

An Intervention on Anxiety Symptoms in Moderate Alzheimer’s Disease through Virtual Reality: A Feasibility Study and Lessons Learned
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.2.1. Neuropsychological, Neuropsychiatric, and Attitude Questionnaires
2.2.2. Hardware and Software
2.3. Procedure
2.4. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Adams, R.L.; Craig, P.L.; Parsons, O.A. Neuropsychology of dementia. Neurol. Clinics 1986, 4, 387–404. [Google Scholar] [CrossRef]
- Cunningham, E.L.; McGuinness, B.; Herron, B.; Passmore, A.P. Dementia. Ulster Med. J. 2015, 84, 79–87. [Google Scholar] [PubMed]
- Pasquini, S.; Margaritini, A.; Gambella, E.; Di Rosa, M.; Maranesi, E.; Bevilacqua, R.; Civerchia, P.; Pelliccioni, G. A psychosocial intervention for supporting informal caregivers of older people with alzheimer disease: Protocol for the Innfamiglia randomized controlled trial. JMIR Res. Protoc. 2022, 11, e37496. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 20 September 2022).
- Lyketsos, C.G.; Carrillo, M.C.; Ryan, J.M.; Kachaturian, A.S.; Trzepacz, P.; Amatniek, J.; Cedarbaum, J.; Brashear, R.; Miller, D.S. Neuropsychiatric symptoms in Alzheimer’s disease. Alzheimers Dement. 2011, 7, 532–539. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Li, H.; Huang, J.; Huang, S.; Bai, Y.; Li, Y.; Huang, W. Efficacy of antidepressant drugs in the treatment of depression in Alzheimer disease patients: A systematic review and network meta-analysis. J. Psychopharmacol. 2021, 35, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Orgeta, V.; Tabet, N.; Nilforooshan, R.; Howard, R. Efficacy of antidepressants for depression in Alzheimer’s disease: Systematic review and meta-analysis. J. Alzheimers Dis. 2017, 58, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Mortby, M.E.; Adler, L.; Agüera-Ortiz, L.; Bateman, D.R.; Brodaty, H.; Cantillon, M.; Geda, Y.E.; Ismail, Z.; Lanctôt, K.L.; Marshall, G.A.; et al. Apathy as a treatment target in Alzheimer’s disease: Implications for clinical trials. Am. J. Geriatr. Psychiatry 2022, 30, 119–147. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, A.L.; Gonzales, M.M.; de Souza, L.C.; Weisenbach, S.L. Revisiting apathy in Alzheimer’s disease: From conceptualization to therapeutic approaches. Behav. Neurol. 2021, 2021, 6319826. [Google Scholar] [CrossRef]
- Caraci, F.; Santagati, M.; Caruso, G.; Cannavò, D.; Leggio, G.M.; Salomone, S.; Drago, F. New antipsychotic drugs for the treatment of agitation and psychosis in Alzheimer’s disease: Focus on brexpiprazole and pimavanserin. F1000Research 2020, 9, F1000 Faculty Rev-686. [Google Scholar] [CrossRef]
- Millán-Calenti, J.C.; Lorenzo-López, L.; Alonso-Búa, B.; de Labra, C.; González-Abraldes, I.; Maseda, A. Optimal nonpharmacological management of agitation in Alzheimer’s disease: Challenges and solutions. Clin. Interv. Aging. 2016, 11, 175–184. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Q.-F.; Tan, L.; Wang, H.-F.; Jiang, T.; Tan, M.-S.; Tan, L.; Xu, W.; Li, J.-Q.; Wang, J.; Lai, T.-J.; et al. The prevalence of neuropsychiatric symptoms in Alzheimer’s disease: Systematic review and metaanalysis. J. Affect. Disord. 2016, 190, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Brodaty, H.; Connors, M.H.; Xu, J.; Woodward, M.; Ames, D.; PRIME Study Group. The course of neuropsychiatric symptoms in dementia: A 3-year longitudinal study. J. Am. Med. Dir. Assoc. 2015, 16, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Kwak, Y.T.; Yang, Y.S.; Kwak, S.G. Clinical characteristics of behavioral and psychological symptoms in patients with drug-naïve Alzheimer’s disease. Dement. Neurocogn. Disord. 2012, 11, 87–94. [Google Scholar] [CrossRef]
- Tanaka, H.; Hashimoto, M.; Fukuhara, R.; Ishikawa, T.; Yatabe, Y.; Kaneda, K.; Yuuki, S.; Honda, K.; Matsuzaki, S.; Tsuyuguchi, A.; et al. Relationship between dementia severity and behavioural and psychological symptoms in early-onset Alzheimer’s disease. Psychogeriatrics 2015, 15, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Chemerinski, E.; Petracca, G.; Manes, F.; Leiguarda, R.; Starkstein, S.E. Prevalence and correlates of anxiety in Alzheimer’s disease. Depress. Anxiety 1998, 7, 166–170. [Google Scholar] [CrossRef]
- Starkstein, S.E.; Jorge, R.; Petracca, G.; Robinson, R.G. The construct of generalized anxiety disorder in Alzheimer disease. Am. J. Geriatr. Psychiatry 2007, 15, 42–49. [Google Scholar] [CrossRef]
- Calleo, J.S.; Kunik, M.E.; Reid, D.; Kraus-Schuman, C.; Paukert, A.; Regev, T.; Wilson, N.; Petersen, N.J.; Snow, A.L.; Stanley, M. Characteristics of generalized anxiety disorder in patients with dementia. Am. J. Alzheimers Dis. Other Demen. 2011, 26, 492–497. [Google Scholar] [CrossRef]
- Kwak, Y.T.; Yang, Y.S.; Koo, M.S. Anxiety in dementia. Dement. Neurocogn. Disord. 2017, 16, 33–39. [Google Scholar] [CrossRef]
- Seignourel, P.J.; Kunik, M.E.; Snow, L.; Wilson, N.; Stanley, M. Anxiety in dementia: A critical review. Clin. Psychol. Rev. 2008, 28, 1071–1082. [Google Scholar] [CrossRef]
- Mah, L.; Binns, M.A.; Steffens, D.C.; Alzheimer’s Disease Neuroimaging Initiative. Anxiety symptoms in amnestic mild cognitive impairment are associated with medial temporal atrophy and predict conversion to Alzheimer disease. Am. J. Geriatr. Psychiatry 2015, 23, 466–476. [Google Scholar] [CrossRef] [Green Version]
- James, I. Using a cognitive rationale to conceptualize anxiety in people with dementia. Behav. Cogn. Psychother. 1999, 27, 345–351. [Google Scholar] [CrossRef]
- Dimitriou, T.D.; Verykouki, E.; Papatriantafyllou, J.; Konsta, A.; Kazis, D.; Tsolaki, M. Non-pharmacological interventions for the anxiety in patients with dementia. A cross-over randomised controlled trial. Behav. Brain Res. 2020, 390, 112617. [Google Scholar] [CrossRef] [PubMed]
- Chirico, A.; Maiorano, P.; Indovina, P.; Milanese, C.; Giordano, G.G.; Alivernini, F.; Iodice, G.; Gallo, L.; De Pietro, G.; Lucidi, F.; et al. Virtual reality and music therapy as distraction interventions to alleviate anxiety and improve mood states in breast cancer patients during chemotherapy. J. Cell. Physiol. 2020, 235, 5353–5362. [Google Scholar] [CrossRef]
- Appel, L.; Appel, E.; Bogler, O.; Wiseman, M.; Cohen, L.; Ein, N.; Abrams, H.B.; Campos, J.L. Older adults with cognitive and/or physical impairments can benefit from immersive virtual reality experiences: A feasibility study. Front. Med. 2020, 6, 329. [Google Scholar] [CrossRef] [PubMed]
- Niki, K.; Yahara, M.; Inagaki, M.; Takahashi, N.; Watanabe, A.; Okuda, T.; Ueda, M.; Iwai, D.; Sato, K.; Ito, T. Immersive virtual reality reminiscence reduces anxiety in the oldest-old without causing serious side effects: A single-center, pilot, and randomized crossover study. Front. Hum. Neurosci. 2021, 14, 598161. [Google Scholar] [CrossRef]
- Brimelow, R.E.; Thangavelu, K.; Beattie, R.; Dissanayaka, N.N. Feasibility of group-based multiple virtual reality sessions to reduce behavioral and psychological symptoms in persons living in residential aged care. J. Am. Med. Dir. Assoc. 2022, 23, 831–837.e2. [Google Scholar] [CrossRef]
- Lozano-Gallego, M.; Hernández-Ferrándiz, M.; Turró-Garriga, O.; Pericot-Nierga, I.; López-Pousa, S.; Vilalta-Franch, J. Validación del Montreal Cognitive Assessment (MoCA): Test de cribado para el deterioro cognitivo leve. Datos preliminares. Alzheimer Real Invest. Demen. 2009, 43, 4–11. [Google Scholar]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Boada, M.; Cejudo, J.C.; Tàrraga, L.; López, O.L.; Kaufer, D. Neuropsychiatric inventory questionnaire (NPI-Q): Spanish validation of an abridged form of the Neuropsychiatric Inventory (NPI). Neurologia 2002, 17, 317–323. [Google Scholar]
- Kaufer, D.I.; Cummings, J.L.; Ketchel, P.; Smith, V.; MacMillan, A.; Shelley, T.; Lopez, O.L.; DeKosky, S.T. Validation of the NPI-Q, a brief clinical form of the Neuropsychiatric Inventory. J. Neuropsychiatry Clin. Neurosci. 2000, 12, 233–239. [Google Scholar] [CrossRef]
- Morris, J.C. The clinical dementia rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef] [PubMed]
- Valoración Clínica de Demencia. Available online: http://www.sld.cu/galerias/pdf/sitios/rehabilitacion/valoracion_clinica_de_demencia.pdf (accessed on 30 November 2021).
- Reisberg, B.; Ferris, S.H.; de León, M.D.; Crook, T. The global deterioration scale for assessment of primary degenerative dementia. Am. J. Psychiatry 1982, 139, 1136–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tárraga, L.L. Evaluación del deterioro cognitive y functional de la demencia. Escalas de mayor interés en la Atención Primaria. In El Medico ante la Demencia y su Entorno, Módulo 1; Boada, M., Tárraga, L.L., Eds.; Bayer, S.A.: Barcelona, Spain, 1995; pp. 37–50. [Google Scholar]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychiat. 1959, 32, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Lobo, A.; Chamorro, L.; Luque, A.; Dal-Ré, R.; Badia, X.; Baró, E.; Grupo de Validación en Español de Escalas Psicométricas (GVEEP). Validation of the Spanish versions of the Montgomery-Asberg Depression Rating Scale and the Hamilton Anxiety Rating Scale for the assessment of depression and anxiety. Med. Clínica 2002, 118, 493–499. [Google Scholar] [CrossRef]
- Fernández-Blázquez, M.A.; Ávila-Villanueva, M.; López-Pina, J.A.; Zea-Sevilla, M.A.; Frades-Payo, B. Psychometric properties of a new short version of the State-Trait Anxiety Inventory (STAI) for the assessment of anxiety in the elderly. Neurología 2015, 30, 352–358. [Google Scholar] [CrossRef]
- Cummings, J.L.; Mega, M.; Gray, K.; Rosenberg-Thompson, S.; Carusi, D.A.; Gornbein, J. The Neuropsychiatric Inventory: Comprehensive assessment of psychopathology in dementia. Neurology 1994, 44, 2308–2314. [Google Scholar] [CrossRef]
- Vilalta-Franch, J.; Lozano-Gallego, M.; Hernández-Ferràndiz, M.; Llinàs-Reglà, J.; López-Pousa, S.; López, O.L. The Neuropsychiatric Inventory. Psychometric properties of its adaptation into Spanish. Rev. Neurol. 1999, 29, 15–19. [Google Scholar]
- Maples-Keller, J.L.; Bunnell, B.E.; Kim, S.-J.; Rothbaum, B.O. The use of virtual reality technology in the treatment of anxiety and other psychiatric disorders. Harv. Rev. Psychiatry 2017, 25, 103–113. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Dakoure, C.; Ben Addessalem, H.; Boukadida, M.; Cuesta, M.; Bruneau, M.-A.; Belleville, S.; Frasson, C. Virtual savannah: An effective therapeutic and relaxing treatment for people with subjective cognitive decline. In Proceedings of the Brain Function Assessment in Learning (BFAL): Second International Conference, Heraklion, Greece, 9–11 October 2020. [Google Scholar] [CrossRef]
- Schrempf, M.C.; Petzold, J.; Petersen, M.A.; Arndt, T.T.; Schiele, S.; Vachon, H.; Vlasenko, D.; Wolf, S.; Anthuber, M.; Müller, G.; et al. A randomised pilot trial of virtual reality-based relaxation for enhancement of perioperative well-being, mood and quality of life. Sci. Rep. 2022, 12, 12067. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Participant | Sex | Age | Education | Medication |
|---|---|---|---|---|
| BA | Female | 88 | Primary (literate) | Memantine 20 mg |
| BE | Female | 86 | Primary (literate) | Memantine 20 mg |
| BF | Female | 64 | Primary (literate) | Memantine 20 mg |
| Psychological and Physiological Dimensions | Instrument |
|---|---|
| Cognitive functions Level of dementia Anxiety Psychopathology Heart rate, SpO2, blood pressure, breathing rate | MoCA CDR, GDS NPI, STAIr, HARS NPI-Q Wristband |
| Pre-Assessment (Baseline) 1st Week | Intervention 2nd, 3rd, 4th Week | Post-Assessment 5th Week |
|---|---|---|
| MoCA NPI-Q CDR GDS HARS STAIr trait STAIr state NPI | Exposure to iVR (9 sessions) + Physiological recordings (pre, 5, 10, and 15 min, and post) + STAIr state | MoCA NPI-Q CDR GDS HARS STAIr trait NPI |
| Test | Timing | Mdn | Min | Max | W | p Value | Rank-Biserial Correlation |
|---|---|---|---|---|---|---|---|
| MoCA | Pre Post | 3 3 | 3 3 | 7 6 | 1.000 | 0.977 | 1.000 |
| NPI-Q | Pre Post | 18 17 | 15 14 | 44 44 | 1.500 | 0.681 | 0.000 |
| CDR | Pre Post | 2 2 | 2 2 | 3 3 | (a) | - | - |
| GDS | Pre Post | 5 5 | 5 5 | 6 5 | (b) | - | - |
| HARS psy | Pre Post | 14 13 | 11 9 | 14 13 | 6.000 | 0.087 | 1.000 |
| HARS som | Pre Post | 6 4 | 0 0 | 6 6 | 1.000 | 0.500 | 1.000 |
| NPI | Pre Post | 0 0 | 0 0 | 1 1 | (a) | - | - |
| STAIr trait | Pre Post | 3 3 | 2 2 | 3 3 | (a) | - | - |
| STAIr state | Pre Week 2 Week 3 Week 4 | 2 2 2 1 | 1 1 1 1 | 2 2 2 2 | Friedman Test χ2 (3) = 1.286 | p = 0.733 |
| Physiological Measure | Friedman Test | p-value | Connover’s Post Hoc |
|---|---|---|---|
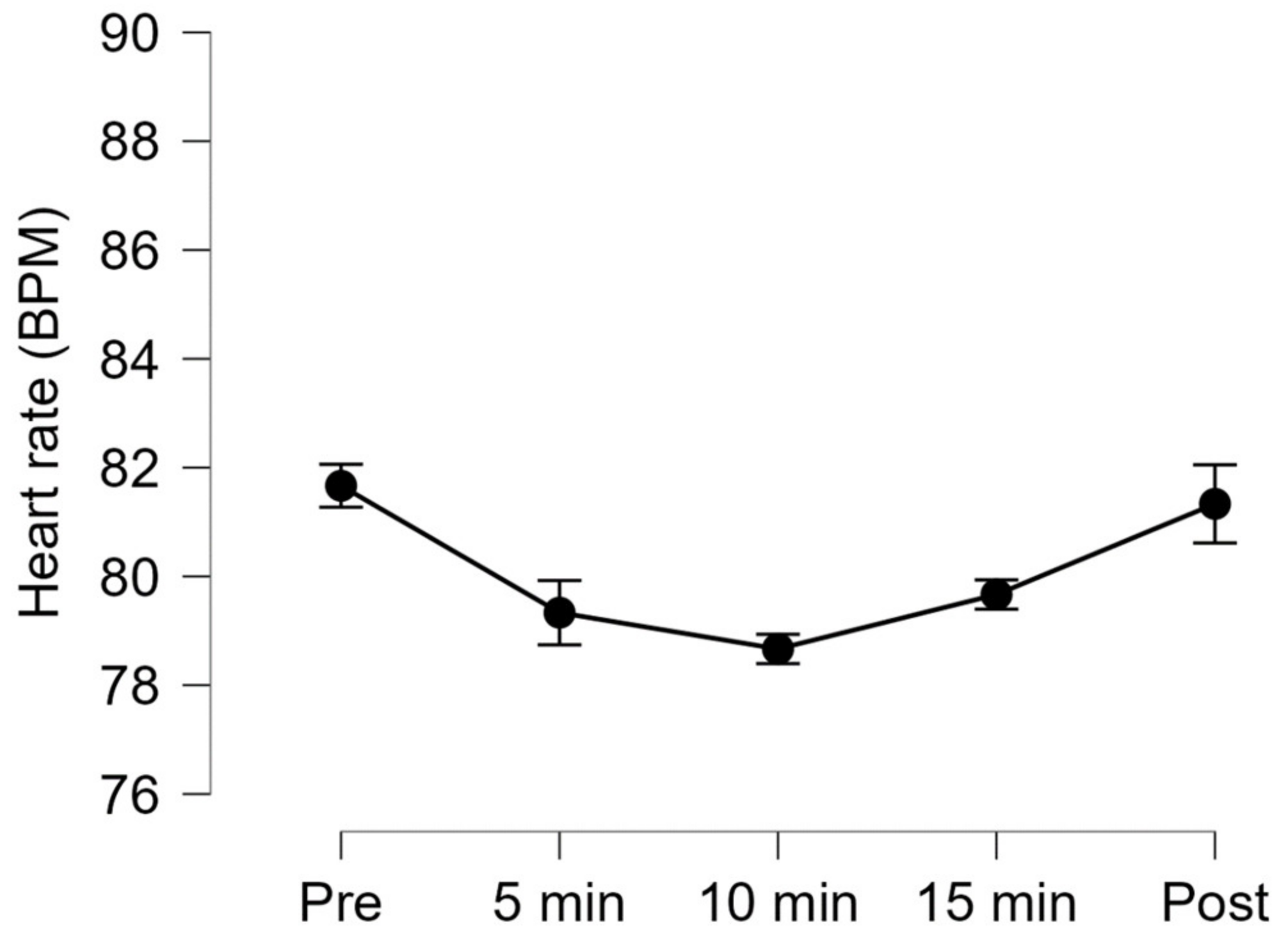
| Heart rate | χ2(4) = 10.538 | 0.032 * | >0.05 for all pairwise comparisons (Holm correction) |
| Breathing rate | χ2(4) = 7.721 | 0.102 | - |
| Diastolic blood presure | χ2(4) = 6.667 | 0.155 | - |
| Systolic blood pressure | χ2(4) = 5.037 | 0.284 | - |
| SpO2 | χ2(4) = 3.000 | 0.558 | - |
| Item | “Nothing” | “Something” | “Much” |
|---|---|---|---|
| “Did you feel well while you were watching the landscapes in VR?” | 0 | 0 | 3 |
| “Did you feel bad while you were watching the landscapes in VR?” | 2 | 1 | 0 |
| “Would you like to continue using VR?” | 0 | 1 | 2 |
| Item | “Nothing” | “Something” | “Much” |
|---|---|---|---|
| “Have the patients expressed pleasure with the VR-based intervention?” | X | ||
| “Have the patients expressed displeasure with the VR-based intervention?” | X | ||
| “Do you think it would be positive to continue using the VR-based intervention?” | X | ||
| “Which benefits do you perceive in this activity?” | Mainly relaxation and motivation for new activities. | ||
| “Which problems do you perceive in this activity?” | None. | ||
| “Would you make any change in the intervention?” | Increase the number of participants and the possibility of interactions. | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Nieto, D.; Castaño-Castaño, S.; Navarro-Martos, R.; Obrero-Gaitán, E.; Cortés-Pérez, I.; Nieto-Escamez, F. An Intervention on Anxiety Symptoms in Moderate Alzheimer’s Disease through Virtual Reality: A Feasibility Study and Lessons Learned. Int. J. Environ. Res. Public Health 2023, 20, 2727. https://doi.org/10.3390/ijerph20032727
Sánchez-Nieto D, Castaño-Castaño S, Navarro-Martos R, Obrero-Gaitán E, Cortés-Pérez I, Nieto-Escamez F. An Intervention on Anxiety Symptoms in Moderate Alzheimer’s Disease through Virtual Reality: A Feasibility Study and Lessons Learned. International Journal of Environmental Research and Public Health. 2023; 20(3):2727. https://doi.org/10.3390/ijerph20032727
Chicago/Turabian StyleSánchez-Nieto, Desirée, Sergio Castaño-Castaño, Remedios Navarro-Martos, Esteban Obrero-Gaitán, Irene Cortés-Pérez, and Francisco Nieto-Escamez. 2023. "An Intervention on Anxiety Symptoms in Moderate Alzheimer’s Disease through Virtual Reality: A Feasibility Study and Lessons Learned" International Journal of Environmental Research and Public Health 20, no. 3: 2727. https://doi.org/10.3390/ijerph20032727