4.1. Main results and Comparison with Other Studies
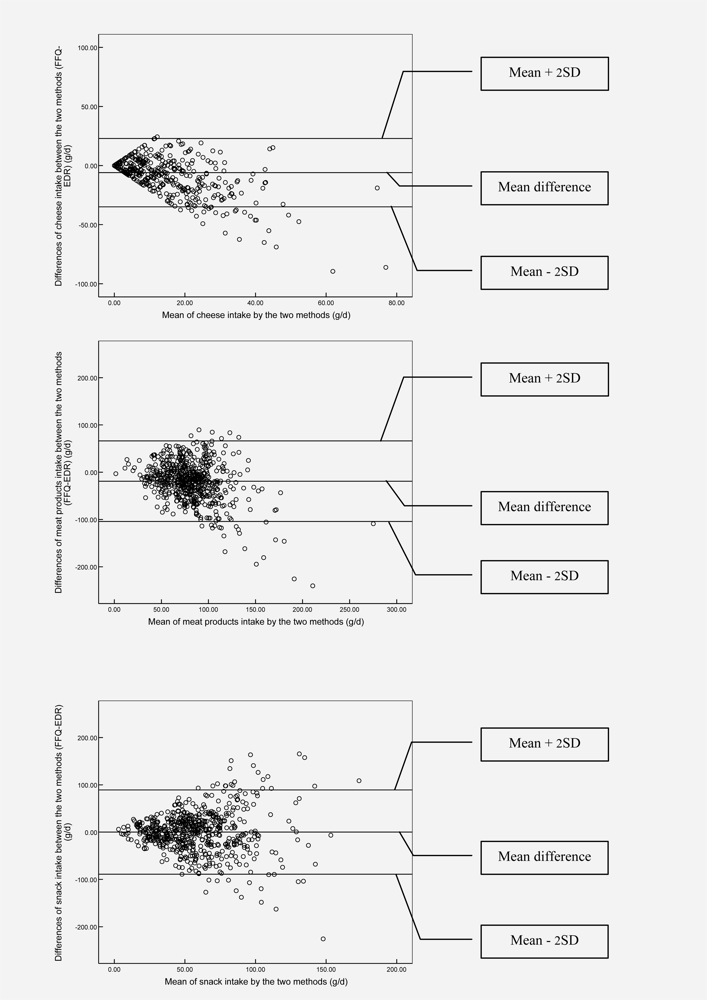
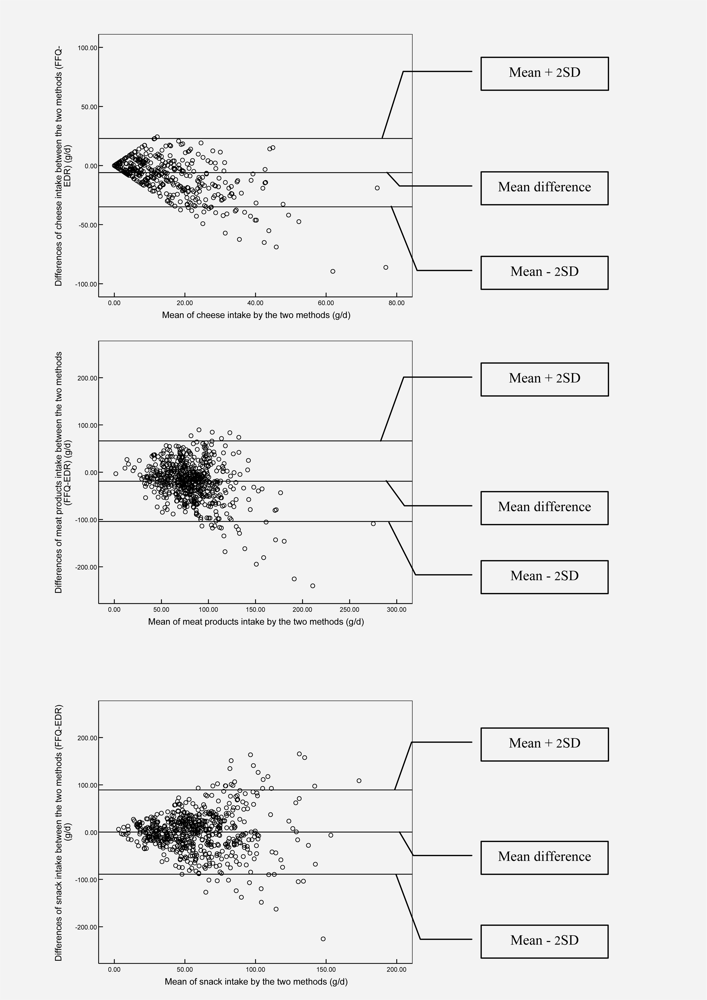
Although this study showed good reproducibility for almost all food groups, large differences in relative validity were found between the different food groups. The largest percentage of mean difference was found for cheese intake for which the mean intake calculated from the EDR was almost twice as large as the mean intake calculated from the FFQ. Though, despite those important differences in mean food group intakes derived from the two different methods, similar conclusions can be drawn from both methods when comparing the mean intakes with the food-based dietary guidelines (FBDG) (presented in
table 1). So, for measuring lacunas in the preschool dietary habits, both instruments could give a similar rough estimation of the major gaps.
However, from the misclassification analysis it was obvious that for different food groups this FFQ and EDR could not equally discriminate between quartiles. Also findings from the weighted κ statistic showed poor to moderate agreement for most of the food groups.
Corrected Spearman correlations between the FFQ and the 3d EDR showed values between 0.32 and 0.75. Other validation studies of intake of food groups and single food items assessed by FFQ have observed correlations, generally between 0.3 and 0.8 [
2,
13–
16].
Although the usefulness and validity of this FFQ for estimating an effect/change in dietary habits over time should be further investigated, from the good reliability (reproducibility) of the FFQ and the moderate to good correlations between the FFQ and the 3d EDR, it could be presumed that this FFQ might be a useful instrument for measuring effect/change in dietary habits among preschool children in future intervention studies.
4.2. Strengths and Weaknesses of the Study
The EDR was chosen as reference method because of its high level of accuracy when validated for assessing dietary intake in infants and children [
17]. Moreover, the measurement errors of the EDR and the FFQ are highly independent, since unlike the FFQ method the EDR does not depend on memory, is open-ended, and involves direct estimation of portion size [
16]. However, like any dietary assessment methodology, the EDR is prone to a degree of misreporting.
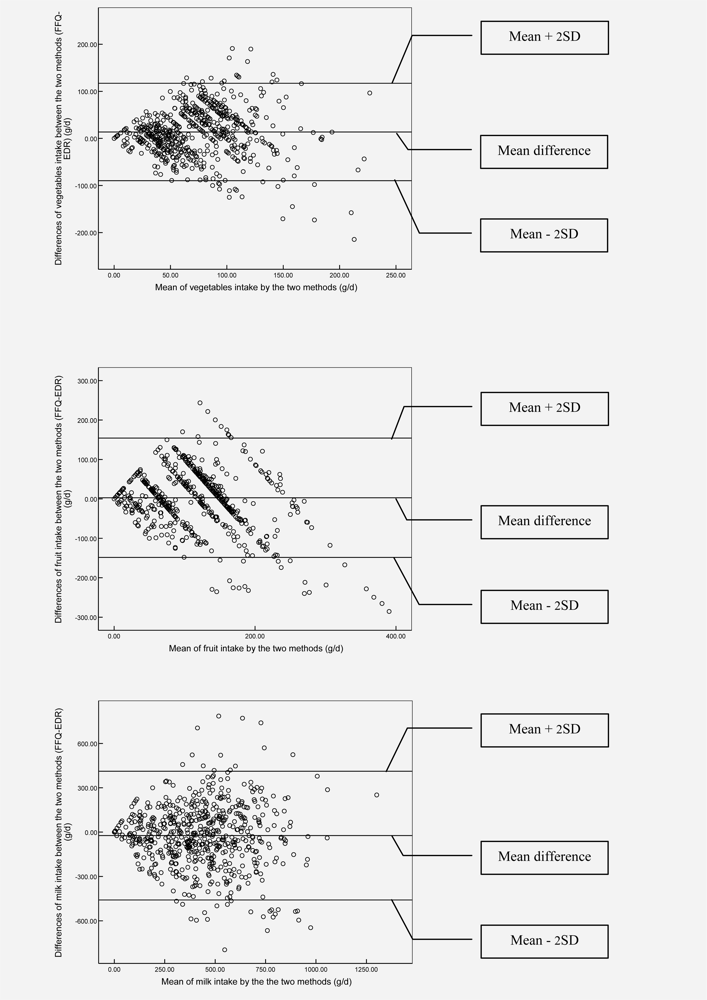
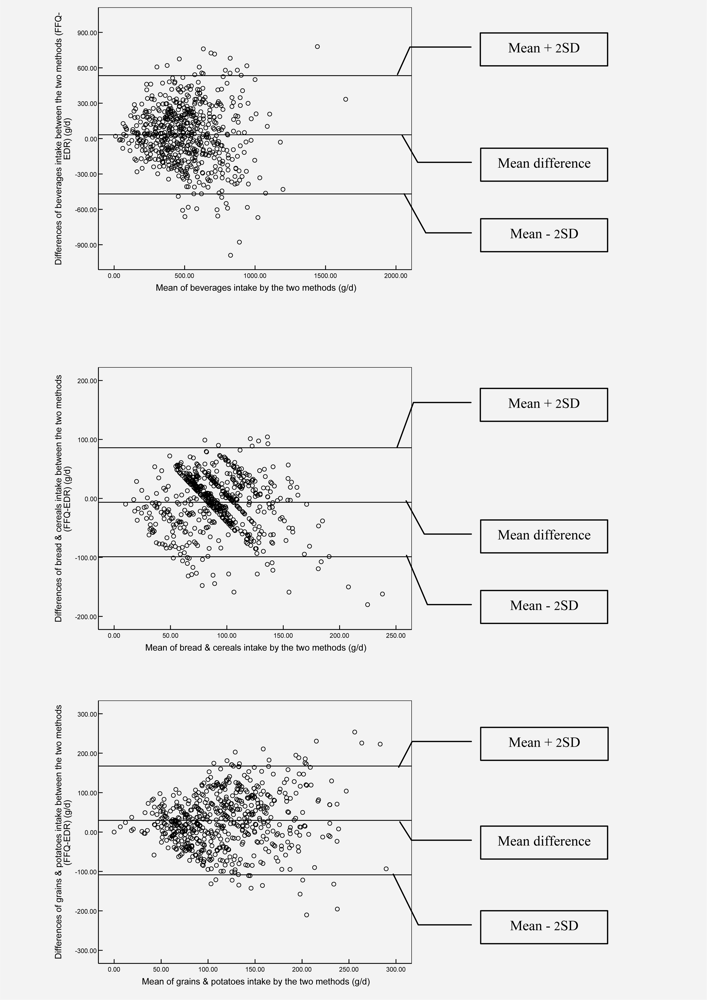
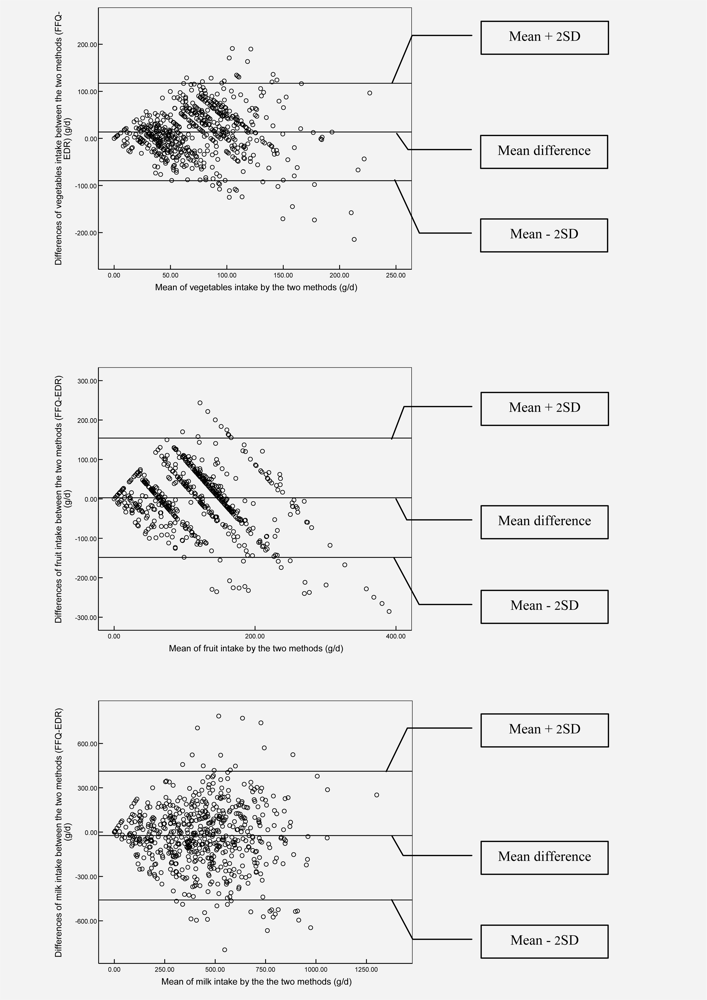
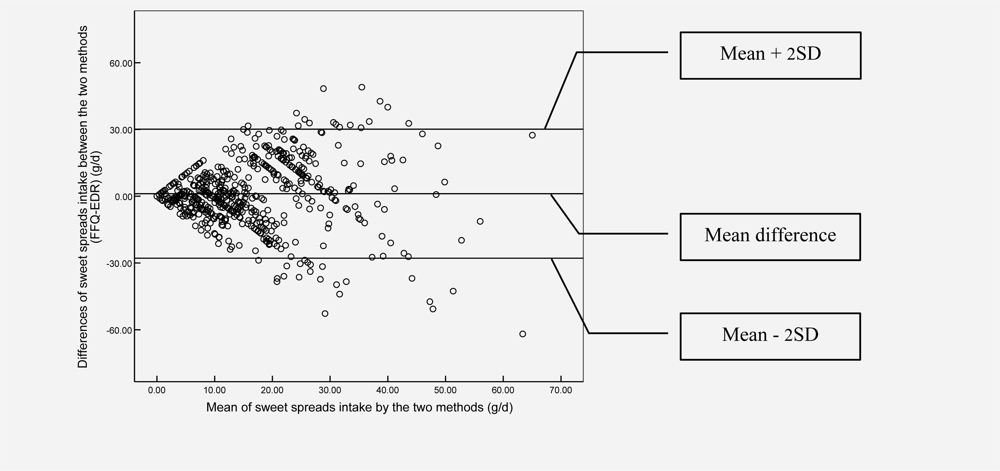
For instance, Day-to-day variability in preschoolers’ diets might be responsible for some larger differences between the results derived from the FFQ and the EDR. The low within- over between-individual variability ratio of milk products implies that most preschool children in Flanders are consuming milk products on a regularly (daily) basis. The high variance ratios for the other food groups however are due to the large day-to-day variability in food consumption. For the food groups showing high variance ratios, the reference (3d EDR) measurements may be biased and imperfectly reflect ranking. Therefore, Spearman correlations were corrected for attenuation, which improved the correlations for all food groups.
It is noteworthy that the low values for agreements between the FFQ and the 3d EDR might also be due to the important within-person variability for some of the food groups derived from the 3d EDR.
Even though many recording days (replicates) should give a better estimate of the habitual intake, the problems with long recording periods are declining accuracy of recording with increasing fatigue and boredom, and potential alterations to dietary habits [
18]. Because of those disadvantages of long recording periods and in the hope to minimize the refusal rate and/or drop-out within the study, it was decided to use 3d EDR in this validation study. However, a higher number of record days, spread over the whole year would have been more optimal as reference method, since this could take into account seasonal variation as well.
In addition, difficulties
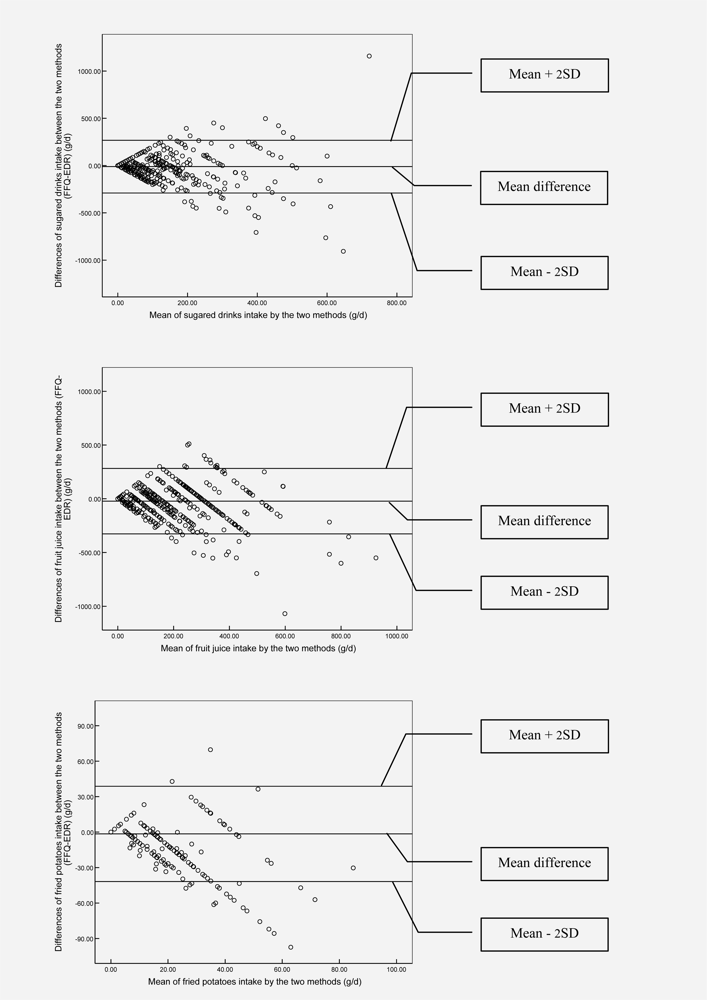
in portion size estimations during completion of the 3d EDR might also bias the true validity of the FFQ. For food groups, which are difficult to quantify in standard or household units in the EDRs (e.g. vegetables, meat, potatoes, rice, etc. which are often part of a mixed dish) the difference could be significant between the FFQ and the EDR results. In the 3-day EDR, for food groups like vegetables, meat products and potatoes, the dieticians coding the EDR had to assign standard portion sizes when the respondent was not able to quantify the consumed amount of food in grams (e.g. during school lunches). Since no standard portion sizes were available for children in Belgium, those from the general Belgian population had to be used instead [
19]. It should be noted that these standard portion sizes could have been too high for children and consequently have introduced non-negligible differences between the FFQ and EDR-results. In addition, a standard portion size, often had to be used for ‘a slice of cheese’ [
19]. However, the authors presume that the weight used for a slice of cheese, [
19] which was also borrowed from the manual of our general Belgian population might have been too high for preschool children, which could explain the higher cheese intake estimated from the EDRs.
As described in more depth previously [
8], like most surveys, our sample of preschool children included in the relative validity analyses was subject to some non-participation bias, in which higher social classes are likely to be over-represented.
A limitation of the reproducibility study could be a possible memory effect during completion of the second FFQ as parents could possibly still remember what they filled in five weeks ago.
Although differences in relative validity and reproducibility between different age categories might exist, the validity and reproducibility analyses were only performed on the total sample of preschool children (between 2.5 and 6.5 years old), as power would be too low for the reproducibility analyses if two different age groups were considered.
At last it should be noted that because of the lack of an external marker, no validity analyses could be performed for the reference method (3-d EDR) that was used in this validation study. Although biochemical measurements of nutrient and contaminant levels in blood or other body tissues/fluids can provide a useful assessment of the intake of certain nutrients or contaminants (especially for those that are measured poorly by other methods in children), it should be noted that children remain a special case with different limitations in the area of biochemical samples as well [
20,
21].
The major disadvantage to biomarkers collected via blood samples is the fact that the invasive nature of venipuncture puts some limits on researchers ability to obtain samples from children or to get high participation rates in large-scale studies. Also urine collections in young children for whom urine collection procedures require special consideration is not always easy. Appropriate sample collection apparatus, such as urine collection bags or toilet inserts, must be provided to collect urine samples from children who are not yet completely toilet trained (e.g. still wearing nappies at night) [
21]. Because of those constraints related to the use of biomarkers in childhood populations, no external markers have been used in the current study.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}