Is the Health and Wellbeing of University Students Associated with their Academic Performance? Cross Sectional Findings from the United Kingdom

Abstract
:1. Introduction
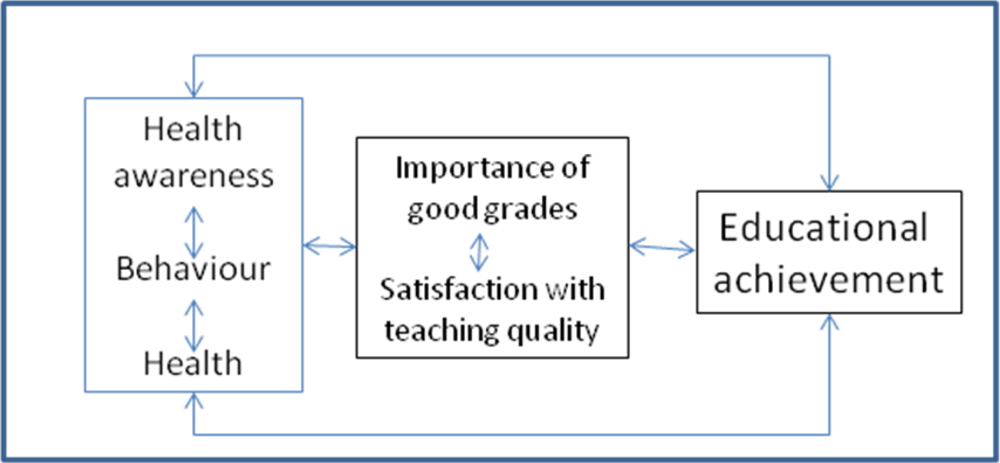
1.2. Conceptual Framework
1.3. Aim of the Study
2. Methods
2.1. Data Collection Procedures
2.2. Students’ Satisfaction Questionnaire and Marks
- Module ran smoothly
- Module increased my interest in the subject
- Module team provided opportunity to ask questions
- Module material was well presented
- Module was thought provoking
- Module assessment methods were appropriate
- Module team displayed good knowledge
- Module team correctly assumed level of skills I had
- Module information available at beginning of module
- Received helpful feedback
- Seminar group sizes were small enough
- References needed for module available in library
- Work required for module was appropriate
- Module elements integrated into meaningful whole
- Module was intellectually stimulating
- Module is expected to be of direct use in my career
- Module made me look at my profession differently
- Module team styles were clear/informative/stimulating
- *Each item was rated on 5-point Likert scale (1 = very positive evaluation, 5 = very negative evaluation).
2.3. Health & Wellbeing Questionnaire
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusion
Acknowledgments
References
- National Commission on the Role of the School and the Community to Improve Adolescent Health. Code Blue: Uniting for Healthier Youth; National Association of State Boards of Education: Alexandria, VA, USA, 1990.
- Novello, AC; Degraw, C; Kleinman, D. Healthy Children Ready to Learn: an Essential Collaboration between Health and Education. Public Health Rep 1992, 107, 3–15. [Google Scholar]
- Tsouros, AD; Dowding, G; Thompson, J; Dooris, M. Health Promoting Universities—Concept, Experience and Framework for Action; World Health Organization: Copenhagen, Denmark, 1998. [Google Scholar]
- O’Donnell, T; Gray, G. The Health Promoting College; Health Education Authority: London, UK, 1993. [Google Scholar]
- Murray, NG; Low, BJ; Hollis, C; Cross, AW; Davis, SM. Coordinated School Health Programs and Academic Achievement: A Systematic Review of the Literature. J. School Health 2007, 77, 589–601. [Google Scholar]
- Trudeau, F; Shephard, RJ. Physical Education, School Physical Activity, School Sports and Academic Achievement. Int. J. Behav. Nutr. Phys. Act 2008, 5, 10. [Google Scholar]
- Keeley, TJH; Fox, KR. The Impact of Physical Activity and Fitness on Academic Achievement and Cognitive Performance in Children. Int. Rev. Sport Exerc. Psychol 2009, 2, 198–214. [Google Scholar]
- Schoenbaum, M; Waidmann, T. Race, Socioeconomic Status and Health: Accounting for Race Differences in Health in the U.S. Elderly. J. Gerontol 1997, 52, 61–73. [Google Scholar]
- Kolbe, LJ. Education Reform and the Goals of Modern School Health Programs. Educ. Stand 2002, 3, 4–11. [Google Scholar]
- Ross, CE; Wu, C. Education, Age, and the Cumulative Advantage in Health. J. Health Soc. Behav 1996, 37, 104–120. [Google Scholar]
- Crum, RM; Ensminger, ME; Ro, MJ; McCord, J. The Association of Educational Achievement and School Dropout with Risk of Alcoholism: a Twenty-Five-Year Prospective Study of Inner-City Children. J. Stud. Alcohol 1998, 59, 318–326. [Google Scholar]
- Kessler, RC; Foster, CL; Saunders, WB; Stang, PE. Social Consequences of Psychiatric Disorders, I: Education Attainment. Am. J. Psychiatry 1995, 152, 1026–1032. [Google Scholar]
- Miller, DS; Miller, TQ. A Test of Socioeconomic Status as a Predictor of Initial Marijuana Use. Addict. Behav 1997, 22, 479–489. [Google Scholar]
- Grossman, M; Kaestner, R. Effects of Education on Health. In The Social Benefits of Education; Berhman, JR, Stacey, N, Eds.; University of Michigan Press: Ann Arbor, MI, USA, 1997. [Google Scholar]
- Nayga, RM, Jr. Schooling, Health Knowledge and Obesity. Appl. Econ 2000, 32, 815–822. [Google Scholar]
- Schorr, LB. Children, Families and the Cycle of Disadvantage. Can. J. Psychiatr 1991, 36, 437–441. [Google Scholar]
- Symons, CW; Cinelli, B. Bridging Student Health Risks and Academic Achievement through Comprehensive School Health Programs. J. School Health 1997, 67, 220–228. [Google Scholar]
- Sculenber, J; Bachman, JG; O’Malley, PM; Johnson, LD. High School Educational Success and Subsequent Substance Use: a Panel Analysis Following Adolescents into Young Adulthood. J. Health Soc. Behav 1994, 35, 45–62. [Google Scholar]
- Eggert, LL; Herting, JR. Drug Involvement among Potential Dropouts and “Typical” Youth. J. Drug Educ 1993, 23, 31–55. [Google Scholar]
- Evans, WP; Skager, R. Academically Successful Drug Users: An Oxymoron? J. Drug Educ 1999, 22, 353–365. [Google Scholar]
- Thorolfur, T; Vilhjalmsson, R. Factors Related to Cigarette Smoking and Alcohol Use among Adolescents. Adolescence 1991, 26, 399–417. [Google Scholar]
- Bouchard, C; Shephard, RJ; Stephens, T; Sutton, JR; McPherson, BD. Exercise, Fitness, and Health: A Consensus of Current Knowledge; Human Kinetics Books: Champaign, IL, USA, 1990. [Google Scholar]
- Centers for Disease Control. Vigorous Physical Activity among High School Students—United States, 1990. JAMA 1992, 267, 1052. [Google Scholar]
- Parker, L. The Relationship between Nutrition and Learning. In A School Employee’s Guide to Information and Action; National Education Association of the United States: Washington, DC, USA, 1989. [Google Scholar]
- Pelican, S; O’Connell, LH; Lewis, C; Byrd-Bredbenner, C. Relationships of Hunger and Malnutrition to Learning Ability and Behavior; Nutrition Education Center of the Pennsylvania State University and the Florida Dept of Citrus: University Park, IL, USA, 1982. [Google Scholar]
- Boot, CR; Donders, NC; Vonk, P; Meijman, FJ. Development of a Student Health Questionnaire: The Necessity of a Symbiosis of Science and Practice. Glob. Health Promot 2009, 16, 35–44. [Google Scholar]
- Wardle, J; Steptoe, A. The European Health and Behaviour Survey: Rationale, Methods and Initial Results for the United Kingdom. Soc. Sci. Med 1991, 33, 925–936. [Google Scholar]
- Al-Kandari, F; Vidal, VL. Correlation of the Health-Promoting Lifestyle, Enrollment Level, and Academic Performance of College of Nursing Students in Kuwait. Nurs. Health Sciences 2007, 9, 112–119. [Google Scholar]
- Hoskins, SL; Newstead, SE; Dennis, I. Degree Performance as a Function of Age, Gender, Prior Qualifications and Discipline Studied. Assess. Eval. Higher Educ 1997, 22, 317–328. [Google Scholar]
- Ofori, R. Age and ‘Type’ of Domain Specific Entry Qualifications as Predictors of Student Nurses’ Performance in Biological, Social and Behavioural Sciences in Nursing Assessments. Nurse Educ. Today 2000, 20, 298–310. [Google Scholar]
- El Ansari, W; Oskrochi, R. What ‘Really’ Affects Health Professions Students’ Satisfaction with their Educational Experience? Implications for Practice and Research. Nurse Educ. Today 2004, 24, 644–655. [Google Scholar]
- El Ansari, W; Oskrochi, R. What Matters Most? Predictors of Student Satisfaction in Public Health Educational Courses. Public Health 2006, 120, 462–473. [Google Scholar]
- Elias, MJ; Gara, MA; Schuyler, TF; Branden-Muller, LR; Sayette, MA. The Promotion of Social Competence: Longitudinal Study of a Preventive School-Based Program. Am. J. Orthopsychiatr 1991, 61, 409–417. [Google Scholar]
- McCord, MT; Klein, JD; Foy, JM; Fothergill, K. School-Based Clinic Use and School Performance. J. Adolesc. Health 1993, 14, 91–98. [Google Scholar]
- Eggert, LL; Thompson, EA; Herting, JR; Nicholas, LJ; Dicker, BG. Preventing Adolescent Drug Abuse and High School Dropout through an Intensive School-Based Social Network Development Program. Am. J. Health Promot 1994, 8, 202–215. [Google Scholar]
- Felner, RD; Jackson, AW; Kasak, D; Mulhall, P; Brand, S; Flowers, N. The Impact of School Reform for the Middle Years. Phi Delta Kappan 1997, 78, 528–532. [Google Scholar]
- Meyers, AF; Sampson, AE; Weitzman, M; Rogers, BL; Kayne, H. School Breakfast Program and School Performance. Am. J. Dis. Child 1989, 143, 1234–1239. [Google Scholar]
- Gall, G; Pagano, ME; Desmond, MS; Perrin, JM; Murphy, JM. Utility of Psychosocial Screening at a School-Based Health Center. J. School Health 2000, 70, 292–298. [Google Scholar]
- Flay, B; Allred, CG; Ordway, C. Effects of the Positive Action Program on Achievement and Discipline: Two Matched-Control Comparisons. Prev. Sci 2001, 2, 71–89. [Google Scholar]
- Dwyer, T; Coonan, WE; Worsley, LA; Leitch, DR. An Assessment of the Effects of Two Physical Activity Programs on Coronary Heart Disease Risk Factors in Primary School Children. Community Health Stud 1979, 3, 196–202. [Google Scholar]
- Evans, D; Clark, NM; Feldman, CH; Rips, J; Kaplan, D; Levison, MJ; Wasilewski, Y; Levin, B; Mellins, RB. A School Health Education Program for Children with Asthma Aged 8−11 Years. Health Educ. Q 1987, 14, 267–279. [Google Scholar]
- Murphy, JM; Pagano, ME; Nachmani, J; Sperling, P; Kane, S; Kleinman, RE. The Relationship of School Breakfast to Psychosocial and Academic Functioning: Cross-Sectional and Longitudinal Observations in an Inner-City School Sample. Arch. Pediatr. Adolesc. Med 1998, 152, 899–907. [Google Scholar]
- Sallis, JF; McKenzie, TL; Kolody, B; Lewis, M; Marshall, S; Rosengard, P. Effects of Health-Related Physical Education on Academic Achievement: Project SPARK. Res. Q. Exerc. Sport 1999, 70, 127–134. [Google Scholar]
- Clark, NM; Brown, R; Joseph, CL; Anderson, EW; Liu, M; Valerio, MA. Effects of a Comprehensive School-Based Asthma Program on Symptoms, Parent Management, Grades, and Absenteeism. Chest 2004, 125, 1674–1679. [Google Scholar]
- Ames, C; Archer, J. Mothers’ Belief about the Role of Ability and Effort in School Learning. J. Educ. Psychol 1987, 79, 409–414. [Google Scholar]
- Maehr, ML. Thoughts about motivation. In Research on Motivation in Education; Ames, C, Ames, R, Eds.; Academic Press: New York, NY, USA, 1989; pp. 299–315. [Google Scholar]
- Elliot, AJ. Integrating the “Classic” and “Contemporary” Approaches to Achievement Motivation: A Hierarchical Model of Approach and Avoidance Achievement Motivation. In Advances in Motivation and Achievement; Maehr, M, Pintrich, P, Eds.; JAI Press: Greenwich, CT, USA, 1997; Volume 10, pp. 243–279. [Google Scholar]
- El Ansari, W; Maxwell, AE; Mikolajczyk, RT; Stock, C; Naydenova, V; Krämer, A. Promoting Public Health: Benefits and Challenges of a Europeanwide Research Consortium on Student Health. Centr. Eur. J. Public Health 2007, 15, 58–65. [Google Scholar]
- Kerridge, JB; Mathews, BP. Student Rating of Courses in HE: Further Challenges and Opportunities. Assess. Eval. Higher Educ 1998, 23, 71–82. [Google Scholar]
- El Ansari, W. Satisfaction Trends in Undergraduate Physiotherapy Education. Physiotherapy 2003, 89, 171–185. [Google Scholar]
- El Ansari, W. Student Nurse Satisfaction Levels with Their Courses: Part I—Effects of Demographic Variables. Nurse Educ. Today 2002, 22, 159–170. [Google Scholar]
- Mikolajczyk, RT; Brzoska, P; Maier, C; Ottova, V; Meier, S; Dudziak, U; Ilieva, S; El Ansari, W. Factors Associated with Self-Rated Health Status in University Students: A Cross-Sectional Study in Three European Countries. BMC Public Health 2008, 18, 215. [Google Scholar]
- Mikolajczyk, RT; El Ansari, W; Maxwell, AE. Food Consumption Frequency and Perceived Stress and Depressive Symptoms among Students in Three European Countries. Nutr. J 2009, 15, 8–31. [Google Scholar]
- Mikolajczyk, RT; Maxwell, AE; El Ansari, W; Naydenova, V; Stock, C; Ilieva, S; Dudziak, U; Naydova, I. Prevalence of Depressive Symptoms in University Students from Germany, Denmark, Poland and Bulgaria. Soc. Psychiatry Psychiatr. Epidemiol 2008, 43, 105–112. [Google Scholar]
- Mikolajczyk, RT; Maxwell, AE; Naydenova, V; Meier, S; El Ansari, W. Depressive Symptoms and Perceived Burdens Related to Being a Student: Survey in Three European Countries. Clin. Pract. Epidemiol. Ment. Health 2008, 4, 19. [Google Scholar]
- Stock, C; Kücük, N; Miseviciene, I; Guillén-Grima, F; Petkeviciene, J; Aguinaga-Ontoso, I; Krämer, A. Differences in Health Complaints Between University Students from Three European Countries. Prev. Med 2003, 37, 535–543. [Google Scholar]
- Stock, C; Mikolajczyk, R; Bloomfield, K; Maxwell, AE; Ozcebe, H; Petkeviciene, J; Naydenova, V; Marin-Fernandez, B; El-Ansari, W; Krämer, A. Alcohol Consumption and Attitudes towards Banning Alcohol Sales on Campus among European University Students. Public Health 2009, 123, 122–129. [Google Scholar]
- Winther Ringgard, L; Birk Nissen, S; Nielsen, GA. Unges Livsstil og Dagligdag 2003; Kræftens Bekæmpelse og; Sundhedsstyrelsen: Copenhagen, Denmark, 2005. [Google Scholar]
- Hurrelmann, K; Kolip, P. [Der Jugendgesundheitssurvey]. In Presseinformationsdienst des SFB 227, No. 11; University of Bielefeld: Bielefeld, Germany, 1994. [Google Scholar]
- American College Health Association. American College Health Association National College Health Assessment (ACHA-NCHA): Spring 2006 Reference Group Report (abridged). J. Am. College Health 2007, 55, 195–206. [Google Scholar]
- Pallant, J. SPSS Survival Manual; Open University Press: Buckingham, UK, 2001. [Google Scholar]
- Kopp, J; Lois, D. Lineare Regression und Beziehungsmuster zwischen Variablen; Technische Universität: Chemnitz, Germany, 2009. [Google Scholar]
- Gatefield, T. Examining Student Satisfaction with Group Projects and Peer Assessment. Assess. Eval. Higher Educ 1999, 24, 365–377. [Google Scholar]
- Ahamed, Y; MacDonald, H; Reed, K; Naylor, PJ; Liu-Ambrose, T; Mckay, H. School-Based Physical Activity Does not Compromise Children’s Academic Performance. Med. Sci. Sports. Exerc 2007, 39, 371–376. [Google Scholar]
- Boot, CRL; Vonk, P; Meijman, FJ. Health-Related Profiles of Study Delay in University Students in the Netherlands. Int. J. Adolesc. Med. Health 2007, 19, 413–423. [Google Scholar]
- Raudsepp, L; Viira, R. Sociocultural Correlates of Physical Activity in Adolescents. Pediatr. Exerc. Sci 2000, 12, 51–60. [Google Scholar]
- Shephard, RJ. Habitual Physical Activity and Academic Performance. Nutr. Rev 1996, 54, 32–36. [Google Scholar]
- Daley, AJ; Ryan, J. Academic Performance and Participation in Physical Activity by Secondary School Adolescents. Percept. Mot. Skills 2000, 91, 531–534. [Google Scholar]
- Tremblay, MS; Inman, JW; Willms, JD. The Relationship between Physical Activity, Self-Esteem, and Academic Achievement in 12-Year-Old Children. Pediatr. Exerci. Sci 2000, 1, 312–323. [Google Scholar]
- Maurage, P; Pesenti, M; Philippot, P; Joassin, F; Campanella, S. Latent Deleterious Effects of Binge Drinking over a Short Period of Time Revealed only by Electrophysiological Measures. J. Psychiatry Neurosci 2009, 34, 111–118. [Google Scholar]
- Martinez, JA; Sher, KJ; Wood, PK. Is Heavy Drinking Really Associated with Attrition from College? The Alcohol-Attrition Paradox. Psychol. Addict. Behav 2008, 22, 450–456. [Google Scholar]
- American College Health Association. American College Health Association National College Health Assessment (ACHA-NCHA): Spring 2005 Reference Group Report (abridged). J. Am. College Health 2006, 55, 5–16. [Google Scholar]
- Wood, P; Sher, K; Bartholow, B. Alcohol Use Disorders and Cognitive Abilities in Young Adulthood: a Prospective Study. J. Consult. Clin. Psychol 2002, 70, 897–907. [Google Scholar]
- Snell, P. Live Issues: Libraries Brought to Book. Nurs. Times 1992, 88, 26–28. [Google Scholar]
- Forth, E. Desperate Measures. Nurs. Stand 1996, 10, 53. [Google Scholar]
- Ford, J; Bosworth, D; Wilson, R. Part-Time Work and Full-Time Higher Education. Stud. Higher Educ 1995, 20, 187–202. [Google Scholar]
- El Ansari, W. Student Nurse Satisfaction Levels with their Courses: Part II—Effects of Academic Variables. Nurse Educ. Today 2002, 22, 171–80. [Google Scholar]
- Lee, RL; Loke, AJ. Health-Promoting Behaviors and Psychosocial Well-Being of University Students in Hong Kong. Public Health Nurs 2005, 22, 209–220. [Google Scholar]
- Richards, A; Kattelmann, KK; Ren, C. Motivating 18- to 24-Year-Olds to Increase their Fruit and Vegetable Consumption. J. Am. Diet Assoc 2006, 106, 1405–1411. [Google Scholar]
- Hsieh, PL. Factors Influencing Student’s Decisions to Choose Healthy or Unhealthy Snacks at the University of Newcastle, Australia. J. Nurs. Res 2004, 12, 83–90. [Google Scholar]
- Ding, W; Lehrer, SF; Rosenquist, JN; Audrain-McGovern, J. The Impact of Poor Health on Academic Performance: New Evidence Using Genetic Markers. J. Health Econ 2009, 28, 578–597. [Google Scholar]

{kind=link}
| Variable | Whole sample (N = 380) | Male (N = 195) | Female (N = 185) | p value |
|---|---|---|---|---|
| Satisfaction Questionnaire | ||||
| Educational Satisfaction‡ | 2.19 (0.72) | 2.27 (0.75) | 2.17 (0.74) | NS |
| Health & Wellbeing Questionnaire | ||||
| 1. Socio-demographic Variables | ||||
| Age in years: Mean (SD) | 22.86 (7.5) | 21.22 (4.7) | 24.58 (9.4) | <0.001 |
| Financial: Income Sufficiency | NS | |||
| Always sufficient | 9.6 | 10.5 | 8.6 | |
| Mostly sufficient | 52.9 | 55.5 | 50.0 | |
| Mostly insufficient | 25.8 | 23.0 | 28.7 | |
| Always insufficient | 11.8 | 11.0 | 12.6 | |
| 2. Health & Wellbeing Variables | ||||
| Alcohol Consumption: Had five or more drinks in a row last month | <0.001 | |||
| None | 20.4 | 13.0 | 28.2 | |
| 1 time | 12.9 | 8.9 | 17.1 | |
| 2 times | 12.9 | 14.1 | 11.6 | |
| 3−5 times | 26,5 | 27.1 | 26.0 | |
| 6−9 times | 15.8 | 19.8 | 11.6 | |
| 10 or more times | 11.5 | 17.2 | 5.5 | |
| Health Complaints: Sleep disorder/ Insomnia during the last 12 months | NS | |||
| Never | 52.4 | 58.5 | 45.9 | |
| Rarely | 25.3 | 22.6 | 28.1 | |
| Sometimes | 16.6 | 14.4 | 18.9 | |
| Very often | 5.8 | 4.6 | 7.0 | |
| General Health | 0.002 | |||
| Excellent | 10.3 | 14.4 | 5.9 | |
| Very good | 39.5 | 43.6 | 35.1 | |
| Good | 44.5 | 39.0 | 50.3 | |
| Fair | 4.7 | 2.1 | 7.6 | |
| Poor | 1.1 | 1.0 | 1.1 | |
| Health Awareness: Extent of keeping an eye on one’s health | 0.012 | |||
| Not at all | 0.8 | 1.0 | 0.5 | |
| Not much | 10.3 | 13.8 | 6.6 | |
| To some extent | 61.4 | 53.8 | 69.4 | |
| Very much | 27.5 | 31.3 | 23.5 | |
| 3. Educational Outcome Variables | ||||
| Importance of having good grades at University | NS | |||
| Very important | 64.1 | 61.7 | 66.7 | |
| Somewhat important | 34.3 | 36.3 | 32.2 | |
| Not very important | 1.3 | 1.6 | 1.1 | |
| Not at all important | 0.3 | 0.5 | 0.0 | |
| Rating of one’s academic performance in comparison with fellow students | NS | |||
| Much better | 2.1 | 3.1 | 1.1 | |
| Better | 21.3 | 22.3 | 20.2 | |
| The same | 62.5 | 62.2 | 62.8 | |
| Worse | 13.8 | 12.4 | 15.3 | |
| Much worse | 0.3 | 0 | 0.5 | |
| University Computerised Student Records | ||||
| Module Mark- actual achieved % grade: Mean (SD) | 54.56 (12.9) | 53.90 (12.1) | 55.68 (12.4) | NS |
| Variable | Importance (of good grades) | Performance (relative to peers) | Module Mark (Actual achieved grade) | |||
|---|---|---|---|---|---|---|
| Standardized β | p Value | Standardized β | p Value | Standardized β | p Value | |
| Higher educational satisfaction (Factor 1)‡ | −0.096 | NS | 0.079 | NS | −0.055 | NS |
| Older age | −0.234 | <0.001 | 0.022 | NS | 0.204 | <0.001 |
| Higher level of income sufficiency | −0.179 | <0.001 | 0.139 | 0.009 | 0.095 | NS |
| Higher frequency of five or more drinks in a row | −0.500 | 0.004 | −0.009 | NS | −0.034 | NS |
| Higher frequency of sleep disorder/ insomnia | −0.008 | NS | −0.003 | NS | −0.109 | NS |
| Higher level of general Health | −0.012 | NS | 0.204 | <0.001 | −0.037 | NS |
| Higher extent of keeping an eye on one’s health | 0.150 | 0.004 | 0.038 | NS | 0.063 | NS |
| Higher importance of having good grades | — | — | 0.289 | <0.001 | 0.129 | 0.033 |
| Higher rating of own academic performance | 0.278 | <0.001 | — | — | 0.114 | NS |
| Higher achieved module mark | 0.112 | 0.033 | 0.103 | NS | — | — |
| Adjusted R2 of the model | 0.21 | 0.18 | 0.09 | |||
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
El Ansari, W.; Stock, C. Is the Health and Wellbeing of University Students Associated with their Academic Performance? Cross Sectional Findings from the United Kingdom. Int. J. Environ. Res. Public Health 2010, 7, 509-527. https://doi.org/10.3390/ijerph7020509
El Ansari W, Stock C. Is the Health and Wellbeing of University Students Associated with their Academic Performance? Cross Sectional Findings from the United Kingdom. International Journal of Environmental Research and Public Health. 2010; 7(2):509-527. https://doi.org/10.3390/ijerph7020509
Chicago/Turabian StyleEl Ansari, Walid, and Christiane Stock. 2010. "Is the Health and Wellbeing of University Students Associated with their Academic Performance? Cross Sectional Findings from the United Kingdom" International Journal of Environmental Research and Public Health 7, no. 2: 509-527. https://doi.org/10.3390/ijerph7020509