
Peripheral Neuropathy in Patients with Hepatitis C Infection—Reversibility after HCV Eradication: A Single Center Study

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion, Exclusion Criteria, Testing, and Follow Up
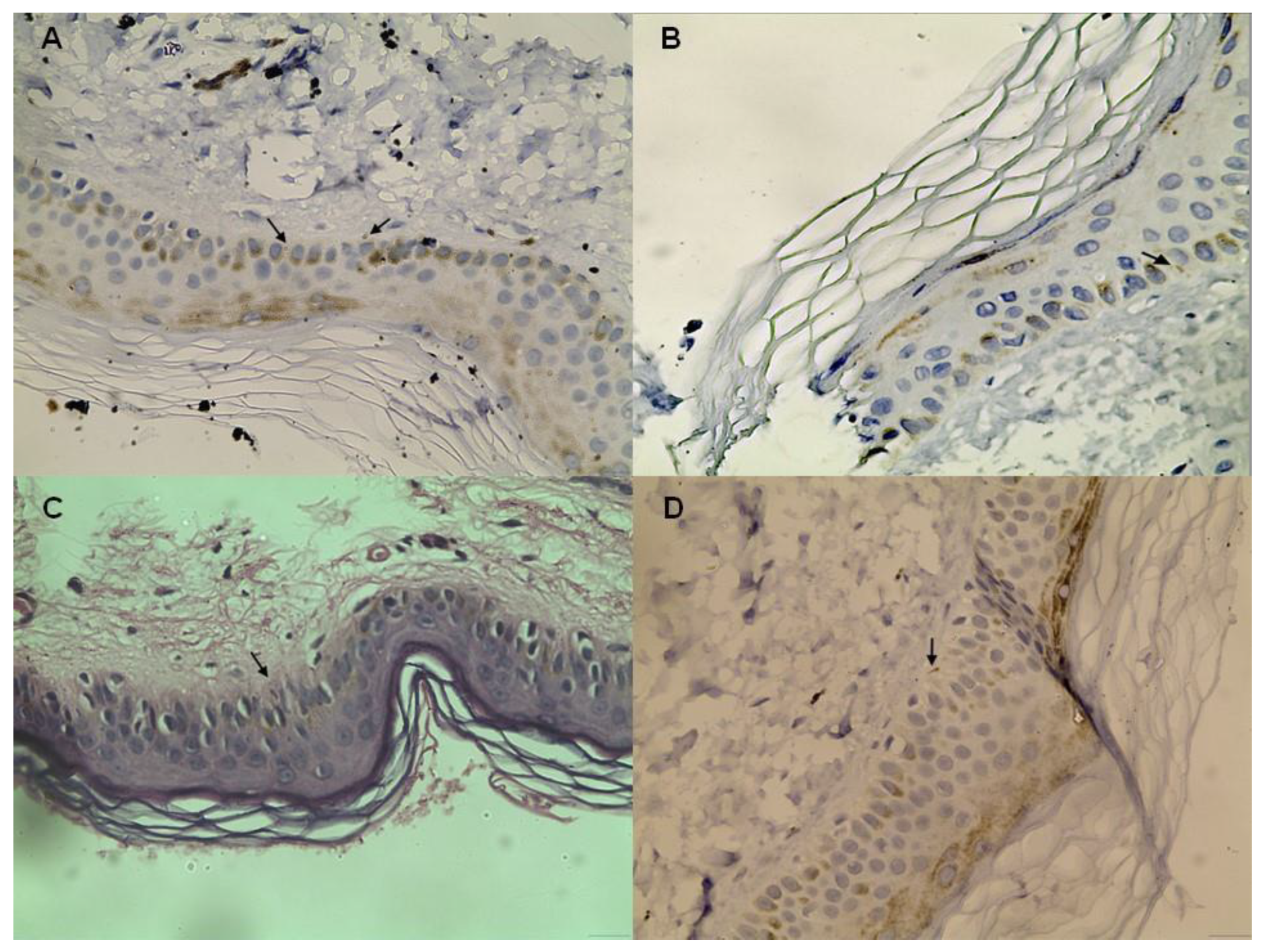
2.2. Skin Biopsy Staining and Evaluation
2.3. Electroneurography
2.4. Statistical Analysis
3. Results
3.1. Demographic and Laboratory Values
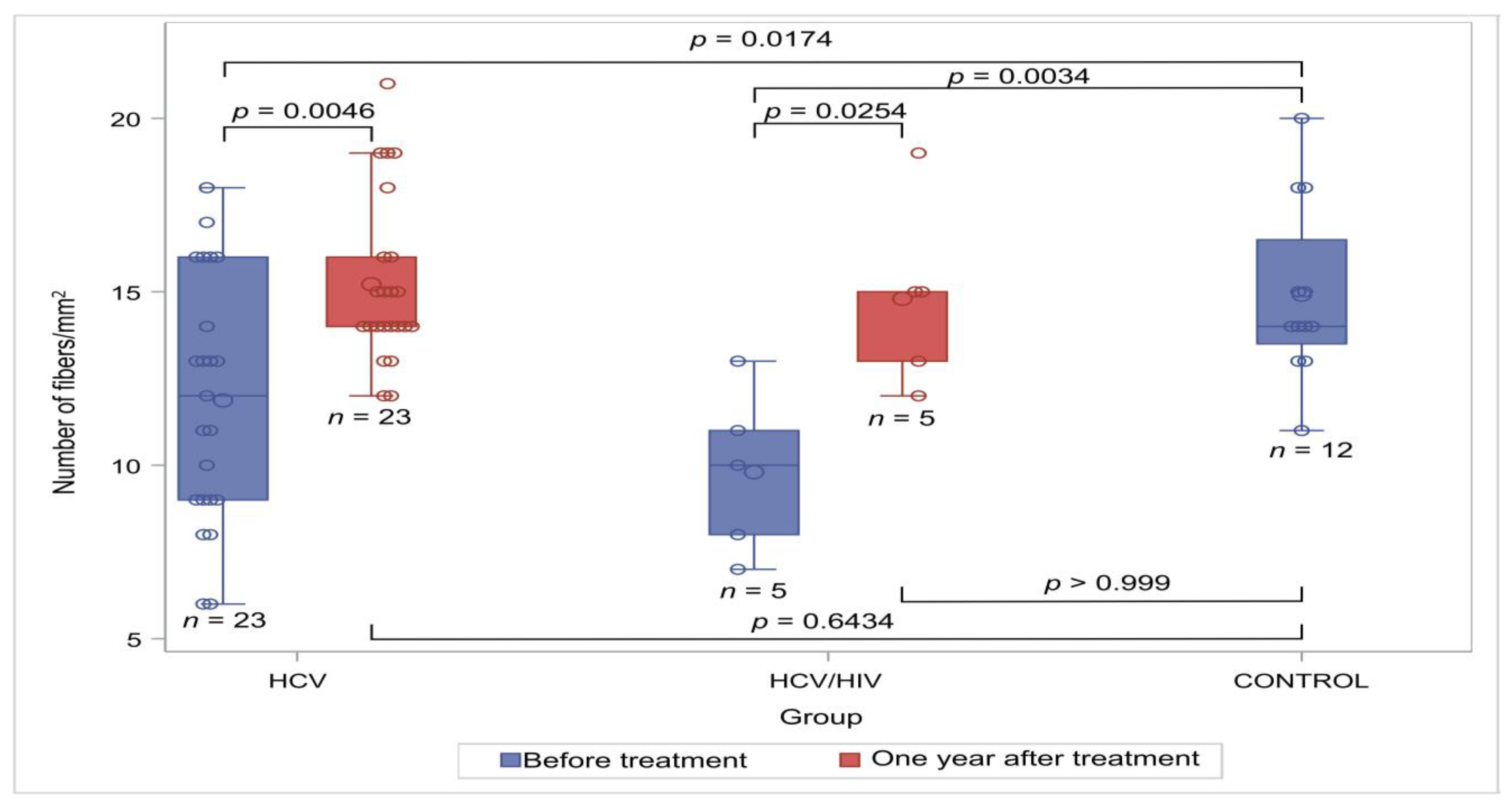
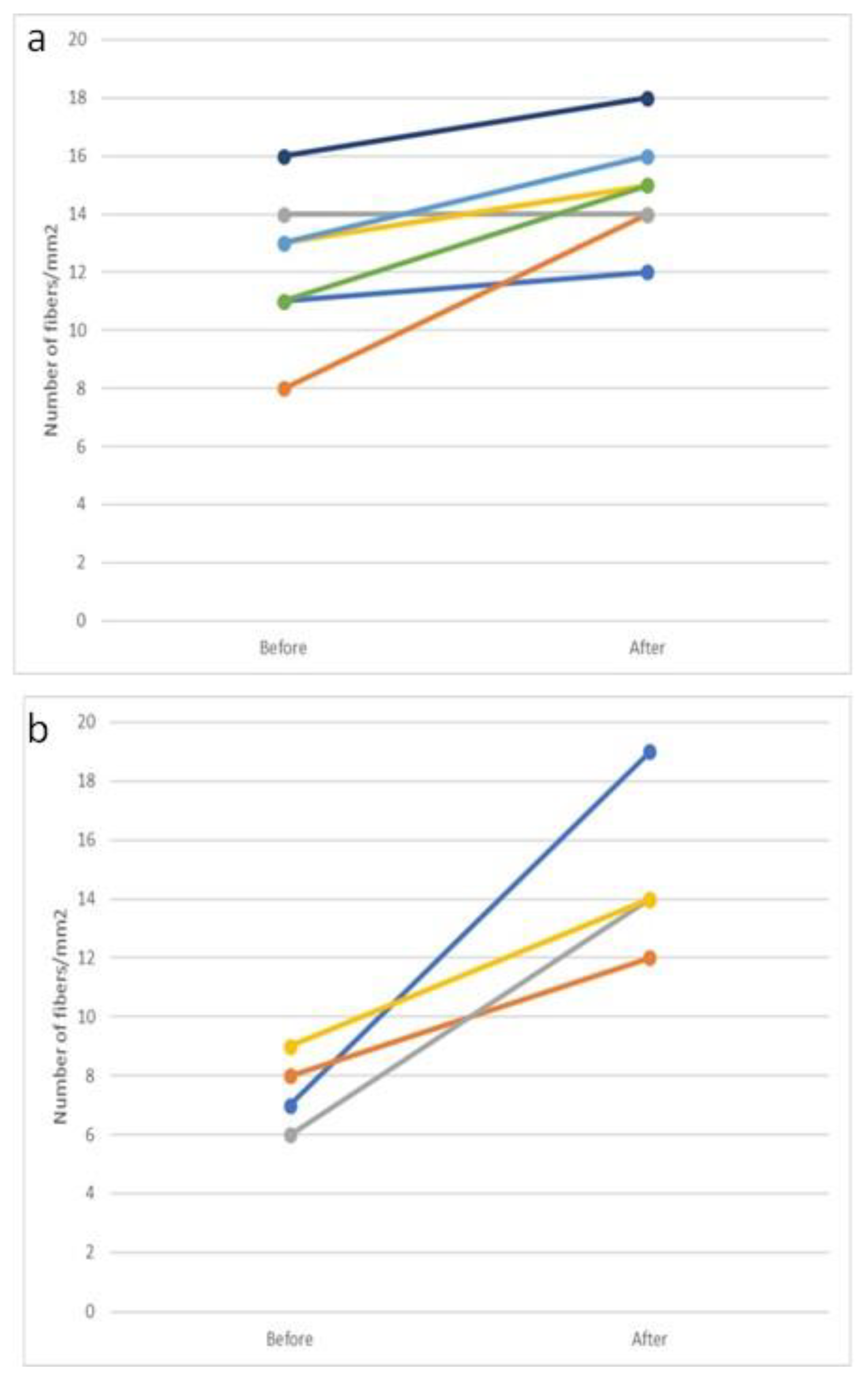
3.2. Neural Biopsies
3.3. Electroneurography Results
3.4. Characteristics of Patients with Peripheral Neuropathy
3.5. Risk Factors for Abnormal ENG
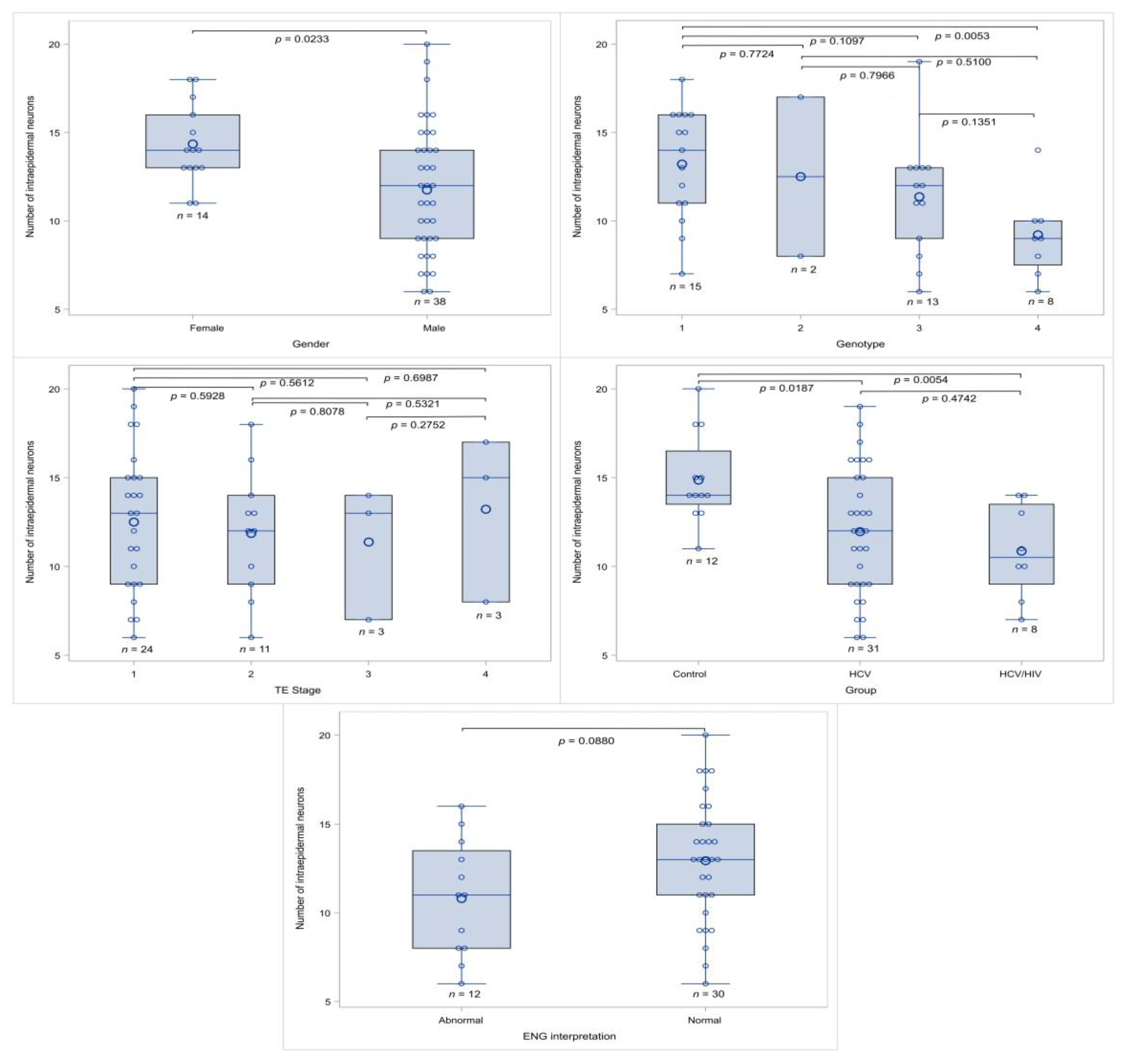
3.6. Factors Affecting Intraepidermal Nerve Density
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robertson, B.; Myers, G.; Howard, C.; Brettin, T.; Bukh, J.; Gaschen, B.; Gojobori, T.; Maertens, G.; Mizokami, M.; Nainan, O.; et al. Classification, nomenclature, and database development for hepatitis C virus (HCV) and related viruses: Proposals for standardization. International Committee on Virus Taxonomy. Arch. Virol. 1998, 143, 2493–2503. [Google Scholar] [CrossRef] [PubMed]
- Jefferies, M.; Rauff, B.; Rashid, H.; Lam, T.; Rafiq, S. Update on global epidemiology of viral hepatitis and preventive strategies. World J. Clin. Cases 2018, 6, 589–599. [Google Scholar] [CrossRef]
- WHO. Global Hepatitis Programme. Global Hepatitis Report 2017. Available online: https://www.who.int/publications/i/item/9789241565455 (accessed on 22 December 2023).
- Falade-Nwulia, O.; Suarez-Cuervo, C.; Nelson, D.R.; Fried, M.W.; Segal, J.B.; Sulkowski, M.S. Oral Direct-Acting Agent Therapy for Hepatitis C Virus Infection: A Systematic Review. Ann. Intern. Med. 2017, 166, 637–648. [Google Scholar] [CrossRef] [PubMed]
- Manns, M.P.; Buti, M.; Gane, E.; Pawlotsky, J.M.; Razavi, H.; Terrault, N.; Younossi, Z. Hepatitis C virus infection. Nat. Rev. Dis. Primers 2017, 3, 17006. [Google Scholar] [CrossRef]
- De Pace, V.; Morelli, M.C.; Ravaioli, M.; Maggi, F.; Galli, S.; Vero, V.; Re, M.C.; Cescon, M.; Pistello, M. Efficacy, Safety, and Predictors of Direct-acting antivirals in Hepatitis C Virus Patients with Heterogeneous Liver Diseases. New Microbiol. 2019, 42, 189–196. [Google Scholar] [PubMed]
- Flores-Chávez, A.; Carrion, J.A.; Forns, X.; Ramos-Casals, M. Extrahepatic manifestations associated with Chronic Hepatitis C Virus Infection. Rev. Esp. Sanid. Penit. 2017, 19, 87–97. [Google Scholar] [PubMed]
- Petta, S.; Craxì, A. Extrahepatic Manifestations of Chronic Viral C Hepatitis. Gastroenterol. Clin. N. Am. 2020, 49, 347–360. [Google Scholar] [CrossRef]
- Kuna, L.; Jakab, J.; Smolic, R.; Wu, G.Y.; Smolic, M. HCV Extrahepatic Manifestations. J. Clin. Transl. Hepatol. 2019, 7, 172–182. [Google Scholar] [CrossRef]
- Bonetti, B.; Scardoni, M.; Monaco, S.; Rizzuto, N.; Scarpa, A. Hepatitis C virus infection of peripheral nerves in type II cryoglobulinaemia. Virchows Arch. 1999, 434, 533–535. [Google Scholar] [CrossRef]
- Cacoub, P.; Renou, C.; Rosenthal, E.; Cohen, P.; Loury, I.; Loustaud-Ratti, V.; Yamamoto, A.M.; Camproux, A.C.; Hausfater, P.; Musset, L.; et al. Extrahepatic manifestations associated with hepatitis C virus infection. A prospective multicenter study of 321 patients. The GERMIVIC. Groupe d’Etude et de Recherche en Medecine Interne et Maladies Infectieuses sur le Virus de l’Hepatite C. Medicine 2000, 79, 47–56. [Google Scholar] [CrossRef]
- Zaltron, S.; Puoti, M.; Liberini, P.; Antonini, L.; Quinzanini, M.; Manni, M.; Forleo, M.A.; Rossi, S.; Spinetti, A.; Zanini, B.; et al. High prevalence of peripheral neuropathy in hepatitis C virus infected patients with symptomatic and asymptomatic cryoglobulinaemia. Ital. J. Gastroenterol. Hepatol. 1998, 30, 391–395. [Google Scholar] [PubMed]
- Cashman, C.R.; Höke, A. Mechanisms of distal axonal degeneration in peripheral neuropathies. Neurosci. Lett. 2015, 596, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Russi, S.; Sansonno, D.; Monaco, S.; Mariotto, S.; Ferrari, S.; Pavone, F.; Lauletta, G.; Dammacco, F. HCV RNA Genomic sequences and HCV-E2 glycoprotein in sural nerve biopsies from HCV-infected patients with peripheral neuropathy. Neuropathol. Appl. Neurobiol. 2018, 44, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, E.; Cacoub, P. Extrahepatic manifestations in chronic hepatitis C virus carriers. Lupus 2015, 24, 469–482. [Google Scholar] [CrossRef] [PubMed]
- Moretti, R.; Giuffrè, M.; Merli, N.; Caruso, P.; Di Bella, S.; Tiribelli, C.; Crocè, L.S. Hepatitis C Virus-Related Central and Peripheral Nervous System Disorders. Brain Sci. 2021, 11, 1569. [Google Scholar] [CrossRef] [PubMed]
- Bonetti, B.; Invernizzi, F.; Rizzuto, N.; Bonazzi, M.L.; Zanusso, G.L.; Chinaglia, G.; Monaco, S. T-cell-mediated epineurial vasculitis and humoral-mediated microangiopathy in cryoglobulinemic neuropathy. J. Neuroimmunol. 1997, 73, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Biasiotta, A.; Casato, M.; La Cesa, S.; Colantuono, S.; Di Stefano, G.; Leone, C.; Carlesimo, M.; Piroso, S.; Cruccu, G.; Truini, A. Clinical, neurophysiological, and skin biopsy findings in peripheral neuropathy associated with hepatitis C virus-related cryoglobulinemia. J. Neurol. 2014, 261, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Saadoun, D.; Bieche, I.; Authier, F.J.; Laurendeau, I.; Jambou, F.; Piette, J.C.; Vidaud, M.; Maisonobe, T.; Cacoub, P. Role of matrix metalloproteinases, proinflammatory cytokines, and oxidative stress-derived molecules in hepatitis C virus-associated mixed cryoglobulinemia vasculitis neuropathy. Arthritis Rheum. 2007, 56, 1315–1324. [Google Scholar] [CrossRef] [PubMed]
- Ammendola, A.; Sampaolo, S.; Ambrosone, L.; Ammendola, E.; Ciccone, G.; Migliaresi, S.; Di Iorio, G. Peripheral neuropathy in hepatitis-related mixed cryoglobulinemia: Electrophysiologic follow-up study. Muscle Nerve 2005, 31, 382–385. [Google Scholar] [CrossRef]
- Nemni, R.; Sanvito, L.; Quattrini, A.; Santuccio, G.; Camerlingo, M.; Canal, N. Peripheral neuropathy in hepatitis C virus infection with and without cryoglobulinaemia. J. Neurol. Neurosurg. Psychiatry 2003, 74, 1267–1271. [Google Scholar] [CrossRef]
- Santoro, L.; Manganelli, F.; Briani, C.; Giannini, F.; Benedetti, L.; Vitelli, E.; Mazzeo, A.; Beghi, E.; HCV Peripheral Nerve Study Group. Prevalence and characteristics of peripheral neuropathy in hepatitis C virus population. J. Neurol. Neurosurg. Psychiatry 2006, 77, 626–629. [Google Scholar] [CrossRef]
- Paoletti, V.; Donnarumma, L.; De Matteis, A.; Mammarella, A.; Labbadia, G.; Musca, A.; Francia, A. Peripheral neuropathy without cryoglobulinemia in patients with hepatitis C virus infection. Panminerva Med. 2000, 42, 175–178. [Google Scholar] [PubMed]
- Ijichi, T.; Kono, I.; Mori, S.; Nakajima, K.; Nakagawa, M.; Okanoue, T. Peripheral neuropathy in Japanese patients with hepatitis C virus infection. Intern. Med. 2003, 42, 394–399. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver; Clinical Practice Guideline Panel. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet. Med. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.H.; Xin, Y.N.; Dong, Q.J.; Wang, Q.; Jiang, X.J.; Zhan, S.H.; Sun, Y.; Xuan, S.Y. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: An updated meta-analysis. Hepatology 2011, 53, 726–736. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Recommendations on Treatment of Hepatitis C 2018. J. Hepatol. 2018, 69, 461–511. [Google Scholar] [CrossRef] [PubMed]
- Pittenger, G.L.; Ray, M.; Burcus, N.I.; McNulty, P.; Basta, B.; Vinik, A.I. Intraepidermal nerve fibers are indicators of small-fiber neuropathy in both diabetic and nondiabetic patients. Diabetes Care 2004, 27, 1974–1979. [Google Scholar] [CrossRef]
- Chien, H.F.; Tseng, T.J.; Lin, W.M.; Yang, C.C.; Chang, Y.C.; Chen, R.C.; Hsieh, S.T. Quantitative pathology of cutaneous nerve terminal degeneration in the human skin. Acta Neuropathol. 2001, 102, 455–461. [Google Scholar] [CrossRef]
- Dalsgaard, C.J.; Rydh, M.; Haegerstrand, A. Cutaneous innervation in man visualized with protein gene product 9.5 (PGP 9.5) antibodies. Histochemistry 1989, 92, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Pica, F.; Volpi, A.; Serafino, A.; Fraschetti, M.; Franzese, O.; Garaci, E. Autocrine nerve growth factor is essential for cell survival and viral maturation in HHV-8-infected primary effusion lymphoma cells. Blood 2000, 95, 2905–2912. [Google Scholar] [CrossRef] [PubMed]
- Raicher, I.; Ravagnani, L.H.C.; Correa, S.G.; Dobo, C.; Mangueira, C.L.P.; Macarenco, R.S.E.S. Investigation of nerve fibers in the skin by biopsy: Technical aspects, indications, and contribution to diagnosis of small-fiber neuropathy. Einstein 2022, 20, eMD8044. [Google Scholar] [CrossRef]
- Lauria, G.; Lombardi, R. Skin biopsy: A new tool for diagnosing peripheral neuropathy. BMJ 2007, 334, 1159–1162. [Google Scholar] [CrossRef]
- McCarthy, B.G.; Hsieh, S.T.; Stocks, A.; Hauer, P.; Macko, C.; Cornblath, D.R.; Griffin, J.W.; McArthur, J.C. Cutaneous innervation in sensory neuropathies: Evaluation by skin biopsy. Neurology 1995, 45, 1848–1855. [Google Scholar] [CrossRef] [PubMed]
- Skopelitis, E.; Aroni, K.; Kontos, A.N.; Konstantinou, K.; Kokotis, P.; Karandreas, N.; Kordossis, T. Early detection of subclinical HIV sensory polyneuropathy using intraepidermal nerve fibre density quantification: Association with HIV stage and surrogate markers. Int. J. STD AIDS 2007, 18, 856–860. [Google Scholar] [CrossRef]
- Xyla, V.; Skopelitis, E.; Ziakas, P.D.; Kontos, A.; Ioannidis, E.; Kordossis, T.; Aroni, K. PGP 9.5 neuronal marker may differentiate immunohistochemically HIV-related from Mediterranean and immunosuppression-associated Kaposi’s sarcoma. Arch. Dermatol. Res. 2013, 305, 917–923. [Google Scholar] [CrossRef] [PubMed]
- McArthur, J.C.; Stocks, E.A.; Hauer, P.; Cornblath, D.R.; Griffin, J.W. Epidermal nerve fiber density: Normative reference range and diagnostic efficiency. Arch. Neurol. 1998, 55, 1513–1520. [Google Scholar] [CrossRef] [PubMed]
- Gemignani, F.; Brindani, F.; Alfieri, S.; Giuberti, T.; Allegri, I.; Ferrari, C.; Marbini, A. Clinical spectrum of cryoglobulinaemic neuropathy. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1410–1414. [Google Scholar] [CrossRef]
- Younossi, Z.; Kallman, J.; Kincaid, J. The effects of HCV infection and management on health-related quality of life. Hepatology 2007, 45, 806–816. [Google Scholar] [CrossRef]
- Mazzaro, C.; Quartuccio, L.; Adinolfi, L.E.; Roccatello, D.; Pozzato, G.; Nevola, R.; Tonizzo, M.; Gitto, S.; Andreone, P.; Gattei, V. A Review on Extrahepatic Manifestations of Chronic Hepatitis C Virus Infection and the Impact of Direct-Acting Antiviral Therapy. Viruses 2021, 13, 2249. [Google Scholar] [CrossRef] [PubMed]
- Chemello, L.; Cavalletto, L.; Ferrari, S.; Monaco, S. Impact of direct acting antivirals (DAA) on neurologic disorders in chronic hepatitis C. Minerva Gastroenterol. 2021, 67, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Androutsakos, T.; Mouziouras, D.; Katelani, S.; Psichogiou, M.; Sfikakis, P.P.; Protogerou, A.D.; Argyris, A.A. A Comparative Study on the Presence and Reversibility of Subclinical Arterial Damage in HCV-Infected Individuals and Matched Controls. Viruses 2023, 15, 1374. [Google Scholar] [CrossRef] [PubMed]
- Cacoub, P.; Comarmond, C.; Vieira, M.; Régnier, P.; Saadoun, D. HCV-related lymphoproliferative disorders in the direct-acting antiviral era: From mixed cryoglobulinaemia to B-cell lymphoma. J. Hepatol. 2022, 76, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Zanone, M.M.; Marinucci, C.; Ciancio, A.; Cocito, D.; Zardo, F.; Spagone, E.; Ferrero, B.; Cerruti, C.; Charrier, L.; Cavallo, F.; et al. Peripheral neuropathy after viral eradication with direct-acting antivirals in chronic HCV hepatitis: A prospective study. Liver Int. 2021, 41, 2611–2621. [Google Scholar] [CrossRef] [PubMed]
- Gøransson, L.G.; Mellgren, S.I.; Lindal, S.; Omdal, R. The effect of age and gender on epidermal nerve fiber density. Neurology 2004, 62, 774–777. [Google Scholar] [CrossRef]
- Provitera, V.; Gibbons, C.H.; Wendelschafer-Crabb, G.; Donadio, V.; Vitale, D.F.; Stancanelli, A.; Caporaso, G.; Liguori, R.; Wang, N.; Santoro, L.; et al. A multi-center, multinational age- and gender-adjusted normative dataset for immunofluorescent intraepidermal nerve fiber density at the distal leg. Eur. J. Neurol. 2016, 23, 333–338. [Google Scholar] [CrossRef]
- Umapathi, T.; Tan, W.L.; Tan, N.C.; Chan, Y.H. Determinants of epidermal nerve fiber density in normal individuals. Muscle Nerve 2006, 33, 742–746. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HCV Group (n = 31) Median (Range) | HCV/HIV Group (n = 9) Median (Range) | Healthy Controls (n = 12) Median (Range) | p Value | |
|---|---|---|---|---|
| Age | 43 (29–64) | 41.5 (32–52) | 57.5 (31–71) | 0.0356 |
| Male n, % | 25 (80.7%) | 8 (88.9%) | 5 (41.7%) | 0.0281 |
| Duration of HCV infection in years | 9 (1–28) | 7 (1–11) | n/a | 0.3823 |
| HCV genotype 1/2/3/4 | 13/2/10/6 | 3/0/3/2 | n/a | 0.0729 |
| HCV RNA in IU/mL | 1,500,000 (110,000–37,000,000) | 3,400,000 (120,000–6,456,000) | n/a | 0.5819 |
| Serum AST value | 35 (15–164) | 54 (21–161) | 25 (10–42) | 0.0023 |
| Serum ALT value | 52 (17–233) | 74 (21–301) | 31.5 (12–41) | 0.0006 |
| Serum ggt value | 35 (9–198) | 61 (30–160) | 28.5 (9–60) | 0.02041 |
| Serum ALP value | 67 (28–272) | 80 (66–147) | 67.5 (34–261) | 0.0955 |
| PLTs value | 210,000 (118,000–452,000) | 169,000 (156,000–329,000) | 275,000 (120,000–401,000) | 0.1454 |
| TE value | 7.7 (3.5–35.5) | 9.3 (4–12) | 5.6 (3.2–8.3) | 0.1889 |
| TE value (≥10/<10) | 4/23 | 3/3 | 0/9 | 0.0426 |
| Fib-4 score | 1.1 (0.2–4.5) | 1.5 (0.5–2.3) | 0.9 (0.3–3) | 0.4397 |
| Fib-4 score (≥1.3/<1.3) | 11/20 | 5/4 | 3/9 | 0.4021 |
| APRI score | 0.6 (0.1–8.7) | 1 (0.3–2.3) | 0.3 (0.1–0.9) | 0.0023 |
| APRI score (≥1.5/<1.5) | 8/23 | 1/8 | 0/12 | 0.1066 |
| HCV Group before Treatment (n = 31) | HCV Group after Treatment (n = 25) | HCV/HIV Group before Treatment (n = 9) | HCV/HIV Group after Treatment (n = 8) | Healthy Controls (n = 12) | p Value | |
|---|---|---|---|---|---|---|
| Number of neuronal fibers/mm2 in upper epidermal layer, median (range) after exclusion of patients lost to follow up | 12 (6–18) | 14 (12–21) | 10 (7–13) | 15 (12–19) | 14 (11–20) | 0.0067 * |
| ENG Outcome | |||
|---|---|---|---|
| Abnormal | Normal | ||
| Characteristic | Median (Range) or Number of Cases | Median (Range) or Number of Cases | p Value |
| Age | 42 (35.5–52) | 39.5 (34–53.5) | 0.8298 |
| Gender (male) | 11/91.67% | 16/76.19% | 0.3792 |
| Genotype (1/2/3/4) | 4/0/6/2 | 10/2/6/4 | 0.5997 |
| HCV duration (years) | 7.5 (2–13.5) | 8 (1–18) | 0.8031 |
| Number of intraepidermal neurons/mm2 | 11 (8–13.5) | 12 (9–13.5) | 0.4113 |
| HCV RNA (IU/mL) | 1,953,585 (612,000–4,829,705) | 1,860,000 (580,000–4,530,000) | 0.7933 |
| Infection (HCV/HCV and HIV) | 8/4 | 18/3 | 0.3774 |
| AFP (ng/mL) | 4 (2.8–5.5) | 3 (2–4) | 0.0803 |
| ALP (IU/L) | 67.5 (65–88) | 67 (53–79) | 0.5872 |
| ALT(IU/L) | 56 (37.5–161.5) | 63 (36–101) | 0.6532 |
| AST(IU/L) | 43.5 (24–112.5) | 35 (27–64) | 0.7361 |
| Direct bilirubin (mg/dL) | 0.5 (0.3–0.7) | 0.3 (0.2–0.5) | 0.0430 |
| Total bilirubin (mg/dL) | 0.87 (0.7–1.2) | 0.8 (0.5–1) | 0.1237 |
| ggt (IU/L) | 69.5 (29.5–114) | 33 (21–49) | 0.0454 |
| HbA1C (%) | 5.25 (5–6) | 5.35 (5.1–5.7) | 0.9151 |
| INR | 1 (1–1.1) | 1 (1–1) | 0.2140 |
| PLTs (k/mL) | 176,000 (160,500–260,500) | 231,000 (177,000–246,000) | 0.5493 |
| APRI | 0.84 (0.3455–1.62) | 0.606 (0.424–1.124) | 0.9106 |
| APRI score (≥1.5/<1.5) | 3/9 | 4/17 | 0.6856 |
| FIB-4 | 1.27 (0.69–2.085) | 0.99 (0.61–1.29) | 0.3691 |
| Fib-4 score (≥1.3/<1.3) | 6/6 | 5/16 | 0.1490 |
| TE score | 6.6 (4.3–9.2) | 7.7 (4.35–8.35) | 0.8951 |
| TE value (≥10/<10) | 2/8 | 2/14 | 0.6254 |
| (A) | ||||
| Variable | Values | Fiber Count (Median (Range)) | p Value | |
| Gender | F | 14 (11–18) | 0.0233 | |
| M | 12 (6–20) | |||
| Group | Control | 14 (11–20) | 0.0175 | |
| HCV | 12 (6–19) | |||
| HCV/HIV | 10.5 (7–14) | |||
| Genotype | 1 | 14 (7–18) | 0.0476 | |
| 2 | 12.5 (8–17) | |||
| 3 | 12 (6–19) | |||
| 4 | 9 (6–14) | |||
| Staging | F0–1 | 13 (6–20) | 0.8343 | |
| F2 | 12 (6–18) | |||
| F3 | 13 (7–14) | |||
| F4 | 15 (8–17) | |||
| ENG | Abnormal | 11 (6–16) | 0.0880 | |
| Normal | 13 (6–20) | |||
| TE value | ≥10 | 13.5 (7–17) | 0.9557 | |
| <10 | 13 (6–20) | |||
| Treatment * | Before treatment | 13 (10–15) | 0.0012 | |
| One year after SVR | 14.5 (14–16) | |||
| (B) | ||||
| Parameter | Beta | Standard Error | p Value | |
| Model a | Gender (female) | 1.57 | 1.11 | 0.1652 |
| Age | -0.01 | 0.04 | 0.7586 | |
| Group HCV (ref non-HCV) | -2.67 | 1.23 | 0.0354 | |
| Model b | Gender female | 2.26 | 1.09 | 0.0439 |
| Age | 0.01 | 0.04 | 0.8601 | |
| Group HIV (ref non-HIV) | -1.46 | 1.34 | 0.2804 | |
| Model c | Gender female | 3.81 | 1.4 | 0.0110 |
| Genotype 1 (reference: genotype 2–4) | 2.51 | 1.18 | 0.0417 | |
| Staging F4 (reference: stage not 4) | 1.3 | 1.69 | 0.4500 | |
| Treatment (reference: before treatment) | 3.63 | 2.35 | 0.1321 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Androutsakos, T.; Tsantzali, I.; Karagiannakis, D.S.; Flevari, P.; Iakovou, D.; Pouliakis, A.; Kykalos, S.; Doris, S.; Xyla, V. Peripheral Neuropathy in Patients with Hepatitis C Infection—Reversibility after HCV Eradication: A Single Center Study. Viruses 2024, 16, 522. https://doi.org/10.3390/v16040522
Androutsakos T, Tsantzali I, Karagiannakis DS, Flevari P, Iakovou D, Pouliakis A, Kykalos S, Doris S, Xyla V. Peripheral Neuropathy in Patients with Hepatitis C Infection—Reversibility after HCV Eradication: A Single Center Study. Viruses. 2024; 16(4):522. https://doi.org/10.3390/v16040522
Chicago/Turabian StyleAndroutsakos, Theodoros, Ioanna Tsantzali, Dimitrios S. Karagiannakis, Pagona Flevari, Despoina Iakovou, Abraham Pouliakis, Stylianos Kykalos, Stylianos Doris, and Vasileia Xyla. 2024. "Peripheral Neuropathy in Patients with Hepatitis C Infection—Reversibility after HCV Eradication: A Single Center Study" Viruses 16, no. 4: 522. https://doi.org/10.3390/v16040522