
COVID-19 Pandemic Fatigue and Its Sociodemographic, Mental Health Status, and Perceived Causes: A Cross-Sectional Study Nearing the Transition to an Endemic Phase in Malaysia
 , ,
, ,  and
and
Abstract
:1. Introduction
Research Questions
- What is the COVID-19 pandemic fatigue prevalence among Malaysians?
- What are the mental health status and perceived causes of pandemic fatigue in Malaysia?
- What is the association between sociodemographic, mental health, and perceived causes of pandemic fatigue with pandemic fatigue?
2. Materials and Methods
2.1. Study Design and Settings
2.2. Measurement of Sociodemographic Characteristics
2.3. Measurement of Pandemic Fatigue
2.4. Measurement of Mental Health
2.5. Measurement of Perceived Causes of Pandemic Fatigue
2.6. Statistical Analysis
3. Results
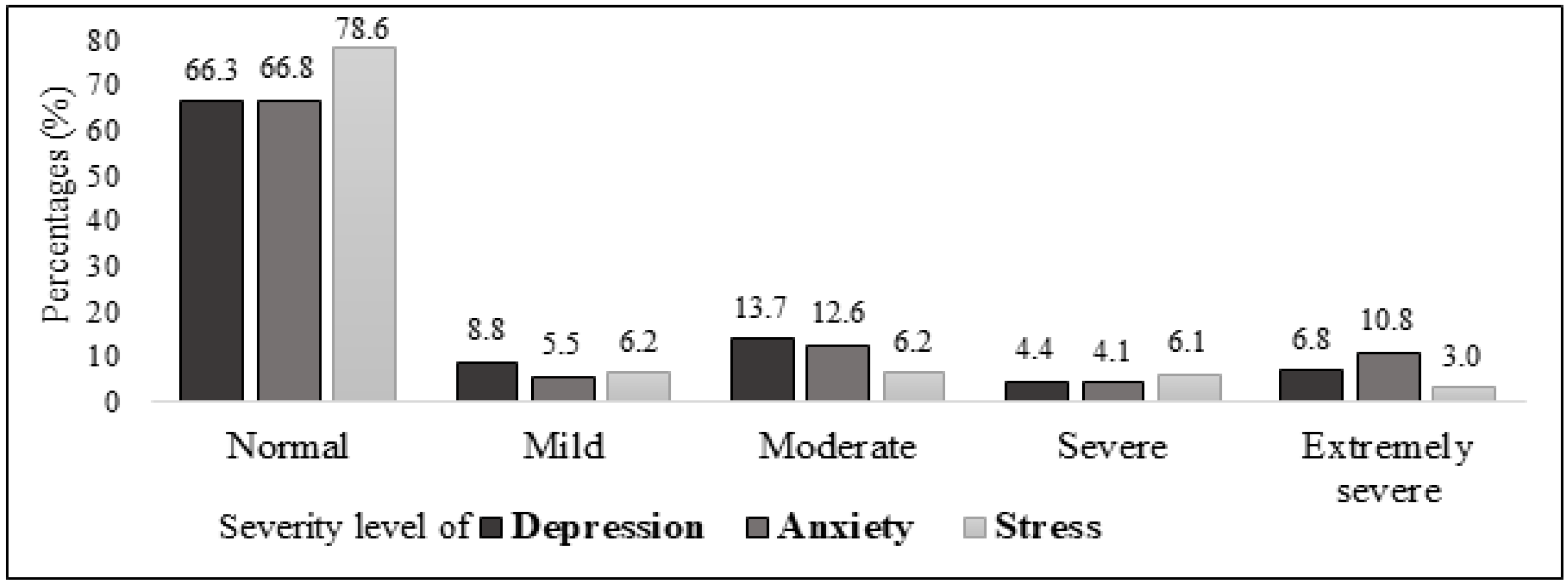
3.1. Description of Pandemic Fatigue, Mental Health Status, and Perceived Causes of Pandemic Fatigue
3.2. Association between Sociodemographic Characteristics and Pandemic Fatigue
3.3. Association between Mental Health and Pandemic Fatigue
3.4. Association between Perceived Causes of Pandemic Fatigue and Fatigue Category
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.W.; Wu, X.X.; Jiang, X.G.; Xu, K.J.; Ying, L.J.; Ma, C.L.; Li, S.B.; Wang, H.Y.; Zhang, S.; Gao, H.N.; et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: Retrospective case series. BMJ 2020, 368, m606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jee, Y. WHO International Health Regulations Emergency Committee for the COVID-19 outbreak. Epidemiol. Health 2020, 42, e2020013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Research Collaboration for Infectious Disease Preparedness. COVID 2019 PHEIC Global Research and Innovation Forum: Towards a Research Roadmap; World Health Organization: Geneva, Switzeland, 2020; Available online: https://www.who.int/publications/m/item/covid-19-public-health-emergency-of-international-concern-(pheic)-global-research-and-innovation-forum (accessed on 15 November 2022).
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 15 November 2022).
- WHO. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?adgroupsurvey={adgroupsurvey}&gclid=Cj0KCQiAg_KbBhDLARIsANx7wAz2vfleJym2JXoOXw2Wsxi-BByC053V_e-JV_Yi-jcb9ukdBKcdJQoaAq2kEALw_wcB (accessed on 15 November 2022).
- Aziz, N.A.; Othman, J.; Lugova, H.; Suleiman, A. Malaysia’s approach in handling COVID-19 onslaught: Report on the Movement Control Order (MCO) and targeted screening to reduce community infection rate and impact on public health and economy. J. Infect. Public Health 2020, 13, 1823–1829. [Google Scholar] [CrossRef]
- Brauner, J.M.; Mindermann, S.; Sharma, M.; Johnston, D.; Salvatier, J.; Gavenčiak, T.; Stephenson, A.B.; Leech, G.; Altman, G.; Mikulik, V.; et al. Inferring the effectiveness of government interventions against COVID-19. Science 2021, 371, eabd9338. [Google Scholar] [CrossRef]
- Ministry of Health, Malaysia. KKMNOW: COVID-19. In The Latest Data on the Pandemic in Malaysia. 2023. Available online: https://data.moh.gov.my/covid (accessed on 17 February 2023).
- Herng, L.C.; Singh, S.; Sundram, B.M.; Zamri, A.S.S.M.; Vei, T.C.; Aris, T.; Ibrahim, H.; Abdullah, N.H.; Dass, S.C.; Gill, B.S. The effects of super spreading events and movement control measures on the COVID-19 pandemic in Malaysia. Sci. Rep. 2022, 12, 2197. [Google Scholar] [CrossRef]
- Kaos, J. PM: Malaysia Will Transition into Endemic Phase from 1 April. The Star, 8 March 2022. Available online: https://www.thestar.com.my/news/nation/2022/03/08/pm-msia-will-enter-endemic-phase-from-april-1#:~:text=KUALA%20LUMPUR%3A%20Malaysia%20will%20begin,face%20masks%20will%20remain%20mandatory(accessed on 17 February 2023).
- Tullett, W.; McCann, H. Sensing the pandemic: Revealing and re-ordering the senses. Senses Soc. 2022, 17, 170–184. [Google Scholar] [CrossRef]
- Luo, W.; Liu, Z.; Zhou, Y.; Zhao, Y.; Li, Y.E.; Masrur, A.; Yu, M. Investigating Linkages Between Spatiotemporal Patterns of the COVID-19 Delta Variant and Public Health Interventions in Southeast Asia: Prospective Space-Time Scan Statistical Analysis Method. JMIR Public Health Surveill 2022, 8, e35840. [Google Scholar] [CrossRef]
- Xie, Q.; Sundararaj, V.; MR, R. Analyzing the factors affecting the attitude of public toward lockdown, institutional trust, and civic engagement activities. J. Community Psychol. 2022, 50, 806–822. [Google Scholar] [CrossRef]
- Abdul Aziz, A.R.; Ali, Z.; Mohd Noor, N.; Sulaiman, S. Exploring the Compliance Behaviour During COVID-19 Pandemic from Social Psychology Perspectives. Int. J. Acad. Res. Bus. Soc. Sci. 2021, 11, 561–578. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P. Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatr. 2016, 15, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, R.; Truchot, D.; Laurent, E.; Brisson, R.; Schonfeld, I.S. Is burnout solely job-related? A critical comment. Scand. J. Psychol. 2014, 55, 357–361. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013; Volume 5. [Google Scholar]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Dai, H.; Zhang, S.X.; Looi, K.H.; Su, R.; Li, J. Perception of Health Conditions and Test Availability as Predictors of Adults’ Mental Health during the COVID-19 Pandemic: A Survey Study of Adults in Malaysia. Int. J. Environ. Res. Public Health 2020, 17, 5498. [Google Scholar] [CrossRef]
- Esterwood, E.; Saeed, S.A. Past Epidemics, Natural Disasters, COVID19, and Mental Health: Learning from History as we Deal with the Present and Prepare for the Future. Psychiatr. Q. 2020, 91, 1121–1133. [Google Scholar] [CrossRef]
- National Center for Immunization and Respiratory Diseases (NCIRD), Division of Viral Diseases. Middle East Respiratory Syndrome (MERS). Available online: https://www.cdc.gov/coronavirus/mers/index.html (accessed on 15 February 2023).
- Jeong, H.; Yim, H.W.; Song, Y.J.; Ki, M.; Min, J.A.; Cho, J.; Chae, J.H. Mental health status of people isolated due to Middle East Respiratory Syndrome. Epidemiol. Health 2016, 38, e2016048. [Google Scholar] [CrossRef] [Green Version]
- Morganstein, J.C.; Ursano, R.J. Ecological Disasters and Mental Health: Causes, Consequences, and Interventions. Front. Psychiatr. 2020, 11, 1. [Google Scholar] [CrossRef] [Green Version]
- Zeng, N.; Zhao, Y.-M.; Yan, W.; Li, C.; Lu, Q.-D.; Liu, L.; Ni, S.-Y.; Mei, H.; Yuan, K.; Shi, L.; et al. A systematic review and meta-analysis of long term physical and mental sequelae of COVID-19 pandemic: Call for research priority and action. Mol. Psychiatr. 2023, 28, 423–433. [Google Scholar] [CrossRef]
- Liu, S.; Haucke, M.N.; Heinzel, S.; Heinz, A. Long-Term Impact of Economic Downturn and Loneliness on Psychological Distress: Triple Crises of COVID-19 Pandemic. J. Clin. Med. 2021, 10, 4596. [Google Scholar] [CrossRef]
- Dragioti, E.; Li, H.; Tsitsas, G.; Lee, K.H.; Choi, J.; Kim, J.; Choi, Y.J.; Tsamakis, K.; Estradé, A.; Agorastos, A.; et al. A large-scale meta-analytic atlas of mental health problems prevalence during the COVID-19 early pandemic. J. Med. Virol. 2022, 94, 1935–1949. [Google Scholar] [CrossRef]
- Robinson, E.; Sutin, A.R.; Daly, M.; Jones, A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J. Affect. Disord. 2022, 296, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Sampogna, G.; Pompili, M.; Fiorillo, A. Mental Health in the Time of COVID-19 Pandemic: A Worldwide Perspective. Int. J. Environ. Res. Public Health 2022, 19, 161. [Google Scholar] [CrossRef] [PubMed]
- WHO. Pandemic Fatigue: Reinvigorating the Public to Prevent COVID-19: Policy Framework for Supporting Pandemic Prevention and Management: Revised Version November 2020. World Health Organization: Regional Office for Europe. Revised Version. Available online: https://apps.who.int/iris/bitstream/handle/10665/337574/WHO-EURO-2020-1573-41324-56242-eng.pdf?sequence=1&isAllowed=y (accessed on 17 November 2022).
- MacIntyre, C.R.; Nguyen, P.-Y.; Chughtai, A.A.; Trent, M.; Gerber, B.; Steinhofel, K.; Seale, H. Mask use, risk-mitigation behaviours and pandemic fatigue during the COVID-19 pandemic in five cities in Australia, the UK and USA: A cross-sectional survey. Int. J. Infect. Dis. 2021, 106, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Rachor, G.S.; Asmundson, G.J.G. Who develops pandemic fatigue? Insights from Latent Class Analysis. PLoS ONE 2022, 17, e0276791. [Google Scholar] [CrossRef] [PubMed]
- Yan, E.; Ng, H.K.L.; Lai, D.W.L.; Lee, V.W.P. Physical, psychological and pandemic fatigue in the fourth wave of COVID-19 outbreak in Hong Kong: Population-based, cross-sectional study. BMJ Open 2022, 12, e062609. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO/Europe Discusses How to Deal with Pandemic Fatigue. Available online: https://www.who.int/news-room/feature-stories/detail/who-europe-discusses-how-to-deal-with-pandemic-fatigue (accessed on 16 November 2022).
- Rahimian Aghdam, S.; Alizadeh, S.S.; Rasoulzadeh, Y.; Safaiyan, A. Fatigue Assessment Scales: A comprehensive literature review. Arch. Hyg. Sci. 2019, 8, 145–153. [Google Scholar] [CrossRef]
- Michielsen, H.J.; De Vries, J.; Van Heck, G.L. Psychometric qualities of a brief self-rated fatigue measure: The Fatigue Assessment Scale. J. Psychosom. Res. 2003, 54, 345–352. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Krejcie, R.V.; Morgan, D.W. Determining sample size for research activities. Educ. Psychol. Meas. 1970, 30, 607–610. [Google Scholar] [CrossRef]
- Drent, M.; Lower, E.E.; De Vries, J. Sarcoidosis-associated fatigue. Eur. Respir. J. 2012, 40, 255. [Google Scholar] [CrossRef] [Green Version]
- Musa, R.; Fadzil, M.A.; Zain, Z. Translation, validation and psychometric properties of Bahasa Malaysia version of the Depression Anxiety and Stress Scales (DASS). ASEAN J. Psychiatr. 2007, 8, 82–89. [Google Scholar]
- Prime Minister’S Department, Department Of Statistics Malaysia. Press Release Current Population Estimates, Malaysia. 2022. Available online: https://www.dosm.gov.my/v1/index.php?r=column/pdfPrev&id=dTZXanV6UUdyUEQ0SHNWOVhpSXNMUT09 (accessed on 15 February 2023).
- Department Of Statistics Malaysia. Press Release. Household Income & Basic Amenities Survey Report 2019. Available online: https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=120&bul_id=TU00TmRhQ1N5TUxHVWN0T2VjbXJYZz09&menu_id=amVoWU54UTl0a21NWmdhMjFMMWcyZz09# (accessed on 15 February 2023).
- National Health and Morbidity Survey (NHMS). Vol. I: NCDs—Non-Communicable Diseases: Risk Factors and Other Health Problems. 2019. Available online: https://iku.gov.my/images/IKU/Document/REPORT/NHMS2019/Report_NHMS2019-NCD_v2.pdf (accessed on 15 February 2023).
- Tabari, P.; Amini, M.; Moghadami, M.; Moosavi, M. International Public Health Responses to COVID-19 Outbreak: A Rapid Review. Iran. J. Med. Sci. 2020, 45, 157–169. [Google Scholar] [CrossRef]
- Morgul, E.; Bener, A.; Atak, M.; Akyel, S.; Aktaş, S.; Bhugra, D.; Ventriglio, A.; Jordan, T.R. COVID-19 pandemic and psychological fatigue in Turkey. Int. J. Soc. Psychiatr. 2020, 67, 128–135. [Google Scholar] [CrossRef]
- Uygur, O.F.; Uygur, H. Association of post-COVID-19 fatigue with mental health problems and sociodemographic risk factors. Fatigue Biomed. Health Behav. 2021, 9, 196–208. [Google Scholar] [CrossRef]
- Leung, H.T.; Gong, W.-J.; Sit, S.M.M.; Lai, A.Y.K.; Ho, S.Y.; Wang, M.P.; Lam, T.H. COVID-19 pandemic fatigue and its sociodemographic and psycho-behavioral correlates: A population-based cross-sectional study in Hong Kong. Sci. Rep. 2022, 12, 16114. [Google Scholar] [CrossRef]
- Xin, L.; Wang, L.; Cao, X.; Tian, Y.; Yang, Y.; Wang, K.; Kang, Z.; Zhao, M.; Feng, C.; Wang, X.; et al. Prevalence and influencing factors of pandemic fatigue among Chinese public in Xi’an city during COVID-19 new normal: A cross-sectional study. Front. Public Health 2022, 10, 971115. [Google Scholar] [CrossRef]
- Santomauro, D.F.; Mantilla Herrera, A.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Knolle, F.; Ronan, L.; Murray, G.K. The impact of the COVID-19 pandemic on mental health in the general population: A comparison between Germany and the UK. BMC Psychol. 2021, 9, 60. [Google Scholar] [CrossRef]
- Shi, L.; Lu, Z.A.; Que, J.Y.; Huang, X.L.; Liu, L.; Ran, M.S.; Gong, Y.M.; Yuan, K.; Yan, W.; Sun, Y.K.; et al. Prevalence of and Risk Factors Associated with Mental Health Symptoms Among the General Population in China During the Coronavirus Disease 2019 Pandemic. JAMA Netw. Open 2020, 3, e2014053. [Google Scholar] [CrossRef]
- Department of Statistics Malaysia. Household Income Estimates and Incidence of Poverty Report, Malaysia. 2020. Available online: https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=493&bul_id=VTNHRkdiZkFzenBNd1Y1dmg2UUrZz09&menu_id=amVoWU54UTl0a21NWmdhMjFMMWcyZz09#:~:text=In%202020%2C%20there%20was%20an,moved%20to%20the%20B40%20group (accessed on 18 November 2022).
- Wong, L.P.; Alias, H.; Md Fuzi, A.A.; Omar, I.S.; Mohamad Nor, A.; Tan, M.P.; Baranovich, D.L.; Saari, C.Z.; Hamzah, S.H.; Cheong, K.W.; et al. Escalating progression of mental health disorders during the COVID-19 pandemic: Evidence from a nationwide survey. PLoS ONE 2021, 16, e0248916. [Google Scholar] [CrossRef]
- Tang, K.H.D. Movement control as an effective measure against COVID-19 spread in Malaysia: An overview. J. Public Health 2022, 30, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Ismail, M.K.; Sarifuddin, S.; Muhamad, M.Z.; Siwar, C. Levels of Stress, Anxiety, and Depression in the Initial Stage of Movement Control Order in Malaysia: A Sociodemographic Analysis. Proceedings 2022, 82, 14. [Google Scholar] [CrossRef]
- Haktanir, A.; Can, N.; Seki, T.; Kurnaz, M.F.; Dilmaç, B. Do we experience pandemic fatigue? current state, predictors, and prevention. Curr. Psychol. 2021, 41, 7314–7325. [Google Scholar] [CrossRef] [PubMed]
- Kesebir, P. A quiet ego quiets death anxiety: Humility as an existential anxiety buffer. J. Personal. Soc. Psychol. 2014, 106, 610. [Google Scholar] [CrossRef]
- Zhang, J.; Peng, J.; Gao, P.; Huang, H.; Cao, Y.; Zheng, L.; Miao, D. Relationship between meaning in life and death anxiety in the elderly: Self-esteem as a mediator. BMC Geriatr. 2019, 19, 308. [Google Scholar] [CrossRef] [Green Version]
- Menzies, R.E.; Menzies, R.G. Death anxiety in the time of COVID-19: Theoretical explanations and clinical implications. Cogn. Behav. Ther. 2020, 13, e19. [Google Scholar] [CrossRef]
- Bulut, M.B. Relationship between COVID-19 anxiety and fear of death: The mediating role of intolerance of uncertainty among a Turkish sample. Curr. Psychol. 2022, 1–10. [Google Scholar] [CrossRef]
- Chalhoub, Z.; Koubeissy, H.; Fares, Y.; Abou-Abbas, L. Fear and death anxiety in the shadow of COVID-19 among the Lebanese population: A cross-sectional study. PLoS ONE 2022, 17, e0270567. [Google Scholar] [CrossRef]
- Bahar Moni, A.S.; Abdullah, S.; Abdullah, M.F.I.L.; Kabir, M.S.; Alif, S.M.; Sultana, F.; Salehin, M.; Islam, S.M.S.; Cross, W.; Rahman, M.A. Psychological distress, fear and coping among Malaysians during the COVID-19 pandemic. PLoS ONE 2021, 16, e0257304. [Google Scholar] [CrossRef]
- Taylor, S. The Psychology of Pandemics. Annu. Rev. Clin. Psychol. 2022, 18, 581–609. [Google Scholar] [CrossRef]
- Leavy, R.L. Social support and psychological disorder: A review. J. Community Psychol. 1983, 11, 3–21. [Google Scholar] [CrossRef]
- Kessler, R.C.; Price, R.H.; Wortman, C.B. Social factors in psychopathology: Stress, social support, and coping processes. Annu. Rev. Psychol. 1985, 36, 531–572. [Google Scholar] [CrossRef]
- McGinty, E.E.; Presskreischer, R.; Han, H.; Barry, C.L. Psychological Distress and Loneliness Reported by US Adults in 2018 and April 2020. JAMA 2020, 324, 93–94. [Google Scholar] [CrossRef]
- Saltzman, L.Y.; Hansel, T.C.; Bordnick, P.S. Loneliness, isolation, and social support factors in post-COVID-19 mental health. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S55–S57. [Google Scholar] [CrossRef]
- Alnazly, E.; Khraisat, O.M.; Al-Bashaireh, A.M.; Bryant, C.L. Anxiety, depression, stress, fear and social support during COVID-19 pandemic among Jordanian healthcare workers. PLoS ONE 2021, 16, e0247679. [Google Scholar] [CrossRef]
- Ministry of Health, Malaysia. National COVID-19 Testing Strategy [Press Release]. Available online: https://covid-19.moh.gov.my/reopeningsafely/nts (accessed on 18 November 2022).
- Esa, M.; Ibrahim, F.S.; Mustafa Kamal, E. COVID-19 pandemic lockdown: The consequences towards project success in Malaysian construction industry. Adv. Sci. Technol. Eng. Syst. J. 2020, 25, 973–983. [Google Scholar] [CrossRef]
- Piraveenan, M.; Sawleshwarkar, S.; Walsh, M.; Zablotska, I.; Bhattacharyya, S.; Farooqui, H.H.; Bhatnagar, T.; Karan, A.; Murhekar, M.; Zodpey, S.; et al. Optimal governance and implementation of vaccination programmes to contain the COVID-19 pandemic. R. Soc. Open Sci. 2021, 8, 210429. [Google Scholar] [CrossRef]
- Md Iderus, N.H.; Lakha Singh, S.S.; Mohd Ghazali, S.; Yoon Ling, C.; Cia Vei, T.; Md Zamri, A.S.S.; Ahmad Jaafar, N.; Ruslan, Q.; Ahmad Jaghfar, N.H.; Gill, B.S. Correlation between Population Density and COVID-19 Cases during the Third Wave in Malaysia: Effect of the Delta Variant. Int. J. Environ. Res. Public Health 2022, 19, 7439. [Google Scholar] [CrossRef]
- Law, L.N.-S.; Loo, K.-Y.; Goh, J.X.H.; Pusparajah, P. Omicron: The rising fear for another wave in Malaysia. Prog. Microbes Mol. Biol. 2021, 4, a0000261. [Google Scholar] [CrossRef]
- Petherick, A.; Goldszmidt, R.; Andrade, E.B.; Furst, R.; Hale, T.; Pott, A.; Wood, A. A worldwide assessment of changes in adherence to COVID-19 protective behaviours and hypothesized pandemic fatigue. Nat. Hum. Behav. 2021, 5, 1145–1160. [Google Scholar] [CrossRef]
- Rashid, A.A.; Rashid, M.R.A.; Yaman, M.N.; Mohamad, I. Teaching Medicine Online During the COVID-19 Pandemic: A Malaysian Perspective. Bangladesh J. Med. Sci. 2020, 19, S77–S81. [Google Scholar] [CrossRef]
- Abiddin, N.Z.; Ibrahim, I.; Abdul Aziz, S.A. A Literature Review of Work From Home Phenomenon During COVID-19 Toward Employees’ Performance and Quality of Life in Malaysia and Indonesia. Front. Psychol. 2022, 13, 819860. [Google Scholar] [CrossRef] [PubMed]
- Van Loenhout, J.A.F.; Vanderplanken, K.; Scheen, B.; Van den Broucke, S.; Aujoulat, I. Determinants of adherence to COVID-19 measures among the Belgian population: An application of the protection motivation theory. Arch. Public Health 2021, 79, 74. [Google Scholar] [CrossRef] [PubMed]
- Dekeyser, S.; Schmits, E.; Glowacz, F.; Klein, O.; Schmitz, M.; Wollast, R.; Yzerbyt, V.; Luminet, O. Predicting Compliance with Sanitary Behaviors among Students in Higher Education During the Second COVID-19 Wave: The Role of Health Anxiety and Risk Perception. Psychol. Belg. 2023, 63, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Supriyati Supriyati, D.; Fahmi Baiquni, M.P.H.; Tri Siswati, D.; Herni Endah Widyawati, S.T.; Gz, R.; Rahmawati, S.T.P.; Wardani, R.K.; Gz, S. Social determinants of health protocol adherence among adults during COVID-19 pandemic in Yogyakarta, Indonesia. Med. J. Malays. 2022, 77, 5–9. [Google Scholar]
- Ojo, A.O.; Arasanmi, C.N.; Raman, M.; Tan, C.N.-L. Ability, motivation, opportunity and sociodemographic determinants of Internet usage in Malaysia. Inf. Dev. 2019, 35, 819–830. [Google Scholar] [CrossRef]
- Kyaw, T.M.; Deng, A.G.; Mano Mohen, S.; Uvaraja, V.D.; Mustafa, S.M. Assessment of Digital Health Literacy and Its Associated Factors Among University Students During COVID-19 Pandemic in Malaysia. J. Health Lit. 2022, 7, 9–27. [Google Scholar] [CrossRef]
- Selvaraj, A.; Radhin, V.; Ka, N.; Benson, N.; Mathew, A.J. Effect of pandemic based online education on teaching and learning system. Int. J. Educ. Dev. 2021, 85, 102444. [Google Scholar] [CrossRef]
- Harun, Z.; Hamzah, F.M.; Mansor, S.; Mahmud, A.S.; Hashim, H.; Sultan, M.T.H.; Mohamed, N.M.Z.N.; Ibrahim, M.D.; Hasin, H.; Saad, M.R. COVID-19 Effects on Students’ Teaching and Learning Perspectives in Malaysian Varsities. Pertanika J. Soc. Sci. Humanit. 2021, 29, 2729–2748. [Google Scholar] [CrossRef]
- Bozkurt, V. Working during a pandemic: Economic concerns, digitalization, and productivity. COVID-19 Pandemic Its Econ. Soc. Political Impacts 2020, 87, 106. [Google Scholar] [CrossRef]
- Banerjee, D.; Vaishnav, M.; Rao, T.S.; Raju, M.; Dalal, P.; Javed, A.; Saha, G.; Mishra, K.K.; Kumar, V.; Jagiwala, M.P. Impact of the COVID-19 pandemic on psychosocial health and well-being in South-Asian (World Psychiatric Association zone 16) countries: A systematic and advocacy review from the Indian Psychiatric Society. Indian J. Psychiatry 2020, 62, S343. [Google Scholar] [CrossRef]
- Ministry of Finance, Malaysia. Budget Speech 2023. Available online: https://budget.mof.gov.my/pdf/2023/ucapan/buku-budget-speech-2023.pdf (accessed on 18 November 2022).



{kind=link}
{kind=link}
| Sociodemographic Characteristics | Official Demographic Data (Million) a | Total (N) (100%) | Fatigued b | Non-Fatigued | Statistic | |
|---|---|---|---|---|---|---|
| (n = 420), n (%) | (n = 355), n (%) | |||||
| Age, mean (standard deviation) | 29.78 (11.115) | 34.6 | OR = 0.967 [95% CI = 0.956, 0.979], p < 0.001 * | |||
| (12.831) | ||||||
| Gender | Male | 17 [41] | 268 | 133 (49.6) | 135 (50.4) | χ2 = 3.44, p = 0.064 |
| Female | 15.7 [41] | 507 | 287 (56.6) | 220 (43.4) | ||
| Ethnicity | Malay | 69.9 [41] | 637 | 333 (52.3) | 304 (47.7) | χ2 = 5.30, p = 0.021 * |
| Non-Malay | 30.1 [41] | 138 | 87 (63.0) | 51 (37.0) | ||
| Regions in Malaysia | North Peninsular | 91 | 53 (58.2) | 38 (41.8) | χ2 = 3.65, p = 0.456 | |
| Central Peninsular | 267 | 154 (57.7) | 113 (42.3) | |||
| South Peninsular | 216 | 112 (51.9) | 104 (48.1) | |||
| East Peninsular | 161 | 81 (50.3) | 80 (49.7) | |||
| East Malaysia | 40 | 20 (50.0) | 20 (50.0) | |||
| Education level | Secondary | 63 | 39 (61.9) | 24 (38.1) | χ2 = 1.64, p = 0.200 | |
| Tertiary | 712 | 381 (53.5) | 331 (46.5) | |||
| Living arrangement | Alone | 412 | 250 (60.7) | 162 (39.3) | χ2 = 14.91, p < 0.001 * | |
| With family/spouse | 363 | 170 (46.8) | 193 (53.2) | |||
| Income category | Low (≤MYR4850) | 2.91 [42] | 303 | 189 (62.4) | 114 (37.6) | χ2 = 13.42, p < 0.001 * |
| Middle/ High (>MYR4850) | 4.37 [42] | 472 | 231 (48.9) | 241 (51.1) | ||
| Having chronic diseases | No | 61.2 (%) [43] | 628 | 343 (54.6) | 285 (45.4) | χ2 = 0.24, p = 0.646 |
| Yes | 38.8 (%) [43] | 147 | 77 (52.3) | 70 (47.6) | ||
| Past COVID-19 infection | No | 511 | 275 (53.8) | 236 (46.2) | χ2 = 0.09, p = 0.769 | |
| Yes | 264 | 145 (54.9) | 119 (45.1) | |||
| Work from home (n = 755) | No | 401 | 209 (52.1) | 192 (47.9) | χ2 = 1.65, p = 0.200 | |
| Yes | 354 | 201 (56.8) | 153 (43.2) | |||
| Variable | B | Crude Odds Ratio | 95% CI | p-Value |
|---|---|---|---|---|
| Depression score | 0.25 | 1.29 | 1.24, 1.34 | <0.001 * |
| Anxiety score | 0.24 | 1.27 | 1.22, 1.32 | <0.001 * |
| Stress score | 0.21 | 1.23 | 1.12, 1.27 | <0.001 * |
| Variable | B | Crude Odds Ratio | 95% CI | p-Value |
|---|---|---|---|---|
| Perception of fatigue to comply with the SOP of COVID-19 | 0.02 | 1.02 | 1.00, 1.04 | 0.018 * |
| Perception risk of infection with COVID-19 | 0.06 | 1.06 | 1.02, 1.11 | 0.008 * |
| Perception of distress due to the pandemic | 0.16 | 1.17 | 1.12, 1.22 | <0.001 * |
| Perception of negligence toward pandemic | 0.10 | 1.10 | 1.05, 1.17 | <0.001 * |
| Perception of change due to pandemic | 0.11 | 1.12 | 1.06, 1.18 | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdul Rashid, M.R.; Syed Mohamad, S.N.; Tajjudin, A.I.A.; Roslan, N.; Jaffar, A.; Mohideen, F.B.S.; Addnan, F.H.; Baharom, N.; Ithnin, M. COVID-19 Pandemic Fatigue and Its Sociodemographic, Mental Health Status, and Perceived Causes: A Cross-Sectional Study Nearing the Transition to an Endemic Phase in Malaysia. Int. J. Environ. Res. Public Health 2023, 20, 4476. https://doi.org/10.3390/ijerph20054476
Abdul Rashid MR, Syed Mohamad SN, Tajjudin AIA, Roslan N, Jaffar A, Mohideen FBS, Addnan FH, Baharom N, Ithnin M. COVID-19 Pandemic Fatigue and Its Sociodemographic, Mental Health Status, and Perceived Causes: A Cross-Sectional Study Nearing the Transition to an Endemic Phase in Malaysia. International Journal of Environmental Research and Public Health. 2023; 20(5):4476. https://doi.org/10.3390/ijerph20054476
Chicago/Turabian StyleAbdul Rashid, Mohd Radzniwan, Sharifah Najwa Syed Mohamad, Ahmad Izzat Ahmad Tajjudin, Nuruliza Roslan, Aida Jaffar, Fathima Begum Syed Mohideen, Faizul Helmi Addnan, Nizam Baharom, and Muslimah Ithnin. 2023. "COVID-19 Pandemic Fatigue and Its Sociodemographic, Mental Health Status, and Perceived Causes: A Cross-Sectional Study Nearing the Transition to an Endemic Phase in Malaysia" International Journal of Environmental Research and Public Health 20, no. 5: 4476. https://doi.org/10.3390/ijerph20054476