Measles Elimination: Identifying Susceptible Sub-Populations to Tailor Immunization Strategies

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Retrospective Seroprevalence Survey
2.2. Susceptibility Estimates from the Electronic Vaccination Registry
2.3. Reported Measles Cases in Tyrol
3. Results
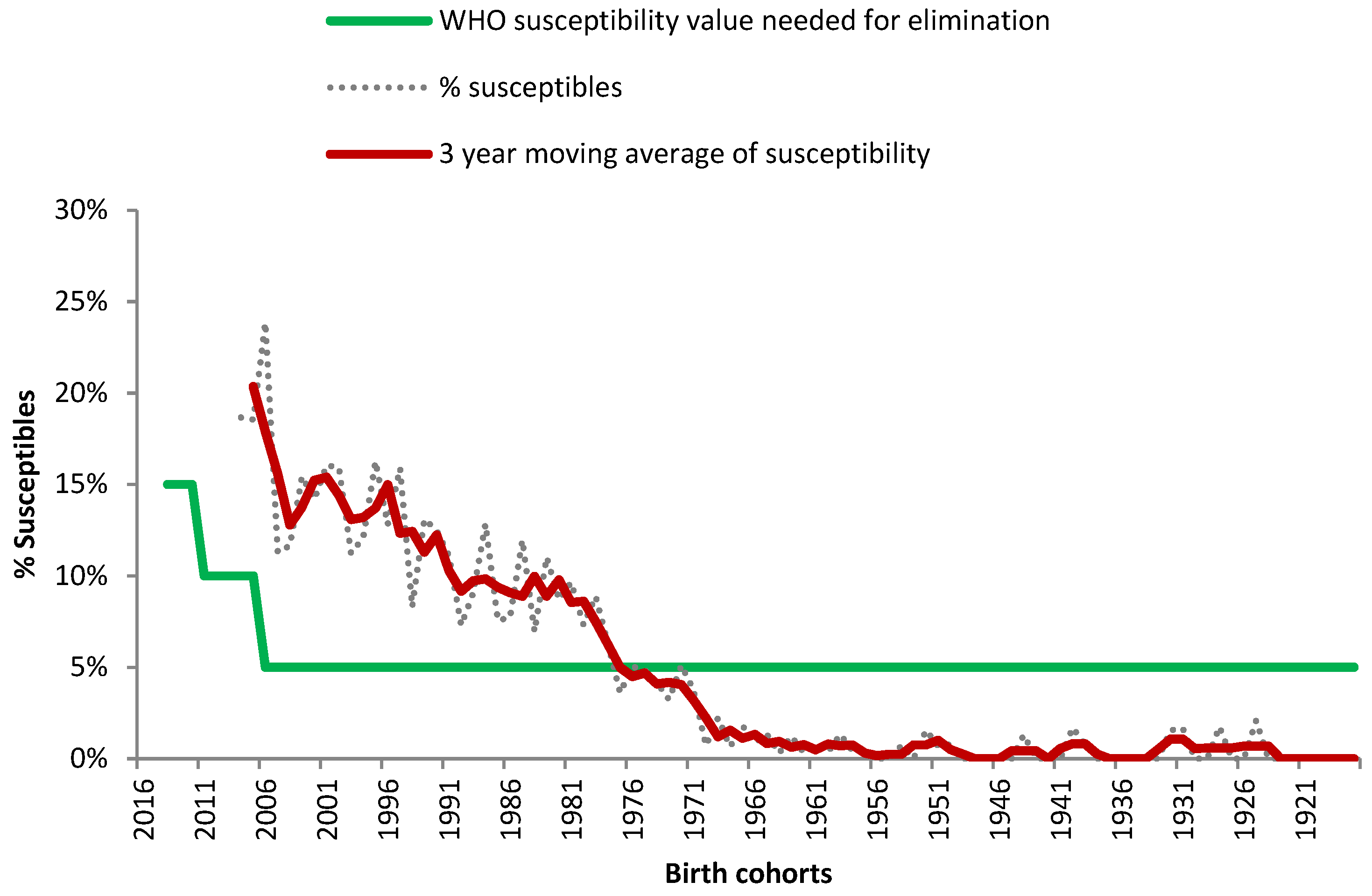
3.1. Retrospective Seroprevalence Survey
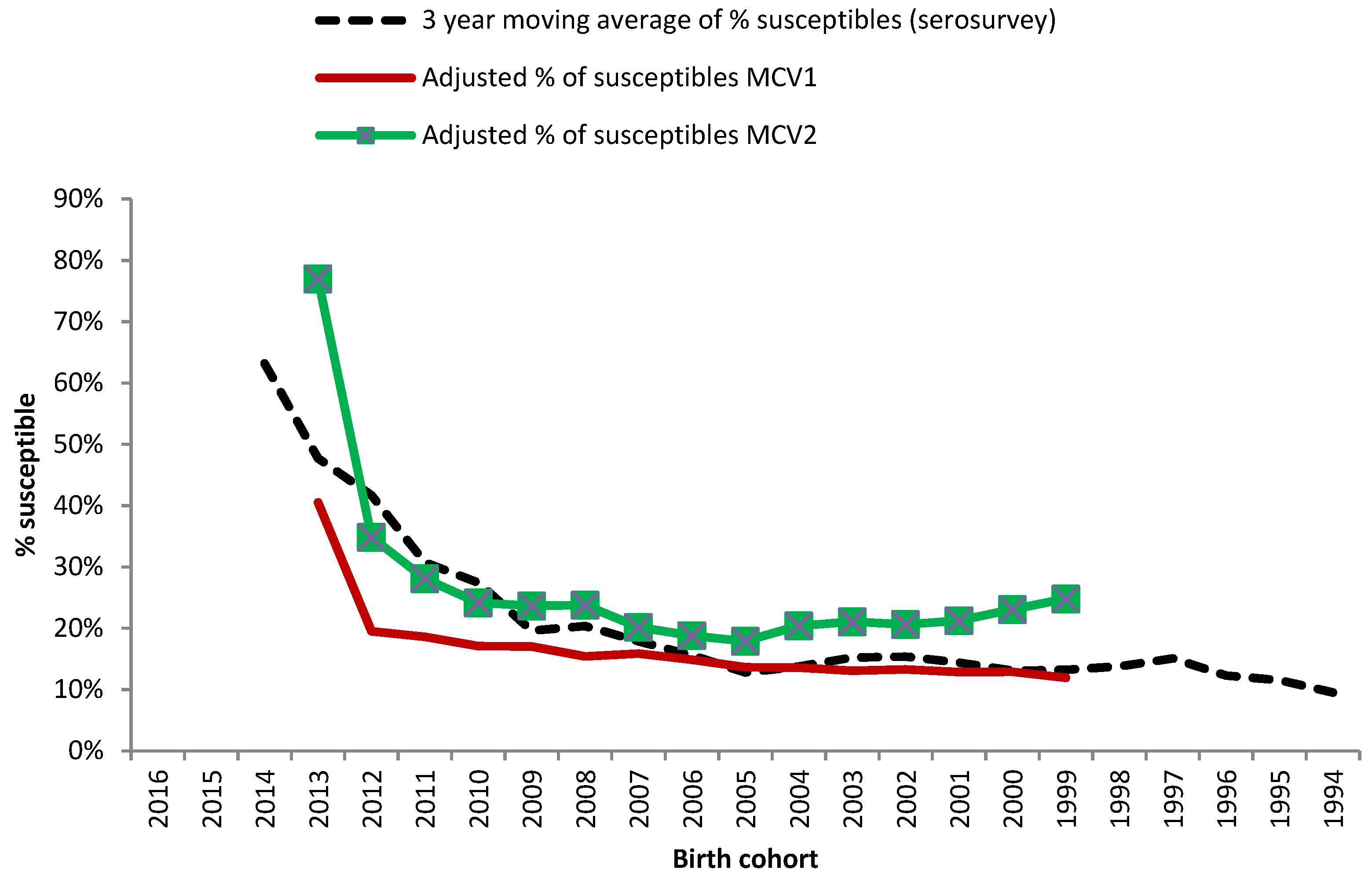
3.2. Coverage Data with Two Doses of Measles Containing Vaccine from the Tyrolean Electronic Vaccine Registry
3.3. Reported Cases of Measles in Tyrol
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zimmerman, L.A.; Muscat, M.; Singh, S.; Ben Mamou, M.; Jankovic, D.; Datta, S.; Alexander, J.P.; Goodson, J.L.; O’Connor, P. Progress toward measles elimination—European region, 2009–2018. MMWR. Morb. Mortal. Wkly. Rep. 2019, 68, 396–401. [Google Scholar] [CrossRef] [PubMed]
- WHO. Eliminating Measles and Rubella and Preventing Congenital Rubella. Who European Region Strategic Plan 2005–2010. Available online: http://www.euro.who.int/__data/assets/pdf_file/0008/79028/E87772.pdf (accessed on 19 May 2019).
- WHO. Measles-European Region. Available online: https://www.who.int/csr/don/06-may-2019-measles-euro/en/ (accessed on 24 July 2019).
- WHO. Ten Threats to Global Health in 2019. Available online: https://www.who.int/emergencies/ten-threats-to-global-health-in-2019 (accessed on 24 July 2019).
- WHO, R.O.f.E. The Guide to Tailoring Immunization Strategies. Available online: http://www.euro.who.int/__data/assets/pdf_file/0003/187347/The-Guide-to-Tailoring-Immunization-Programmes-TIP.pdf?ua=1 (accessed on 24 July 2019).
- de Melker, H.; Pebody, R.G.; Edmunds, W.J.; Levy-Bruhl, D.; Valle, M.; Rota, M.C.; Salmaso, S.; van den Hof, S.; Berbers, G.; Saliou, P.; et al. The seroepidemiology of measles in western europe. Epidemiol. Infect. 2001, 126, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Österreich, R. 114. Bundesgesetz: Nderung des Epidemiegesetzes von 1950. Available online: https://www.ris.bka.gv.at/Dokumente/Bundesnormen/NOR40185444/NOR40185444.rtf (accessed on 25 July 2019).
- Hendriks, J.; Blume, S. Measles vaccination before the measles–mumps–rubella vaccine. Am. J. Public Health 2013, 103, 1393–1401. [Google Scholar] [CrossRef]
- UNICEF, C.W. Measles and Rubella Initiative 2018. Available online: https://s3.amazonaws.com/wp-agility2/measles/wp-content/uploads/2018/02/2018-MRI-Factsheet.pdf (accessed on 25 July 2019).
- Schmid, D.; Holzmann, H.; Alfery, C.; Wallenko, H.; Popow-Kraupp, T.H.; Allerberger, F. Mumps outbreak in young adults following a festival in austria, 2006. Euro Surveill 2008, 13. [Google Scholar] [CrossRef]
- BMASGK. Impfplan Sterreich 2019. Available online: https://www.sozialministerium.at/cms/site/attachments/5/4/7/CH4062/CMS1546865142466/190211_impfplan_oesterreich_2019_web.pdf (accessed on 8 May 2019).
- BMASGK. Kurzbericht Masern. Available online: https://www.sozialministerium.at/cms/site/attachments/1/7/5/CH4062/CMS1540470756902/kurzbericht_masern_2018_version_1.1.pdf (accessed on 24 July 2019).
- Austria, S. Bevölkerung. Available online: http://www.statistik-austria.at/web_de/statistiken/menschen_und_gesellschaft/bevoelkerung/index.html (accessed on 8 February 2019).
- Österreich, G. Tiroler Gesundheitsbericht 2012. Available online: https://www.tirol.gv.at/fileadmin/themen/gesundheit-vorsorge/influenza/downloads/TLGB2012.pdf (accessed on 8 July 2019).
- Europe, W.R.O.f. Guidance on Conducting Serosurveys in Support of Measles and Rubella Elimination in the Who European Region. Available online: http://www.euro.who.int/__data/assets/pdf_file/0011/236648/Guidance-on-conducting-serosurveys-in-support-of-measles-and-rubella-elimination-in-the-WHO-European-Region.pdf (accessed on 4 December 2019).
- BMG. Nationaler Aktionsplan Masern-/Röteln-Elimination. Available online: http://www.bmgf.gv.at/cms/home/attachments/8/1/7/CH1472/CMS1366715694431/nap_masernroeteln_langfassung_20130522.pdf (accessed on 8 July 2019).
- BMGF. Häufige Fragestellung in Bezug auf das Epidemiologische Meldesystem (ems). Available online: https://www.sozialministerium.at/cms/site/attachments/2/9/9/CH4059/CMS1491916792014/haeufigefragenems.pdf (accessed on 24 July 2019).
- Carrillo-Santisteve, P.; Lopalco, P.L. Measles still spreads in europe: Who is responsible for the failure to vaccinate? Clin. Microbiol. Infect. 2012, 18 (Suppl. 5), 50–56. [Google Scholar] [CrossRef] [PubMed]
- Colzani, E.; McDonald, S.A.; Carrillo-Santisteve, P.; Busana, M.C.; Lopalco, P.; Cassini, A. Impact of measles national vaccination coverage on burden of measles across 29 member states of the european union and european economic area, 2006–2011. Vaccine 2014, 32, 1814–1819. [Google Scholar] [CrossRef] [PubMed]
- Boyce, T.; Gudorf, A.; de Kat, C.; Muscat, M.; Butler, R.; Habersaat, K.B. Towards equity in immunisation. Euro. Surveill. 2019, 24, 1800204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoes, J.; Knol, M.J.; Mollema, L.; Buisman, A.; de Melker, H.E.; van der Klis, F.R.M. Comparison of antibody response between boys and girls after infant and childhood vaccinations in the netherlands. Vaccine 2019, 37, 4504–4510. [Google Scholar] [CrossRef] [PubMed]
- CDC. How Well does the mmr Vaccine Work. Available online: https://www.cdc.gov/vaccines/vpd/mmr/public/index.html (accessed on 25 July 2019).
- Moore, C.; Cottrell, S.; Hoffmann, J.; Carr, M.; Evans, H.; Dunford, L.; Lawson, H.; Brown, K.E.; Jones, R. Self-collected buccal swabs and rapid, real-time pcr during a large measles outbreak in wales: Evidence for the protective effect of prior mmr immunisation. J. Clin. Virol. 2015, 67, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Pillsbury, A.; Quinn, H. An assessment of measles vaccine effectiveness, australia, 2006–2012. West. Pac. Surveill. Response J. WPSAR 2015, 6, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Kreidl, P.; de Kat, C. Utilization and impact of european immunization week to increase measles, mumps, rubella vaccine uptake in austria in 2016. Vaccine 2017, 35, 4836–4839. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Birth Cohorts | Age Groups | N Participants | % |
|---|---|---|---|
| 2016–2013 | 24 months to 4 years | 45 | 0.3 |
| 2012–2008 | 5 to 9 years | 331 | 2.5 |
| 2007–2003 | 10 to 14 years | 733 | 5.6 |
| 2002–1993 | 15 to 24 years | 1780 | 13.6 |
| 1992–1978 | 25 to 39 years | 2701 | 20.7 |
| 1997–1958 | 40 to 59 years | 4186 | 32.1 |
| 1957–1917 | 60+ years | 3284 | 25.2 |
| TOTAL | 13,060 | 100 |
| Birth Cohorts | Age Groups | % Susceptible | Maximum WHO Recommended Value |
|---|---|---|---|
| 2014–2013 | 24 months to 4 years | 60.0 | 15 |
| 2012–2008 | 5 to 9 years | 23.9 | 10 |
| 2007–2003 | 10 to 14 years | 14.9 | 5 |
| 2002–1993 | 15 to 24 years | 13.0 | 5 |
| 1992–1978 | 25 to 39 years | 8.8 | 5 |
| 1997–1958 | 40 to 59 years | 1.9 | 5 |
| 1957–1917 | 60+ years | 0.4 | 5 |
| Total | 5.9 |
| Year of Reporting | Number of Cases |
|---|---|
| 2003 | 2 |
| 2004 | - |
| 2005 | 2 |
| 2006 | 2 |
| 2007 | 2 |
| 2008 | 14 |
| 2009 | 2 |
| 2010 | 1 |
| 2011 | 16 |
| 2012 | 3 |
| 2013 | 15 |
| 2014 | 14 |
| 2015 | 3 |
| 2016 | 3 |
| 2017 | 10 |
| 2018 | 1 |
| 2019 | 9 |
| Total | 99 |
| District | Mean Population 1996–2016 | Proportion Susceptibles | Number of Cases | Mean Annual Incidence (2009–2019 *) Cases per 1,000,000 Inhabitants |
|---|---|---|---|---|
| Imst | 56,073 | 5.0% | 4 | 6.74 |
| Innsbruck Land | 164,010 | 5.6% | 13 | 7.49 |
| Innsbruck Stadt | 116,202 | 6.0% | 17 | 13.82 |
| Kitzbühel | 69,991 | 8.6% | 15 | 20.25 |
| Kufstein | 99,433 | 6.9% | 19 | 18.06 |
| Landeck | 44,092 | 6.9% | 0 | 0.00 |
| Lienz | 49,783 | 7.2% | 2 | 3.80 |
| Reutte | 31,729 | 5.4% | 5 | 14.89 |
| Schwaz | 78,303 | 5.8% | 2 | 2.32 |
| Total | 709,616 | 77 | 9.86 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kreidl, P.; Ammerer, D.; Würzner, R.; Luckner Hornischer, A.; von Laer, D.; Borena, W. Measles Elimination: Identifying Susceptible Sub-Populations to Tailor Immunization Strategies. Viruses 2019, 11, 765. https://doi.org/10.3390/v11080765
Kreidl P, Ammerer D, Würzner R, Luckner Hornischer A, von Laer D, Borena W. Measles Elimination: Identifying Susceptible Sub-Populations to Tailor Immunization Strategies. Viruses. 2019; 11(8):765. https://doi.org/10.3390/v11080765
Chicago/Turabian StyleKreidl, Peter, David Ammerer, Reinhard Würzner, Anita Luckner Hornischer, Dorothee von Laer, and Wegene Borena. 2019. "Measles Elimination: Identifying Susceptible Sub-Populations to Tailor Immunization Strategies" Viruses 11, no. 8: 765. https://doi.org/10.3390/v11080765
APA StyleKreidl, P., Ammerer, D., Würzner, R., Luckner Hornischer, A., von Laer, D., & Borena, W. (2019). Measles Elimination: Identifying Susceptible Sub-Populations to Tailor Immunization Strategies. Viruses, 11(8), 765. https://doi.org/10.3390/v11080765