Nutritional Rehabilitation of HIV-Exposed Infants in Malawi: Results from the Drug Resources Enhancement Against AIDS and Malnutrition Program


Abstract
:1. Introduction
2. Sample and Methods
2.1. Procedures

{kind=link}
| Demographic, social and housing features of the study population | % |
|---|---|
| Inadequate housing | 27% |
| Access to drinking water | 22% |
| Access to hygienic toilets | 6% |
| Access to electrical power | 28% |
| Maternal illiteracy | 11% |
| Unemployment | 84% |
2.2. DREAM Malnutrition Program
2.3. Nutritional Counselling
- Vicious cycle of HIV, malnutrition, infection;
- Macronutrients, vitamins, micronutrients: their functions and needs;
- Food groups and dietary diversity;
- Health and a balanced diet;
- Feeding of healthy and sick children;
- Nutritional care of malnourished children;
- Promotion of breastfeeding;
- Nutritional advice on weaning and complementary feeding;
- Water and food hygiene.
2.4. Anthropometric Assessments and Classification of Malnutrition
2.5. Food Survey and Calculation of Nutritional Intake
2.6. Statistical Analysis
3. Results
| Anthropometric characteristics of study subjects at baseline and on follow-up. | Admission (n = 36) | 6 month follow-up (n = 36) | p-value * |
|---|---|---|---|
| Age (months), mean (SD) | 11.8 ± 3.0 | 17.7 ± 2.9 | |
| Weight, mean (SD) kg | 6.7 ± 0.91 | 8.2 ± 0.92 | <0.0001 |
| Height, mean (SD) cm | 67.4 ± 3.87 | 72.4 ± 3.44 | <0.0001 |
| Middle upper arm circumference, mean (SD) cm | 12.8 ± 1.21 | 14.58 ± 1.25 | <0.0001 |
| Weight for age z-score, mean (SD) | −2.96 ± 0.77 | −2.31 ± 0.73 | <0.0001 |
| Height for age z-score, mean (SD) | −3.03 ± 1.13 | −3.31 ± 0.96 | 0.011 |
| Weight for height z-score, mean (SD) | −1.78 ± 1.06 | −0.88 ± 0.83 | 0.007 |
| Children with bilateral edema n. % | 4 (11) | 0 | |
| Children with Severe Acute Malnutrition, n (%) (MUAC <115 mm and/or Bilateral oedema and/or WHZ < −3) | 12 (33) | 0 | |
| Children with Moderate Acute Malnutrition, n (%) (MUAC < 119 mm and/or WHZ < −2 and/or WAZ < −3 and/or two consecutive static or declining weights) | 24 (67) | 6 (16) | |
| Growth Velocity z-score at follow-up, mean (SD) | −1.27 ± 1.3 |
| Growth velocity z-score according to malaria status | Children with malaria (n = 17) | Children without malaria (n = 19) | P-value * |
|---|---|---|---|
| Height gain at follow-up, mean (SD) | 4.4 ± 1.7 | 5.6 ± 1.7 | p < 0.048 (CL95% 2.32 − 0.01) |
| Growth Velocity z-score at follow-up, mean (SD) | −1.6 ± 1.2 | 0.82 ± 1.2 | p < 0.046 (CL95% 1.7 − 0.01) |
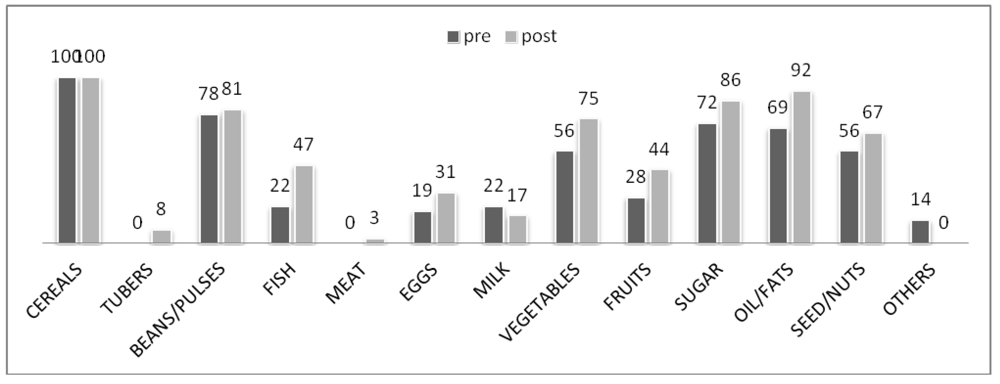
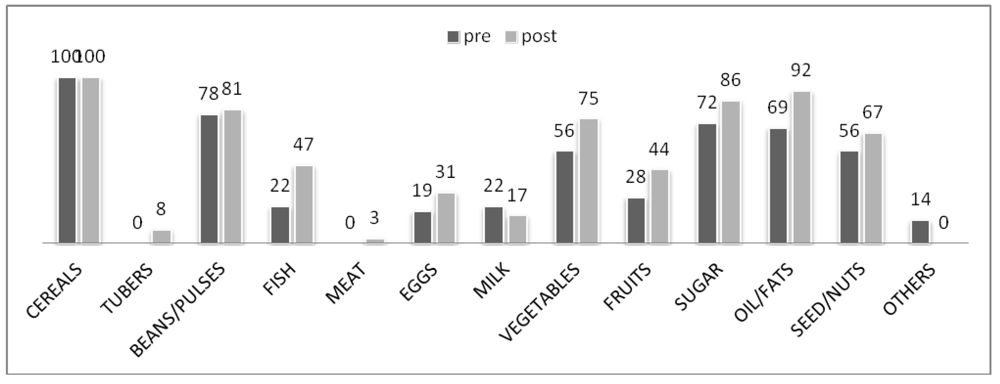
| Dietary characteristics of the population | Admission | Follow-up | p-value |
|---|---|---|---|
| Number meals, mean (SD) | 4 ± 1 | 5 ± 1 | 0.050 |
| Dietary diversity score, mean (SD) | 5.3 ± 1.9 | 6.5 ± 1.3 | 0.012 |
| Energy, mean (SD), Kcal | 916 ± 391 | 1,180 ± 342 | 0.003 |
| Proteins, mean (SD), g | 31 ± 17 | 42 ± 16 | 0.010 |
| Fats, mean (SD), g | 27 ± 19 | 35 ± 18 | NS |
| Carbohydrates, mean (SD), g | 135 ± 55 | 170 ± 51 | 0.006 |
| Percentage of children with energy intake lower than 75% of Required Daily Amount-RDA (WHO/FAO) n (%) | 14 (39) | 10 (27.8) | |
| Percentage of children with protein intake lower than 75% of Required Daily Amount-RDA (WHO/FAO) n (%) | 4 (11) | 0 |
4. Discussion
5. Conclusions
Acknowledgments
Conflict of Interest
References
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar]
- Bhutta, Z.A.; Ahmed, T.; Black, R.E.; Cousens, S.; Dewey, K.; Giugliani, E.; Haider, B.A.; Kirkwood, B.; Morris, S.S.; Sachdev, H.P.; Shekar, M. Maternal and Child Undernutrition Study Group. What works? Interventions for maternal and child undernutrition and survival. Lancet 2008, 371, 417–440. [Google Scholar]
- Briend, A.; Prudhon, C.; Prinzo, Z.W.; Daelmans, B.M.; Mason, J.B. Putting the management of severe malnutrition back on the international health agenda. Food Nutr. Bull. 2006, 27, S3–S6. [Google Scholar]
- Fergusson, P.; Chikaphupha, K.; Bongololo, G.; Makwiza, I.; Nyirenda, L.; Chinkhumba, J.; Aslam, A.; Theobald, S. Quality of care in nutritional rehabilitation in HIV-endemic Malawi: Caregiver perspectives. Matern. Child Nutr. 2010, 6, 89–100. [Google Scholar]
- Mason, J.B.; Bailes, A.; Mason, K.E.; Yambi, O.; Jonsson, U.; Hudspeth, C.; Hailey, P.; Kendle, A.; Brunet, D.; Martel, P. AIDS, drought, and child malnutrition in southern Africa. Public Health Nutr. 2005, 8, 551–563. [Google Scholar]
- Thurstans, S.; Kerac, M.; Maleta, K.; Banda, T.; Nesbitt, A. HIV prevalence in severely malnourished children admitted to nutrition rehabilitation units in Malawi: Geographical & seasonal variations a cross-sectional study. BMC Pediatr. 2008, 8. [Google Scholar]
- Victora, C.G.; Adair, L.; Fall, C.; Hallal, P.C.; Martorell, R.; Richter, L.; Sachdev, H.S. Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Consequences for adult health and human capital. Lancet 2008, 371, 340–357. [Google Scholar]
- Victora, C.G.; de Onis, M.; Hallal, P.C.; Blössner, M.; Shrimpton, R. Worldwide timing of growth faltering: Revisiting implications for interventions. Pediatrics 2010, 125, e473–e480. [Google Scholar]
- Lin, C.A.; Manary, M.J.; Maleta, K.; Briend, A.; Ashorn, P. An energy-dense complementary food is associated with a modest increase in weight gain when compared with a fortified porridge in Malawian children aged 6–18 months. J. Nutr. 2008, 138, 593–598. [Google Scholar]
- Ashworth, A.; Ferguson, E. Dietary Counselling in the Management of Moderately Malnourished Children; WHO Technical Background Paper: London, UK, 2008; pp. 1–37. [Google Scholar]
- Penny, M.E.; Creed-Kanashiro, H.M.; Robert, R.C.; Narro, M.R.; Caulfield, L.E.; Black, R.E. Effectiveness of an educational intervention delivered through the health services to improve nutrition in young children: A cluster-randomised controlled trial. Lancet 2005, 365, 1863–1872. [Google Scholar]
- Gakidou, E.; Cowling, K.; Lozano, R.; Murray, C.J.L. Increased educational attainment and its effect on child mortality in 175 countries between 1970 and 2009: A systematic analysis. Lancet 2010, 376, 959–974. [Google Scholar]
- Hotz, C.; Gibson, R.S. Participatory nutrition education and adoption of new feeding practices are associated with improved adequacy of complementary diets among rural Malawian children: A pilot study. Eur. J. Clin. Nutr. 2005, 59, 226–237. [Google Scholar]
- Newell, M.L.; Borja, M.C.; Peckham, C. Height, weight, and growth in children born to mothers with HIV-1 infection in Europe. Pediatrics 2003, 111, e52–e60. [Google Scholar] [CrossRef]
- Arpadi, S.; Fawzy, A.; Aldrovandi, G.M.; Kankasa, C.; Sinkala, M.; Mwiya, M.; Thea, D.M.; Kuhn, L. Growth faltering due to breastfeeding cessation in uninfected children born to HIV-infected mothers in Zambia. Am. J. Clin. Nutr. 2009, 90, 344–353. [Google Scholar]
- Newell, M.L.; Coovadia, H.; Cortina-Borja, M.; Rollins, N.; Gaillard, P.; Dabis, F. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: A pooled analysis. Lancet 2004, 364, 1236–1243. [Google Scholar]
- Creek, T.L.; Kim, A.; Lu, L.; Bowen, A.; Masunge, J.; Arvelo, W.; Smit, M.; Mach, O.; Legwaila, K.; Motswere, C.; et al. Hospitalization and mortality among primarily nonbreastfed children during a large outbreak of diarrhea and malnutrition in Botswana, 2006. J. Acquir. Immune Defic. Syndr. 2010, 53, 14–19. [Google Scholar] [CrossRef]
- Kuhn, L.; Aldrovandi, G.M.; Sinkala, M.; Kankasa, C.; Semrau, K.; Mwiya, M.; Kasonde, P.; Scott, N.; Vwalika, C.; Walter, J.; et al. Effects of early, abrupt weaning on HIV-free survival of children in Zambia, Zambia Exclusive Breastfeeding Study. N. Engl. J. Med. 2008, 359, 130–141. [Google Scholar]
- Marazzi, C.M.; Germano, P.; Liotta, G.; Guidotti, G.; Loureiro, S.; Gomes-Ada, C.; Blazquez, M.C.; Narciso, P.; Perno, C.F.; Mancinelli, S.; et al. Implementing antiretroviral triple therapy to prevent HIV mother-to-child transmission: A public health approach in resource-limited settings. Eur. J. Pediatr. 2007, 166, 1305–1307. [Google Scholar] [CrossRef] [Green Version]
- de Vincenzi, I. Kesho Bora Study Group. Triple antiretroviral compared with zidovudine and single-dose nevirapine prophylaxis during pregnancy and breastfeeding for prevention of mother-to-child transmission of hiv-1 (Kesho Bora study): A randomised controlled trial. Lancet Infect. Dis. 2011, 11, 171–180. [Google Scholar] [CrossRef]
- WHO Rapid Advice: Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants; WHO: Geneva, Switzerland, November 30 2009; Revised June 2010.
- WHO Rapid Advice: HIV and Infant Feeding. Revised Principles and Recommendations; WHO: Geneva, Switzerland, November 2009.
- Palombi, L.; Marazzi, M.C.; Voetberg, A.; Magid, N.A. Treatment acceleration program and the experience of the DREAM program in prevention of mother-to-child transmission of HIV. AIDS 2007, 21, S65–S71. [Google Scholar]
- Giuliano, M.; Guidotti, G.; Andreotti, M.; Pirillo, M.F.; Villani, P.; Liotta, G.; Marazzi, M.C.; Mancini, M.G.; Cusato, M.; Germano, P.; et al. Triple antiretroviral prophylaxis administered during pregnancy and after delivery significantly reduces breast milk viral load: A study within the Drug Resource Enhancement Against AIDS and Malnutrition program. J. Acquir. Immune Defic. Syndr. 2007, 44, 286–291. [Google Scholar] [CrossRef]
- Marazzi, M.C.; Germano, P.; Liotta, G.; Buonomo, E.; Guidotti, G.; Palombi, L. Pediatric highly active antiretroviral therapy in Mozambique: An integrated model of care. Minerva Pediatr. 2006, 58, 483–490. [Google Scholar]
- Magnano San Lio, M.; Mancinelli, S.; Palombi, L.; Buonomo, E.; Altan, A.D.; Germano, P.; Magid, N.A.; Pesaresi, A.; Renzi, E.; Scarcella, P.; et al. The DREAM model’s effectiveness in health promotion of AIDS patients in Africa. Health Promot. Int. 2009, 24, 6–15. [Google Scholar]
- Marazzi, M.C.; Liotta, G.; Nielsen-Saines, K.; Haswell, J.; Magid, N.A.; Buonomo, E.; Scarcella, P.; Doro Altan, A.M.; Mancinelli, S.; Palombi, L. Extended antenatal antiretroviral use correlates with improved infant outcomes throughout the first year of life. AIDS 2010, 24, 2819–2826. [Google Scholar] [Green Version]
- Marazzi, M.C.; Nielsen-Saines, K.; Buonomo, E.; Scarcella, P.; Germano, P.; Majid, N.A.; Zimba, I.; Ceffa, S.; Palombi, L. Increased infant human immunodeficiency virus-type one free survival at one year of age in Sub-Saharan Africa with maternal use of highly active antiretroviral therapy during breastfeeding. Pediatr. Infect. Dis. J. 2009, 28, 483–487. [Google Scholar]
- Palombi, L.; Buonomo, E.; Scarcella, P.; Doro Altan, A.M.; Nielsen-Saines, K.; Tembo, D.; Zimba, I.; Germano, P.; Marazzi, M.C. Provision of Highly Active Antiretroviral Therapy (HAART) to mothers while breastfeeding and nutritional supplementation during the weaning process favorably impact infant growth and survival in African HIV-exposed infants. In Proceedings of the 5th International AIDS Society Conference on HIV Pathogenesis Treatment and Prevention, Cape Town, South Africa, July 2009.
- Nucita, A.; Bernava, G.M.; Bartolo, M.; Masi, F.D.; Giglio, P.; Peroni, M.; Pizzimenti, G.; Palombi, L. A global approach to the management of EMR (electronic medical records) of patients with HIV/AIDS in Sub-Saharan Africa: The experience of DREAM software. BMC Med. Inform. Decis. Mak. 2009, 9. [Google Scholar]
- WHO Anthro for Personal Computers, Version 3.1; Software for Assessing Growth and Development of the World’s Children, WHO: Geneva, Switzerland, 2010; (accessed on 12 January 2012). Available online: http://www.who.int/childgrowth/software/en/.
- Interim Guidelines for the Management of Acute Malnutrition; Government of Malawi, Ministry of Health: Blantyre, Malawi, 2006.
- WHO (WHO Multicentre Growth Reference Study Group). WHO child growth standards based on length/height, weight and age. Acta Paediatr. 2006, 450S, 76–85.
- Guidelines for the Management of Moderate Acute Malnutrition; Government of Malawi, Ministry of Health: Blantyre, Malawi, 2006.
- WHO Child Growth Standards and the Identification of Severe Acute Malnutrition in Infants and Children; WHO/UNICEF: Geneva, Switzerland, 2009.
- Arimond, M.; Ruel, M.T. Dietary diversity is associated with child nutritional status: Evidence from 11 demographic and health surveys. J. Nutr. 2004, 134, 2579–2585. [Google Scholar]
- Rah, J.H.; Akhter, N.; Semba, R.D.; de Pee, S.; Bloem, M.W.; Campbell, A.A.; Moench-Pfanner, R.; Sun, K.; Badham, J.; Kraemer, K. Low dietary diversity is a predictor of child stunting in rural Bangladesh. Eur. J. Clin. Nutr. 2010, 64, 1393–1398. [Google Scholar]
- Lunney, K.M.; Jenkins, A.L.; Tavengwa, N.V.; Majo, F.; Chidhanguro, D.; Iliff, P.; Strickland, G.T.; Piwoz, E.; Iannotti, L.; Humphrey, J.H. HIV-positive poor women may stop breastfeeding early to protect their infants from HIV infection although available replacement diets are grossly inadequate. J. Nutr. 2008, 138, 351–357. [Google Scholar]
- Keriann, H.P.; Muti, M.; Chasekwa, B.; Mbuya, M.N.N.; Madzima, R.C.; Humphrey, J.H.; Stoltzfus, R.C. Complementary feeding messages that target cultural barriers enhance both the use of lipid-based nutrient supplements and underlying feeding practices to improve infant diets in rural Zimbabwe. Mat. Child. Nutr. 2010, in press. [Google Scholar]
- FAO/WHO/ONU, Human Energy Requirements; WHO: Geneva, Switzerland and Brussels, Belgium, 2001.
- WHO, Protein and Amino Acid Requirements Human Nutrition; WHO Technical Report Series 935; WHO: Geneva, Switzerland and Brussels, Belgium, 2002.
- Food Composition Table for Africa; Food and Agriculture Organization: Rome, Italy, 1970.
- Mumba, P.P.; McDonald, J. Nutrient composition of selected fresh and processed fish species from Lake Malawi: A nutritional possibility for people living with HIV/AIDS. Int. J. Consum. Stud. 2005, 29, 72–77. [Google Scholar]
- IBM SPSS-the market leader for predictive analysis. SPSS software for Windows. 2010, version 19.0. Available online: http://www-01.ibm.com/software/analytics/spss (accessed on 26 January 2012).
- Ashworth, A. Efficacy and effectiveness of community-based treatment of severe malnutrition. Food Nutr. Bull. 2006, 27, S24–S48. [Google Scholar]
- Berkley, J.A.; Bejon, P.; Mwangi, T.; Gwer, S.; Maitland, K.; Williams, T.N.; Mohammed, S.; Osier, F.; Kinyanjui, S.; Fegan, G.; et al. HIV infection, malnutrition, and invasive bacterial infection among children with severe malaria. Clin. Infect. Dis. 2009, 49, 336–343. [Google Scholar]
- Scarcella, P.; Buonomo, E.; Zimba, I.; Doro Altan, A.M.; Germano, P.; Palombi, L.; Marazzi, M.C. The impact of integrating food supplementation, nutritional education and HAART (highly active antiretroviral therapy) on the nutritional status of patients living with HIV/AIDS in Mozambique: Results from the DREAM programme. Ig. Sanita. Pubbl. 2011, 67, 41–52. [Google Scholar]
- Petrou, S.; Kupek, E. Poverty and childhood undernutrition in developing countries: A multi-national cohort study. Soc. Sci. Med. 2010, 71, 1366–1373. [Google Scholar]
- Shapiro, R.L.; Lockman, S. Mortality among HIV-exposed infants: The first and final frontier. Clin. Infect. Dis. 2010, 50, 445–447. [Google Scholar]
- Nyakeriga, A.M.; Troye-Blomberg, M.; Chemtai, A.K.; Marsh, K.; Williams, T.N. Malaria and nutritional status in children living on the coast of Kenya. Am. J. Clin. Nutr. 2004, 80, 1604–1610. [Google Scholar]
- Olney, D.K.; Kariger, P.K.; Stoltzfus, R.J.; Khalfan, S.S.; Ali, N.S.; Tielsch, J.M.; Sazawal, S.; Black, R.; Allen, L.H.; Pollitt, E. Development of nutritionally at-risk young children is predicted by malaria, anemia, and stunting in Pemba, Zanzibar. J. Nutr. 2009, 139, 763–772. [Google Scholar] [CrossRef]
- Deen, J.L.; Walraven, G.E.; von Seidlein, L. Increased risk for malaria in chronically malnourished children under 5 years of age in rural Gambia. J. Trop. Pediatr. 2002, 48, 78–83. [Google Scholar]
- Ehrhardt, S.; Burchard, G.D.; Mantel, C.; Cramer, J.P.; Kaiser, S.; Kubo, M.; Otchwemah, R.N.; Bienzle, U.; Mockenhaupt, F.P. Malaria, anemia, and malnutrition in African children-defining intervention priorities. J. Infect. Dis. 2006, 194, 108–114. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Buonomo, E.; De Luca, S.; Tembo, D.; Scarcella, P.; Germano, P.; Doro Altan, A.M.; Palombi, L.; Liotta, G.; Nielsen-Saines, K.; Erba, F.; et al. Nutritional Rehabilitation of HIV-Exposed Infants in Malawi: Results from the Drug Resources Enhancement Against AIDS and Malnutrition Program. Int. J. Environ. Res. Public Health 2012, 9, 421-434. https://doi.org/10.3390/ijerph9020421
Buonomo E, De Luca S, Tembo D, Scarcella P, Germano P, Doro Altan AM, Palombi L, Liotta G, Nielsen-Saines K, Erba F, et al. Nutritional Rehabilitation of HIV-Exposed Infants in Malawi: Results from the Drug Resources Enhancement Against AIDS and Malnutrition Program. International Journal of Environmental Research and Public Health. 2012; 9(2):421-434. https://doi.org/10.3390/ijerph9020421
Chicago/Turabian StyleBuonomo, Ersilia, Simona De Luca, Dyna Tembo, Paola Scarcella, Paola Germano, Anna Maria Doro Altan, Leonardo Palombi, Giuseppe Liotta, Karin Nielsen-Saines, Fulvio Erba, and et al. 2012. "Nutritional Rehabilitation of HIV-Exposed Infants in Malawi: Results from the Drug Resources Enhancement Against AIDS and Malnutrition Program" International Journal of Environmental Research and Public Health 9, no. 2: 421-434. https://doi.org/10.3390/ijerph9020421