K.; Ferreira, P.; Harky, A.; Rogers, L.J.; Gashaw, H.H.; Kirkby, N.S.; Mitchell, J.A. The COVID-19 ibuprofen controversy: A systematic review of NSAIDs in adult acute lower respiratory tract infections. Br. J. Clin. Pharmacol. 2021, 87, 776–784. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administration. Coronavirus (COVID-19) Update: FDA Authorizes Drug for Treatment of COVID-19. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-drug-treatment-covid-19 (accessed on 24 February 2023).
- Chiu, L.; Shen, M.; Lo, C.H.; Chiu, N.; Chen, A.; Shin, H.J.; Prsic, E.H.; Hur, C.; Chow, R.; Lebwohl, B. Effect of famotidine on hospitalized patients with COVID-19: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0259514. [Google Scholar] [CrossRef] [PubMed]
- Hogan Ii, R.B.; Hogan Iii, R.B.; Cannon, T.; Rappai, M.; Studdard, J.; Paul, D.; Dooley, T.P. Dual-histamine receptor blockade with cetirizine—Famotidine reduces pulmonary symptoms in COVID-19 patients. Pulm. Pharmacol. Ther. 2020, 63, 101942. [Google Scholar] [CrossRef]
- Kerget, B.; Kerget, F.; Aydin, M.; Karasahin, O. Effect of montelukast therapy on clinical course, pulmonary function, and mortality in patients with COVID-19. J. Med. Virol. 2021, 94, 1950–1958. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Patel, D.; Bittel, B.; Wolski, K.; Wang, Q.; Kumar, A.; Il’Giovine, Z.J.; Mehra, R.; McWilliams, C.; Nissen, S.E.; et al. Effect of High-Dose Zinc and Ascorbic Acid Supplementation vs Usual Care on Symptom Length and Reduction Among Ambulatory Patients With SARS-CoV-2 Infection: The COVID A to Z Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e210369. [Google Scholar] [CrossRef] [PubMed]
- Sies, H.; Parnham, M.J. Potential therapeutic use of ebselen for COVID-19 and other respiratory viral infections. Free Radic. Biol. Med. 2020, 156, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Tolouian, R.; Mulla, Z.D.; Jamaati, H.; Babamahmoodi, A.; Marjani, M.; Eskandari, R.; Dastan, F. Effect of bromhexine in hospitalized patients with COVID-19. J. Investig. Med. 2021, 71, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Mikhaylov, E.N.; Lyubimtseva, T.A.; Vakhrushev, A.D.; Stepanov, D.; Lebedev, D.S.; Vasilieva, E.Y.; Konradi, A.O.; Shlyakhto, E.V. Bromhexine Hydrochloride Prophylaxis of COVID-19 for Medical Personnel: A Randomized Open-Label Study. Interdiscip. Perspect. Infect. Dis. 2022, 2022, 4693121. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.C.; Yu, L.M.; Dorward, J.; Gbinigie, O.; Hayward, G.; Saville, B.R.; Van Hecke, O.; Berry, N.; Detry, M.A.; Saunders, C.; et al. Doxycycline for community treatment of suspected COVID-19 in people at high risk of adverse outcomes in the UK (PRINCIPLE): A randomised, controlled, open-label, adaptive platform trial. Lancet Respir. Med. 2021, 9, 1010–1020. [Google Scholar] [CrossRef] [PubMed]
- Egiz, A.; Gala, D. Clofazimine: Another potential magic bullet for the treatment of COVID-19? Postgrad. Med. J. 2021, 98, e124. [Google Scholar] [CrossRef] [PubMed]
- Blum, V.F.; Cimerman, S.; Hunter, J.R.; Tierno, P.; Lacerda, A.; Soeiro, A.; Cardoso, F.; Bellei, N.C.; Maricato, J.; Mantovani, N.; et al. Nitazoxanide superiority to placebo to treat moderate COVID-19—A Pilot prove of concept randomized double-blind clinical trial. EClinicalMedicine 2021, 37, 100981. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.; Mirchandani, M.; Pilkington, V. Ivermectin for COVID-19: Addressing potential bias and medical fraud. Open Forum. Infect. Dis. 2022, 9, ofab645. [Google Scholar] [CrossRef] [PubMed]
- Izcovich, A.; Peiris, S.; Ragusa, M.; Tortosa, F.; Rada, G.; Aldighieri, S.; Reveiz, L. Bias as a source of inconsistency in ivermectin trials for COVID-19: A systematic review. Ivermectin’s suggested benefits are mainly based on potentially biased results. J. Clin. Epidemiol. 2021, 144, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Feher, M.; Joy, M.; Munro, N.; Hinton, W.; Williams, J.; de Lusignan, S. Fenofibrate as a COVID-19 modifying drug: Laboratory success versus real-world reality. Atherosclerosis 2021, 339, 55–56. [Google Scholar] [CrossRef]
- Aman, J.; Duijvelaar, E.; Botros, L.; Kianzad, A.; Schippers, J.R.; Smeele, P.J.; Azhang, S.; Bartelink, I.H.; Bayoumy, A.A.; Bet, P.M.; et al. Imatinib in patients with severe COVID-19: A randomised, double-blind, placebo-controlled, clinical trial. Lancet Respir. Med. 2021, 9, 957–968. [Google Scholar] [CrossRef] [PubMed]
- Roschewski, M.; Lionakis, M.S.; Sharman, J.P.; Roswarski, J.; Goy, A.; Monticelli, M.A.; Roshon, M.; Wrzesinski, S.H.; Desai, J.V.; Zarakas, M.A.; et al. Inhibition of bruton tyrosine kinase in patients with severe COVID-19. Sci. Immunol. 2020, 5, eabd0110. [Google Scholar] [CrossRef] [PubMed]
- Mas, M.; García-Vicente, J.A.; Estrada-Gelonch, A.; Pérez-Mañá, C.; Papaseit, E.; Torrens, M.; Farré, M. Antidepressant drugs and COVID-19: A review of basic and clinical evidence. J. Clin. Med. 2022, 11, 4038. [Google Scholar] [CrossRef]
- Bramante, C.T.; Ingraham, N.E.; Murray, T.A.; Marmor, S.; Hovertsen, S.; Gronski, J.; McNeil, C.; Feng, R.; Guzman, G.; Abdelwahab, N.; et al. Metformin and risk of mortality in patients hospitalised with COVID-19: A retrospective cohort analysis. Lancet Healthy Longev. 2021, 2, e34–e41. [Google Scholar] [CrossRef]
- Chirinos, J.A.; Lopez-Jaramillo, P.; Giamarellos-Bourboulis, E.J.; Dávila-Del-Carpio, G.H.; Bizri, A.R.; Andrade-Villanueva, J.F.; Salman, O.; Cure-Cure, C.; Rosado-Santander, N.R.; Cornejo Giraldo, M.P.; et al. A randomized clinical trial of lipid metabolism modulation with fenofibrate for acute coronavirus disease 2019. Nat. Metab. 2022, 4, 1847–1857. [Google Scholar] [CrossRef] [PubMed]
- Lan, S.H.; Lee, H.Z.; Chao, C.M.; Chang, S.P.; Lu, L.C.; Lai, C.C. Efficacy of melatonin in the treatment of patients with COVID-19: A systematic review and meta-analysis of randomized controlled trials. J. Med. Virol. 2022, 94, 2102–2107. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Zhang, L.; Xu, Y.; Yang, D.; Zhang, L.; Yang, S.; Zhang, W.; Wang, J.; Tian, S.; Yang, S.; et al. The comprehensive study on the therapeutic effects of baicalein for the treatment of COVID-19 in vivo and in vitro. Biochem. Pharmacol. 2021, 183, 114302. [Google Scholar] [CrossRef] [PubMed]
- Hemila, H.; Chalker, E. Carrageenan nasal spray may double the rate of recovery from coronavirus and influenza virus infections: Re-analysis of randomized trial data. Pharmacol. Res. Perspect. 2021, 9, e00810. [Google Scholar] [CrossRef] [PubMed]
- Peña-Silva, R.; Duffull, S.B.; Steer, A.C.; Jaramillo-Rincon, S.X.; Gwee, A.; Zhu, X. Pharmacokinetic considerations on the repurposing of ivermectin for treatment of COVID-19. Br. J. Clin. Pharmacol. 2021, 87, 1589–1590. [Google Scholar] [CrossRef] [PubMed]
- LeCher, J.C.; Zandi, K.; Costa, V.V.; Amblard, F.; Tao, S.; Patel, D.; Lee, S.; da Silva Santos, F.R.; Goncalves, M.R.; Queroz-Junior, C.M.; et al. Discovery of a 2′-Fluoro,2′-bromouridine phosphoramidate prodrug exhibiting anti-yellow fever virus activity in culture and in mice. Microorganisms 2022, 10, 2098. [Google Scholar] [CrossRef] [PubMed]
- Zandi, K.; Musall, K.; Oo, A.; Cao, D.; Liang, B.; Hassandarvish, P.; Lan, S.; Slack, R.L.; Kirby, K.A.; Bassit, L.; et al. Baicalein and baicalin inhibit SARS-CoV-2 RNA-dependent-RNA polymerase. Microorganisms 2021, 9, 893. [Google Scholar] [CrossRef] [PubMed]
- American Type Culture Collection (ATCC). Vero CCL-81™. Available online: https://www.atcc.org/products/ccl-81 (accessed on 18 December 2022).
- American Type Culture Collection (ATCC). Caco-2 HTB-37™. Available online: https://www.atcc.org/products/htb-37 (accessed on 18 December 2022).
- American Type Culture Collection (ATCC). Calu-3 HTB-55™. Available online: https://www.atcc.org/products/htb-55 (accessed on 18 December 2022).
- JCRB Cell Bank. JCRB0403 HuH-7. Available online: https://cellbank.nibiohn.go.jp/~cellbank/en/search_res_det.cgi?RNO=jcrb0403 (accessed on 18 December 2022).
- Patil, S.; Kamath, S.; Sanchez, T.; Neamati, N.; Schinazi, R.F.; Buolamwini, J.K. Synthesis and biological evaluation of novel 5(H)-phenanthridin-6-ones, 5(H)-phenanthridin-6-one diketo acid, and polycyclic aromatic diketo acid analogs as new HIV-1 integrase inhibitors. Bioorg. Med. Chem. 2007, 15, 1212–1228. [Google Scholar] [CrossRef] [PubMed]
- Chou, T.C.; Talalay, P. Quantitative analysis of dose-effect relationships: The combined effects of multiple drugs or enzyme inhibitors. Adv. Enzym. Regul. 1984, 22, 27–55. [Google Scholar] [CrossRef] [PubMed]
- Zandi, K.; Amblard, F.; Musall, K.; Downs-Bowen, J.; Kleinbard, R.; Oo, A.; Cao, D.; Liang, B.; Russell, O.O.; McBrayer, T.; et al. Repurposi[Singh, 2011 #363]ng nucleoside analogs for human coronaviruses. Antimicrob. Agents Chemother. 2020, 65, e01652-20. [Google Scholar] [CrossRef] [PubMed]
- Gilead Sciences Inc. Sofosbuvir and Velpatasvir Tablets. Highlights of Prescribing Information. Available online: https://www.asegua.com/~/media/Files/pdfs/medicines/liver-disease/asegua/asegua_sof_vel_pi.pdf (accessed on 18 December 2022).
- Gilead Sciences. DESCOVY® (Emtricitabine and Tenofovir Alafenamide) Tablets. Highlights of Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/208215s012lbl.pdf (accessed on 18 December 2022).
- Gilead Sciences. TRUVADA® (Emtricitabine and Tenofovir Disoproxil Fumarate). Highlights of Prescribing Information. Available online: https://www.gilead.com/~/media/files/pdfs/medicines/hiv/truvada/truvada_pi.pdf (accessed on 18 December 2022).
- Axelrod, F.B.; Liebes, L.; Gold-Von Simson, G.; Mendoza, S.; Mull, J.; Leyne, M.; Norcliffe-Kaufmann, L.; Kaufmann, H.; Slaugenhaupt, S.A. Kinetin improves IKBKAP mRNA splicing in patients with familial dysautonomia. Pediatr. Res. 2011, 70, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Taisho Toyama Pharmaceutical Co., Ltd. AVIGAN Tablets (290 mg Favipiravir). Available online: https://www.cdc.gov.tw/File/Get/ht8jUiB_MI-aKnlwstwzvw (accessed on 18 December 2022).
- Hashemian, S.M.; Farhadi, T.; Velayati, A.A. A review on favipiravir: The properties, function, and usefulness to treat COVID-19. Expert. Rev. Anti Infect. Ther. 2021, 19, 1029–1037. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, R.; Esaki, T.; Kawashima, H.; Natsume-Kitatani, Y.; Nagao, C.; Ohashi, R.; Mizuguchi, K. Predicting fraction unbound in human plasma from chemical structure: Improved accuracy in the low value ranges. Mol. Pharm. 2018, 15, 5302–5311. [Google Scholar] [CrossRef] [PubMed]
- Zeitlinger, M.A.; Derendorf, H.; Mouton, J.W.; Cars, O.; Craig, W.A.; Andes, D.; Theuretzbacher, U. Protein binding: Do we ever learn? Antimicrob. Agents Chemother. 2011, 55, 3067–3074. [Google Scholar] [CrossRef] [PubMed]
- Qian, H.J.; Wang, Y.; Zhang, M.Q.; Xie, Y.C.; Wu, Q.Q.; Liang, L.Y.; Cao, Y.; Duan, H.Q.; Tian, G.H.; Ma, J.; et al. Safety, tolerability, and pharmacokinetics of VV116, an oral nucleoside analog against SARS-CoV-2, in Chinese healthy subjects. Acta Pharmacol. Sin. 2022, 43, 3130–3138. [Google Scholar] [CrossRef] [PubMed]
- Yan, V. First-in-Woman safety, tolerability, and pharmacokinetics of orally administered GS-441524: A broad-spectrum antiviral treatment for COVID-19. In OSF Preprints; Center for Open Science: Charlottesville, VA, USA, 2021. [Google Scholar]
- Tao, S.; Zandi, K.; Bassit, L.; Ong, Y.T.; Verma, K.; Liu, P.; Downs-Bowen, J.A.; McBrayer, T.; LeCher, J.C.; Kohler, J.J.; et al. Comparison of anti-SARS-CoV-2 activity and intracellular metabolism of remdesivir and its parent nucleoside. Curr. Res. Pharmacol. Drug Discov. 2021, 2, 100045. [Google Scholar] [CrossRef] [PubMed]
- Pfizer Inc. Highlights of Prescribing Information Paxlovid™. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217188s000lbl.pdf (accessed on 3 November 2023).
- Romark Laboratories, L.C. Alinia® (Nitazoxanide) Tablets. (Nitazoxanide) for Oral Suspension. Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2005/021818lbl.pdf (accessed on 18 December 2022).
- Singh, N.; Narayan, S. Nitazoxanide: A broad spectrum antimicrobial. Med. J. Armed. Forces India 2011, 67, 67–68. [Google Scholar] [CrossRef] [PubMed]
- Guzzo, C.A.; Furtek, C.I.; Porras, A.G.; Chen, C.; Tipping, R.; Clineschmidt, C.M.; Sciberras, D.G.; Hsieh, J.Y.-K.; Lasseter, K.C. Safety, tolerability, and pharmacokinetics of escalating high doses of ivermectin in healthy adult subjects. J. Clin. Pharmacol. 2002, 42, 1122–1133. [Google Scholar] [CrossRef]
- Buonfrate, D.; Chesini, F.; Martini, D.; Roncaglioni, M.C.; Fernandez, M.L.O.; Alvisi, M.F.; De Simone, I.; Rulli, E.; Nobili, A.; Casalini, G.; et al. High-dose ivermectin for early treatment of COVID-19 (COVER study): A randomised, double-blind, multicentre, phase II, dose-finding, proof-of-concept clinical trial. Int. J. Antimicrob. Agents 2022, 59, 106516. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, J.; Ballester, M.R.; Antonijoan, R.M.; Gich, I.; Rodríguez, M.; Colli, E.; Gold, S.; Krolewiecki, A.J. Safety and pharmacokinetic profile of fixed-dose ivermectin with an innovative 18mg tablet in healthy adult volunteers. PLoS Negl. Trop. Dis. 2018, 12, e0006020. [Google Scholar] [CrossRef] [PubMed]
- Peng, B.; Lloyd, P.; Schran, H. Clinical pharmacokinetics of imatinib. Clin. Pharmacokinet. 2005, 44, 879–894. [Google Scholar] [CrossRef] [PubMed]
- Harb, W.A.; Diefenbach, C.S.; Lakhani, N.; Rutherford, S.C.; Schreeder, M.T.; Ansell, S.M.; Sher, T.; Aboulafia, D.M.; Cohen, J.B.; Nix, D.; et al. Phase 1 clinical safety, pharmacokinetics (PK), and activity of apilimod dimesylate (LAM-002A), a first-in-class inhibitor of phosphatidylinositol-3-phosphate 5-kinase (PIKfyve), in ratients with relapsed or refractory B-cell malignancies. Blood 2017, 130, 4119. [Google Scholar]
- Ikonomov, O.C.; Sbrissa, D.; Shisheva, A. Small molecule PIKfyve inhibitors as cancer therapeutics: Translational promises and limitations. Toxicol. Appl. Pharmacol. 2019, 383, 114771. [Google Scholar] [CrossRef] [PubMed]
- G.D. Searle LLC. CELEBREX® (Celecoxib) Capsules Drug Safety Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2005/020998s017lbl.pdf (accessed on 18 December 2022).
- Abbott Laboratories, Inc. ZYFLO® (Zileuton Tablets) Drug Safety Data (Reference ID: 314232). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020471s017lbl.pdf (accessed on 18 December 2022).
- Gandhi, Y.; Eley, T.; Fura, A.; Li, W.; Bertz, R.J.; Garimella, T. Daclatasvir: A Review of Preclinical and Clinical Pharmacokinetics. Clin. Pharmacokinet. 2018, 57, 911–928. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.B.; Spence, J.D. Clinical pharmacokinetics of fibric acid derivatives (fibrates). Clin. Pharmacokinet. 1998, 34, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Kil, J.; Harruff, E.E.; Longenecker, R.J. Development of ebselen for the treatment of sensorineural hearing loss and tinnitus. Hear. Res. 2022, 413, 108209. [Google Scholar] [CrossRef] [PubMed]
- Jazz Pharmaceuticals Inc. LUVOX® (Fluvoxamine Maleate) Tablets 25 mg, 50 mg and 100 mg. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2007/021519lbl.pdf (accessed on 18 December 2022).
- Perucca, E.; Gatti, G.; Spina, E. Clinical pharmacokinetics of fluvoxamine. Clin. Pharmacokinet. 1994, 27, 175–190. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.H.; Cai, L.L.; Zhang, X.Y.; Deng, L.Y.; Zheng, H.; Deng, C.Y.; Wen, J.; Zhao, X.; Wei, Y.; Chen, L. Improved solubility and pharmacokinetics of PEGylated liposomal honokiol and human plasma protein binding ability of honokiol. Int. J. Pharm. 2011, 410, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Rawashdeh, N.M.; Najib, N.M.; Jalal, I.M. Comparative bioavailability of two capsule formulations of mefenamic acid. Int. J. Clin. Pharmacol. Ther. 1997, 35, 329–333. [Google Scholar] [PubMed]
- U.S. Food & Drug Administration. PONSTEL® (Mefenamic Acid Capsules, USP). Drug Safety Data. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2008/015034s040lbl.pdf (accessed on 18 December 2022).
- Warner Chilcott (US) Ltd. DORYX® (Doxycycline Hyclate) Delayed-Release Tablets, 75 mg, 100 mg and 150 mg for Oral Use. Highlights of Prescribing information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2008/050795s005lbl.pdf (accessed on 14 November 2023).
- Alghamdi, W.A.; Al-Shaer, M.H.; Kipiani, M.; Barbakadze, K.; Mikiashvili, L.; Kempker, R.R.; Peloquin, C.A. Pharmacokinetics of bedaquiline, delamanid and clofazimine in patients with multidrug-resistant tuberculosis. J. Antimicrob. Chemother. 2021, 76, 1019–1024. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration. NDA Application 022519Orig1s000. Duexis (Ibuprofen/Famotidine). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2011/022519Orig1s000ClinPharmR.pdf (accessed on 18 December 2022).
- Pathirana, S.; Jayawardena, S.; Meeves, S.; Thompson, G.A. Brompheniramine and chlorpheniramine pharmacokinetics following single-dose oral administration in children aged 2 to 17 years. J. Clin. Pharmacol. 2018, 58, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Toutain, C.E.; Seewald, W.; Jung, M. The intravenous and oral pharmacokinetics of lotilaner in dogs. Parasit. Vectors 2017, 10, 522. [Google Scholar] [CrossRef] [PubMed]
- Nycomed GmbH. ALVESCO® (Ciclesonide) Inhalation Aerosol 80 mcg, Highlights of Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/021658s006lbl.pdf (accessed on 18 December 2022).
- Merck & Co. Inc. SINGULAIR® (Montelukast Sodium) Drug Safety Data. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020829s051_020830s052_021409s028lbl.pdf (accessed on 16 December 2022).
- Zhang, W.; Feng, F.; Wang, Y. Bioequivalence study of bromhexine by liquid chromatography-electrospray ionization-mass spectrometry after oral administration of bromhexine hydrochloride tablets. J. Pharm. Biomed. Anal. 2008, 48, 1206–1210. [Google Scholar] [CrossRef] [PubMed]
- Merck & Co. Inc. ZEPATIER® (Elbasvir and Grazoprevir) Tablets Highlighrs of Prescribing Information. Available online: https://www.merck.com/product/usa/pi_circulars/z/zepatier/zepatier_pi.pdf (accessed on 18 December 2022).
- deVries, T.; Dentiste, A.; Handiwala, L.; Jacobs, D. Bioavailability and pharmacokinetics of once-daily amantadine extended-release tablets in healthy volunteers: Results from three randomized, crossover, open-Label, Phase 1 studies. Neurol. Ther. 2019, 8, 449–460. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Liu, H.; Galasiti Kankanamalage, A.C.; Weerasekara, S.; Hua, D.H.; Groutas, W.C.; Chang, K.-O.; Pedersen, N.C. Reversal of the progression of fatal coronavirus infection in cats by a broad-spectrum coronavirus protease inhibitor. PLoS Pathog. 2016, 12, e1005531. [Google Scholar]
- Schwope, D.M.; Karschner, E.L.; Gorelick, D.A.; Huestis, M.A. Identification of recent cannabis use: Whole-blood and plasma free and glucuronidated cannabinoid pharmacokinetics following controlled smoked cannabis administration. Clin. Chem. 2011, 57, 1406–1414. [Google Scholar] [CrossRef] [PubMed]
- Harpsøe, N.G.; Andersen, L.P.; Gögenur, I.; Rosenberg, J. Clinical pharmacokinetics of melatonin: A systematic review. Eur. J. Clin. Pharmacol. 2015, 71, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.K.; Vyas, K.H.; Brandt, K.D. In vitro protein binding of diclofenac sodium in plasma and synovial fluid. J. Pharm. Sci 1987, 76, 105–108. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administration. Diclofenac Potassium Powder for Oral Solution. Clinical Pharmacology Review. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/022165s000ClinPharmR.pdf (accessed on 14 November 2023).
- Ramaswamy, B.; Phelps, M.A.; Baiocchi, R.; Bekaii-Saab, T.; Ni, W.; Lai, J.P.; Wolfson, A.; Lustberg, M.E.; Wei, L.; Wilkins, D.; et al. A dose-finding, pharmacokinetic and pharmacodynamic study of a novel schedule of flavopiridol in patients with advanced solid tumors. Investig. New Drugs 2012, 30, 629–638. [Google Scholar] [CrossRef] [PubMed]
- AstraZeneca Pharmaceuticals LP. CALQUENCE® (Acalabrutinib) Capsules, for Oral Use. Highlights of Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/210259s000lbl.pdf (accessed on 22 November 2023).
- Low, Z.Y.; Yip, A.J.W.; Lal, S.K. Repositioning ivermectin for COVID-19 treatment: Molecular mechanisms of action against SARS-CoV-2 replication. Biochim. Biophys. Acta Mol. Basis Dis. 2022, 1868, 166294. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Lee, J.S.; Ju, Y.S. Experimental models for SARS-CoV-2 infection. Mol Cells 2021, 44, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Mosbauer, K.; Hofmann-Winkler, H.; Kaul, A.; Kleine-Weber, H.; Kruger, N.; Gassen, N.C.; Muller, M.A.; Drosten, C.; Pohlmann, S. Chloroquine does not inhibit infection of human lung cells with SARS-CoV-2. Nature 2020, 585, 588–590. [Google Scholar] [CrossRef] [PubMed]
- Ou, T.; Mou, H.; Zhang, L.; Ojha, A.; Choe, H.; Farzan, M. Hydroxychloroquine-mediated inhibition of SARS-CoV-2 entry is attenuated by TMPRSS2. PLoS Pathog. 2021, 17, e1009212. [Google Scholar] [CrossRef] [PubMed]
- Gavriatopoulou, M.; Korompoki, E.; Fotiou, D.; Ntanasis-Stathopoulos, I.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Organ-specific manifestations of COVID-19 infection. Clin. Exp. Med. 2020, 20, 493–506. [Google Scholar] [CrossRef]
- Jockusch, S.; Tao, C.; Li, X.; Chien, M.; Kumar, S.; Morozova, I.; Kalachikov, S.; Russo, J.J.; Ju, J. Sofosbuvir terminated RNA is more resistant to SARS-CoV-2 proofreader than RNA terminated by Remdesivir. Sci. Rep. 2020, 10, 16577. [Google Scholar] [CrossRef] [PubMed]
- Baddock, H.T.; Brolih, S.; Yosaatmadja, Y.; Ratnaweera, M.; Bielinski, M.; Swift, L.P.; Cruz-Migoni, A.; Fan, H.; Keown, J.R.; Walker, A.P.; et al. Characterization of the SARS-CoV-2 ExoN (nsp14ExoN-nsp10) complex: Implications for its role in viral genome stability and inhibitor identification. Nucleic Acids Res. 2022, 50, 1484–1500. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.J.; Chang, L.; Yang, Y.; Wang, X.; Xie, Y.C.; Shen, J.S.; Tan, B.; Liu, J. Pharmacokinetics and tissue distribution of remdesivir and its metabolites nucleotide monophosphate, nucleotide triphosphate, and nucleoside in mice. Acta Pharmacol. Sin. 2021, 42, 1195–1200. [Google Scholar] [CrossRef]
- Pond, S.M.; Tozer, T.N. First-pass elimination. Basic concepts and clinical consequences. Clin. Pharmacokinet. 1984, 9, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, S.J.; Schinazi, R.F. Practical considerations for developing nucleoside reverse transcriptase inhibitors. Drug Discov. Today Technol. 2012, 9, e183–e193. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, S.J.; Schinazi, R.F. Prodrug strategies for improved efficacy of nucleoside antiviral inhibitors. Curr. Opin HIV AIDS 2013, 8, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, H.B.; Jürgens, G.; Thomsen, R.; Taboureau, O.; Zeth, K.; Hansen, P.E.; Hansen, P.R. Cellular uptake and Intracellular phosphorylation of GS-441524: Implications for Its effectiveness against COVID-19. Viruses 2021, 13, 1369. [Google Scholar] [CrossRef] [PubMed]
- Humeniuk, R.; Mathias, A.; Kirby, B.J.; Lutz, J.D.; Cao, H.; Osinusi, A.; Babusis, D.; Porter, D.; Wei, X.; Ling, J.; et al. Pharmacokinetic, pharmacodynamic, and drug-interaction profile of remdesivir, a SARS-CoV-2 replication inhibitor. Clin. Pharmacokinet. 2021, 60, 569–583. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Assessment Report. Procedure under Article 5(3) of Regulation (EC) No 726/2004. Use of Molnupiravir for the Treatment of COVID-19. Available online: https://www.ema.europa.eu/en/documents/referral/lagevrio-also-known-molnupiravir-mk-4482-covid-19-article-53-procedure-assessment-report_en.pdf (accessed on 16 December 2022).
- Mackman, R.L.; Hui, H.C.; Perron, M.; Murakami, E.; Palmiotti, C.; Lee, G.; Stray, K.; Zhang, L.; Goyal, B.; Chun, K.; et al. Prodrugs of a 1′-CN-4-Aza-7,9-dideazaadenosine C-nucleoside leading to the discovery of remdesivir (gs-5734) as a potent inhibitor of respiratory syncytial virus with efficacy in the african green monkey model of RSV. J. Med. Chem. 2021, 64, 5001–5017. [Google Scholar] [CrossRef] [PubMed]
- Jubalent Pharma Ltd. Jubilant Reveals Promising Safety, Absorption Data for Oral Form of COVID-19 Drug Remdesivir. Available online: https://www.clinicaltrialsarena.com/news/jubilant-oral-form-remdesivir/ (accessed on 12 March 2023).
- Xie, J.; Wang, Z. Can remdesivir and its parent nucleoside GS-441524 be potential oral drugs? An in vitro and in vivo DMPK assessment. Acta Pharm. Sin. B 2021, 11, 1607–1616. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, H.B.; Thomsen, R.; Hansen, P.R. Nucleoside analog GS-441524: Pharmacokinetics in different species, safety, and potential effectiveness against COVID-19. Pharmacol. Res. Perspect. 2022, 10, e00945. [Google Scholar] [CrossRef] [PubMed]
- Pruijssers, A.J.; George, A.S.; Schäfer, A.; Leist, S.R.; Gralinksi, L.E.; Dinnon, K.H., 3rd; Yount, B.L.; Agostini, M.L.; Stevens, L.J.; Chappell, J.D.; et al. Remdesivir inhibits SARS-CoV-2 in human lung cells and chimeric SARS-CoV expressing the SARS-CoV-2 RNA polymerase in mice. Cell Rep. 2020, 32, 107940. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Cao, L.; Li, G.; Cong, F.; Li, Y.; Sun, J.; Luo, Y.; Chen, G.; Li, G.; Wang, P.; et al. Remdesivir metabolite GS-441524 effectively Inhibits SARS-CoV-2 Infection in mouse models. J. Med. Chem. 2022, 65, 2785–2793. [Google Scholar] [CrossRef] [PubMed]
- Pitts, J.; Babusis, D.; Vermillion, M.S.; Subramanian, R.; Barrett, K.; Lye, D.; Ma, B.; Zhao, X.; Riola, N.; Xie, X.; et al. Intravenous delivery of GS-441524 is efficacious in the African green monkey model of SARS-CoV-2 infection. Antivir. Res. 2022, 203, 105329. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, S.J.; Asif, G.; Kivel, N.M.; Schinazi, R.F. Development of an optimized dose for coformulation of zidovudine with drugs that select for the K65R mutation using a population pharmacokinetic and enzyme kinetic simulation model. Antimicrob. Agents Chemother. 2008, 52, 4241–4250. [Google Scholar] [CrossRef] [PubMed]
- Schilling, W.H.K.; Jittamala, P.; Watson, J.A.; Ekkapongpisit, M.; Siripoon, T.; Ngamprasertchai, T.; Luvira, V.; Pongwilai, S.; Cruz, C.; Callery, J.J.; et al. Pharmacometrics of high-dose ivermectin in early COVID-19 from an open label, randomized, controlled adaptive platform trial (PLATCOV). Elife 2023, 12, e83201. [Google Scholar] [CrossRef]
- Hurwitz, S.J.; Schinazi, R.F. In silico study supports the efficacy of a reduced dose regimen for stavudine. Antivir. Res. 2011, 92, 372–377. [Google Scholar] [CrossRef]
- Owen, D.R.; Allerton, C.M.N.; Anderson, A.S.; Aschenbrenner, L.; Avery, M.; Berritt, S.; Boras, B.; Cardin, R.D.; Carlo, A.; Coffman, K.J.; et al. An oral SARS-CoV-2 M(pro) inhibitor clinical candidate for the treatment of COVID-19. Science 2021, 374, 1586–1593. [Google Scholar] [CrossRef]
- Najjar-Debbiny, R.; Gronich, N.; Weber, G.; Khoury, J.; Amar, M.; Stein, N.; Goldstein, L.H.; Saliba, W. Effectiveness of paxlovid in reducing severe COVID-19 and mortality in high risk patients. Clin. Infect. Dis. 2022, 76, e342–e349. [Google Scholar] [CrossRef] [PubMed]
- Sokhela, S.; Bosch, B.; Hill, A.; Simmons, B.; Woods, J.; Johnstone, H.; Akpomiemie, G.; Ellis, L.; Owen, A.; Casas, C.P.; et al. Randomized clinical trial of nitazoxanide or sofosbuvir/daclatasvir for the prevention of SARS-CoV-2 infection. J. Antimicrob. Chemother. 2022, 77, 2706–2712. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Institutes of Health. COVID-19 Treatment Guidelines Nitazoxanide. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 18 December 2022).
- U.S. National Institutes of Health. COVID-19 Treatment Guidelines Ivermectin. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/miscellaneous-drugs/ivermectin (accessed on 18 December 2022).
- Japan Pharmaceuticals and Medical Devices Agency. Evaluation and Licensing Division Report on the Deliberation Results—Avigan. Available online: https://www.pmda.go.jp/files/000210319.pdf (accessed on 12 November 2023).
- Logue, J.; Chakraborty, A.R.; Johnson, R.; Goyal, G.; Rodas, M.; Taylor, L.J.; Baracco, L.; McGrath, M.E.; Haupt, R.; Furlong, B.A.; et al. PIKfyve-specific inhibitors restrict replication of multiple coronaviruses in vitro but not in a murine model of COVID-19. Commun. Biol. 2022, 5, 808. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.J.; Toots, M.; Lee, S.; Lee, M.E.; Ludeke, B.; Luczo, J.M.; Ganti, K.; Cox, R.M.; Sticher, Z.M.; Edpuganti, V.; et al. Orally efficacious broad-spectrum ribonucleoside analog inhibitor of influenza and respiratory syncytial viruses. Antimicrob. Agents Chemother. 2018, 62, 10–1128. [Google Scholar] [CrossRef] [PubMed]
- Özlüşen, B.; Kozan, Ş.; Akcan, R.E.; Kalender, M.; Yaprak, D.; Peltek, İ.B.; Keske, Ş.; Gönen, M.; Ergönül, Ö. Effectiveness of favipiravir in COVID-19: A live systematic review. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 2575–2583. [Google Scholar] [CrossRef] [PubMed]
- Nelson, E.A.; Dyall, J.; Hoenen, T.; Barnes, A.B.; Zhou, H.; Liang, J.Y.; Michelotti, J.; Dewey, W.H.; DeWald, L.E.; Bennett, R.S.; et al. The phosphatidylinositol-3-phosphate 5-kinase inhibitor apilimod blocks filoviral entry and infection. PLoS Negl. Trop Dis. 2017, 11, e0005540. [Google Scholar] [CrossRef] [PubMed]
- Qiu, S.; Leung, A.; Bo, Y.; Kozak, R.A.; Anand, S.P.; Warkentin, C.; Salambanga, F.D.R.; Cui, J.; Kobinger, G.; Kobasa, D.; et al. Ebola virus requires phosphatidylinositol (3,5) bisphosphate production for efficient viral entry. Virology 2018, 513, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Elkin, P.L.; Resendez, S.; Mullin, S.; Troen, B.R.; Mammen, M.J.; Chang, S.; Franklin, G.; McCray, W.; Brown, S.H. Leukotriene inhibitors with dexamethasone show promise in the prevention of death in COVID-19 patients with low oxygen saturations. J. Clin. Transl. Sci. 2022, 6, e74. [Google Scholar] [CrossRef] [PubMed]
- Sharpley, A.L.; Williams, C.; Holder, A.A.; Godlewska, B.R.; Singh, N.; Shanyinde, M.; MacDonald, O.; Cowen, P.J. A phase 2a randomised, double-blind, placebo-controlled, parallel-group, add-on clinical trial of ebselen (SPI-1005) as a novel treatment for mania or hypomania. Psychopharmacology 2020, 237, 3773–3782. [Google Scholar] [CrossRef] [PubMed]
- Riva, L.; Yuan, S.; Yin, X.; Martin-Sancho, L.; Matsunaga, N.; Pache, L.; Burgstaller-Muehlbacher, S.; De Jesus, P.D.; Teriete, P.; Hull, M.V.; et al. Discovery of SARS-CoV-2 antiviral drugs through large-scale compound repurposing. Nature 2020, 586, 113–119. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine. A Study of LAM-002A for the Prevention of Progression of COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04446377 (accessed on 11 January 2023).
- Baranov, M.V.; Bianchi, F.; van den Bogaart, G. The PIKfyve inhibitor apilimod: A double-edged sword against COVID-19. Cells 2020, 10, 30. [Google Scholar] [CrossRef] [PubMed]
- Citron, F.; Perelli, L.; Deem, A.K.; Genovese, G.; Viale, A. Leukotrienes, a potential target for COVID-19. Prostaglandins Leukot Essent Fat. Acids 2020, 161, 102174. [Google Scholar] [CrossRef] [PubMed]
- Kil, J.; Pierce, C.; Tran, H.; Gu, R.; Lynch, E.D. Ebselen treatment reduces noise induced hearing loss via the mimicry and induction of glutathione peroxidase. Hear. Res. 2007, 226, 44–51. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine. SPI-1005 Treatment in Moderate COVID-19 Patients. Available online: https://clinicaltrials.gov/ct2/show/NCT04484025 (accessed on 18 December 2022).
- Hoertel, N.; Sánchez-Rico, M.; Vernet, R.; Beeker, N.; Jannot, A.S.; Neuraz, A.; Salamanca, E.; Paris, N.; Daniel, C.; Gramfort, A.; et al. Association between antidepressant use and reduced risk of intubation or death in hospitalized patients with COVID-19: Results from an observational study. Mol. Psychiatry 2021, 26, 5199–5212. [Google Scholar] [CrossRef] [PubMed]
- Zimniak, M.; Kirschner, L.; Hilpert, H.; Geiger, N.; Danov, O.; Oberwinkler, H.; Steinke, M.; Sewald, K.; Seibel, J.; Bodem, J. The serotonin reuptake inhibitor Fluoxetine inhibits SARS-CoV-2 in human lung tissue. Sci. Rep. 2021, 11, 5890. [Google Scholar] [CrossRef] [PubMed]
- Oskotsky, T.; Maric, I.; Tang, A.; Oskotsky, B.; Wong, R.J.; Aghaeepour, N.; Sirota, M.; Stevenson, D.K. Mortality risk among patients with COVID-19 prescribed selective serotonin reuptake inhibitor antidepressants. JAMA Netw. Open 2021, 4, e2133090. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Institutes of Health. COVID-19 Treatment Guidelines—Fluvoxamine. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/miscellaneous-drugs/fluvoxamine/ (accessed on 14 December 2022).
- McKeage, K.; Keating, G.M. Fenofibrate: A review of its use in dyslipidaemia. Drugs 2011, 71, 1917–1946. [Google Scholar] [CrossRef] [PubMed]
- Keating, G.M. Fenofibrate: A review of its lipid-modifying effects in dyslipidemia and its vascular effects in type 2 diabetes mellitus. Am. J. Cardiovasc. Drugs 2011, 11, 227–247. [Google Scholar] [CrossRef]
- Davies, S.P.; Mycroft-West, C.J.; Pagani, I.; Hill, H.J.; Chen, Y.H.; Karlsson, R.; Bagdonaite, I.; Guimond, S.E.; Stamataki, Z.; De Lima, M.A.; et al. The hyperlipidaemic drug fenofibrate significantly reduces infection by SARS-CoV-2 in cell culture models. Front. Pharmacol. 2021, 12, 660490. [Google Scholar] [CrossRef] [PubMed]
- Guzman-Esquivel, J.; Galvan-Salazar, H.R.; Guzman-Solorzano, H.P.; Cuevas-Velazquez, A.C.; Guzman-Solorzano, J.A.; Mokay-Ramirez, K.A.; Paz-Michel, B.A.; Murillo-Zamora, E.; Delgado-Enciso, J.; Melnikov, V.; et al. Efficacy of the use of mefenamic acid combined with standard medical care vs. standard medical care alone for the treatment of COVID-19: A randomized double-blind placebo-controlled trial. Int. J. Mol. Med. 2022, 49, 1–9. [Google Scholar] [CrossRef]
- Gold-von Simson, G.; Goldberg, J.D.; Rolnitzky, L.M.; Mull, J.; Leyne, M.; Voustianiouk, A.; Slaugenhaupt, S.A.; Axelrod, F.B. Kinetin in familial dysautonomia carriers: Implications for a new therapeutic strategy targeting mRNA splicing. Pediatr. Res. 2009, 65, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Souza, T.M.L.; Pinho, V.D.; Setim, C.F.; Sacramento, C.Q.; Marcon, R.; Fintelman-Rodrigues, N.; Chaves, O.A.; Heller, M.; Temerozo, J.R.; Ferreira, A.C.; et al. Preclinical development of kinetin as a safe error-prone SARS-CoV-2 antiviral able to attenuate virus-induced inflammation. Nat. Commun. 2023, 14, 199. [Google Scholar] [CrossRef]
- Rydén, L.; Grant, P.J.; Anker, S.D.; Berne, C.; Cosentino, F.; Danchin, N.; Deaton, C.; Escaned, J.; Hammes, H.P.; Huikuri, H.; et al. ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD—Summary. Diab. Vasc. Dis. Res. 2014, 11, 133–173. [Google Scholar] [CrossRef] [PubMed]
- Ventura-López, C.; Cervantes-Luevano, K.; Aguirre-Sánchez, J.S.; Flores-Caballero, J.C.; Alvarez-Delgado, C.; Bernaldez-Sarabia, J.; Sánchez-Campos, N.; Lugo-Sánchez, L.A.; Rodríguez-Vázquez, I.C.; Sander-Padilla, J.G.; et al. Treatment with metformin glycinate reduces SARS-CoV-2 viral load: An in vitro model and randomized, double-blind, Phase IIb clinical trial. Biomed. Pharmacother. 2022, 152, 113223. [Google Scholar] [CrossRef] [PubMed]
- Parthasarathy, H.; Tandel, D.; Siddiqui, A.H.; Harshan, K.H. Metformin suppresses SARS-CoV-2 in cell culture. Virus. Res. 2022, 323, 199010. [Google Scholar] [CrossRef] [PubMed]
- Schaller, M.A.; Sharma, Y.; Dupee, Z.; Nguyen, D.; Urueña, J.; Smolchek, R.; Loeb, J.C.; Machuca, T.N.; Lednicky, J.A.; Odde, D.J.; et al. Ex vivo SARS-CoV-2 infection of human lung reveals heterogeneous host defense and therapeutic responses. JCI Insight 2021, 6, e148003. [Google Scholar] [CrossRef] [PubMed]
- Bristol-Myers Squibb Co. GLUCOPHAGE® (Metformin Hydrochloride) Tablets. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/020357s037s039,021202s021s023lbl.pdf (accessed on 26 July 2023).
- Bramante, C.T.; Buse, J.; Tamaritz, L.; Palacio, A.; Cohen, K.; Vojta, D.; Liebovitz, D.; Mitchell, N.; Nicklas, J.; Lingvay, I.; et al. Outpatient metformin use is associated with reduced severity of COVID-19 disease in adults with overweight or obesity. J. Med. Virol. 2021, 93, 4273–4279. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Yang, X.; Yan, P.; Sun, T.; Zeng, Z.; Li, S. Metformin in patients with COVID-19: A systematic review and meta-analysis. Front. Med. 2021, 8, 704666. [Google Scholar] [CrossRef] [PubMed]
- Krausz, S.; Boumans, M.J.; Gerlag, D.M.; Lufkin, J.; van Kuijk, A.W.; Bakker, A.; de Boer, M.; Lodde, B.M.; Reedquist, K.A.; Jacobson, E.W.; et al. Brief report: A phase IIa, randomized, double-blind, placebo-controlled trial of apilimod mesylate, an interleukin-12/interleukin-23 inhibitor, in patients with rheumatoid arthritis. Arthritis. Rheum. 2012, 64, 1750–1755. [Google Scholar] [CrossRef] [PubMed]
- Bramante, C.T.; Huling, J.D.; Tignanelli, C.J.; Buse, J.B.; Liebovitz, D.M.; Nicklas, J.M.; Cohen, K.; Puskarich, M.A.; Belani, H.K.; Proper, J.L.; et al. Randomized trial of metformin, ivermectin, and fluvoxamine for COVID-19. N. Engl. J. Med. 2022, 387, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Zhao, H.; Tebbutt, S.J. A glimpse into long COVID and symptoms. Lancet Respir. Med. 2022, 10, e81. [Google Scholar] [CrossRef] [PubMed]
- U.S. Centers for Disease Control and Prevention. Post-COVID Conditions: Information for Healthcare Providers. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-conditions.html (accessed on 26 July 2023).
- Bramante, C.T.; Buse, J.B.; Liebovitz, D.M.; Nicklas, J.M.; Puskarich, M.A.; Cohen, K.; Belani, H.K.; Anderson, B.J.; Huling, J.D.; Tignanelli, C.J.; et al. Outpatient treatment of COVID-19 and incidence of post-COVID-19 condition over 10 months (COVID-OUT): A multicentre, randomised, quadruple-blind, parallel-group, phase 3 trial. Lancet Infect. Dis. 2023, 23, 1119–1129. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Morrone, M.C.; Patrono, C.; Santoro, M.G.; Schiaffino, S.; Remuzzi, G.; Bussolati, G. Long Covid: Where we stand and challenges ahead. Cell Death Differ. 2022, 29, 1891–1900. [Google Scholar] [CrossRef] [PubMed]
- Rauf, A.; Olatunde, A.; Imran, M.; Alhumaydhi, F.A.; Aljohani, A.S.M.; Khan, S.A.; Uddin, M.S.; Mitra, S.; Emran, T.B.; Khayrullin, M.; et al. Honokiol: A review of its pharmacological potential and therapeutic insights. Phytomedicine 2021, 90, 153647. [Google Scholar] [CrossRef] [PubMed]
- Tanikawa, T.; Hayashi, T.; Suzuki, R.; Kitamura, M.; Inoue, Y. Inhibitory effect of honokiol on furin-like activity and SARS-CoV-2 infection. J. Tradit. Complement. Med. 2022, 12, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.P.; Tsai, S.Y.; Lee Chao, P.D.; Chen, Y.C.; Hou, Y.C. Pharmacokinetics, bioavailability, and tissue distribution of magnolol following single and repeated dosing of magnolol to rats. Planta Med. 2011, 77, 1800–1805. [Google Scholar] [CrossRef] [PubMed]
- Pacheco-Quito, E.M.; Ruiz-Caro, R.; Veiga, M.D. Carrageenan: Drug delivery systems and other biomedical applications. Mar. Drugs 2020, 18, 583. [Google Scholar] [CrossRef] [PubMed]
- Bansal, S.; Jonsson, C.B.; Taylor, S.L.; Figueroa, J.M.; Dugour, A.V.; Palacios, C.; Vega, J.C. Iota-carrageenan and xylitol inhibit SARS-CoV-2 in Vero cell culture. PLoS ONE 2021, 16, e0259943. [Google Scholar] [CrossRef]
- Hebar, A.; Koller, C.; Seifert, J.M.; Chabicovsky, M.; Bodenteich, A.; Bernkop-Schnürch, A.; Grassauer, A.; Prieschl-Grassauer, E. Non-clinical safety evaluation of intranasal iota-carrageenan. PLoS ONE 2015, 10, e0122911. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, J.M.; Lombardo, M.E.; Dogliotti, A.; Flynn, L.P.; Giugliano, R.; Simonelli, G.; Valentini, R.; Ramos, A.; Romano, P.; Marcote, M.; et al. Efficacy of a nasal spray containing iota-carrageenan in the postexposure prophylaxis of COVID-19 in hospital personnel dedicated to patients care with COVID-19 disease. Int. J. Gen. Med. 2021, 14, 6277–6286. [Google Scholar] [CrossRef] [PubMed]
- Nwabufo, C.K.; Hoque, M.T.; Yip, L.; Khara, M.; Mubareka, S.; Pollanen, M.S.; Bendayan, R. SARS-CoV-2 infection dysregulates the expression of clinically relevant drug metabolizing enzymes in Vero E6 cells and membrane transporters in human lung tissues. Front. Pharmacol. 2023, 14, 1124693. [Google Scholar] [CrossRef]
- Blair, H.A. Remdesivir: A Review in COVID-19. Drugs 2023, 83, 1215–1237. [Google Scholar] [CrossRef] [PubMed]
- Gerhart, J.; Cox, D.S.; Singh, R.S.P.; Chan, P.L.S.; Rao, R.; Allen, R.; Shi, H.; Masters, J.C.; Damle, B. A Comprehensive review of the clinical pharmacokinetics, pharmacodynamics, and drug interactions of nirmatrelvir/ritonavir. Clin. Pharmacokinet. 2024, 63, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Wattanakul, T.; Chotsiri, P.; Scandale, I.; Hoglund, R.M.; Tarning, J. A pharmacometric approach to evaluate drugs for potential repurposing as COVID-19 therapeutics. Expert. Rev. Clin. Pharmacol. 2022, 15, 945–958. [Google Scholar] [CrossRef] [PubMed]
- Delorey, T.M.; Ziegler, C.G.K.; Heimberg, G.; Normand, R.; Yang, Y.; Segerstolpe, Å.; Abbondanza, D.; Fleming, S.J.; Subramanian, A.; Montoro, D.T.; et al. COVID-19 tissue atlases reveal SARS-CoV-2 pathology and cellular targets. Nature 2021, 595, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Salim, A.K.; Ingraham, N.E.; Murray, T.A.; Marmor, S.; Hovertsen, S.; Gronski, J.; McNeil, C.; Feng, R.; Guzman, G.; Abdelwahab, N.; et al. Time to Stop Using Ineffective COVID-19 Drugs. N. Engl. J. Med. 2022, 387, 654–655. [Google Scholar]
- Abrescia, N. Preventing SARS-CoV-2 infection and its severe outcomes in HIV-infected people. Aids 2023, 37, 1473–1475. [Google Scholar] [CrossRef] [PubMed]
- Verburgh, M.L.; van der Valk, M.; Rijnders, B.J.A.; Reiss, P.; Wit, F. No association between use of tenofovir disoproxil fumarate, etravirine, or integrase-strand transfer inhibitors and acquisition or severe outcomes of SARS-CoV-2 infection in people with HIV in the Netherlands. Aids 2023, 37, 1481–1486. [Google Scholar] [CrossRef] [PubMed]
| Calu-3 | Caco-2 | Vero | PBM | CEM | Huh7 | |
|---|---|---|---|---|---|---|
| Drug | CC50 (μM) | CC50 (μM) {Unbound} | CC50 (μM) {Unbound} | CC50 (μM) {Unbound} | CC50 (μM) {Unbound} | CC50 (μM) {Unbound} |
| * NHC | >100 | >100 | 18.8 {18.8} | 59.8 {59.8} | 2.4 {2.4} | 59.1 {59.1} |
| GS-441524 | >100 | >100 | >100 | >100 | >100 | >100 |
| Remdesivir | >100 | >100 | >100 | 4.5 {3.7} | 11 {10.1} | 2.1 {1.9} |
| Nirmatrelvir | >100 | >100 | >100 | >100 | >100 | >100 |
| Nitazoxanide | 49.8 | 7.2 | 8.7 {7.8} | 8.3 {6.7} | 15.5 {14} | 54.3 {48.9} |
| Ivermectin | 17.5 | 5.8 | 35.2 {31.9} | 29.2 {23.8} | 12 {9.5} | 5.6 {5.1} |
| Imatinib | 90 | 66 | 12.3 {11.1} | 13.9 {11.3} | 14.1 {12.8} | 11.9 {10.8} |
| Apilimod mesylate | >100 | >100 | >100 | >100 | 68.5 {62.2} | 60.3 {54.8} |
| Celecoxib | 70.5 | 59.1 | 50 {45.2} | >100 | 77.1 {69.6} | 31.1 {28.1}} |
| Zileuton | 46.7 | >100 | >100 | >100 | >100 | >100 |
| Daclatasvir | >100 | 67.6 | 50.6 {45.6} | 36.4 {29.2} | 26.2 {23.6} | 53.6 {48.3} |
| Fenofibrate | ≥100 | >100 | >100 | 38.9 {31.2} | 28.5 | >100 |
| Ebselen | >100 | >100 | 22.4 {20.3} | 93.2 {75.5} | 46.7 {42.3} | 84.3 {76.3} |
| Favipiravir | >300 | >300 | >100 | >100 | >100 | >100 |
| Fluvoxamine (maleate) | >100 | >100 | 35.5 {32.8} | 35.4 {29.9} | 20.0 {18.5} | 36.7 {33.9} |
| Honokiol | 27.5 | 18.4 | 40.4 {37.8} | 30.4 {26.5} | 28.6 {26.8} | 13.2 {12.4} |
| Iota-Carrageenan | >100 | >100 | >100 | >100 | 95.9 {NE} | >100 |
| Mefenamic acid | >100 | >100 | >100 | >100 | >100 | >100 |
| Vero CCL-81 Cells | Cmax (μM) | ||||||
|---|---|---|---|---|---|---|---|
| Drug Typical Dose | EC50/EC90 (μM) | CC50 (μM) | (% CV or Range) {Unbound} | Fun | Unbound Cmax/EC50 | Therapeutic Category | Refs |
| Doxycycline 100 mg bid then 100 mg/d | 69.3/102 | ≥100 | 3.67 (50%) {0.55} | 0.15 | 0.008 | ABA | [111] |
| Clofazimine 200 mg/d | 0.5/3 | 34.3 | 1.67 (2.14–2.60) {0.002} | 0.001 | 0.003 | ABA | [112] |
| Famotidine 40 mg bid | 160/NE | >100 | 0.2 (29%) {0.16} | 0.8 | 0.001 | AH | [113] |
| Chlorpheniramine maleate 8 mg q 4–6 h | 31/104 | >100 | 0.027 (41%) {0.008} | 0.28 | 0.0002 | AH | [114] |
| Lotilaner 20 mg/kg, once (dog or cat) | 1.9/4.9 | 44.3 | 6.72 (25%) {0.007} | 0.001 | 0.0035 | APA | [115] |
| Ciclesonide Inhale 80 mg bid | 4.1/7.8 | 33.9 | 0.001 {0.0000/1} | 0.01 | 1.9 × 10−6 | GC | [116] |
| Montelukast sodium 10 mg/d | 4.9/7.2 | 35.9 | 0.58 (0.3–0.90) {0.009} | 0.01 | 0.002 | LM | [117] |
| Bromhexine 16 mg bid | 0.8/6.2 | >100 | 0.093 (24% {0.005}) | 0.05 | 0.006 | ML | [118] |
| Elbasivir 50 mg/d | 3.4/12.5 | >100 | 0.26 (47%) {0.003} | 0.01 | 0.001 | NNAV | [119] |
| Amantadine 129 mg bid | 138/288 | >100 | 2.17 (9%) {0.002} | 0.001 | 0.0002 | NNAV | [120] |
| Velpatasvir 100 mg/d | 19.1/79.6 | >100 | 0.29 (54%) {0.001} | 0.005 | 7.8 × 10−5 | NNAV | [81] |
| GC376 10 mg/kg (in cats) | 0.2/0.6 | >100 | 1.7 {NE} | NE | NE | NNAV | [121] |
| Cannabinol cigarette (0.79 g) with 6.8% TH | 2.7/8.7 | 37.3 | 0.032 (0.012–0.051) {0.013} | 0.1 | 0.0011 | NP | [122] |
| Melatonin 2–6 mg/d | 22/NE | >100 | 0.0215 (0.009–0.034) {0.005} | 0.22 | 0.0002 | NP | [123] |
| Diclofenac sodium 50 mg tid | 97.6/141 | >100 | 2.41 {0.012} | 0.005 | 0.0001 | NSAID | [124,125] |
| Flavopiridol 30 mg/m2 + 60 mg/m2 infusion | 0.1/1.1 | 0.031 | 1.92 (55.7%) {0.096} | 0.05 | 0.99 | ONC | [126] |
| Acalabrutinib 100 mg bid | 11.1/70.9 | >100 | 0.69 {0.017} | 0.025 | 0.002 | ONC | [127] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hurwitz, S.J.; De, R.; LeCher, J.C.; Downs-Bowen, J.A.; Goh, S.L.; Zandi, K.; McBrayer, T.; Amblard, F.; Patel, D.; Kohler, J.J.; et al. Why Certain Repurposed Drugs Are Unlikely to Be Effective Antivirals to Treat SARS-CoV-2 Infections. Viruses 2024, 16, 651. https://doi.org/10.3390/v16040651
Hurwitz SJ, De R, LeCher JC, Downs-Bowen JA, Goh SL, Zandi K, McBrayer T, Amblard F, Patel D, Kohler JJ, et al. Why Certain Repurposed Drugs Are Unlikely to Be Effective Antivirals to Treat SARS-CoV-2 Infections. Viruses. 2024; 16(4):651. https://doi.org/10.3390/v16040651
Chicago/Turabian StyleHurwitz, Selwyn J., Ramyani De, Julia C. LeCher, Jessica A. Downs-Bowen, Shu Ling Goh, Keivan Zandi, Tamara McBrayer, Franck Amblard, Dharmeshkumar Patel, James J. Kohler, and et al. 2024. "Why Certain Repurposed Drugs Are Unlikely to Be Effective Antivirals to Treat SARS-CoV-2 Infections" Viruses 16, no. 4: 651. https://doi.org/10.3390/v16040651