Norovirus Infections and Disease in Lower-Middle- and Low-Income Countries, 1997–2018


Department of Medical Virology, Faculty of Health Sciences, University of Pretoria; Pretoria 0001, South Africa
Viruses 2019, 11(4), 341; https://doi.org/10.3390/v11040341
Submission received: 21 March 2019
/
Revised: 5 April 2019
/
Accepted: 8 April 2019
/
Published: 10 April 2019
(This article belongs to the Special Issue Noroviruses)
Abstract
:Noroviruses are a major cause of viral gastroenteritis. The burden of the norovirus in low-resource settings is not well-established due to limited data. This study reviews the norovirus prevalence, epidemiology, and genotype diversity in lower-middle-income countries (LMIC) and in low-income countries (LIC). PubMed was searched up to 14 January 2019 for norovirus studies from all LIC and LMIC (World Bank Classification). Studies that tested gastroenteritis cases and/or asymptomatic controls for norovirus by reverse transcription-polymerase chain reaction (RT-PCR) were included. Sixty-four studies, the majority on children <5 years of age, were identified, and 14% (95% confidence interval; CI 14–15, 5158/36,288) of the gastroenteritis patients and 8% (95% CI 7–9, 423/5310) of healthy controls tested positive for norovirus. In LMIC, norovirus was detected in 15% (95% CI 15–16) of cases and 8% (95% CI 8–10) of healthy controls. In LIC, 11% (95% CI 10–12) of symptomatic cases and 9% (95% CI 8–10) of asymptomatic controls were norovirus positive. Norovirus genogroup II predominated overall. GII.4 was the predominant genotype in all settings, followed by GII.3 and GII.6. The most prevalent GI strain was GI.3. Norovirus causes a significant amount of gastroenteritis in low-resource countries, albeit with high levels of asymptomatic infection in LIC and a high prevalence of coinfections.
1. Introduction
Noroviruses are a major cause of sporadic and epidemic gastroenteritis worldwide [1]. Severe disease is most often observed in young children (<5 years of age) [2], the elderly population (>65 years of age) [3], and immunocompromised individuals [4]. Noroviruses form a genus of the Caliciviridae family and are divided into at least seven genogroups (GI–GVII) [5]. Of these GI, GII, and GIV infect humans, with GII detected most frequently in clinical surveillance studies throughout the world [6]. The genogroups are subdivided in >30 genotypes. The predominant strain causing both outbreaks and sporadic cases of gastroenteritis is GII.4 [7,8]. Novel variants of GII.4 emerge periodically, spread rapidly across the globe, and cause pandemics [9]. Recently, other genotypes such as GII.17 and GII.2 have emerged and have become predominant in certain regions of the world [10,11]. A comprehensive understanding of the global burden of norovirus illness as well the genotype diversity, dominant strains, and strain replacement patterns is essential for a successful vaccine design [12].
In 2008, Patel and colleagues estimated the global norovirus prevalence at 12% (95% CI 10–15) based on 31 studies published between January 1990 and February 2008 [13]. More recently, the norovirus prevalence was estimated at 18% (95% CI 17–19) based on 175 studies spanning January 2008 to March 2014 [1]. Norovirus-associated infections are estimated to annually cause 677 million cases of disease and approximately 200,000 deaths globally [14]. The majority of these deaths occur in low-resource countries. Several systematic reviews have reported the prevalence of the norovirus in specific regions such as Latin America (15%; 95% CI 13–18) [15,16], China (19.8%–21.0%) [17], the Middle East and North Africa (MENA) (15.3%—median infection rate) [18], and 46 low-resource (developing) countries (17%; 95% CI 15–18) [19].
On the whole, there is still a lack of data on the norovirus prevalence in low-income countries (LIC). The World Bank classifies countries into one of four categories (high income countries, upper-middle-income countries (UMIC), lower-middle-income countries (LMIC), and LIC) based on their annual gross national incomes. The majority of data used to estimate global norovirus prevalence emanated from studies performed in high- and upper-middle-income countries [1,13,19]. In recent years, there has been an increase in studies from low-resource settings [20,21,22,23,24,25,26,27,28], reflecting a growing awareness of the importance of noroviruses as enteropathogens. Studies on the burden of norovirus are complicated by the frequent occurrence of asymptomatic infections [29], a significant proportion of norovirus disease that manifests with vomiting only symptoms [30], and a high prevalence of coinfections with other gastroenteritis pathogens [31].
The Etiology, Risk Factors, and Interactions of Enteric Infections and Malnutrition and the Consequences for Child Health and Development (MAL-ED) cohort study evaluated the aetiology of diarrhoea in children 0–2 years old in community settings in eight low-resource locations [32]. Molecular diagnostic assays were used to screen 6625 diarrhoeal and 30,968 control stools from 1715 children for 29 enteropathogens [33]. Viral diarrhoea was found to be more common than bacterial diarrhoea, and ten pathogens were responsible for 95% of diarrhoeal diseases. Norovirus was among the top ten pathogens and was found to cause 15.4 attributable diarrhoea episodes per 100 child-years, 95% CI 13.5–20.1, with the highest incidence in children <11 months of age. Another study utilized the Global Rotavirus Surveillance Network to investigate the aetiology of severe acute watery diarrhoea [34]. Operario and coworkers screened 878 acute watery diarrhoeal samples collected from children <5 years of age from 16 countries (8 LIC, 5 LMIC, and 3 UMIC) for multiple pathogens by polymerase chain reaction (PCR). Norovirus GII was the third most commonly detected pathogen after rotavirus and enteroaggregative E. coli with an overall attributable fraction of 6.2 (95% CI 2.8–9.2). These studies show that noroviruses are important pathogens globally, but there is still a need for more data on the prevalence and diversity of noroviruses in LICs.
This review focused on studies published between 1997 and 2018 on norovirus prevalence, epidemiology, and diversity in LIC and LMIC and includes 64 studies of which 17 (5 LIC and 12 LMIC) were published after March 2016 and have not been included in previous systematic reviews. The aim of the study is to review the norovirus prevalence in symptomatic and asymptomatic cases; to identify the predominant genotype circulating in LIC and LMIC; and to summarise the clinical features, seasonality, and pathogen coinfections of norovirus infections in low-resource settings.
2. Methods
2.1. Search Strategy and Inclusion Criteria
The PubMed database was searched up to 14 January 2019 with the following search terms: “norovirus”, “calicivirus”, and “Caliciviridae” in combination with the names of each of the LIC (34) and LMIC (47) countries as defined by the June 2018 World Bank list of economies [35]. The search filter was set to exclude hits containing the term “outbreak” or “outbreaks” in the title (see Supplementary File 1), since the review was aimed at sporadic norovirus disease. Only studies published in English were considered. Studies were included if they detected the norovirus with reverse transcription (RT)-PCR-based methods in individuals with acute gastroenteritis symptoms and/or asymptomatic control groups or populations. No limitations were set on the study size, duration, or age group of the study population. Studies which reported on norovirus detection in consecutive samples of cases and/or controls were excluded.
2.2. Data Extraction
The following information was extracted from each included study: First author; year of publication; study duration; study setting (i.e., inpatient or outpatient/community); age group; number of cases screened; number of cases positive for the norovirus; number of control subjects screened for the norovirus; number of control subjects positive for the norovirus; age information for norovirus positive cases and controls; number of norovirus GI, GII, and GIV detections if available; clinical symptoms associated with norovirus detection; coinfections with other pathogens; genotype information; and data on seasonality. Where GenBank accession numbers were provided, the sequences were analysed by the online norovirus genotyping tool (https://www.rivm.nl/mpf/typingtool/norovirus/) to confirm the genotypes. The data was stratified according to LIC and LMIC, hospitalized and outpatient/community groups, combined inpatient and outpatient data, age groups of 0–<5 years, 0–18 years, mixed ages, and asymptomatic infections including all age groups.
2.3. Statistical Analysis
The web-based open-source statistical calculator OpenEpi version 3 (https://www.openepi.com) was used to calculate the 95% confidence intervals for proportions [36]. Statistically significant differences between the norovirus proportions in different settings were compared with a z-test using EpiTools epidemiological calculators (http://epitools.ausvet.com.au/content.php?page=z-test-2).
3. Results
The PubMed literature search identified 352 articles, of which 331 titles and abstracts were screened for possible inclusion. Two hundred and twenty-five nonrelevant articles were excluded, and 106 full text articles were evaluated for inclusion. Forty-two of the 106 articles were excluded for reasons listed in Figure 1. Sixty-four studies were included in the review of the norovirus prevalence. Forty-three studies, in total, were included for a norovirus genotype analysis. Of these, 37 were studies that reported both the prevalence and genotype data, and 6 were studies that reported the genotyping data from noroviruses detected in pathogen-negative specimens (Figure 1).
Sixty-four studies representing eight LIC (15 studies) and 21 LMIC (49 studies) (see Supplementary File 1) were included in the review of the norovirus prevalence (Figure 2). Additional studies from countries which tested rotavirus-negative specimens for noroviruses were included in the world map with their respective norovirus prevalence. The median size of the study populations in LIC was 250, and studies ranged from very small (48 participants) to large (2678 participants). Studies in LMIC had a median sample size of 265 and ranged from 34 to 2495 participants. The majority of LMIC studies were from India (13), Vietnam (7), and Bangladesh (5), whereas between one to three studies from each LIC were included.
3.1. Norovirus Prevalence in LIC and LMIC
Overall, across all age groups in LIC and LMIC, norovirus was detected in 14% (95% CI 14–15) of individuals with gastroenteritis symptoms and in 8% (95% CI 7–9) of asymptomatic controls. Norovirus was detected more frequently in symptomatic cases of gastroenteritis in LMIC (15%; 95% CI 15–16, range 0–43%) than in LIC (11%; 95% CI 11–12, range 6–42%) (Table 1). In asymptomatic controls, noroviruses were detected in 9% (CI 8–10, range 3–12%) in LIC and in 8% (CI 7–9, range 0–19%) in LMIC studies. In both the LIC and LIMC settings, there was a statistically significant difference in the norovirus prevalence between children (<5 years of age) that were hospitalized (LMIC: 17% CI 17–18; LIC: 11% CI 10–12) and nonhospitalized children (outpatients/community) (LMIC: 12% CI 10–14; LIC: 9% CI 8–11; LMIC p < 0.0001 and LIC p = 0.0058).
From 37 studies in children <5 years of age, norovirus was detected most frequently in children <1 year of age in five studies and in children <2 years of age in 16 studies. An additional 10 studies reported the median age of the norovirus-positive population, ranging between 6–15.5 months of age.
The prevalence of norovirus GI in relation to GII was similar in symptomatic infections in both settings (Table 2). The increased detection of norovirus GI was reported in asymptomatic controls in both LIC and LMIC (21.6% and 24% vs. 12% and 13% in symptomatic cases). Only three studies from Bangladesh screened stool specimens for norovirus GIV, and this genogroup represented 3% of the norovirus positives in these studies.
3.2. Norovirus Clinical Features
Most of the studies that presented data on clinical symptoms reported vomiting, fever, and abdominal pain in patients with diarrhoea. In 20 studies, the percentage of patients with vomiting ranged between 37.5% and 92%, with a median of 68%. There was a larger variation in the number of patients with fever. Within 16 studies, the percentage of patients with a fever ranged from 5% to 84%, with a median of 46%. Abdominal pain was reported in six studies, and the median percentage of patients with this symptom was 57% (ranging from 46% to 65%). Since data was not provided on the combination of symptoms in patients, it is not possible to estimate how often these symptoms occur as single symptoms or in combination. Six studies reported severe dehydration in the following percentages of single norovirus infections, 15.5% [26], 18.9% [77,97], 19% [48], 19.4% [38], and 30.3% [71]. Mild dehydration was observed in a larger number of the patients, 37.8% [97] and 60% [26]. Some studies categorised dehydration as moderate to severe and reported between 2.9% and 38% of patients with this level of dehydration.
3.3. Norovirus and Coinfections
The studies included in this review that reported on coinfections of norovirus with other gastroenteritis pathogens can be divided into three types: (a) studies that tested for norovirus and rotavirus (n = 12); (b) studies that tested for a range of gastroenteritis viruses (n = 12); and (c) studies that tested for enteric viruses, bacterial pathogens, and/or parasites (n = 8). Figure 3 provides an overview of the norovirus coinfections described in 26 studies from 15 LMIC and 6 studies from 4 LIC. Overall, these studies detected the norovirus in 2899 cases, of these 2131 (73.5%) were single norovirus infections and 768 (26.5%) were coinfections with various gastroenteritis pathogens. The majority were norovirus/rotavirus coinfections (18.3%), and 8.2% represented coinfections with other pathogens. The percentage of coinfections detected in the different studies ranged from 5% to 76.7%, with a median of 26.7%.
3.4. Norovirus Seasonality
The LIC and LMIC in this review are generally located in the tropical or subtropical regions of the world. Thirty-eight of the LMIC studies and seven LIC studies reported data on seasonality. In the majority of studies, norovirus was detected throughout the year with peaks of norovirus activity varying between months or seasons. To determine seasonal trends, the studies were grouped into the following geographical regions: Asia, Southeast Asia, North Africa/Middle East, West Africa, East Africa, and Central and South America. However, no clear seasonality was apparent from the different studies when grouped into these regions. Two studies in Nicaragua both reported a peak in norovirus detection during the early rainy season in June and July [21,77]. The three countries that published multiple norovirus studies are Bangladesh, India, and Vietnam. One Bangladesh study [28] reported norovirus detection throughout the year, with a peak in the hot summer months of March to April. The second Bangladesh study spanned three years and reported a slightly higher detection rate in the winter and summer seasons compared to the rainy season [29]. Another Bangladesh study performed between October 2004 and September 2005 detected a peak of norovirus activity between January and March 2004, which corresponded to the cooler months of the year [37]. No clear trend is discernable from these studies. A two-year study in western India by Chhabra and coworkers [54] showed a peak of norovirus detection in March, which coincided with decreased humidity, minimal rainfall, and higher temperatures. The other studies from India did not provide clear data on seasonality. Three studies from southern Vietnam reported peak norovirus detection in the rainy season [89,98] or towards the end of the season [99]. According to Tra My and colleagues there was a positive linear correlation between rainfall and norovirus infections [98].
3.5. Norovirus Genotype Diversity
Norovirus genotypes are classified with a phylogeny-based dual-typing system using partial polymerase and complete capsid nucleotide sequences (i.e., GII.Pe/GII.4) [100]. Overall, 37/64 studies reported norovirus capsid genotyping data (Supplementary File 1). An additional six studies with capsid genotyping data were included in the genotype diversity analysis. These were excluded from the prevalence review because only rotavirus-negative stool specimens were screened [87,88,99,101,102,103]. Ten out of 15 LIC studies from six countries included in the review reported norovirus genotyping data (Figure 4a). The studies were conducted between 1997 and 2013, and 30 genotypes (9 GI, 1 unassigned GI and 20 GII) were described, with GII.4 having the widest distribution (6 countries) followed by GI.3, GII.2, and GII.6 that were reported from 5 countries. Norovirus GI.5, GII.3, GII.10, and GII.14 were detected in four countries. The genotypes that were found in three countries were GI.4, GI.7, GII.7, GII.16, and GII.17.
Norovirus genotyping data were reported in 27/49 LMIC studies from 14 countries (Figure 4b). These studies were published between 2004 and 2018 and represent a range of timeframes between 1997–2015. Overall, 28 genotypes (9 GI, 19 GII) were circulating in the LMIC. As with LIC, GII.4 was detected in all of the countries (14), with GII.2 and GII.3 being the next most widely distributed genotypes reported in 11 countries; GII.6 was identified in 10 countries, GII.1 in 9 countries, and GII.7, GII.14 and GII.16 were identified in 8 countries.
Overall, the most common and widely distributed genogroup I strain was GI.3 followed by GI.7, GI.5, GI.2, and GI.1. Among the genogroup II strains, GII.4 was the most frequently detected in a total of 1490 cases (250 LIC and 1240 LMIC), with GII.3 as the second most dominant strain identified in 389 cases. The other strains that were detected in multiple countries in at least 50 cases are GII.6, GII.2, GII.21, GII.13, and GII.1.
Norovirus GII.4 variants are distinguished based on a phylogenetic analysis of the complete capsid gene [100]. New variants are recognised once they have been established in at least two separate geographic locations [100]. Fourteen different norovirus GII.4 variants were reported between 1997 and 2015 in LIC and LMIC (Figure 5). In LIC, Yerseke 2006a, Osaka 2007, New Orleans 2009, and Sydney 2012 represented the majority of variants. In LMIC, Hunter 2004, Den Haag 2006b, New Orleans 2009, and Sydney 2012 were the most frequently reported.
4. Discussion
The World Bank list of economies classified 81 countries as LMIC and LIC in June 2018. Of these, 29 were represented in this review of norovirus prevalence and diversity in low-resource countries. Overall, 36,288 symptomatic gastroenteritis cases were tested for norovirus in 64 studies over a period of 19 years. Twenty-three of the 64 studies tested 5310 healthy controls for norovirus. Across all ages, norovirus was detected in 14% (95% CI 14–15, 5158/36288) of symptomatic cases and in 8% (95% CI 7–9, 423/5310) of healthy control subjects. This correlates with previous global prevalence estimates of 14% (95% CI 11–16) in symptomatic cases in high-mortality developing countries and 7% (95% CI 3–10) in asymptomatic controls [1]. When countries were grouped according to income, norovirus was detected across all ages in 11% (95% CI 11–12) of symptomatic cases and 9% (95% CI 8–10) of asymptomatic controls in LIC. The detection rate for both symptomatic and asymptomatic norovirus infections in LIC was higher than the 6% (95% CI 3–10) and 5% (95% CI 4–8) estimated previously [19]. This is likely due to the additional data included in this review. The five studies from LIC that were published since 2016 had a mean norovirus prevalence of 15% and contributed 224/1455 norovirus positive cases to the current review. This may also reflect the improved detection via quantitative RT-PCR, as four of the five studies used quantitative versus qualitative RT-PCR [20,22,27,81], which was used in many earlier studies in LIC. In the current review, norovirus was detected in LMIC in 15% (95% CI 15–16) of symptomatic cases and 8% (95% CI 7–9) of healthy controls. The percentage of norovirus detected overall in symptomatic cases correlates well with previous estimates in LMIC (15%; 95% CI 13–18) [19], in Latin America (15%; 95% CI 13–18) [15], and in MENA countries (15.3% median) [18]. The asymptomatic detection rate of 8% is comparable to the previous LMIC (5%; 95% CI 3–10) [19] and Latin American (8%; 95% CI 4–13) estimates [15]. These data are in agreement with a seroepidemiological study in Uganda [104], which detected norovirus antibodies in 77% of children by 1 year of age and in 99% of two-year old children and strongly suggest that the rate of asymptomatic infections in infancy and early childhood is high in low-resource settings.
More than half of the included studies screened for noroviruses in children <5 years of age. Due to the relatively small number of outpatients and patients in community settings, these groups were combined and compared with hospitalized children. In LIC, 11% (95% CI 10–12) of inpatient children tested positive for norovirus, whereas 9% (95% CI 8–11) of outpatients tested positive (Table 1). In LMIC, a larger difference was observed with a 17% (95% CI 17–18) norovirus detection in inpatients <5 years of age and only 12% (95% CI 10–14) in outpatients of the same age. Both differences were statistically significant. In contrast, Ahmed and coworkers [1] found that the norovirus prevalence was higher in community (24%; 95% CI 18–30) and outpatient (20%; 95% CI 16–24) settings, compared to inpatients (17%; 95% CI 15–19). Their study included a smaller number of studies from low-resource countries and were classified according to mortality rates rather than income, which may explain the differences. In Latin America, the norovirus prevalence was comparable between inpatients (16%; 95% CI 12–21) and outpatients (14%; 95% CI 10–19) and in the community (15%; 95% CI 13–18) [15].
Norovirus GII was the predominant genogroup detected in all studies in LIC and LMIC. Similar GI and GII distributions were reported (GI/GII/mixed: 12/87/0.9, 13/83/3) in symptomatic infections. Only three studies in Bangladesh screened for GIV and detected it at approximately 3% of gastroenteritis cases. Norovirus GI occurred more frequently in the asymptomatic control population in both LIC (22:78 GI:GII) and LMIC (24:73 GI:GII). This correlates with norovirus-specific data from the MAL-ED study [105] which showed that GII infections had an 85% increased odds of being symptomatic compared to GI infections.
The inclusion criteria for 87% of the LMIC studies were the classic diarrhoea definition of ≥3 loose stools in the last 24 h. The clinical features of norovirus infections, in addition to diarrhoea, reported most often were vomiting and fever. Seven studies added “with or without vomiting” to their definition of gastroenteritis, but only one study stated vomiting only cases in addition to diarrhoeal cases in their inclusion criteria. Therefore, as with the majority of norovirus surveillance studies, vomiting only cases were missed, which suggests that the prevalence of the norovirus might be underestimated. The classification of dehydration varied between studies, and since few actually reported on dehydration, it is not possible to estimate the overall level of dehydration that norovirus infections caused in the LIC and LMIC settings. Six studies reported severe dehydration in 15–30% of single norovirus positive cases, and mild dehydration was observed in up to 60% of norovirus infections in a recent study in Cameroon [26]. Four studies provided comparative data on dehydration for norovirus and rotavirus. In two of these, rotavirus caused dehydration in a higher percentage of patients (64% vs. 18.9% [77] and 56% vs. 30% [71]) than norovirus. In a study in Ethiopia, norovirus caused dehydration in 19% of single norovirus infections compared to only 5% of rotavirus infections that led to severe dehydration [48]. Another study in Zambia reported comparable levels of mild and moderate dehydration for patients infected with rotavirus or norovirus but no severe dehydration [96]. Thus, the limited available data suggest that norovirus could display an increased severity in some settings, but in general, rotavirus causes a more severe disease.
With the advent of multiplex testing for large pathogen panels, widespread coinfections with enteropathogens have been observed in many studies [68,106,107,108]. Approximately a third of the studies (11/32) that reported coinfections in this review tested only for rotavirus and norovirus. Thus, the median of 26.7% coinfections is most likely an underestimation, since the percentage of coinfections will increase with the testing of more pathogens. Another third of the studies (12/32) tested for additional enteric viruses, and among these, six studies still only detected norovirus/rotavirus coinfections. One study from India [52] that tested for a large panel of pathogens also only detected norovirus and rotavirus infections and coinfections. In three studies, one on hospitalized neonates in India [60] and two others in India [55] and Pakistan [79], the rotavirus coinfections equaled or exceeded the single norovirus infections. The highest percentage of coinfections were detected in studies from Burkina Faso (65.5%, [27]), India (77%, [60]), and Tunisia (74.2%, [88]). Two recent studies on coinfections in diarrhoeal disease based on symptomatic and asymptomatic study populations from Rwanda and Zanzibar [109] and Tanzania [31] detected 65% and 58.1% of coinfections in symptomatic cases. Andersson and coworkers [109] found a negative association (coinfections less common than expected from probability) between rotavirus and norovirus GII in symptomatic patients. Statistically, pathogens that independently cause diarrhoea are expected to be negatively associated in symptomatic patients [109]. The other study reported four pathogens, rotavirus, norovirus GII, Cryptosporidium, and Shigella species/EIEC to be associated with diarrhoea in both mono-infections and coinfections [31]. Both these studies provide evidence for norovirus GII as a pathogen that causes diarrhoea in both mono- and coinfections.
In the northern hemisphere, norovirus has a very clear winter seasonality [110]; however, in other regions of the world, the seasonality is less well-defined. In this review, two countries, Nicaragua and Vietnam, reported a peak norovirus detection during the rainy season. Bucardo and colleagues provided data from Nicaragua between 1999 and 2015 that showed a clear peak of norovirus detection in June and July [21]. Furthermore, a one-year longitudinal study on norovirus in children <5 years of age in Nicaragua reported that norovirus infections peaked early in the rainy season (April–June) [111]. Data from Vietnam suggest that norovirus infections are positively correlated with rainfall, and three different studies detected norovirus peaks during the rainy season. In a systematic review on norovirus seasonality, Ahmed and coworkers found an association between norovirus season strength and average rainfall in the wettest month for outbreaks but not for sporadic cases [110]. Between 2002–2007 in Victoria, Australia, the norovirus outbreaks peaked approximately three months after the highest average rainfall [112]. The mechanism by which rainfall impacts on norovirus infections is not understood but may be linked with the environmental spread of the virus. Norovirus seasonal patterns are determined by complex factors, and it is clear that additional larger studies spanning several years are needed to understand seasonal distribution in tropical and subtropical low resource regions.
The norovirus genotype distribution in LIC and LMIC were very similar, with GII.4 overall detected at the highest frequency (1490/3233 typed strains) and with the widest distribution (20 countries). Norovirus GII.3 was clearly the second most prevalent genotype (389/3233 typed strains) and circulated in 15 countries. The third most prominent genotype was GII.6 (131/3233 typed strains), which was detected in 16 countries. Although GII.4 predominated in general, there were instances in Bhutan [41], Ethiopia [48], India [60], and Tunisia [86] where GII.3 was more prevalent than GII.4, and in 2001–2012, GII.21 was the most prevalent type detected in Bhutan [42]. Since the studies that form part of this review were performed between 1997 and 2015, the more recent emergence of novel GII.17 [11,113] and GII.2 [10] in LIC and LMIC could not be evaluated. Overall, the data correlate well with those reported by Hao-Tran and colleagues [8] in a review on the global distribution of norovirus genotypes in children with sporadic gastroenteritis, where GII.4 and GII.3 were the predominant genotypes circulating in children globally. The well-known predominance of GII.4 may be related to its ability to evade the immune system by the conformational occlusion of blockade antibody epitopes [114] and the variation in epitopes that allow an escape from immunity without impairing binding to cellular ligands [115]. There is a lack of genogroup I genotyping data globally, since GI strains are generally detected in less than 20% of sporadic norovirus cases. The 43 studies that reported genotypes from LIC and LMIC characterised 236 GI strains. The GI.3 strain predominated at 31% with GI.7 (15%), GI.2 (10%), and GI.1 (9%) among the other prevalent strains.
The GII.4 variant distribution differed slightly between LIC and LMIC; whereas New Orleans 2009 and Sydney 2012 were predominant in both settings, in LIC, Yerseke 2006a and Osaka 2007 were also commonly reported but Hunter 2004 and Den Haag 2006b were more prevalent in LMIC. These patterns may reflect the varying time frames of the different studies rather than the predominance of a particular variant in a certain region.
There are several limitations to this review since the studies were quite heterogeneous. In general, the studies had small population sizes and some were of a short duration, which specifically impacted the conclusions on seasonality. The level of reporting varied greatly between different studies; thus, a full picture of the clinical presentation and coinfection levels could not be obtained.
5. Conclusions
An improved understanding of the norovirus epidemiology in low-resource settings is essential for successful vaccine development and implementation of interventions to counter the detrimental consequences of multiple gastroenteritis episodes early in life. The recent data on norovirus detections in LIC and LMIC correlate with the earlier estimates on the norovirus prevalence in these settings and emphasizes that noroviruses are important pathogens in low-resource countries. The predominance of norovirus GII.4 and GII.3, at least in the paediatric population is very clear, with a great diversity of genotypes circulating at a low frequency. However, to date, there are molecular-based norovirus data available for only 29 out of 81 low-resource countries, and more studies from various regions and in different age groups are necessary to aid strategies to combat norovirus gastroenteritis.
Supplementary Materials
The following are available online at https://www.mdpi.com/1999-4915/11/4/341/s1.
Funding
This research received no external funding.
Acknowledgments
I would like to acknowledge Maureen Taylor and Walda van Zyl for the critical reading of the manuscript.
Conflicts of Interest
The author declares no conflict of interest.
References
- Ahmed, S.M.; Hall, A.J.; Robinson, A.E.; Verhoef, L.; Premkumar, P.; Parashar, U.D.; Koopmans, M.; Lopman, B.A. Global prevalence of norovirus in cases of gastroenteritis: A systematic review and meta-analysis. Lancet Infect. Dis. 2014, 14, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Riera-Montes, M.; O’Ryan, M.; Verstraeten, T. Norovirus and Rotavirus Disease Severity in Children: Systematic Review and Meta-analysis. Pediatr. Infect. Dis. J. 2018, 37, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, L.; Wolter, J.; De Coster, I.; Van Damme, P.; Verstraeten, T. A decade of norovirus disease risk among older adults in upper-middle and high income countries: A systematic review. BMC Infect. Dis. 2015, 15, 425. [Google Scholar] [CrossRef]
- Green, K.Y. Norovirus infection in immunocompromised hosts. Clin. Microbiol. Infect. 2014, 20, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Vinje, J. Advances in laboratory methods for detection and typing of norovirus. J. Clin. Microbiol. 2015, 53, 373–381. [Google Scholar] [CrossRef]
- Van Beek, J.; de Graaf, M.; Al-Hello, H.; Allen, D.J.; Ambert-Balay, K.; Botteldoorn, N.; Brytting, M.; Buesa, J.; Cabrerizo, M.; Chan, M.; et al. Molecular surveillance of norovirus, 2005–2016: An epidemiological analysis of data collected from the NoroNet network. Lancet Infect. Dis. 2018, 18, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Hasing, M.E.; Lee, B.E.; Qiu, Y.; Xia, M.; Pabbaraju, K.; Wong, A.; Tipples, G.; Jiang, X.; Pang, X.L. Changes in norovirus genotype diversity in gastroenteritis outbreaks in Alberta, Canada: 2012–2018. BMC Infect. Dis. 2019, 19, 177. [Google Scholar] [CrossRef]
- Hoa Tran, T.N.; Trainor, E.; Nakagomi, T.; Cunliffe, N.A.; Nakagomi, O. Molecular epidemiology of noroviruses associated with acute sporadic gastroenteritis in children: Global distribution of genogroups, genotypes and GII.4 variants. J. Clin. Virol. 2013, 56, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Siebenga, J.J.; Vennema, H.; Zheng, D.P.; Vinje, J.; Lee, B.E.; Pang, X.L.; Ho, E.C.; Lim, W.; Choudekar, A.; Broor, S.; et al. Norovirus illness is a global problem: Emergence and spread of norovirus GII.4 variants, 2001–2007. J. Infect. Dis. 2009, 200, 802–812. [Google Scholar] [CrossRef] [PubMed]
- Thongprachum, A.; Okitsu, S.; Khamrin, P.; Maneekarn, N.; Hayakawa, S.; Ushijima, H. Emergence of norovirus GII.2 and its novel recombination during the gastroenteritis outbreak in Japanese children in mid-2016. Infect. Genet. Evol. 2017, 51, 86–88. [Google Scholar] [CrossRef]
- Zhang, P.; Chen, L.; Fu, Y.; Ji, L.; Wu, X.; Xu, D.; Han, J. Clinical and molecular analyses of norovirus-associated sporadic acute gastroenteritis: The emergence of GII.17 over GII.4, Huzhou, China, 2015. BMC Infect. Dis. 2016, 16, 717. [Google Scholar] [CrossRef]
- Cortes-Penfield, N.W.; Ramani, S.; Estes, M.K.; Atmar, R.L. Prospects and Challenges in the Development of a Norovirus Vaccine. Clin. Ther. 2017, 39, 1537–1549. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.M.; Widdowson, M.A.; Glass, R.I.; Akazawa, K.; Vinje, J.; Parashar, U.D. Systematic literature review of role of noroviruses in sporadic gastroenteritis. Emerg. Infect. Dis. 2008, 14, 1224–1231. [Google Scholar] [CrossRef] [PubMed]
- Pires, S.M.; Fischer-Walker, C.L.; Lanata, C.F.; Devleesschauwer, B.; Hall, A.J.; Kirk, M.D.; Duarte, A.S.; Black, R.E.; Angulo, F.J. Aetiology-Specific Estimates of the Global and Regional Incidence and Mortality of Diarrhoeal Diseases Commonly Transmitted through Food. PLoS ONE 2015, 10, e0142927. [Google Scholar] [CrossRef]
- O’Ryan, M.; Riera-Montes, M.; Lopman, B. Norovirus in Latin America: Systematic Review and Meta-analysis. Pediatr Infect. Dis. J. 2017, 36, 127–134. [Google Scholar] [CrossRef]
- da Silva Polo, T.; Peiro, J.R.; Mendes, L.C.; Ludwig, L.F.; de Oliveira-Filho, E.F.; Bucardo, F.; Huynen, P.; Melin, P.; Thiry, E.; Mauroy, A. Human norovirus infection in Latin America. J. Clin. Virol. 2016, 78, 111–119. [Google Scholar] [CrossRef]
- Zhou, H.L.; Zhen, S.S.; Wang, J.X.; Zhang, C.J.; Qiu, C.; Wang, S.M.; Jiang, X.; Wang, X.Y. Burden of acute gastroenteritis caused by norovirus in China: A systematic review. J. Infect. 2017, 75, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Kreidieh, K.; Charide, R.; Dbaibo, G.; Melhem, N.M. The epidemiology of Norovirus in the Middle East and North Africa (MENA) region: A systematic review. Virol. J. 2017, 14, 220. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.T.; Phan, K.; Teng, I.; Pu, J.; Watanabe, T. A systematic review and meta-analysis of the prevalence of norovirus in cases of gastroenteritis in developing countries. Medicine (Baltimore) 2017, 96, e8139. [Google Scholar] [CrossRef] [PubMed]
- Bonkoungou, I.J.O.; Ouédraogo, N.; Tamini, L.; Teguera, R.K.; Yaméogo, P.; Drabo, M.K.; Medah, I.; Barro, N.; Sharma, S.; Svensson, L.; et al. Rotavirus and norovirus in children with severe diarrhea in Burkina Faso before rotavirus vaccine introduction. J. Med. Virol. 2018, 90, 1453–1460. [Google Scholar] [CrossRef] [PubMed]
- Bucardo, F.; Reyes, Y.; Becker-Dreps, S.; Bowman, N.; Gruber, J.F.; Vinjé, J.; Espinoza, F.; Paniagua, M.; Balmaseda, A.; Svensson, L.; et al. Pediatric norovirus GII.4 infections in Nicaragua, 1999–2015. Infect. Genet. Evol. 2017, 55, 305–312. [Google Scholar] [CrossRef]
- Cardemil, C.V.; Sherchand, J.B.; Shrestha, L.; Sharma, A.; Gary, H.E.; Estivariz, C.F.; Diez-Valcarce, M.; Ward, M.L.; Bowen, M.D.; Vinjé, J.; et al. Pathogen-Specific Burden of Outpatient Diarrhea in Infants in Nepal: A Multisite Prospective Case-Control Study. J. Pediatr. Infect. Dis. Soc. 2017, 6, e75–e85. [Google Scholar] [CrossRef]
- Esteves, A.; Nordgren, J.; Tavares, C.; Fortes, F.; Dimbu, R.; Saraiva, N.; Istrate, C. Genetic diversity of norovirus in children under 5 years of age with acute gastroenteritis from Angola. Epidemiol. Infect. 2018, 146, 551–557. [Google Scholar] [CrossRef]
- Hoa-Tran, T.N.; Nakagomi, O.; Dao, A.T.H.; Nguyen, A.T.; Agbemabiese, C.A.; Vu, H.M.; Nakagomi, T.; Thanh, N.T.H. Molecular epidemiology of noroviruses detected in Vietnamese children with acute gastroenteritis from 2012 to 2015. J. Med. Microbiol. 2017, 66, 34–45. [Google Scholar] [CrossRef]
- Horwood, P.F.; Soli, K.W.; Maure, T.; Naito, Y.I.; Morita, A.; Natsuhara, K.; Tadokoro, K.; Baba, J.; Odani, S.; Tomitsuka, E.; et al. A High Burden of Asymptomatic Gastrointestinal Infections in Traditional Communities in Papua New Guinea. Am. J. Trop. Med. Hyg. 2017, 97, 1872–1875. [Google Scholar] [CrossRef]
- Mugyia, A.E.; Ndze, V.N.; Akoachere, J.-F.T.K.; Browne, H.; Boula, A.; Ndombo, P.K.; Cannon, J.L.; Vinjé, J.; Ndip, L.M. Molecular epidemiology of noroviruses in children under 5 years of age with acute gastroenteritis in Yaoundé, Cameroon. J. Med. Virol. 2019, 91, 738–743. [Google Scholar] [CrossRef]
- Ouedraogo, N.; Ngangas, S.M.T.; Bonkoungou, I.J.O.; Tiendrebeogo, A.B.; Traore, K.A.; Sanou, I.; Traore, A.S.; Barro, N. Temporal distribution of gastroenteritis viruses in Ouagadougou, Burkina Faso: Seasonality of rotavirus. BMC Public Health 2017, 17, 274. [Google Scholar] [CrossRef]
- Rahman, M.; Rahman, R.; Nahar, S.; Hossain, S.; Ahmed, S.; Golam Faruque, A.S.; Azim, T. Norovirus diarrhea in Bangladesh, 2010–2014: Prevalence, clinical features, and genotypes. J. Med. Virol. 2016, 88, 1742–1750. [Google Scholar] [CrossRef]
- Hossain, M.E.; Rahman, R.; Ali, S.I.; Islam, M.M.; Rahman, M.Z.; Ahmed, S.; Faruque, A.S.G.; Barclay, L.; Vinje, J.; Rahman, M. Epidemiologic and Genotypic distribution of Noroviruses among children with Acute Diarrhea and Healthy Controls in a Low-income Rural Setting. Clin. Infect. Dis. 2018. [Google Scholar] [CrossRef]
- Kirby, A.E.; Streby, A.; Moe, C.L. Vomiting as a Symptom and Transmission Risk in Norovirus Illness: Evidence from Human Challenge Studies. PLoS ONE 2016, 11, e0143759. [Google Scholar] [CrossRef]
- Moyo, S.J.; Kommedal, Ø.; Blomberg, B.; Hanevik, K.; Tellevik, M.G.; Maselle, S.Y.; Langeland, N. Comprehensive Analysis of Prevalence, Epidemiologic Characteristics, and Clinical Characteristics of Monoinfection and Coinfection in Diarrheal Diseases in Children in Tanzania. Am. J. Epidemiol. 2017, 186, 1074–1083. [Google Scholar] [CrossRef]
- Platts-Mills, J.A.; Babji, S.; Bodhidatta, L.; Gratz, J.; Haque, R.; Havt, A.; McCormick, B.J.J.; McGrath, M.; Olortegui, M.P.; Samie, A.; et al. Pathogen-specific burdens of community diarrhoea in developing countries: A multisite birth cohort study (MAL-ED). Lancet Glob. Health 2015, 3, e564–e575. [Google Scholar] [CrossRef]
- Platts-Mills, J.A.; Liu, J.; Rogawski, E.T.; Kabir, F.; Lertsethtakarn, P.; Siguas, M.; Khan, S.S.; Praharaj, I.; Murei, A.; Nshama, R.; et al. Use of quantitative molecular diagnostic methods to assess the aetiology, burden, and clinical characteristics of diarrhoea in children in low-resource settings: A reanalysis of the MAL-ED cohort study. Lancet Glob. Health 2018, 6, e1309–e1318. [Google Scholar] [CrossRef]
- Operario, D.J.; Platts-Mills, J.A.; Nadan, S.; Page, N.; Seheri, M.; Mphahlele, J.; Praharaj, I.; Kang, G.; Araujo, I.T.; Leite, J.P.G.; et al. Etiology of Severe Acute Watery Diarrhea in Children in the Global Rotavirus Surveillance Network Using Quantitative Polymerase Chain Reaction. J. Infect. Dis. 2017, 216, 220–227. [Google Scholar] [CrossRef]
- The World Bank. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 9 December 2018).
- Sullivan, K.M.; Dean, A.; Sow, M.M. OpenEpi: A web-based epidemiologic and statistical calculator for public health. Public Health Rep. 2009, 124, 471–474. [Google Scholar]
- Dey, S.K.; Nguyen, T.A.; Phan, T.G.; Nishio, O.; Salim, A.F.M.; Rahman, M.; Yagyu, F.; Okitsu, S.; Ushijima, H. Molecular and epidemiological trend of norovirus associated gastroenteritis in Dhaka City, Bangladesh. J. Clin. Virol. 2007, 40, 218–223. [Google Scholar] [CrossRef]
- Nahar, S.; Afrad, M.H.; Begum, N.; Al-Mamun, F.; Sarker, A.K.; Das, S.K.; Faruque, A.S.G.; Pourkarim, M.R.; Choudhuri, M.S.K.; Azim, T.; et al. High prevalence of noroviruses among hospitalized diarrheal patients in Bangladesh, 2011. J. Infect. Dev. Ctries. 2013, 7, 892–896. [Google Scholar] [CrossRef]
- Rahman, M.; Nahar, S.; Afrad, M.H.; Faruque, A.S.; Azim, T. Norovirus variant GII.4/Sydney/2012, Bangladesh. Emerg. Infect. Dis. 2013, 19, 1347–1348. [Google Scholar] [CrossRef]
- McAtee, C.L.; Challappa, R.; Saito, M.; Mejia, C.; Bern, C.; Webman, R.; Pajuelo, M.; Gilman, R.H.; Soria, R.; Ribera, J.P.; et al. Burden of Norovirus and Rotavirus in Children after Rotavirus Vaccine Introduction, Cochabamba, Bolivia. Am. J. Trop. Med. Hyg. 2016, 94, 212–217. [Google Scholar] [CrossRef]
- Wangchuk, S.; Matsumoto, T.; Iha, H.; Ahmed, K. Surveillance of norovirus among children with diarrhea in four major hospitals in Bhutan: Replacement of GII.21 by GII.3 as a dominant genotype. PLoS ONE 2017, 12, e0184826. [Google Scholar] [CrossRef]
- Yahiro, T.; Wangchuk, S.; Wada, T.; Dorji, C.; Matsumoto, T.; Mynak, M.L.; Tshering, K.P.; Nishizono, A.; Ahmed, K. Norovirus GII.21 in Children with Diarrhea, Bhutan. Emerg. Infect. Dis. 2015, 165, 732–734. [Google Scholar] [CrossRef]
- Nordgren, J.; Nitiema, L.W.; Ouermi, D.; Simpore, J.; Svensson, L. Host Genetic Factors Affect Susceptibility to Norovirus Infections in Burkina Faso. PLoS ONE 2013, 8. [Google Scholar] [CrossRef]
- Di Cristanziano, V.; Timmen-Wego, M.; Lübke, N.; Kaiser, R.; Pfister, H.; Di Cave, D.; Berrilli, F.; Kaboré, Y.; D’Alfonso, R. Application of Luminex Gastrointestinal Pathogen Panel to human stool samples from Côte d’Ivoire. J. Infect. Dev. Ctries. 2015, 9, 884–889. [Google Scholar] [CrossRef]
- Meng, C.Y.; Smith, B.L.; Bodhidatta, L.; Richard, S.A.; Vansith, K.; Thy, B.; Srijan, A.; Serichantalergs, O.; Mason, C.J. Etiology of Diarrhea in Young Children and Patterns of Antibiotic Resistance in Cambodia. Pediatr. Infect. Dis J. 2011, 30, 331–335. [Google Scholar] [CrossRef]
- Kamel, A.H.; Ali, M.A.; El-Nady, H.G.; de Rougemont, A.; Pothier, P.; Belliot, G. Predominance and Circulation of Enteric Viruses in the Region of Greater Cairo, Egypt. J. Clin. Microbiol. 2009, 47, 1037–1045. [Google Scholar] [CrossRef]
- Sisay, Z.; Djikeng, A.; Berhe, N.; Belay, G.; Gebreyes, W.; Abegaz, W.E.; Njahira, M.N.; Wang, Q.H.; Saif, L.J. Prevalence and molecular characterization of human noroviruses and sapoviruses in Ethiopia. Arch. Virol. 2016, 161, 2169–2182. [Google Scholar] [CrossRef]
- Yassin, M.A.; Kirby, A.; Mengistu, A.A.; Arbide, I.; Dove, W.; Beyer, M.; Cunliffe, N.A.; Cuevas, L.E. Unusual norovirus and rotavirus genotypes in Ethiopia. Paediatr. Int. Child. Health 2013, 32, 51–55. [Google Scholar] [CrossRef]
- Chhabra, P.; Samoilovich, E.; Yermalovich, M.; Chernyshova, L.; Gheorghita, S.; Cojocaru, R.; Shugayev, N.; Sahakyan, G.; Lashkarashvili, M.; Chubinidze, M.; et al. Viral gastroenteritis in rotavirus negative hospitalized children <5 years of age from the independent states of the former Soviet Union. Infect. Genet. Evol. 2014, 28, 283–288. [Google Scholar] [CrossRef]
- Krumkamp, R.; Sarpong, N.; Schwarz, N.G.; Adelkofer, J.; Loag, W.; Eibach, D.; Hagen, R.M.; Adu-Sarkodie, Y.; Tannich, E.; May, J. Gastrointestinal Infections and Diarrheal Disease in Ghanaian Infants and Children: An Outpatient Case-Control Study. PLoS Neg. Trop. Dis. 2015, 9, e0003568. [Google Scholar] [CrossRef]
- Reither, K.; Ignatius, R.; Weitzel, T.; Seidu-Korkor, A.; Anyidoho, L.; Saad, E.; Djie-Maletz, A.; Ziniel, P.; Amoo-Sakyi, F.; Danikuu, F.; et al. Acute childhood diarrhoea in northern Ghana: Epidemiological, clinical and microbiological characteristics. BMC Infect. Dis. 2007, 7, 104. [Google Scholar] [CrossRef]
- Ajjampur, S.S.R.; Rajendran, P.; Ramani, S.; Banerjee, I.; Monica, B.; Sankaran, P.; Rosario, V.; Arumugam, R.; Sarkar, R.; Ward, H.; et al. Closing the diarrhoea diagnostic gap in Indian children by the application of molecular techniques. J. Med. Microbiol. 2008, 57, 1364–1368. [Google Scholar] [CrossRef]
- Chhabra, P.; Chitambar, S.D. Norovirus genotype IIb associated acute gastroenteritis in India. J. Clin. Virol. 2008, 42, 429–432. [Google Scholar] [CrossRef]
- Chhabra, P.; Dhongade, R.K.; Kalrao, V.R.; Bavdekar, A.R.; Chitambar, S.D. Epidemiological, clinical, and molecular features of norovirus infections in western India. J. Med. Virol. 2009, 81, 922–932. [Google Scholar] [CrossRef]
- Gupta, S.; Singh, K.P.; Jain, A.; Srivastava, S.; Kumar, V.; Singh, M. Aetiology of childhood viral gastroenteritis in Lucknow, north India. Indian J. Med. Res. 2015, 141, 469–472. [Google Scholar] [CrossRef]
- Jain, S.; Thakur, N.; Grover, N.; Vashistt, J.; Changotra, H. Prevalence of rotavirus, norovirus and enterovirus in diarrheal diseases in Himachal Pradesh, India. Virus Dis. 2016, 27, 77–83. [Google Scholar] [CrossRef]
- Kang, G. Detection of ’Norwalk-like viruses’ in Vellore, southern India. Trans. R. Soc. Trop. Med. Hyg. 2000, 94, 681–683. [Google Scholar] [CrossRef]
- Kulkarni, R.; Patel, A.; Bhalla, S.; Chhabra, P.; Cherian, S.; Chitambar, S.D. Characterization of GII.4 noroviruses circulating among children with acute gastroenteritis in Pune, India: 2005–2013. Infect. Genet. Evol. 2016, 37, 163–173. [Google Scholar] [CrossRef]
- Menon, V.K.; Agarwal, I.; Moses, P.D.; Sarkar, R.; Kang, G.; Simon, A. Norovirus Genogroup II Gastroenteritis in Hospitalized Children in South India. Am. J. Trop. Med. Hyg. 2013, 89, 1019–1022. [Google Scholar] [CrossRef]
- Menon, V.K.; George, S.; Ramani, S.; Illiayaraja, J.; Sarkar, R.; Jana, A.K.; Kuruvilla, K.A.; Kang, G. Genogroup IIb Norovirus Infections and Association with Enteric Symptoms in a Neonatal Nursery in Southern India. J. Clin. Microbiol. 2010, 48, 3212–3215. [Google Scholar] [CrossRef]
- Monica, B.; Ramani, S.; Banerjee, I.; Primrose, B.; Iturriza-Gomara, M.; Gallimore, C.I.; Brown, D.W.; M, F.; Moses, P.D.; Gray, J.J.; et al. Human caliciviruses in symptomatic and asymptomatic infections in children in Vellore, South India. J. Med. Virol. 2007, 79, 544–551. [Google Scholar] [CrossRef]
- Nataraju, S.M.; Ghosh, M.; Ganesh, B.; Bhattacharya, M.K.; Das, S.; Chatterjee, M.K.; Sarkar, U.; Mitra, U.; Arora, R.; Kobayashi, N.; et al. Emergence of Noroviruses homologous to strains reported from Djibouti (horn of Africa), Brazil, Italy, Japan and USA among children in Kolkata, India. Eur. Rev. Med. Pharmacol. Sci. 2010, 14, 789–794. [Google Scholar]
- Nataraju, S.M.; Pativada, M.; Chatterjee, D.; Nayak, M.K.; Ganesh, B.; Bhattacharya, M.K.; Ramamurthy, T.; Ganguly, S.; Saha, D.R.; Rajendran, K.; et al. Molecular epidemiology of norovirus infections in children and adults: Sequence analysis of region C indicates genetic diversity of NVGII strains in Kolkata, India. Epidemiol. Infect. 2011, 139, 910–918. [Google Scholar] [CrossRef]
- Nayak, M.K.; Chatterjee, D.; Nataraju, S.M.; Pativada, M.; Mitra, U.; Chatterjee, M.K.; Saha, T.K.; Sarkar, U.; Krishnan, T. A new variant of Norovirus GII.4/2007 and inter-genotype recombinant strains of NVGII causing acute watery diarrhoea among children in Kolkata, India. J. Clin. Virol. 2009, 45, 223–229. [Google Scholar] [CrossRef]
- Rachakonda, G.; Choudekar, A.; Parveen, S.; Bhatnagar, S.; Patwari, A.; Broor, S. Genetic diversity of noroviruses and sapoviruses in children with acute sporadic gastroenteritis in New Delhi, India. J. Clin. Virol. 2008, 43, 42–48. [Google Scholar] [CrossRef]
- Subekti, D.; Lesmana, M.; Tjaniadi, P.; Safari, N.; Frazier, E.; Simanjuntak, C.; Komalarini, S.; Taslim, J.; Campbell, J.R.; Oyofo, B.A. Incidence of Norwalk-like viruses, rotavirus and adenovirus infection in patients with acute gastroenteritis in Jakarta, Indonesia. FEMS Immunol. Med. Microbiol. 2002, 33, 27–33. [Google Scholar]
- Subekti, D.S.; Tjaniadi, P.; Lesmana, M.; Simanjuntak, C.; Komalarini, S.; Digdowirogo, H.; Setiawan, B.; Corwin, A.L.; Campbell, J.R.; Porter, K.R.; et al. Characterization of Norwalk-like virus associated with gastroenteritis in Indonesia. J. Med. Virol. 2002, 67, 253–258. [Google Scholar] [CrossRef]
- Shioda, K.; Cosmas, L.; Audi, A.; Gregoricus, N.; Vinjé, J.; Parashar, U.D.; Montgomery, J.M.; Feikin, D.R.; Breiman, R.F.; Hall, A.J. Population-Based Incidence Rates of Diarrheal Disease Associated with Norovirus, Sapovirus, and Astrovirus in Kenya. PLoS ONE 2016, 11, e0145943. [Google Scholar] [CrossRef]
- Papaventsis, D.C.; Dove, W.; Cunliffe, N.A.; Nakagomi, O.; Combe, P.; Grosjean, P.; Hart, C.A. Norovirus Infection in Children with Acute Gastroenteritis, Madagascar, 2004–2005. Emerg. Infect. Dis. 2007, 13, 908–911. [Google Scholar] [CrossRef]
- Benmessaoud, R.; Jroundi, I.; Nezha, M.; Moraleda, C.; Tligui, H.; Seffar, M.; Alvarez-Martinez, M.J.; Pons, M.J.; Chaacho, S.; Hayes, E.B.; et al. Aetiology, epidemiology and clinical characteristics of acute moderate-to-severe diarrhoea in children under 5 years of age hospitalized in a referral paediatric hospital in Rabat, Morocco. J. Med. Microbiol. 2014, 64, 84–92. [Google Scholar] [CrossRef]
- El Qazoui, M.; Oumzil, H.; Baassi, L.; El Omari, N.; Sadki, K.; Amzazi, S.; Benhafid, M.; El Aouad, R. Rotavirus and Norovirus infections among acute gastroenteritis children in Morocco. BMC Infect. Dis. 2014, 14, 300. [Google Scholar] [CrossRef]
- Dove, W.; Cunliffe, N.A.; Gondwe, J.S.; Broadhead, R.L.; Molyneux, M.E.; Nakagomi, O.; Hart, C.A. Detection and characterization of human caliciviruses in hospitalized children with acute gastroenteritis in Blantyre, Malawi. J. Med. Virol. 2005, 77, 522–527. [Google Scholar] [CrossRef]
- Trainor, E.; Lopman, B.; Iturriza-Gomara, M.; Dove, W.; Ngwira, B.; Nakagomi, O.; Nakagomi, T.; Parashar, U.; Cunliffe, N. Detection and molecular characterisation of noroviruses in hospitalised children in Malawi, 1997–2007. J. Med. Virol. 2013, 85, 1299–1306. [Google Scholar] [CrossRef]
- Hoa-Tran, T.N.; Nakagomi, T.; Sano, D.; Sherchand, J.B.; Pandey, B.D.; Cunliffe, N.A.; Nakagomi, O. Molecular epidemiology of noroviruses detected in Nepalese children with acute diarrhea between 2005 and 2011: Increase and predominance of minor genotype GII.13. Infect. Genet. Evol. 2015, 30, 27–36. [Google Scholar] [CrossRef]
- Japhet, M.O.; Adesina, O.A.; Famurewa, O.; Svensson, L.; Nordgren, J. Molecular epidemiology of rotavirus and norovirus in Ile-Ife, Nigeria: High prevalence of G12P[8] rotavirus strains and detection of a rare norovirus genotype. J. Med. Virol. 2012, 84, 1489–1496. [Google Scholar] [CrossRef]
- Japhet, M.O.; Famurewa, O.; Adesina, O.A.; Opaleye, O.O.; Wang, B.; Höhne, M.; Bock, C.T.; Mas Marques, A.; Niendorf, S. Viral gastroenteritis among children of 0-5 years in Nigeria: Characterization of the first Nigerian aichivirus, recombinant noroviruses and detection of a zoonotic astrovirus. J. Clin. Virol. 2019, 111, 4–11. [Google Scholar] [CrossRef]
- Bucardo, F.; Reyes, Y.; Svensson, L.; Nordgren, J. Predominance of Norovirus and Sapovirus in Nicaragua after Implementation of Universal Rotavirus Vaccination. PLoS ONE 2014, 9, e98201. [Google Scholar] [CrossRef]
- Soli, K.W.; Maure, T.; Kas, M.P.; Bande, G.; Bebes, S.; Luang-Suarkia, D.; Siba, P.M.; Morita, A.; Umezaki, M.; Greenhill, A.R.; et al. Detection of enteric viral and bacterial pathogens associated with paediatric diarrhoea in Goroka, Papua New Guinea. Int. J. Infect. Dis. 2014, 27, 54–58. [Google Scholar] [CrossRef]
- Alam, A.; Qureshi, S.A.; Vinjé, J.; Zaidi, A. Genetic characterization of norovirus strains in hospitalized children from Pakistan. J. Med. Virol. 2016, 88, 216–223. [Google Scholar] [CrossRef]
- Alam, M.; Khurshid, A.; Shaukat, S.; Rana, M.; Sharif, S.; Angez, M.; Nisar, N.; Aamir, U.; Naeem, M.; Zaidi, S. Viral Etiologies of Acute Dehydrating Gastroenteritis in Pakistani Children: Confounding Role of Parechoviruses. Viruses 2015, 7, 378–393. [Google Scholar] [CrossRef]
- Kabayiza, J.-C.; Andersson, M.E.; Nilsson, S.; Bergström, T.; Muhirwa, G.; Lindh, M. Real-time PCR Identification of Agents Causing Diarrhea in Rwandan Children Less Than 5 Years of Age. Pediatr. Infect. Dis. J. 2014, 33, 1037–1042. [Google Scholar] [CrossRef]
- Adam, M.A.; Wang, J.; Enan, K.-A.; Shen, H.; Wang, H.; El Hussein, A.R.; Musa, A.B.; Khidir, I.M.; Ma, X. Molecular Survey of Viral and Bacterial Causes of Childhood Diarrhea in Khartoum State, Sudan. Front. Microbiol. 2018, 9, 112. [Google Scholar] [CrossRef]
- Elfving, K.; Andersson, M.; Msellem, M.I.; Welinder-Olsson, C.; Petzold, M.; Bjorkman, A.; Trollfors, B.; Martensson, A.; Lindh, M. Real-Time PCR Threshold Cycle Cutoffs Help to Identify Agents Causing Acute Childhood Diarrhea in Zanzibar. J. Clin. Microbiol. 2014, 52, 916–923. [Google Scholar] [CrossRef]
- Liu, J.; Kibiki, G.; Maro, V.; Maro, A.; Kumburu, H.; Swai, N.; Taniuchi, M.; Gratz, J.; Toney, D.; Kang, G.; et al. Multiplex reverse transcription PCR Luminex assay for detection and quantitation of viral agents of gastroenteritis. J. Clin. Virol. 2011, 50, 308–313. [Google Scholar] [CrossRef]
- Moyo, S.; Hanevik, K.; Blomberg, B.; Kommedal, O.; Vainio, K.; Maselle, S.; Langeland, N. Genetic diversity of norovirus in hospitalised diarrhoeic children and asymptomatic controls in Dar es Salaam, Tanzania. Infect. Genet. Evol. 2014, 26, 340–347. [Google Scholar] [CrossRef]
- Ben-Salem Ben Nejma, I.; Hassine Zaafrane, M.; Hassine, F.; Sdiri-Loulizi, K.; Ben Said, M.; Aouni, M.; Mzoughi, R. Etiology of Acute Diarrhea in Tunisian Children with Emphasis on Diarrheagenic Escherichia coli: Prevalence and Identification of E. coli Virulence Markers. Iran. J. Public Health 2014, 43, 947–960. [Google Scholar]
- Hassine-Zaafrane, M.; Sdiri-Loulizi, K.; Kaplon, J.; Salem, I.B.; Pothier, P.; Aouni, M.; Ambert-Balay, K. Prevalence and genetic diversity of norovirus infection in Tunisian children (2007–2010). J. Med. Virol. 2013, 85, 1100–1110. [Google Scholar] [CrossRef]
- Sdiri-Loulizi, K.; Ambert-Balay, K.; Gharbi-Khelifi, H.; Sakly, N.; Hassine, M.; Chouchane, S.; Guediche, M.N.; Pothier, P.; Aouni, M. Molecular Epidemiology of Norovirus Gastroenteritis Investigated Using Samples Collected from Children in Tunisia during a Four-Year Period: Detection of the Norovirus Variant GGII.4 Hunter as Early as January 2003. J. Clin. Microbiol. 2009, 47, 421–429. [Google Scholar] [CrossRef]
- Nguyen, T.A.; Hoang, L.; Pham, L.D.; Hoang, K.T.; Okitsu, S.; Mizuguchi, M.; Ushijima, H. Norovirus and Sapovirus Infections among Children with Acute Gastroenteritis in Ho Chi Minh City during 2005–2006. J. Trop. Ped. 2008, 54, 102–113. [Google Scholar] [CrossRef]
- Nguyen, T.A.; Yagyu, F.; Okame, M.; Phan, T.G.; Trinh, Q.D.; Yan, H.; Hoang, K.T.; Cao, A.T.H.; Le Hoang, P.; Okitsu, S.; et al. Diversity of viruses associated with acute gastroenteritis in children hospitalized with diarrhea in Ho Chi Minh City, Vietnam. J. Med. Virol. 2007, 79, 582–590. [Google Scholar] [CrossRef]
- Tamura, T.; Nishikawa, M.; Anh, D.; Suzuki, H. Molecular Epidemiological Study of Rotavirus and Norovirus Infections among Children with Acute Gastroenteritis in Nha Trang, Vietnam, December 2005–June 2006. Jpn. J. Infect. Dis. 2010, 63, 405–411. [Google Scholar]
- Tra, P.M.V.; Thompson, C.; Phuc, H.L.; Tuyet, P.T.N.; Vinh, H.; Hoang, N.V.M.; Minh, P.V.; Vinh, N.T.; Thuy, C.T.; Nga, T.T.T.; et al. Endemic Norovirus Infections in Children, Ho Chi Minh City, Vietnam, 2009–2010. Emerg. Infect. Dis. 2013, 19, 977–980. [Google Scholar] [CrossRef]
- Trang, N.V.; Choisy, M.; Nakagomi, T.; Chinh, N.T.M.; Doan, Y.H.; Yamashiro, T.; Bryant, J.E.; Nakagomi, O.; Anh, D.D. Determination of cut-off cycle threshold values in routine RT–PCR assays to assist differential diagnosis of norovirus in children hospitalized for acute gastroenteritis. Epidemiol. Infect. 2015, 143, 3292–3299. [Google Scholar] [CrossRef]
- Trang, N.V.; Luan, L.T.; Kim-Anh, L.T.; Hau, V.T.B.; Nhung, L.T.H.; Phasuk, P.; Setrabutr, O.; Shirley, H.; Vinjé, J.; Anh, D.D.; et al. Detection and molecular characterization of noroviruses and sapoviruses in children admitted to hospital with acute gastroenteritis in Vietnam. J. Med. Virol. 2012, 84, 290–297. [Google Scholar] [CrossRef]
- Kirby, A.; Al-Eryani, A.; Al-Sonboli, N.; Hafiz, T.; Beyer, M.; Al-Aghbari, N.; Al-Moheri, N.; Dove, W.; Cunliffe, N.A.; Cuevas, L.E. Rotavirus and norovirus infections in children in Sana’a, Yemen. Trop. Med. Int. Health 2011, 16, 680–684. [Google Scholar] [CrossRef]
- Howard, L.M.; Mwape, I.; Siwingwa, M.; Simuyandi, M.; Guffey, M.B.; Stringer, J.S.A.; Chi, B.H.; Edwards, K.M.; Chilengi, R. Norovirus infections in young children in Lusaka Province, Zambia: Clinical characteristics and molecular epidemiology. BMC Infect. Dis. 2017, 17, 92. [Google Scholar] [CrossRef]
- Rahman, M.; Hassan, Z.; Nahar, Z.; Faruque, A.S.G.; Ranst, M.; Rahman, S.R.; Azim, T. Molecular detection of noroviruses in hospitalized patients in Bangladesh. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 937–945. [Google Scholar] [CrossRef]
- Tra My, P.V.; Lam, H.M.; Thompson, C.N.; Phuc, H.L.; Tuyet, P.T.N.; Vinh, H.; Hoang, N.V.M.; Minh, P.; Vinh, N.T.; Thuy, C.T.; et al. The dynamics of GII.4 Norovirus in Ho Chi Minh City, Vietnam. Infect. Genet. Evol. 2013, 18, 335–343. [Google Scholar] [CrossRef]
- Hansman, G.S.; Doan, L.T.P.; Kguyen, T.A.; Okitsu, S.; Katayama, K.; Ogawa, S.; Natori, K.; Takeda, N.; Kato, Y.; Nishio, O.; et al. Detection of norovirus and sapovirus infection among children with gastroenteritis in Ho Chi Minh City, Vietnam. Arch. Virol. 2004, 149, 1673–1688. [Google Scholar] [CrossRef]
- Kroneman, A.; Vega, E.; Vennema, H.; Vinje´, J.; White, P.; Hansman, G.; Green, K.; Martella, V.; Katayama, K.; Koopmans, M. Proposal for a unified norovirus nomenclature and genotyping. Arch. Virol. 2013, 158, 2059–2068. [Google Scholar] [CrossRef]
- Armah, G.E.; Gallimore, C.I.; Binka, F.N.; Asmah, R.H.; Green, J.; Ugoji, U.; Anto, F.; Brown, D.W.G.; Gray, J.J. Characterisation of norovirus strains in rural Ghanaian children with acute diarrhoea. J. Med. Virol. 2006, 78, 1480–1485. [Google Scholar] [CrossRef]
- Mitui, M.T.; Bozdayi, G.; Ahmed, S.; Matsumoto, T.; Nishizono, A.; Ahmed, K. Detection and molecular characterization of diarrhea causing viruses in single and mixed infections in children: A comparative study between Bangladesh and Turkey. J. Med. Virol. 2014, 86, 1159–1168. [Google Scholar] [CrossRef]
- Phan, T.G.; Okame, M.; Nguyen, T.A.; Maneekarn, N.; Nishio, O.; Okitsu, S.; Ushijima, H. Human astrovirus, norovirus (GI, GII), and sapovirus infections in Pakistani children with diarrhea. J. Med. Virol. 2004, 73, 256–261. [Google Scholar] [CrossRef]
- Thorne, L.; Nalwoga, A.; Mentzer, A.J.; de Rougemont, A.; Hosmillo, M.; Webb, E.; Nampiija, M.; Muhwezi, A.; Carstensen, T.; Gurdasani, D.; et al. The First Norovirus Longitudinal Seroepidemiological Study from Sub-Saharan Africa Reveals High Seroprevalence of Diverse Genotypes Associated with Host Susceptibility Factors. J. Infect. Dis. 2018, 218, 716–725. [Google Scholar] [CrossRef]
- Rouhani, S.; Penataro Yori, P.; Paredes Olortegui, M.; Siguas Salas, M.; Rengifo Trigoso, D.; Mondal, D.; Bodhidatta, L.; Platts-Mills, J.; Samie, A.; Kabir, F.; et al. Norovirus Infection and Acquired Immunity in 8 Countries: Results from the MAL-ED Study. Clin. Infect. Dis. 2016, 62, 1210–1217. [Google Scholar] [CrossRef]
- Eibach, D.; Krumkamp, R.; Hahn, A.; Sarpong, N.; Adu-Sarkodie, Y.; Leva, A.; Käsmaier, J.; Panning, M.; May, J.; Tannich, E. Application of a multiplex PCR assay for the detection of gastrointestinal pathogens in a rural African setting. BMC Infect. Dis. 2016, 16, 150. [Google Scholar] [CrossRef]
- Seid, L.; Stokes, W.; Bayih, A.G.; Getie, S.; Abere, A.; Tesfa, H.; Pillai, D.R. Molecular detection of Enteropathogens from diarrheic stool of HIV positive patients in Gondar, Ethiopia. BMC Infect. Dis. 2018, 18, 354. [Google Scholar] [CrossRef]
- Spina, A.; Kerr, K.G.; Cormican, M.; Barbut, F.; Eigentler, A.; Zerva, L.; Tassios, P.; Popescu, G.A.; Rafila, A.; Eerola, E.; et al. Spectrum of enteropathogens detected by the FilmArray GI Panel in a multicentre study of community-acquired gastroenteritis. Clin. Microbiol. Infect. 2015, 21, 719–728. [Google Scholar] [CrossRef]
- Andersson, M.; Kabayiza, J.-C.; Elfving, K.; Nilsson, S.; Msellem, M.I.; Mårtensson, A.; Björkman, A.; Bergström, T.; Lindh, M. Coinfection with Enteric Pathogens in East African Children with Acute Gastroenteritis—Associations and Interpretations. Am. J. Trop. Med. Hyg. 2018, 98, 1566–1570. [Google Scholar] [CrossRef]
- Ahmed, S.M.; Lopman, B.A.; Levy, K. A systematic review and meta-analysis of the global seasonality of norovirus. PLoS ONE 2013, 8, e75922. [Google Scholar] [CrossRef]
- Becker-Dreps, S.; Cuthbertson, C.C.; Bucardo, F.; Vinje, J.; Paniagua, M.; Giebultowicz, S.; Espinoza, F.; Emch, M. Environmental factors associated with childhood norovirus diarrhoea in Leon, Nicaragua. Epidemiol. Infect. 2017, 145, 1597–1605. [Google Scholar] [CrossRef]
- Bruggink, L.D.; Marshall, J.A. The incidence of norovirus-associated gastroenteritis outbreaks in Victoria, Australia (2002–2007) and their relationship with rainfall. Int. J. Environ. Res. Public Health 2010, 7, 2822–2827. [Google Scholar] [CrossRef]
- Sang, S.; Yang, X. Evolutionary dynamics of GII.17 norovirus. PeerJ 2018, 6, e4333. [Google Scholar] [CrossRef]
- Lindesmith, L.C.; Mallory, M.L.; Debbink, K.; Donaldson, E.F.; Brewer-Jensen, P.D.; Swann, E.W.; Sheahan, T.P.; Graham, R.L.; Beltramello, M.; Corti, D.; et al. Conformational Occlusion of Blockade Antibody Epitopes, a Novel Mechanism of GII.4 Human Norovirus Immune Evasion. mSphere 2018, 3, e00518-17. [Google Scholar] [CrossRef]
- Lindesmith, L.C.; Brewer-Jensen, P.D.; Mallory, M.L.; Yount, B.; Collins, M.H.; Debbink, K.; Graham, R.L.; Baric, R.S. Human Norovirus Epitope D Plasticity Allows Escape from Antibody Immunity without Loss of Capacity for Binding Cellular Ligands. J. Virol. 2019, 93, e01813-18. [Google Scholar] [CrossRef]
Figure 1.
The study selection flow diagram.

Figure 2.
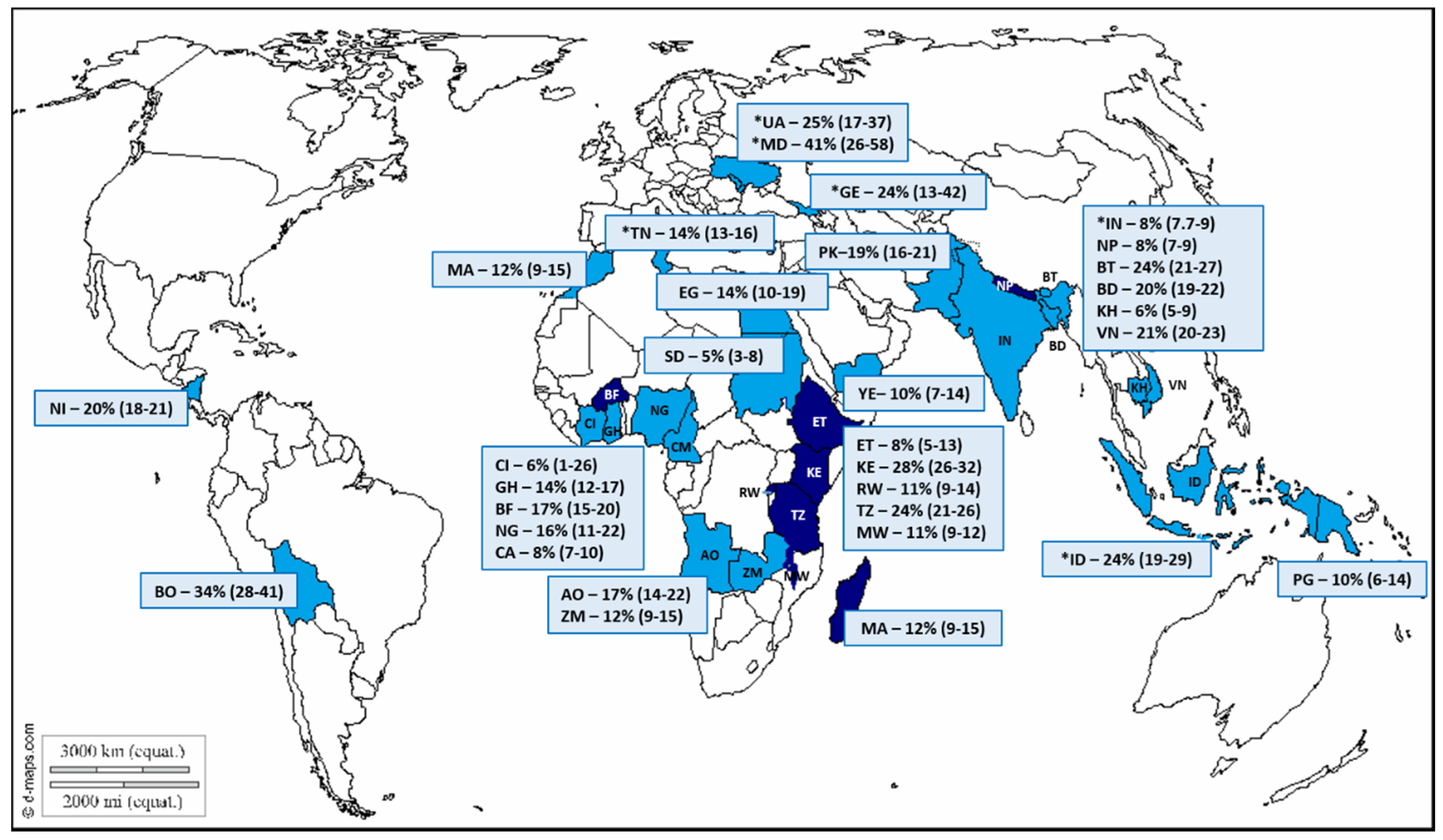
The world map indicating the low-income countries (LIC; dark blue) and lower-middle-income countries (LMIC; light blue) that are represented by the norovirus studies. The average norovirus prevalence and 95% confidence interval (95% CI) is indicated for each country. Countries are identified by two-letter International Organization for Standardization (ISO) codes, and the study references are indicated in brackets. AO, Angola [23]; BD, Bangladesh [28,29,37,38,39]; BO, Bolivia [40]; BT, Bhutan [41,42]; BF, Burkina Faso [20,27,43]; CI, Cote d’Ivoire [44]; CM, Cameroon [26]; KH, Cambodia [45]; EG, Egypt [46]; ET, Ethiopia [47,48]; GE, Georgia* [49]; GH, Ghana [50,51]; IN, India [52,53,54,55,56,57,58,59,60,61,62,63,64,65]; ID, Indonesia [66,67]; KE, Kenya [68]; MG, Madagascar [69]; MA, Morocco [70,71]; MW, Malawi [72,73]; MD, Republic of Moldova* [49]; NP, Nepal [22,74]; NG, Nigeria [75,76]; NI, Nicaragua [21,77]; PG, Papua New Guinea [78]; PK, Pakistan [79,80]; RW, Rwanda [81]; SD, Sudan [82]; TZ, Tanzania [83,84,85]; TN, Tunisia [86,87,88]; UA, Ukraine* [49]; VN, Vietnam [24,89,90,91,92,93,94]; YE, Yemen [95]; ZM, Zambia [96]. (https://d-maps.com/carte.php?num_car=13181&lang=en). *Includes data from studies that screened pathogen-negative stool specimens for norovirus.
Figure 2.
The world map indicating the low-income countries (LIC; dark blue) and lower-middle-income countries (LMIC; light blue) that are represented by the norovirus studies. The average norovirus prevalence and 95% confidence interval (95% CI) is indicated for each country. Countries are identified by two-letter International Organization for Standardization (ISO) codes, and the study references are indicated in brackets. AO, Angola [23]; BD, Bangladesh [28,29,37,38,39]; BO, Bolivia [40]; BT, Bhutan [41,42]; BF, Burkina Faso [20,27,43]; CI, Cote d’Ivoire [44]; CM, Cameroon [26]; KH, Cambodia [45]; EG, Egypt [46]; ET, Ethiopia [47,48]; GE, Georgia* [49]; GH, Ghana [50,51]; IN, India [52,53,54,55,56,57,58,59,60,61,62,63,64,65]; ID, Indonesia [66,67]; KE, Kenya [68]; MG, Madagascar [69]; MA, Morocco [70,71]; MW, Malawi [72,73]; MD, Republic of Moldova* [49]; NP, Nepal [22,74]; NG, Nigeria [75,76]; NI, Nicaragua [21,77]; PG, Papua New Guinea [78]; PK, Pakistan [79,80]; RW, Rwanda [81]; SD, Sudan [82]; TZ, Tanzania [83,84,85]; TN, Tunisia [86,87,88]; UA, Ukraine* [49]; VN, Vietnam [24,89,90,91,92,93,94]; YE, Yemen [95]; ZM, Zambia [96]. (https://d-maps.com/carte.php?num_car=13181&lang=en). *Includes data from studies that screened pathogen-negative stool specimens for norovirus.

Figure 3.
An overview of the norovirus coinfections from 26 studies in 15 LMIC countries and six studies in four LIC countries: Twelve studies tested for norovirus and rotavirus; 12 studies tested for a range of enteric viruses; five studies tested for viruses and bacteria; and three studies tested for viruses, bacteria, and parasites.
Figure 3.
An overview of the norovirus coinfections from 26 studies in 15 LMIC countries and six studies in four LIC countries: Twelve studies tested for norovirus and rotavirus; 12 studies tested for a range of enteric viruses; five studies tested for viruses and bacteria; and three studies tested for viruses, bacteria, and parasites.

Figure 4.
(a) The distribution of norovirus capsid genotypes detected in six LIC between 1997 and 2013; (b) the distribution of norovirus capsid genotypes circulating in 14 LMIC between 1990 to 1994 and 1998 to 2015. The years in which the studies were conducted are indicated in parenthesis after each country. NA = not assigned a GI genotype.
Figure 4.
(a) The distribution of norovirus capsid genotypes detected in six LIC between 1997 and 2013; (b) the distribution of norovirus capsid genotypes circulating in 14 LMIC between 1990 to 1994 and 1998 to 2015. The years in which the studies were conducted are indicated in parenthesis after each country. NA = not assigned a GI genotype.

Figure 5.
The distribution of norovirus GII.4 variants in (a) LIC (5 countries, 9 studies, and 167 typed variants) and (b) LMIC (14 countries, 25 studies, and 945 typed variants) between 1997 and 2015. The GII.4 variant was determined based on partial capsid genotyping.
Figure 5.
The distribution of norovirus GII.4 variants in (a) LIC (5 countries, 9 studies, and 167 typed variants) and (b) LMIC (14 countries, 25 studies, and 945 typed variants) between 1997 and 2015. The GII.4 variant was determined based on partial capsid genotyping.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
The detection of norovirus in LIC and LMIC in gastroenteritis cases and asymptomatic controls.
Table 1.
The detection of norovirus in LIC and LMIC in gastroenteritis cases and asymptomatic controls.
| Group | No. of Studies/ No. of Countries | Number of Cases Tested | Number of Norovirus + | Norovirus Detection % (95% CI) |
|---|---|---|---|---|
| LIC | ||||
| <5 years inpatient | 9/6 | 6713 | 733 | 11 (10–12) |
| <5 years outpatient | 5/4 | 2430 | 226 | 9 (8–11) |
| Mixed age inpatient | 1/1 | 229 | 95 | 42 (35–48) |
| Mixed age and setting | 3/3 | 994 | 127 | 13 (11–15) |
| Overall symptomatic cases | 15/8 | 10366 | 1181 | 11 (11–12) |
| Asymptomatic controls | 7/6 | 1903 | 166 | 9 (8–10) |
| LMIC | ||||
| <5 years inpatient | 30/13 | 13228 | 2294 | 17 (17–18) |
| <5 years outpatient | 8/4 | 1058 | 123 | 12 (10–14) |
| <18 years inpatient | 6/6 | 1603 | 142 | 9 (8–10) |
| Mixed age and setting | 14/10 | 9969 | 1401 | 14 (13–15) |
| Overall symptomatic cases | 49/21 | 25922 | 3977 | 15 (15–16) |
| Asymptomatic controls | 16/11 | 3407 | 257 | 8 (8–10) |
+ Number of norovirus positives.
Table 2.
The prevalence of norovirus GI, GII, and GIV in LIC and LMIC in symptomatic norovirus cases and asymptomatic controls.
Table 2.
The prevalence of norovirus GI, GII, and GIV in LIC and LMIC in symptomatic norovirus cases and asymptomatic controls.
| Setting | Norovirus Positives | GI n (%) | GII n (%) | GI + GII n (%) | GIV * |
|---|---|---|---|---|---|
| LIC | |||||
| Symptomatic | 694 | 82 (11.8) | 606 (87.3) | 6 (0.9) | nt |
| Asymptomatic | 139 | 30 (21.6) | 108 (77.7) | 1 (0.7) | nt |
| LMIC | |||||
| Symptomatic | 3169 | 425 (13.4) | 2642 (83.4) | 86 (2.7) | 16 (0.5) |
| Asymptomatic | 136 | 33 (24) | 99 (73) | 4 (3) | 0 |
* Three studies from Bangladesh detected norovirus GIV in 16/566 norovirus-positive specimens. nt = not tested.
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Mans, J. Norovirus Infections and Disease in Lower-Middle- and Low-Income Countries, 1997–2018. Viruses 2019, 11, 341. https://doi.org/10.3390/v11040341
AMA Style
Mans J. Norovirus Infections and Disease in Lower-Middle- and Low-Income Countries, 1997–2018. Viruses. 2019; 11(4):341. https://doi.org/10.3390/v11040341
Chicago/Turabian StyleMans, Janet. 2019. "Norovirus Infections and Disease in Lower-Middle- and Low-Income Countries, 1997–2018" Viruses 11, no. 4: 341. https://doi.org/10.3390/v11040341
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.