
Cost-Effectiveness Analysis of COVID-19 Case Quarantine Strategies in Two Australian States: New South Wales and Western Australia

Abstract
:1. Introduction
2. Literature Review
3. Data and Methods
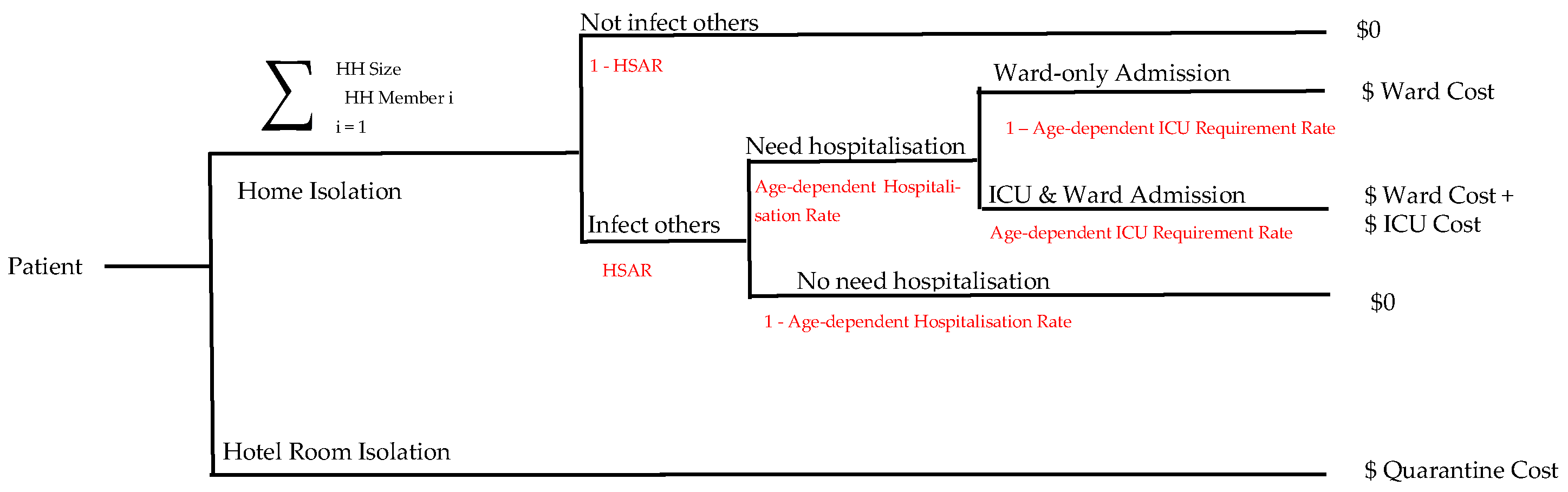
3.1. Decision Tree Model for Cost-Effectiveness Analysis
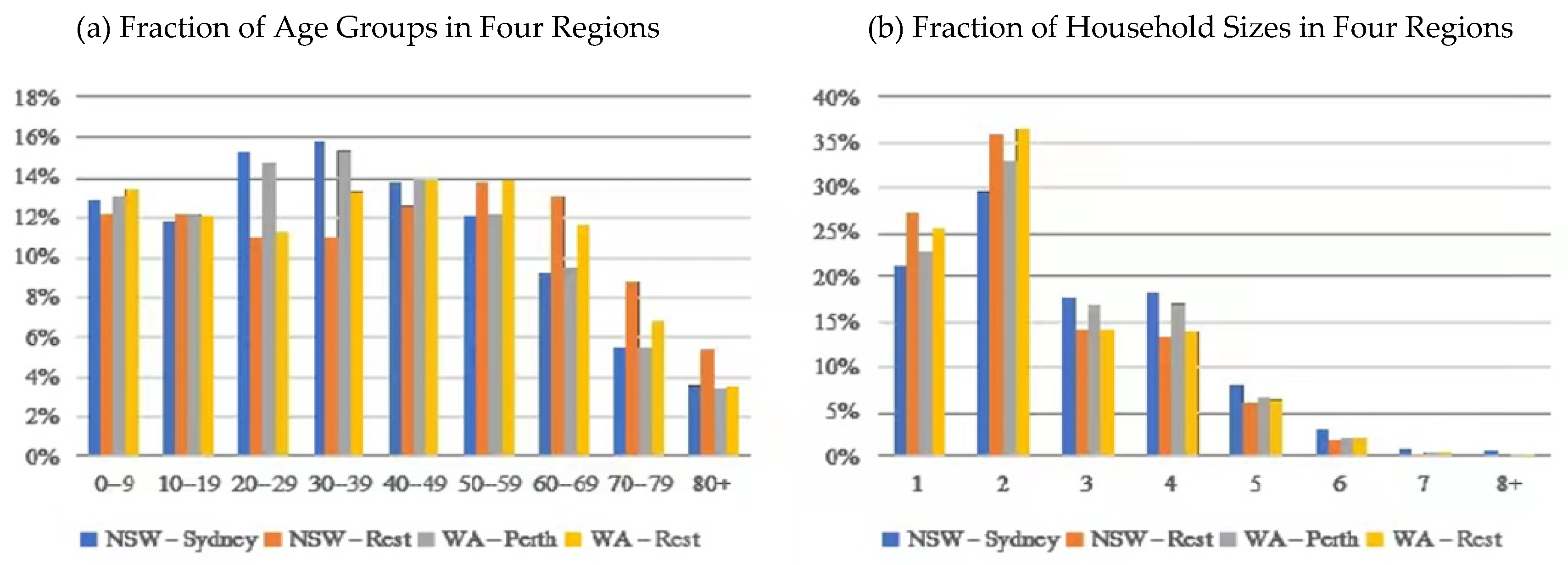
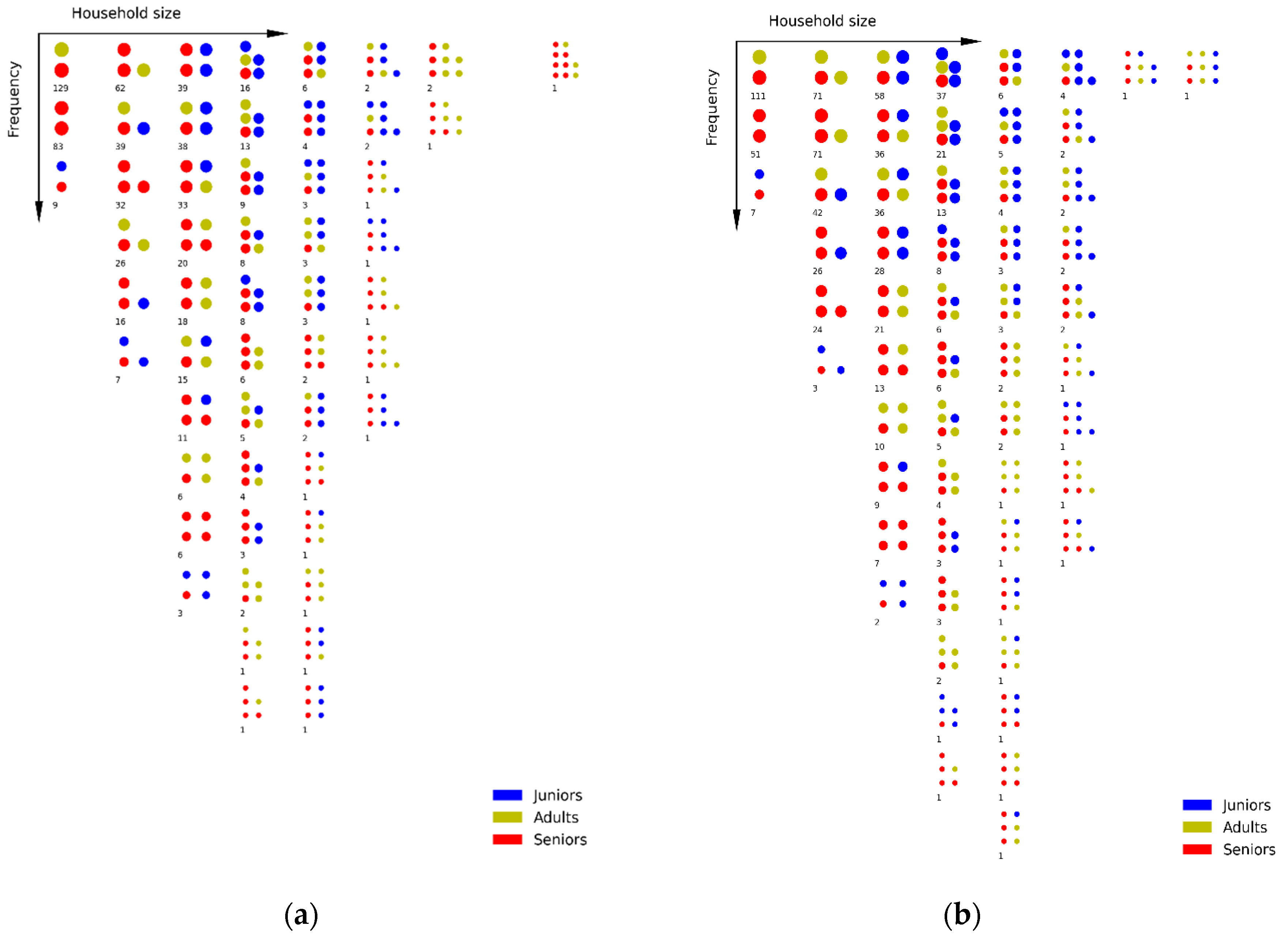
3.2. Simulation Model: Age Distribution of Household Members
4. Results and Discussion
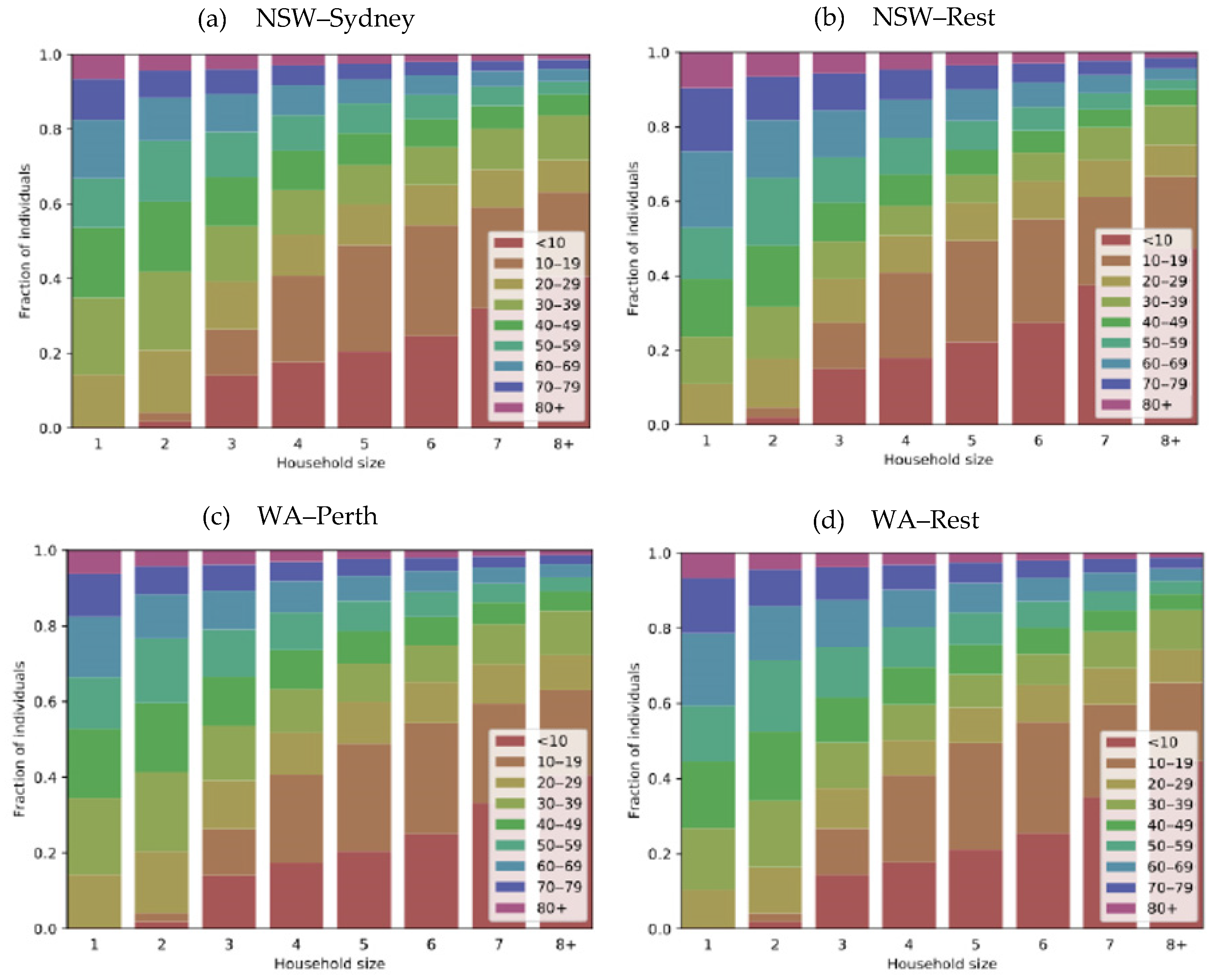
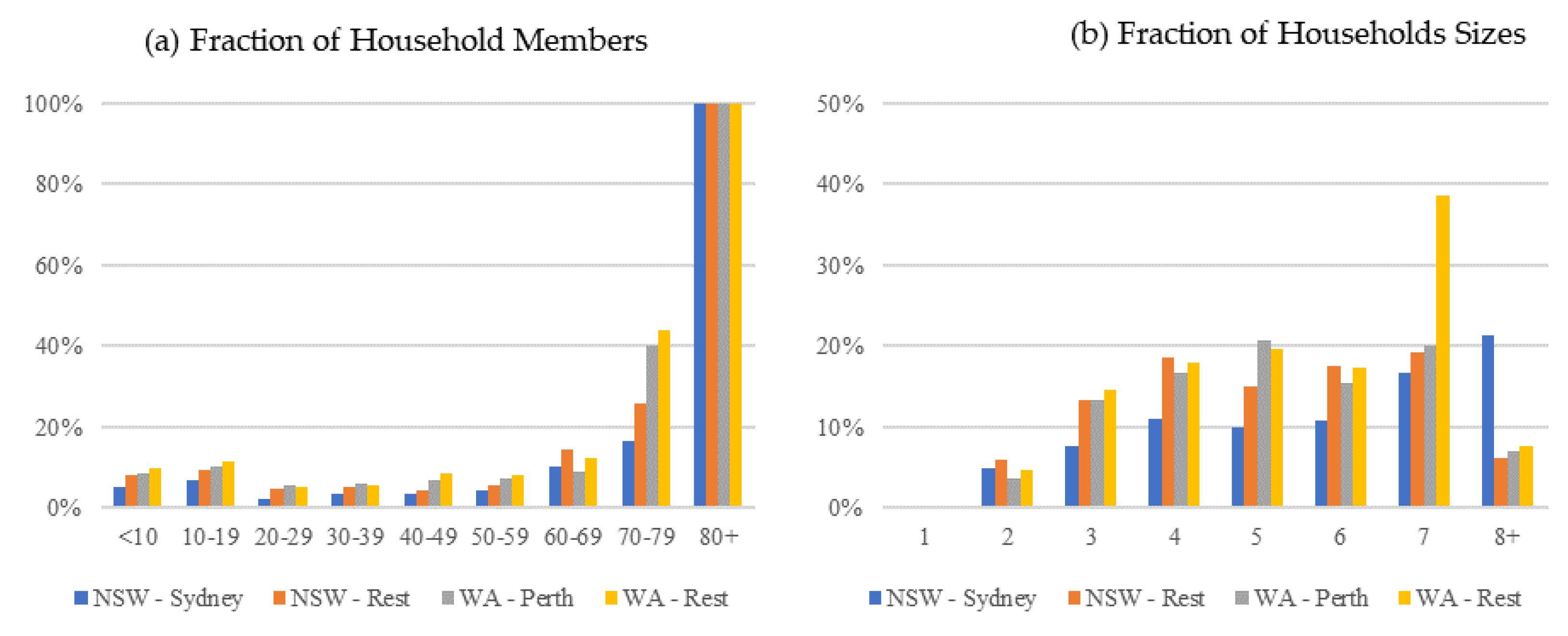
4.1. Simulated Households
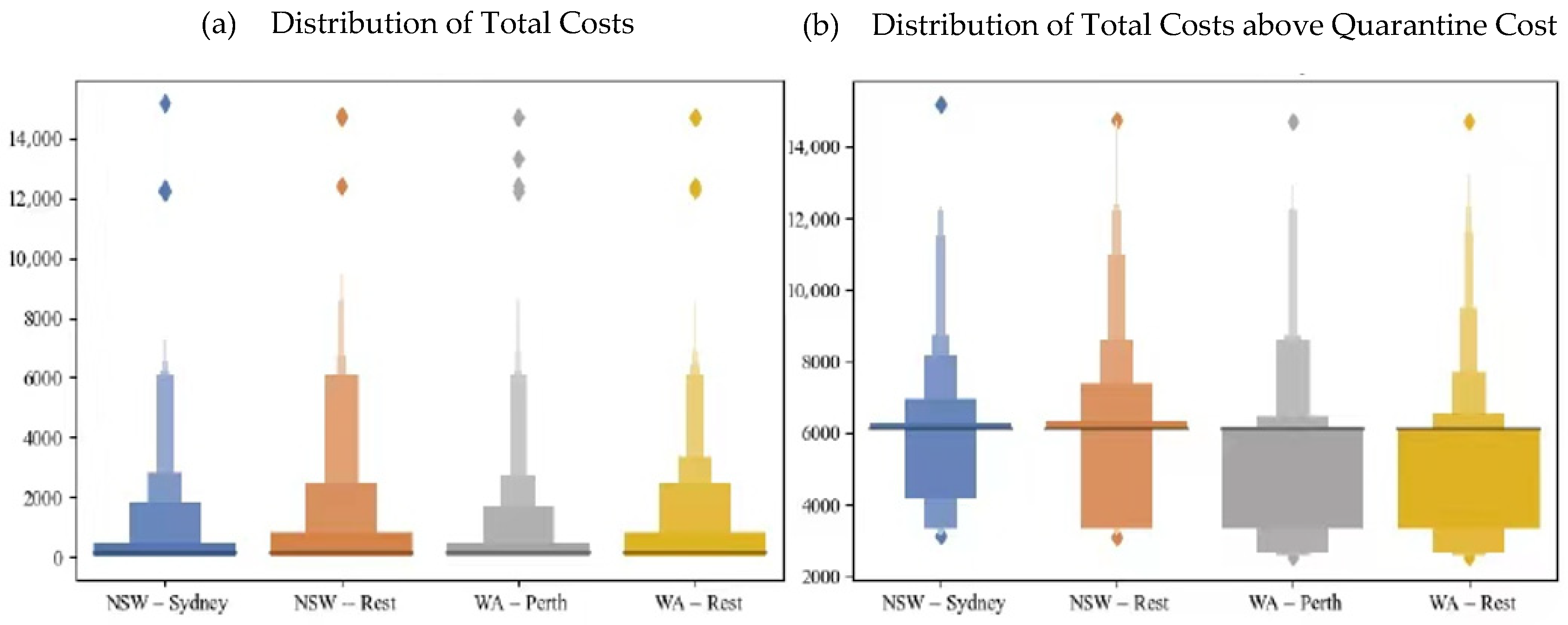
4.2. Estimating the Isolation Cost
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
| 1 | The Python program of the simulation model can be accessed from https://github.com/nicgeard/sim-demog (accessed on 16 July 2020). |
| 2 | There is no household infection within the individual households. |
References
- Al Zobbi, Mohammed, Belal Alsinglawi, Omar Mubin, and Fady Alnajjar. 2020. Measurement Method for Evaluating the Lockdown Policies during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health 17: 5574. [Google Scholar] [CrossRef]
- Arnedo-Pena, Alberto, Susana Sabater-Vidal, Noemí Meseguer-Ferrer, Mª Rosario Pac-Sa, Pilar Mañes-Flor, Juan Carlos Gascó-Laborda, Rosa Mª Larrea, Mª Dolores Tirado-Balaguer, MA Romeu-García, and María Gil-Fortuño. 2020. COVID-19 secondary attack rate and risk factors in household contacts in Castellon (Spain): Preliminary report. Enfermedades Emergentes 19: 64–70. [Google Scholar]
- Australian Bureau of Statistics. 2016. Census 2016 by Statistical Area SA2+ (ASGS 2016). Available online: http://stat.data.abs.gov.au/Index.aspx?DataSetCode=ABS_C16_T01_SA (accessed on 16 July 2020).
- Australian Government. 2020. Impact of COVID-19: Theoretical Modelling of How the Health System Can Respond. Available online: https://www.pm.gov.au/sites/default/files/files/covid19-icu-modelling-summary.pdf (accessed on 16 July 2020).
- Australian Government Department of Health. 2020. Novel Coronavirus (COVID-19): Information for Clinicians. Available online: https://www.health.gov.au/sites/default/files/documents/2020/03/coronavirus-covid-19-information-for-clinicians.pdf (accessed on 16 July 2020).
- Bai, Yan, Lingsheng Yao, Tao Wei, Fei Tian, Dong-Yan Jin, Lijuan Chen, and Meiyun Wang. 2020. Presumed asymptomatic carrier transmission of COVID-19. JAMA 323: 1406–7. [Google Scholar] [CrossRef] [Green Version]
- Bodas, Moran, and Kobi Peleg. 2020. Self-Isolation Compliance In The COVID-19 Era Influenced By Compensation: Findings from a recent survey in Israel: Public attitudes toward the COVID-19 outbreak and self-isolation: A cross sectional study of the adult population of Israel. Health Affairs 39: 936–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Böhmer, Merle M., Udo Buchholz, Victor M. Corman, Martin Hoch, Katharina Katz, Durdica V. Marosevic, Stefanie Böhm, Tom Woudenberg, Nikolaus Ackermann, and Regina Konrad. 2020. Investigation of a COVID-19 outbreak in Germany resulting from a single travel-associated primary case: A case series. The Lancet Infectious Diseases 20: 920–28. [Google Scholar] [CrossRef]
- Burke, Rachel M., Claire M. Midgley, Alissa Dratch, Marty Fenstersheib, Thomas Haupt, Michelle Holshue, Isaac Ghinai, M. Claire Jarashow, Jennifer Lo, and Tristan D. McPherson. 2020. Active monitoring of persons exposed to patients with confirmed COVID-19—United States, January–February 2020. Morbidity and Mortality Weekly Report 69: 245. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Hao-Yuan, Shu-Wan Jian, Ding-Ping Liu, Ta-Chou Ng, Wan-Ting Huang, and Hsien-Ho Lin. 2020. Contact tracing assessment of COVID-19 transmission dynamics in Taiwan and risk at different exposure periods before and after symptom onset. JAMA Internal Medicine 180: 1156–63. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 National Incident Room Surveillance Team. 2020. COVID-19, Australia: Epidemiology Report 20: Fortnightly Reporting Period Ending 5 July 2020. Communicable Diseases Intelligence 44: 1–31. [Google Scholar] [CrossRef]
- De Wit, Emmie, Neeltje Van Doremalen, Darryl Falzarano, and Vincent J. Munster. 2016. SARS and MERS: Recent insights into emerging coronaviruses. Nature Reviews Microbiology 14: 523. [Google Scholar] [CrossRef]
- Dickens, Borame L., Joel R. Koo, Annelies Wilder-Smith, and Alex R. Cook. 2020. Institutional, not home-based, isolation could contain the COVID-19 outbreak. The Lancet 395: 1541–42. [Google Scholar] [CrossRef]
- Ferguson, Neil, Daniel Laydon, Gemma Nedjati-Gilani, Natsuko Imai, Kylie Ainslie, Marc Baguelin, Sangeeta Bhatia, Adhiratha Boonyasiri, Zulma M. Cucunubá, Gina Cuomo-Dannenburg, and et al. 2020. Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand. Imperial College London. [Google Scholar] [CrossRef]
- Gao, Zan, Jung Eun Lee, Daniel J. McDonough, and Callie Albers. 2020. Virtual Reality Exercise as a Coping Strategy for Health and Wellness Promotion in Older Adults during the COVID-19 Pandemic. Journal of Clinical Medicine 9: 1986. [Google Scholar] [CrossRef]
- Geard, Nicholas, James M. McCaw, Alan Dorin, Kevin B. Korb, and Jodie McVernon. 2013. Synthetic population dynamics: A model of household demography. Journal of Artificial Societies and Social Simulation 16: 8. [Google Scholar] [CrossRef]
- Gudbjartsson, Daniel F., Agnar Helgason, Hakon Jonsson, Olafur T. Magnusson, Pall Melsted, Gudmundur L. Norddahl, Jona Saemundsdottir, Asgeir Sigurdsson, Patrick Sulem, and Arna B. Agustsdottir. 2020. Spread of SARS-CoV-2 in the Icelandic population. New England Journal of Medicine 382: 2302–15. [Google Scholar] [CrossRef]
- Gungoraydinoglu, Ali, Ilke Öztekin, and Özde Öztekin. 2021. The Impact of COVID-19 and Its Policy Responses on Local Economy and Health Conditions. Journal of Risk and Financial Management 14: 233. [Google Scholar] [CrossRef]
- Hassan, Mohammad Mahmudul, Md Abul Kalam, Shahanaj Shano, Md Raihan Khan Nayem, Md Kaisar Rahman, Shahneaz Ali Khan, and Ariful Islam. 2020. Assessment of Epidemiological Determinants of COVID-19 Pandemic Related to Social and Economic Factors Globally. Journal of Risk and Financial Management 13: 194. [Google Scholar] [CrossRef]
- He, Xi, Eric H. Y. Lau, Peng Wu, Xilong Deng, Jian Wang, Xinxin Hao, Yiu Chung Lau, Jessica Y Wong, Yujuan Guan, and Xinghua Tan. 2020. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nature Medicine 26: 672–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hicks, Peter, Sue Huckson, Emma Fenney, Isobel Leggett, David Pilcher, and Edward Litton. 2019. The financial cost of intensive care in Australia: A multicentre registry study. Medical Journal of Australia 211: 324–25. [Google Scholar] [CrossRef] [Green Version]
- Ji, Yunpeng, Zhongren Ma, Maikel P. Peppelenbosch, and Qiuwei Pan. 2020. Potential association between COVID-19 mortality and health-care resource availability. The Lancet Global Health 8: e480. [Google Scholar] [CrossRef] [Green Version]
- Jing, Qin-Long, Ming-Jin Liu, Zhou-Bin Zhang, Li-Qun Fang, Jun Yuan, An-Ran Zhang, Natalie E. Dean, Lei Luo, Meng-Meng Ma, and Ira Longini. 2020. Household secondary attack rate of COVID-19 and associated determinants in Guangzhou, China: A retrospective cohort study. The Lancet Infectious Diseases 20: 1141–50. [Google Scholar] [CrossRef]
- Li, Wei, Bo Zhang, Jianhua Lu, Shihua Liu, Zhiqiang Chang, Cao Peng, Xinghua Liu, Peng Zhang, Yan Ling, and Kaixiong Tao. 2020. Characteristics of household transmission of COVID-19. Clinical Infectious Diseases 71: 1943–46. [Google Scholar] [CrossRef]
- Liu, Jiaye, Xuejiao Liao, Shen Qian, Jing Yuan, Fuxiang Wang, Yingxia Liu, Zhaoqin Wang, Fu-Sheng Wang, Lei Liu, and Zheng Zhang. 2020. Community transmission of severe acute respiratory syndrome coronavirus 2, Shenzhen, China, 2020. Emerging Infectious Diseases 26: 1320. [Google Scholar] [CrossRef] [PubMed]
- Lu, Hongzhou, Charles W Stratton, and Yi-Wei Tang. 2020. Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle. Journal of Medical Virology 92: 401–2. [Google Scholar] [CrossRef] [Green Version]
- Niwa, Makoto, Yasushi Hara, Shintaro Sengoku, and Kota Kodama. 2020. Effectiveness of Social Measures against COVID-19 Outbreaks in Selected Japanese Regions Analyzed by System Dynamic Modeling. International Journal of Environmental Research and Public Health 17: 6238. [Google Scholar] [CrossRef] [PubMed]
- NSW Government. 2020. Quarantine Arrangements for International Travellers. Available online: https://www.nsw.gov.au/covid-19/what-you-can-and-cant-do-under-rules/quarantine (accessed on 16 July 2020).
- Oke, Jason, and Carl Heneghan. 2020. Global Covid-19 Case Fatality Rates. Centre for Evidence-Based Medicine: University of Oxford. Available online: https://www.cebm.net/covid-19/global-covid-19-case-fatality-rates/ (accessed on 14 February 2021).
- Park, Shin Young, Young-Man Kim, Seonju Yi, Sangeun Lee, Baeg-Ju Na, Chang Bo Kim, Jung-il Kim, Hea Sook Kim, Young Bok Kim, and Yoojin Park. 2020. Coronavirus disease outbreak in call center, South Korea. Emerging Infectious Diseases 26: 1666. [Google Scholar] [CrossRef]
- Regmi, Krishna, and Cho Mar Lwin. 2021. Factors Associated with the Implementation of Non-Pharmaceutical Interventions for Reducing Coronavirus Disease 2019 (COVID-19): A Systematic Review. International Journal of Environmental Research and Public Health 18: 4274. [Google Scholar] [CrossRef] [PubMed]
- Rothe, Camilla, Mirjam Schunk, Peter Sothmann, Gisela Bretzel, Guenter Froeschl, Claudia Wallrauch, Thorbjörn Zimmer, Verena Thiel, Christian Janke, and Wolfgang Guggemos. 2020. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. New England Journal of Medicine 382: 970–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- She, Jun, Jinjun Jiang, Ling Ye, Lijuan Hu, Chunxue Bai, and Yuanlin Song. 2020. 2019 novel coronavirus of pneumonia in Wuhan, China: Emerging attack and management strategies. Clinical and Translational Medicine 9: 1–7. [Google Scholar] [CrossRef]
- Siachpazidou, Dimitra I., Ourania S. Kotsiou, Grigorios Chatziparasidis, Dimitrios Papagiannis, George D. Vavougios, Eudoxia Gogou, Vasileios T. Stavrou, and Konstantinos I. Gourgoulianis. 2021. Action and Reaction of Pre-Primary and Primary School-Age Children to Restrictions during COVID-19 Pandemic in Greece. Journal of Personalized Medicine 11: 451. [Google Scholar] [CrossRef]
- Tang, Biao, Francesca Scarabel, Nicola Luigi Bragazzi, Zachary McCarthy, Michael Glazer, Yanyu Xiao, Jane M. Heffernan, Ali Asgary, Nicholas Hume Ogden, and Jianhong Wu. 2020. De-Escalation by Reversing the Escalation with a Stronger Synergistic Package of Contact Tracing, Quarantine, Isolation and Personal Protection: Feasibility of Preventing a COVID-19 Rebound in Ontario, Canada, as a Case Study. Biology 9: 100. [Google Scholar] [CrossRef]
- Van Doremalen, Neeltje, Trenton Bushmaker, Dylan H. Morris, Myndi G. Holbrook, Amandine Gamble, Brandi N. Williamson, Azaibi Tamin, Jennifer L. Harcourt, Natalie J. Thornburg, and Susan I. Gerber. 2020. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. New England Journal of Medicine 382: 1564–67. [Google Scholar] [CrossRef]
- Verity, Robert, Lucy C. Okell, Ilaria Dorigatti, Peter Winskill, Charles Whittaker, Natsuko Imai, Gina Cuomo-Dannenburg, Hayley Thompson, Patrick GT Walker, and Han Fu. 2020. Estimates of the severity of coronavirus disease 2019: A model-based analysis. The Lancet Infectious Diseases 20: 669–77. [Google Scholar] [CrossRef]
- WA Government. 2020. Paying for Hotel Quarantine in WA Frequently Asked Questions. Available online: https://www.wa.gov.au/government/publications/paying-hotel-quarantine-wa-frequently-asked-questions (accessed on 16 July 2020).
- Wang, Zhongliang, Wanli Ma, Xin Zheng, Gang Wu, and Ruiguang Zhang. 2020. Household transmission of SARS-CoV-2. Journal of Infection 81: 179–82. [Google Scholar] [CrossRef] [PubMed]
- Xu, Yi, Xufang Li, Bing Zhu, Huiying Liang, Chunxiao Fang, Yu Gong, Qiaozhi Guo, Xin Sun, Danyang Zhao, and Jun Shen. 2020. Characteristics of pediatric SARS-CoV-2 infection and potential evidence for persistent fecal viral shedding. Nature Medicine 26: 502–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Juanjuan, Maria Litvinova, Yuxia Liang, Yan Wang, Wei Wang, Shanlu Zhao, Qianhui Wu, Stefano Merler, Cécile Viboud, and Alessandro Vespignani. 2020. Changes in contact patterns shape the dynamics of the COVID-19 outbreak in China. Science 368: 1481–86. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Shi, Qianyin Lin, Jinjun Ran, Salihu S. Musa, Guangpu Yang, Weiming Wang, Yijun Lou, Daozhou Gao, Lin Yang, and Daihai He. 2020. Preliminary estimation of the basic reproduction number of novel coronavirus (2019-nCoV) in China, from 2019 to 2020: A data-driven analysis in the early phase of the outbreak. International Journal of Infectious Diseases 92: 214–17. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Yanshan, Conor J. Bloxham, Katina D. Hulme, Jane E. Sinclair, Zhen Wei Marcus Tong, Lauren E. Steele, Ellesandra C. Noye, Jiahai Lu, Keng Yih Chew, and Janessa Pickering. 2020. Children are unlikely to have been the primary source of household SARS-CoV-2 infections. medRxiv. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Scenario 1 (Hotel Isolation) | Scenario 2 (Home Isolation) |
|---|---|---|
| Quarantine Cost | ||
| NSW | AU$3000.00 per person | |
| WA | AU$2520.00 per person | |
| Household Secondary Attack Rate (HSAR) | 25.03% | |
| Age-dependent Hospitalisation (ICU Requirement) Rate: | ||
| 0–9 | 0.062% (0.018%) | |
| 10–19 | 0.062% (0.018%) | |
| 20–29 | 0.78% (0.23%) | |
| 30–39 | 2.9% (0.85%) | |
| 40–49 | 5.1% (1.5%) | |
| 50–59 | 9.9% (2.9%) | |
| 60–69 | 15.5% (4.44%) | |
| 70–79 | 35.8% (10.5%) | |
| 80+ | 65.9% (19.4%) | |
| Ward Stay: Median | ||
| <20 | 5 | |
| 20–59 | 6 | |
| 60+ | 9 | |
| ICU Stay: Median | ||
| <20 | 0 | |
| 20–59 | 13 | |
| 60+ | 21 | |
| Ward Cost | AU$1800 per night | |
| ICU Cost | AU$5000 per night |
| Parameter | NSW–Sydney | NSW–Rest | WA–Perth | WA–Rest | Source |
|---|---|---|---|---|---|
| Initial population size | 4,496,259 | 2,971,159 | 1,847,107 | 620,972 | Australian Bureau of Statistics (2016) |
| Mortality probabilities | By year of age | Australian Bureau of Statistics (2016) | |||
| Fertility probabilities | By year of age | Australian Bureau of Statistics (2016) | |||
| Birth gap | mean: 365 days; SD: 90 days | Geard et al. (2013) | |||
| Couple formation parameters | age range: 18–60 years; annual probability: 7.5% | Geard et al. (2013) | |||
| Partner age difference | mean: 2 years; SD: 2 years | Geard et al. (2013) | |||
| Couple dissolution parameters | age range: 18–60; annual probability: 1.5% | Geard et al. (2013) | |||
| Leaving home parameters | minimum age: 18; annual probability: 0.8% | Geard et al. (2013) | |||
| Region | Count | Mean | STD | Min | 25% | 50% | 75% | Max |
|---|---|---|---|---|---|---|---|---|
| NSW—Sydney | 3953 | 892.03 | 1652.47 | 1.44 | 85.02 | 170.04 | 834.80 | 15,208.53 |
| NSW—Rest | 3974 | 1215.59 | 1975.41 | 1.44 | 86.46 | 323.25 | 1004.30 | 14,752.45 |
| WA—Perth | 3891 | 906.91 | 1680.62 | 1.44 | 85.02 | 178.43 | 834.80 | 14,730.37 |
| WA—Rest | 3940 | 1003.72 | 1731.57 | 1.44 | 86.46 | 323.25 | 837.69 | 14,731.81 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melia, A.; Lee, D.; Mahmoudi, N.; Li, Y.; Paolucci, F. Cost-Effectiveness Analysis of COVID-19 Case Quarantine Strategies in Two Australian States: New South Wales and Western Australia. J. Risk Financial Manag. 2021, 14, 305. https://doi.org/10.3390/jrfm14070305
Melia A, Lee D, Mahmoudi N, Li Y, Paolucci F. Cost-Effectiveness Analysis of COVID-19 Case Quarantine Strategies in Two Australian States: New South Wales and Western Australia. Journal of Risk and Financial Management. 2021; 14(7):305. https://doi.org/10.3390/jrfm14070305
Chicago/Turabian StyleMelia, Adrian, Doowon Lee, Nader Mahmoudi, Yameng Li, and Francesco Paolucci. 2021. "Cost-Effectiveness Analysis of COVID-19 Case Quarantine Strategies in Two Australian States: New South Wales and Western Australia" Journal of Risk and Financial Management 14, no. 7: 305. https://doi.org/10.3390/jrfm14070305