2.1. CAALYX: Complete Ambient Assisted Living Experiment
CAALYX (01/2007-12/2008 -
http://caalyx.eu/) is a two-year eHealth project funded by the European Commission under FP6 (Sixth Framework Programme) [
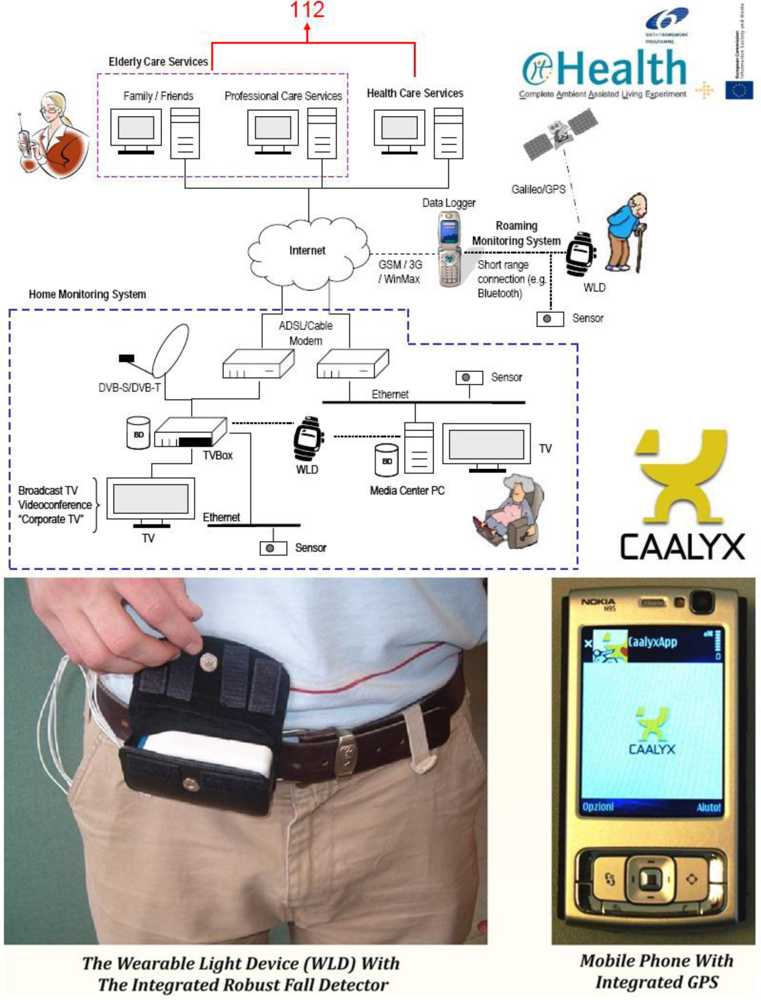
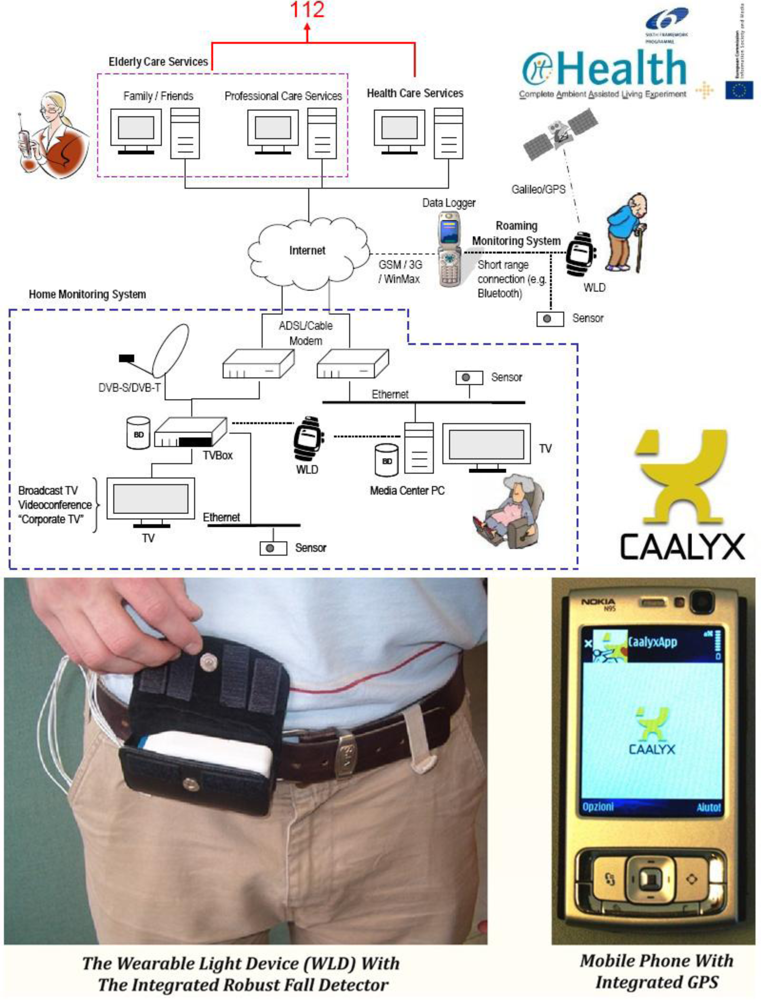
8]. It integrates the efforts of eight research, telecomm/industrial and end-user partners from six European countries, with the common goal of monitoring the health status of elderly users 24 hours a day, seven days a week, for the purpose of predicting/detecting any unfolding adverse health conditions and preventing complications before they develop, all while respecting users’ privacy and personal life needs. In the unfortunate event that an adverse condition arises, the system relays a high priority message to an emergency service (e.g., 112), including the geographic position and clinical condition of the elder user. In order to achieve these objectives as unobtrusively as possible, the service is composed of three distinct subsystems (
Figure 1):
- The Mobile (Roaming) Monitoring Subsystem:
- Collects and monitors key vital signs and detects adverse health events and falls when users are outdoors;
- Facilitates efficient communications between the user and his/her caretakers and family in the event of an emergency when the elder person is away from the home environment.
- The Home Monitoring Subsystem:
- Monitors users while at home and also helps keep them in touch with their family and caretakers;
- Delivers classic services (television, videophone) and features rich Internet communications.
- The Caretaker’s Monitoring Subsystem (Elderly Care Services):
While at home, a series of smart sensors (some of them, e.g., body temperature and ECG sensors, are worn on the body as a BAN, and others, e.g., weighing scale, are not) connect wirelessly via Bluetooth to a media-centre Personal Computer (PC), which records and analyses user parameters such as body weight, body temperature, blood pressure, cardiac function, etc. An ‘always-on’ connection to the Internet keeps the user within reach of their caretakers and family.
When the user is outdoors (for example, shopping in the city), he/she remains watched over and connected by carrying, in addition to his/her GPS-enabled mobile phone, a Wearable Light Device (WLD) that continues recording and analysing key vital parameters (body temperature, electrocardiogram, respiratory rate, etc.), and is also equipped with a reliable Fall Sensor (a tri-axial accelerometer) and a Panic Button. In essence, the WLD complements the functionality provided by the user’s mobile phone, acting as an active Bluetooth-enabled ‘sensor peripheral’ for it, and providing specialised hardware that is normally not available in a common mobile phone.
In order to respect the privacy of elder users, all the data processing required to evaluate their health condition is taking place locally, either on the Home or the Roaming Monitoring Subsystems, and only the outcome of this intelligent processing is shared with external entities, such as the carers, when this is necessary, e.g., during an emergency or if a fall is detected.
This approach, of sending selected data only when needed rather than streaming all data continuously, not only preserves the elder’s privacy, but also helps prolonging the Mobile Subsystem’s battery life and making best use of its Internet bandwidth.
Caretakers and other trusted entities with suitable access rights can request data and other information through the Caretaker’s Monitoring Subsystem. Because of the nature of the monitoring service, it should be possible in a future iteration of the system for the Caretaker’s Monitoring Subsystem to have access to a patient’s Health Record data over a standardised connection with the national health and social care infrastructure/databases where these are available.
The monitoring solution proposed by CAALYX is amongst a currently small number of solutions that are able to monitor the well-being of individuals both at home and while they are mobile. Wireless communications have played an important role in making the system usable and most importantly portable. Bluetooth is used extensively for the communications between the sensors that compose a Wireless BAN, which means that the system looks more like a set of wearable items rather than a bulky and heavy wire harness that would put-off potential users. The connection maintained through the user’s mobile phone and the GSM network, along with the high speed Internet connection of the Home Monitoring Subsystem, ensure that the patient is always within reach in case of an emergency. In this case wireless technologies have enabled a shift in the patient-doctor relationship, minimising the need for routine visits without losing touch, and also contributing to the autonomy and confidence of the users, which is an important psychological factor for the elderly.
2.2. eCAALYX: Enhanced Complete Ambient Assisted Living Experiment
eCAALYX (06/2009-05/2012 –
http://ecaalyx.org/) is a three-year project funded by the European Commission under the Ambient Assisted Living (AAL) Joint Programme (
http://www.aal-europe.eu/). The project builds on the strengths of the infrastructure and functionality already developed in the CAALYX project (see above), and in fact, six of the participants in new eCAALYX project (Telefónica Investigación y Desarrollo, Spain; INESC Porto – Instituto de Engenharia de Sistemas e Computadores do Porto, Portugal; University of Plymouth [Enterprise Ltd], UK; University of Limerick, Ireland; Corscience GmbH & Co KG, Germany; and Fundació Hospital Comarcal Sant Antoni Abat, Spain) were members of the previous CAALYX project consortium, with four new participants joining them in eCAALYX (Fraunhofer Portugal; CETEMMSA Technological Centre, Spain [project coordinator]; Ev. Krankenhaus Witten GmbH, Germany; and TeleMedic Systems, UK).
eCAALYX’s objectives can be summarized as follows:
- Health monitoring of older and elderly persons with multiple chronic conditions, at home and on the move (the original CAALYX did not cover the health monitoring and management of older people with comorbidity).
- Improve the quality of life of elderly persons by increasing their freedom and safety.
- Prevent deterioration of the patient condition by providing continuous support, guidance, and relevant health education.
- Achieve all of the above goals by providing a solution that is commercially viable, acceptable by all users/stakeholders, reliable, long-term, flexible, scalable, and virtually maintenance-free in non-technical environments, thus suitable for real-world deployment.
Chronic cardio-respiratory diseases are a major cause of death and admission to hospital among elderly people in Europe and are often concurrent with a number of other chronic health conditions. During the course of such diseases, repeated decompensation episodes typically occur, leading to frequent and costly hospitalisation of patients.
eCAALYX provides a complete solution to improve the quality of life of elderly patients in such a situation, by monitoring their health condition, assessing their health risk, promptly detecting and controlling any decompensation episodes, and offering them focused education on leading a healthy lifestyle, so that their independent life at home can be extended and their hospitalisation or admission in nursing homes avoided for longer periods. This ‘(self-)management and prevention’ approach is based on a ‘health agenda’ concept that is available at home and also when the aged person visits alternative homes during holidays or when visiting relatives, even in other European countries.
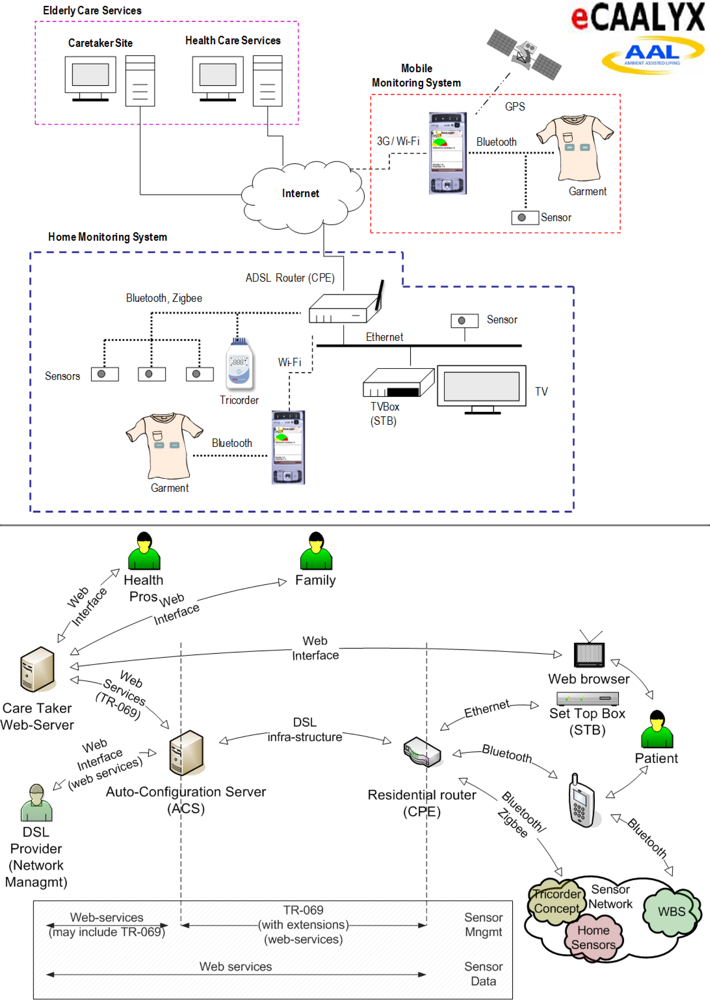
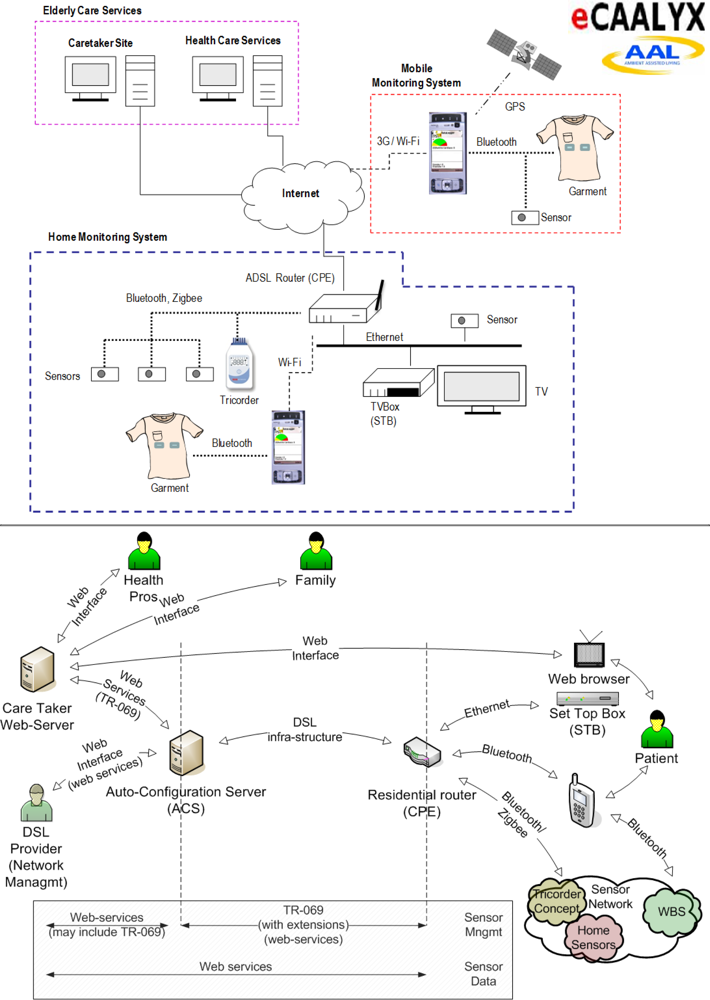
eCAALYX is composed of three main subsystems (
Figure 2):
- The Home Subsystem, which includes Customer Premises Equipment (CPE), Set-top-box (STB)/interactive TV (to deliver health education and other functions), Tricorder and home sensors (those sensors that are stationary and not continuously worn on the body), all of them located at home;
- The Mobile Subsystem, which includes a “smart” garment, with all sensors integrated into a wireless BAN—Wearable Body Sensors (WBS), and a mobile phone;
- The Caretaker Site, which includes the Caretaker Server and the Auto-configuration Server.
The key features and main components of the three subsystems are described below.
eCAALYX will apply and extend standard network management standards, e.g., DSL Forum TR-069 (
http://www.broadband-forum.org/), used by telecommunication service providers, to eHealth systems. Such interfaces and communications mechanisms can be used to remotely manage eHealth equipment, helping reduce operating costs, improve reliability and enhance user satisfaction. Integration of eHealth functionalities in standard (and low-cost) home networking equipment, namely DSL (Digital Subscriber Line) residential routers and set-top-boxes will reduce the equipment investment required.
The Tricorder device will combine the most relevant sensors for monitoring the prevalent chronic conditions and health risks in elderly people, such as hypertension, stroke, respiratory diseases and congestive heart failure. Thus sensors for the measurement of heart rate, ECG and pulse oximetry/SPO2 (Saturation of Peripheral Oxygen) will be included. By applying suitable processing and analysis algorithms to captured vital parameters, possible risk factors such as atrial fibrillation (an important risk factor for stroke), rise of blood pressure, progression of chronic obstructive pulmonary disease (COPD) can be detected. Inspiration effort/respiratory rate can be determined out of ECG measurements, and specifically out of the ‘pulse transit time’.
The basic sensor system of the Tricorder will be scalable; thus, interfaces for integration of additional sensors will be provided. Moreover, a Bluetooth interface will facilitate the linking of further Bluetooth-enabled medical devices such as weighing scales, blood pressure meters or glucose meters.
Algorithms and improved sensors/accelerometers will also be developed and evaluated for Activities of Daily Living (ADL) event detection (for falling, walking, climbing stairs, sitting, etc.), with improved sensitivity, specificity and power consumption, and these events (with alert status) will be forwarded optimally to the Home and Caretaker Subsystems.
This ADL/patient mobility component of eCAALYX will include algorithm development for gait variability measurement and for transmission of gait variability measures for data mining of fall risk. Based on the identified importance of energy expenditure for mobility qualified physiological signs, more accurate energy expenditure measurements derived from ECG, skin temperature, GSR (Galvanic Skin Resistance) and accelerometer signals will also be explored.
The integration of GPS (including the European Galileo Satellite Positioning System, when it becomes available) will allow detailed patterns of mobility to be determined, which can be used to further qualify measurements, and will be used to determine, in conjunction with data mining techniques, if any deterioration in mobility is occurring.
Using conductive textile materials, a comfortable garment will be developed for improved usability, user acceptance and performance. It will have conductive areas which will be used as heart rate/ECG electrodes when in contact with the skin. Conductive fabrics allow electrodes to be smooth to the touch and comfortable. Moreover, using conductive fabrics for data transmission between the non-wireless parts of a BAN is a major improvement in a wearable system, replacing bulky electric wires by conductive textile ribbons. Solutions will be selected according to comfort requirements such as garment flexibility, elasticity and washability.
A standard GPS enabled smart phone (3G/UMTS—Universal Mobile Telecommunications System) running a completely autonomous software application, requiring no user interaction, will manage the personalised BAN, which comprises the garment and other user specific sensors, and continuously analyse sensor data in order to identify problem situations and alert health professionals. This software application will be a refinement of the one developed for the CAALYX project, the development this time being focused on areas such as reliability, network management (3G/Wi-Fi switching), improving remote and automatic configuration and management, and reducing mobile phone battery consumption.
A distributed, adaptable and scalable monitoring infrastructure will be implemented to allow for the continuous acquisition of the users’ sensors data and to provide these data in a meaningful and controlled way to the client applications on the Caretaker Server, the Home Subsystem and the Mobile Subsystem. This infrastructure will allow for the health professionals to easily configure software/virtual sensors for each user (‘observation patterns’ or schedules), using the set of available real and pre-existing virtual sensors, i.e., the user’s BAN, other sensors at home, the Mobile Subsystem (geo-positioning), relevant user data/history stored on the Caretaker Server and, eventually, data from the person’s national/central health and medical records.
Coordinating teams of healthcare professionals can be a major issue when dealing with patients with comorbidity, whose conditions require the expertise of, and input from, multiple specialists. The Caretaker Server will address this issue by providing appropriate means for coordination, e.g., an electronic health record and personalised forums for each patient, as well as direct and easy modes of communication between health professionals such as video-conferencing.
Besides enabling reactive actions in response to acute event alerts, the Caretaker Site will proactively use data mining techniques to correlate data from sensors, assess risk levels and help switching any corresponding ‘preventive actions’ in the ‘health agenda’ in a timely manner. Pattern detection via data mining of readings from multiple sensors (i.e., looking for normal and abnormal patterns, plus changes and trends over time) and the provision of effective reporting mechanisms to the caretaker will be implemented.
Contextualisation of body sensor data using ambient sensors in the home (RFID—Radio-Frequency Identification and PIR—Passive Infrared Sensors) will enhance the home mobility data of monitored patients by facilitating the linkage of these data to the person’s daily activities in the home. Data from GPS and weather stations will enhance the mobility data of the monitored patients outdoors. Factors such as when, where and to what extent the person is sitting, lying or walking will be examined, since these factors could be significant in assessing the health status of the patient.
Communications security and elder’s privacy are ensured by using standards recommended by HL7 (Health Level 7 -
http://www.hl7.org/) and including ‘audit trailing’ capabilities to log ‘who has done what and when’. Standards developed under the Service Oriented Architecture (SOA) architecture will be applied. It should also be possible to make all relevant components of eCAALYX compliant with Continua Health Alliance (
http://www.continuaalliance.org/) recommendations, which are based on ISO/IEEE 11073 and Bluetooth standards.
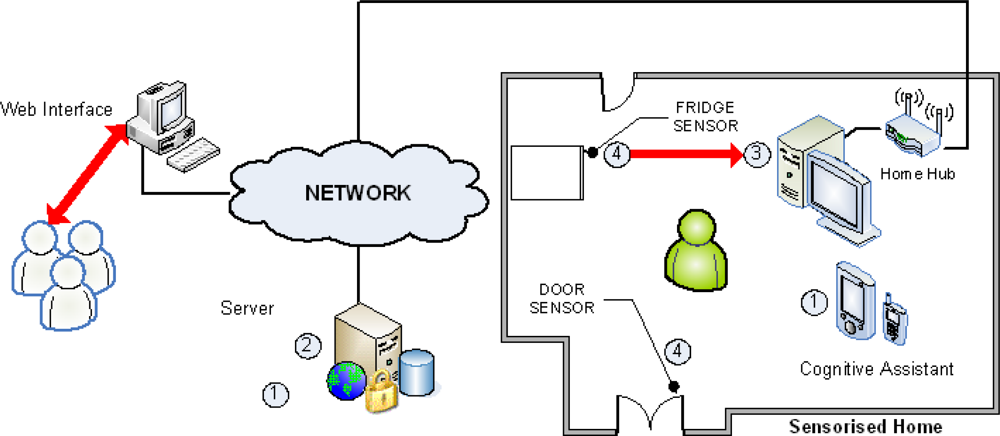
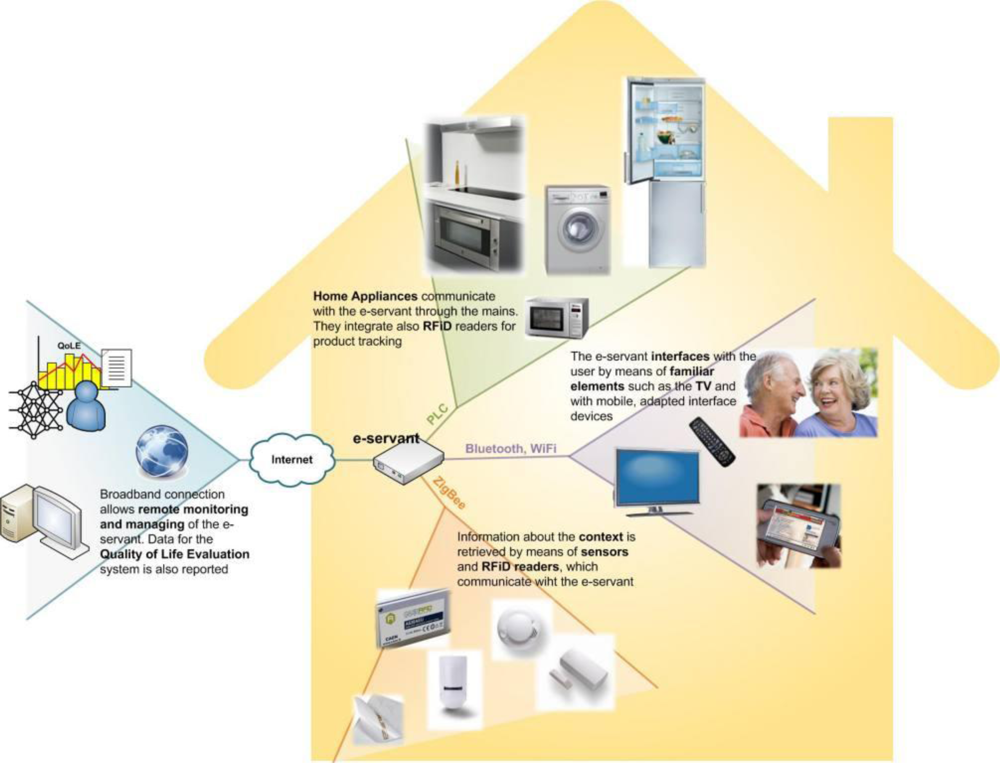
2.4. EasyLine+: Low Cost Advanced White Goods for a Longer Independent Life of Elderly People
EasyLine+ (01/2007-06/2009 -
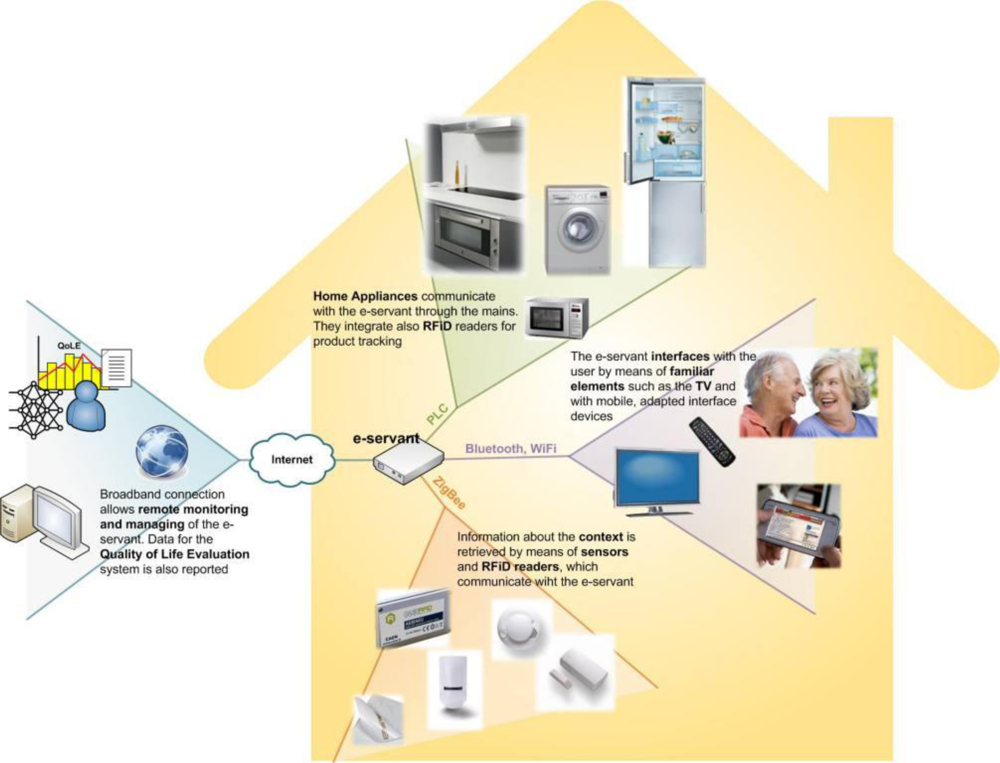
http://www.easylineplus.com/) is a two-and-half-year project funded by the European Commission under the FP6 eInclusion programme. Six partners from three European countries have developed prototypes suitable for the market of advanced white goods to support elderly people with or without disabilities in carrying out a longer independent life at home, and to compensate for any loss of physical and/or cognitive abilities they might have in the kitchen. This is achieved by bringing ambient intelligence to the kitchen environment. The project’s architecture is shown in
Figure 4.
Within the modern kitchen environment, white goods are perhaps the most important elements, whether they are “intelligent” or not. To achieve EasyLine+’s goals, new ambient “intelligence” and interfaces have to be introduced across the whole system, but this does not necessarily imply that existing white goods have to be made “smarter” or to incorporate new adapted interfaces. Such radical modifications would only increase their unit price, make their installation harder (as adapting their functioning to a user’s particular case would require custom configuration), and consequently hinder their market penetration.
Instead of relying on new “smart” appliances with accessible interfaces, EasyLine+ features a ‘central intelligence system’ that is aware of the status of all white goods in the kitchen, able to control them, and also able to interact with the user. This essentially means giving home appliances the capacity to communicate.
Besides the developments related to white goods, EasyLine+ introduces diverse sensors that are usually used for context awareness tasks. Some sensors are already used inside today’s kitchens (temperature, fire, smoke, and flooding), while others are not yet common (presence, door opening, etc.). The project team have also considered using RFID readers to identify clothes and food. The use of RFID and EPC (Electronic Product Code -
http://www.epcglobalinc.org/) can provide useful information about what is in the washing machine or fridge, what does the user want to eat or have just bought, etc. Food information can be used to inform the elderly person about any food ingredient that is missing, which food is nearing or has reached its expiry date, which meal the user may prepare and eat, etc. Cloth information can be helpful in determining which washing programme is best suited for clothes introduced in the washing machine.
A Human-Machine Interface (HMI) is managing user interaction and is of key importance to the system. HMI devices should be easy to use and suit any kind of user, with the ability to change the interface according to various user profiles. They do not necessarily require powerful processing capabilities or a high data storage capacity, but should have a standard communications interface. There are many different types of mobile clients that can be used to interact with the system such as PDAs, smart phones, ultra-mobile PCs and others. This means that the user can carry them around the house and be able to monitor the house appliances wherever he or she might be. Fixed devices such as desktop computers, digital TVs or devices in the form of embedded ‘control panels’ in the actual appliances can also be used as control interfaces.
The system as a whole is called e-servant and is aware of its environment and users. The “intelligence” of white goods is enhanced by offering new functions that facilitate their use. The system adapts to any disabilities or preferences the user might have by analysing all the data it gathers and extracting relevant information that can be used to adapt the system to suit the needs of its user. In the case of an emergency, the system can send a warning message to a remote care centre.
E-servant is also the ‘coordinator’ with which all the other system components communicate. In order for the system’s operation to be transparent to the user, the different building blocks communicate with each other using various modes of communication:
- Power Line Communication (PLC) over the mains wires is used to get the status of appliances and to control them. PLC is the best option for white goods because they all have to be mains powered and there are already European standards being promoted in this respect. Moreover, no configuration is needed to install a new appliance.
- A ‘wireless sensor network’ supports all the sensors in the kitchen and also the acquisition RFID data from corresponding readers. This sensor network is operating over ZigBee (
http://www.zigbee.org/), as this is becoming the de-facto standard for home environments.
- Bluetooth and Wi-Fi are employed for the communications between the interfaces due to the widespread availability of these technologies in personal computers and mobile devices.
- Finally, communication with the “outside world”/the Internet (e.g., to send to social services or family information about the user’s quality of life, as well as alarms about possible technical problems or any appliance maintenance needed, etc.) is carried out using standard protocols such as DSL (Digital Subscriber Line) or Wi-Fi.
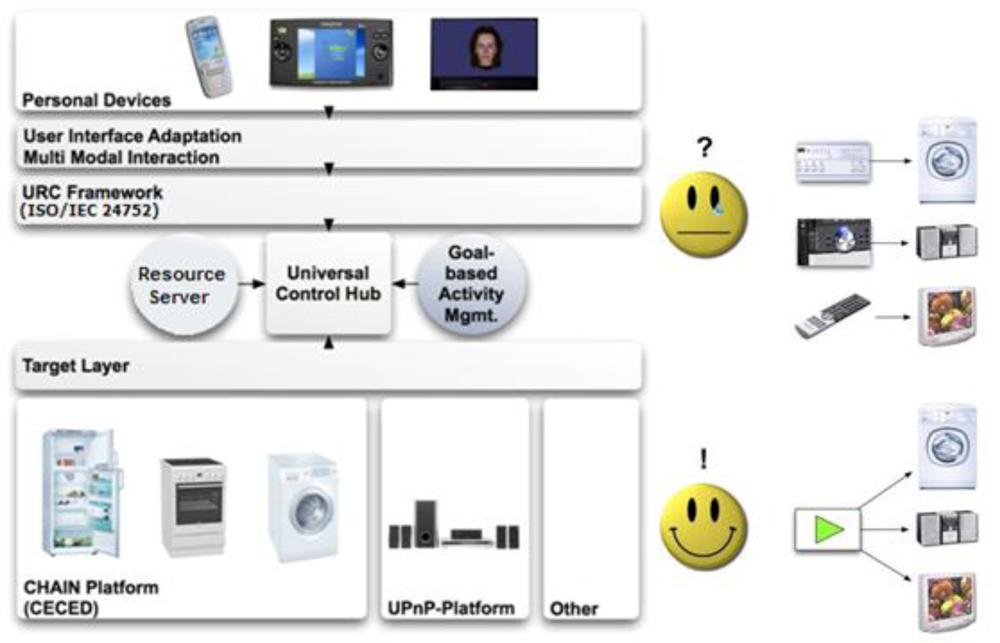
2.5. I2HOME: Intuitive Interaction for Everyone with Home Appliances based on Industry Standards
I2HOME (9/2006-8/2009 -
http://www.i2home.org/) is a three-year project funded by the European Commission under the FP6 eInclusion programme. The project consortium is composed of nine partners from five European countries, with competences ranging from technology development to accessibility expertise and experience with persons with special needs. The project builds on two main pillars:
Current research and technology provide the necessary building blocks for realising “smart” home environments, heralding an era of new interaction paradigms for persons with special needs. However, most of this technology is either proprietary or incompatible with some existing components. Moreover, current user interfaces are targeting advanced users by offering them to go in detail through every feature of the service or appliance. This can quickly become overwhelming, not only for persons with cognitive disorders but even for ordinary users wanting to complete a quick task. At the same time, knowledge on how to design accessible user interfaces is expanding but the corresponding technologies are not adequately marketed and implemented in practice. There is clearly a need for an open universal platform for connecting interaction devices with appliances and for services that provide more flexible user interfaces.
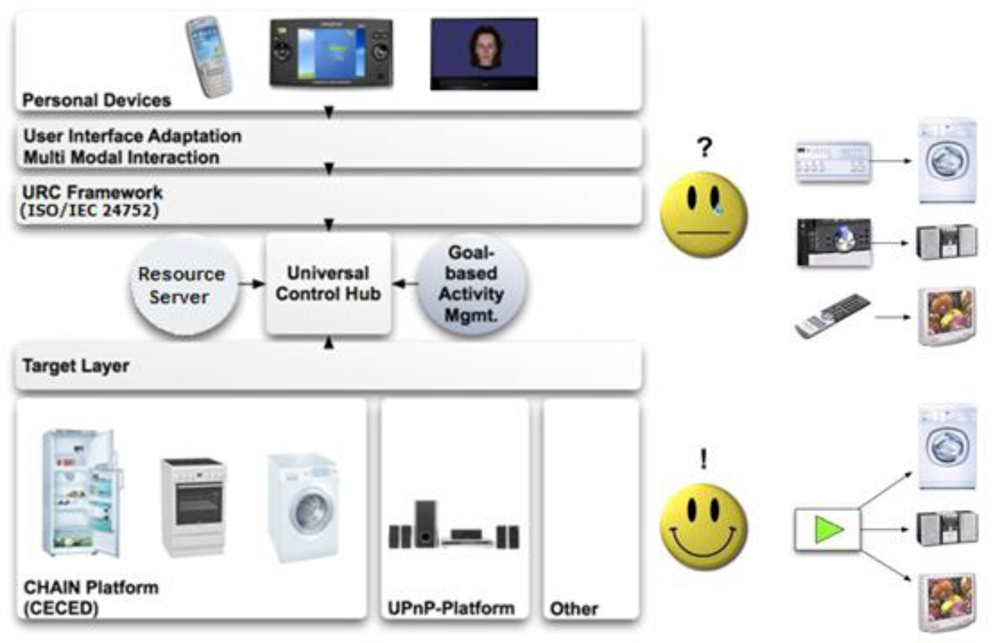
These requirements are met by the ISO/IEC 24752 URC standard depicted in
Figure 5. The architecture includes a hub for connecting various appliances and services with exchangeable, pluggable user interfaces, as well as Resource Servers that enable the sharing of various resources, such as target adaptors or remote user interfaces. The ability to switch user interfaces and the presence of Resource Servers are highly innovative concepts and present a major advantage over other approaches.
I2HOME followed a user-centred design methodology to develop four distinct user interface prototypes for the cognitively disabled, Alzheimer’s patients, the elderly, and sensory impaired patients. The main functionality of these user interfaces enables the interaction with main stream technology such as Siemens Serve@Home platform (
http://www.se-presse.com/download.php?pfad=downloads/en/19-1012-0501e.doc) and Google Calendar (
http://calendar.google.com/). Further work will focus on streaming technologies for the purpose of video conferencing. This is an important and necessary prerequisite to support a level of social networking functionality.
The project is an important step towards the creation of a European ecosystem for URC technology and is already in close collaboration with other projects of the European Commission eInclusion programme, acting as a technology supplier to them.
I2HOME has the potential to make the following contributions to eHealthcare through the innovative use of URC technology:
- Overcome the ‘one-size-fits-all’ limitations through pluggable user interfaces;
- Adapt and customise the services and associated user interfaces via shared resources;
- Develop next-generation user interfaces with simplicity and ease of use in mind through task-orientation and natural language interaction;
- Offer to other projects and manufacturers the ability to re-use the Universal Control Hub product for the development of a standards-based middleware architecture for the digital home of the future.
I2HOME’s ultimate goal is to provide a unified and accessible user interface to common home appliances and consumer electronics based on industry standards. This approach should make it much easier for people with cognitive disabilities and older persons to operate these devices, e.g., by using an intuitive interface running on an Apple iPhone, without having to learn and remember a different and complex operating interface for each appliance separately, thus helping these persons live independently at their own homes for longer periods of time. An online video demonstration of some aspects of the technology adopted in I2HOME is publicly available at
http://www.youtube.com/watch?v=wElYM_nb7gI.



 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}