
Analysis of Exertion-Related Injuries and Fatalities in Laborers in the United States
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Extraction for Exertion-Related Injuries and Fatalities
2.2. Data Sources and Extraction for Accident Fatalities
2.3. Statistical Analysis
3. Results
3.1. Exertion-Related Injuries
3.2. Exertion-Related Fatalities
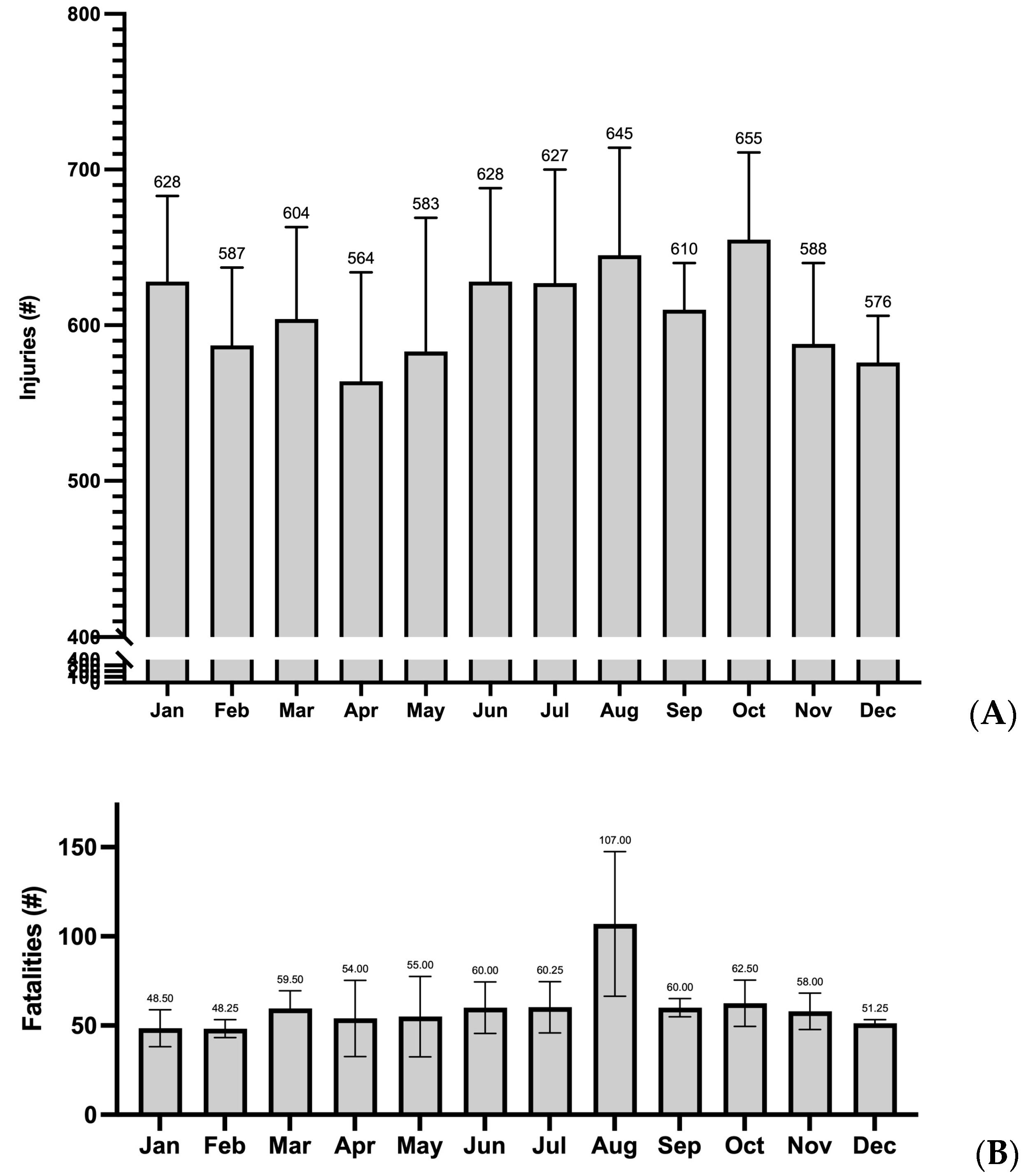
3.3. Accident-Related Injuries and Fatalities
4. Discussion
4.1. Limitations
4.2. Practical Implications and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Labour Organization. ILO: Work Hazards Kill Millions, Cost Billions. 2003. Available online: http://www.ilo.org/global/about-the-ilo/mission-and-objectives/features/WCMS_075615/lang--en/index.htm (accessed on 20 September 2022).
- Gubernot, D.M.; Anderson, G.B.; Hunting, K.L. Characterizing occupational heat-related mortality in the United States, 2000–2010: An analysis using the Census of Fatal Occupational Injuries database. Am. J. Ind. Med. 2015, 58, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Gubernot, D.M.; Anderson, G.B.; Hunting, K.L. The epidemiology of occupational heat exposure in the United States: A review of the literature and assessment of research needs in a changing climate. Int. J. Biometeorol. 2014, 58, 1779–1788. [Google Scholar] [CrossRef] [PubMed]
- Tustin, A.W.; Lamson, G.E.; Jacklitsch, B.L.; Thomas, R.; Arbury, S.; Cannon, D.; Gonzales, R.; Hodgson, M. Evaluation of Occupational Exposure Limits for Heat Stress in Outdoor Workers—United States, 2011–2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 733–737. [Google Scholar] [CrossRef] [PubMed]
- Spector, J.T.; Krenz, J.; Calkins, M.; Ryan, D.; Carmona, J.; Pan, M.; Zemke, A.; Sampson, P.D. Associations between heat exposure, vigilance, and balance performance in summer tree fruit harvesters. Appl. Ergon. 2018, 67, 1–8. [Google Scholar] [CrossRef]
- Spector, J.T.; Bonauto, D.K.; Sheppard, L.; Busch-Isaksen, T.; Calkins, M.; Adams, D.; Lieblich, M.; Fenske, R.A. A Case-Crossover Study of Heat Exposure and Injury Risk in Outdoor Agricultural Workers. PLoS ONE 2016, 11, e0164498. [Google Scholar] [CrossRef]
- Flouris, A.D.; Dinas, P.C.; Ioannou, L.G.; Nybo, L.; Havenith, G.; Kenny, G.P.; Kjellstrom, T. Workers’ health and productivity under occupational heat strain: A systematic review and meta-analysis. Lancet Planet Health 2018, 2, e521–e531. [Google Scholar] [CrossRef]
- Medical Surveillance of Injuries in the U.S. Military Descriptive Epidemiology and Recommendations for Improvement—PubMed. Available online: https://pubmed-ncbi-nlm-nih-gov.ezproxy.lib.uconn.edu/20117600/ (accessed on 17 August 2022).
- Descriptive Epidemiology of Collegiate Men’s Baseball Injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 Through 2003–2004—PMC. Available online: https://www-ncbi-nlm-nih-gov.ezproxy.lib.uconn.edu/pmc/articles/PMC1941283/ (accessed on 17 August 2022).
- Descriptive Epidemiology of 153 Diving Injuries With Rebreathers Among French Military Divers From 1979 to 2009|Military Medicine|Oxford Academic. Available online: https://academic-oup-com.ezproxy.lib.uconn.edu/milmed/article/176/4/446/4345389 (accessed on 17 August 2022).
- Speakman, R.O. Descriptive Epidemiology of Air Transportation Fatalities from the United States Air Force Mortality Registry. Available online: https://corescholar.libraries.wright.edu/mph/203/ (accessed on 17 August 2022).
- Boden, B.P.; Breit, I.; Beachler, J.A.; Williams, A.; Mueller, F.O. Fatalities in High School and College Football Players. Am. J. Sports Med. 2013, 41, 1108–1116. [Google Scholar] [CrossRef]
- Boden, B.P.; Fine, K.M.; Breit, I.; Lentz, W.; Anderson, S.A. Nontraumatic Exertional Fatalities in Football Players, Part 1: Epidemiology and Effectiveness of National Collegiate Athletic Association Bylaws. 2020. Available online: https://journals-sagepub-com.ezproxy.lib.uconn.edu/doi/full/10.1177/2325967120942490 (accessed on 17 August 2022).
- Probability of Competing Beyond High School—NCAA.org. Available online: https://www.ncaa.org/sports/2013/12/17/probability-of-competing-beyond-high-school.aspx (accessed on 17 August 2022).
- Military Active-Duty Personnel, Civilians by State. Governing. 2013. Available online: https://www.governing.com/archive/military-civilian-active-duty-employee-workforce-numbers-by-state.html (accessed on 17 August 2022).
- Census of Fatal Occupational Injuries Summary, 2020—2020 A01 Results. Available online: https://www.bls.gov/news.release/cfoi.nr0.htm (accessed on 16 August 2022).
- Occupational Safety and Health Administration. OSH Act of 1970. Available online: https://www.osha.gov/laws-regs/oshact/completeoshact (accessed on 19 March 2021).
- Survey of Occupational Injuries and Illnesses Data. Available online: https://www.bls.gov/iif/soii-data.htm (accessed on 19 November 2020).
- Occupational Safety and Health Administration. Severe Injury Reports. Available online: https://www.osha.gov/severeinjury/ (accessed on 17 August 2022).
- OIICS Table of Contents. Available online: https://www.bls.gov/iif/oshoiics.htm (accessed on 17 August 2022).
- Occupational Safety and Health Administration. Fatality Inspection Data. Available online: https://www.osha.gov/fatalities (accessed on 17 August 2022).
- U.S. Department of Labor. Data and Statistics. Available online: https://www.dol.gov/agencies/wb/data (accessed on 10 November 2020).
- Occupational Safety and Health Administration. Heat Injury and Illness Prevention in Outdoor and Indoor Work Settings Rulemaking. Available online: https://www.osha.gov/heat-exposure/rulemaking (accessed on 15 October 2022).
- Diem, J.E.; Stauber, C.E.; Rothenberg, R. Heat in the southeastern United States: Characteristics, trends, and potential health impact. PLoS ONE 2017, 12, e0177937. [Google Scholar] [CrossRef]
- Basu, R.; Samet, J.M. Relation between elevated ambient temperature and mortality: A review of the epidemiologic evidence. Epidemiol. Rev. 2002, 24, 190–202. [Google Scholar] [CrossRef]
- Culp, K.; Tonelli, S. Heat-Related Illness in Midwestern Hispanic Farmworkers: A Descriptive Analysis of Hydration Status and Reported Symptoms. Workplace Health Saf. 2019, 67, 168–178. [Google Scholar] [CrossRef]
- Bethel, J.W.; Harger, R. Heat-Related Illness among Oregon Farmworkers. Int. J. Environ. Res. Public Health 2014, 11, 9273–9285. [Google Scholar] [CrossRef]
- Hansen, A.; Saniotis, A.; Nitschke, M. Vulnerability to Extreme Heat and Climate Change: Is Ethnicity a Factor? Glob. Health Action 2013, 6, 21364. [Google Scholar] [CrossRef]
- Santha, S.D.; Jaswal, S.; Sasidevan, D.; Datta, K.; Khan, A.; Kuruvilla, A. Climate Change, Livelihoods and Health Inequities: The Vulnerability of Migrant Workers in Indian Cities. Available online: https://pubs.iied.org/10728iied (accessed on 21 December 2021).
- Jung, J.; Uejio, C.K.; Kintziger, K.W.; Duclos, C.; Reid, K.; Jordan, M.; Spector, J.T. Heat illness data strengthens vulnerability maps. BMC Public Health 2021, 21, 1999. [Google Scholar] [CrossRef]
- Equitable Growth. Temperature, Workplace Safety, and Labor Market Inequality. Available online: https://equitablegrowth.org/working-papers/temperature-workplace-safety-and-labor-market-inequality/ (accessed on 29 October 2021).
- Boiling Point—Public Citizen. Available online: https://www.citizen.org/article/boiling-point/ (accessed on 18 October 2022).
- Berube, A.; Tiffany, T. The “State” of Low-Wage Workers: How the EITC Benefits Urban and Rural Communities in the 50 States; EITC Series; The Brookings Institution: Washington, DC, USA, 2004. [Google Scholar]
- Tigchelaar, M.; Battisti, D.S.; Spector, J.T. Work adaptations insufficient to address growing heat risk for U.S. agricultural workers. Environ. Res. Lett. 2020, 15, 094035. [Google Scholar] [CrossRef]
- Jackson, L.L.; Rosenberg, H.R. Preventing heat-related illness among agricultural workers. J. Agromed. 2010, 15, 200–215. [Google Scholar] [CrossRef]
- Hagedorn, J.; Paras, C.A.; Greenwich, H.; Hagopian, A. The Role of Labor Unions in Creating Working Conditions That Promote Public Health. Am. J. Public Health 2016, 106, 989–995. [Google Scholar] [CrossRef]
- Dong, X.S.; West, G.H.; Holloway-Beth, A.; Wang, X.; Sokas, R.K. Heat-related deaths among construction workers in the United States. Am. J. Ind. Med. 2019, 62, 1047–1057. [Google Scholar] [CrossRef]
- Dutta, P.; Rajiva, A.; Andhare, D.; Azhar, G.S.; Tiwari, A.; Sheffield, P.; Ahmedabad Heat and Climate Study Group. Perceived heat stress and health effects on construction workers. Indian J. Occup. Environ. Med. 2015, 19, 151–158. [Google Scholar] [CrossRef]
- El-Shafei, D.A.; Bolbol, S.A.; Awad Allah, M.B.; Abdelsalam, A.E. Exertional heat illness: Knowledge and behavior among construction workers. Environ. Sci. Pollut. Res. 2018, 25, 32269–32276. [Google Scholar] [CrossRef]
- Altassan, K.A.; Sakr, C.J.; Galusha, D.; Slade, M.D.; Tessier-Sherman, B.; Cantley, L.F. Risk of Injury by Unionization: Survival Analysis of a Large Industrial Cohort. J. Occup. Environ. Med. 2018, 60, 827–831. [Google Scholar] [CrossRef]
- Unionized Workers Are More Likely to Assert Their Right to a Safe and Healthy Workplace. Available online: https://theconversation.com/unionized-workers-are-more-likely-to-assert-their-right-to-a-safe-and-healthy-workplace-144718 (accessed on 21 December 2021).
- Tsao, T.-Y.; Konty, K.J.; Van Wye, G.; Barbot, O.; Hadler, J.L.; Linos, N.; Bassett, M.T. Estimating Potential Reductions in Premature Mortality in New York City From Raising the Minimum Wage to $15. Am. J. Public Health 2016, 106, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.J. The Decline of American Unions Is a Threat to Public Health. Am. J. Public Health 2016, 106, 968–969. [Google Scholar] [CrossRef]
- Morrissey, M.C.; Brewer, G.J.; Williams, W.J.; Quinn, T.; Casa, D.J. Impact of occupational heat stress on worker productivity and economic cost. Am. J. Ind. Med. 2021, 64, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Axelson, O. Influence of heat exposure on productivity. Work Environ. Health 1974, 11, 94–99. [Google Scholar] [PubMed]
- Mitchell, R.J.; Bates, P. Measuring Health-Related Productivity Loss. Popul. Health Manag. 2011, 14, 93–98. [Google Scholar] [CrossRef]
- Ioannou, L.G.; Mantzios, K.; Tsoutsoubi, L.; Panagiotaki, Z.; Kapnia, A.; Ciuha, U.; Nybo, L.; Flouris, A.; Mekjavic, I. Effect of a Simulated Heat Wave on Physiological Strain and Labour Productivity. Int. J. Environ. Res. Public Health 2021, 18, 3011. [Google Scholar] [CrossRef]
- Injuries, Illnesses, and Fatalities. Available online: https://www.bls.gov/iif/home.htm (accessed on 16 October 2022).
- NIOSH; CDC. Data and Statistics—Traumatic Occupational Injuries. Available online: https://www.cdc.gov/niosh/injury/data.html (accessed on 16 October 2022).
- Schramm, P.J.; Vaidyanathan, A.; Radhakrishnan, L.; Gates, A.; Hartnett, K.; Breysse, P. Heat-Related Emergency Department Visits During the Northwestern Heat Wave—United States, June 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1020–1021. [Google Scholar] [CrossRef]
- Heal, G.; Park, J. Reflections—Temperature Stress and the Direct Impact of Climate Change: A Review of an Emerging Literature. Rev. Environ. Econ. Policy 2016, 10, 347–362. [Google Scholar] [CrossRef]
- Chen, X.; Li, N.; Liu, J.; Zhang, Z.; Liu, Y.; Huang, C. Changes in Global and Regional Characteristics of Heat Stress Waves in the 21st Century. Earths Future 2020, 8, e2020EF001636. [Google Scholar] [CrossRef]
- Perkins, S.E. A review on the scientific understanding of heatwaves—Their measurement, driving mechanisms, and changes at the global scale. Atmos. Res. 2015, 164–165, 242–267. [Google Scholar] [CrossRef]
- Djalante, R. Key assessments from the IPCC special report on global warming of 1.5 °C and the implications for the Sendai framework for disaster risk reduction. Prog. Disaster Sci. 2019, 1, 100001. [Google Scholar] [CrossRef]
- Mora, C.; Spirandelli, D.; Franklin, E.C.; Lynham, J.; Kantar, M.B.; Miles, W.; Smith, C.Z.; Freel, K.; Moy, J.; Louis, L.V.; et al. Broad threat to humanity from cumulative climate hazards intensified by greenhouse gas emissions. Nat. Clim. Chang. 2018, 8, 1062–1071. [Google Scholar] [CrossRef]
- Levin, K. Half a Degree and a World Apart: The Difference in Climate Impacts Between 1.5 °C and 2 °C of Warming. 2018. Available online: http://www.wri.org/insights/half-degree-and-world-apart-difference-climate-impacts-between-15c-and-2c-warming (accessed on 15 October 2022).



{kind=link}
{kind=link}
| Injuries | N | Percent of Overall | Percent of Exertion Injuries |
|---|---|---|---|
| Overall | 58,648 | 100% | - |
| Non-Exertion | 56,966 | 97.1% | - |
| Accidents * | 41,368 | 70.5% | - |
| Non-Accidents ** | 15,696 | 26.8% | - |
| Exertion *** | 1682 | 2.9% | 100% |
| Heat-related Injury | 1546 | 2.6% | 91.9% |
| Cardiac | 101 | 0.2% | 6.0% |
| Anaphylactic Shock | 18 | 0.03% | 1.07% |
| Cold-related Injury | 15 | 0.03% | 0.9% |
| Pulmonary Embolism | 1 | 0.002% | 0.06% |
| Anemia | 1 | 0.002% | 0.1% |
| Anemia | Cold-Related Injury | Cardiac | Pulmonary Embolism | Anaphylactic Shock | Heat-Related Injury | Total * | |
|---|---|---|---|---|---|---|---|
| Total | 1 | 15 | 101 | 1 | 18 | 1546 | 1682 |
| Average Yearly Injury Rate ** [95% CI] | 0.0001 [0.001, 0.005] | 0.002 [0.001, 0.003] | 0.012 [0.001, 0.003] | 0.0001 [0.001, 0.005] | 0.002 [0.001, 0.003] | 0.19 [0.18, 0.2] | 0.20 [0.19, 0.22] |
| US Region | |||||||
| Southeast | 0 | 4 | 15 | 0 | 4 | 615 | 638 |
| Southwest | 1 | 2 | 15 | 0 | 2 | 474 | 494 |
| Midwest | 0 | 4 | 25 | 1 | 5 | 241 | 276 |
| Northeast | 0 | 5 | 36 | 0 | 5 | 168 | 214 |
| West | 0 | 0 | 10 | 0 | 2 | 48 | 60 |
| Occupation | |||||||
| Construction and Extraction | 0 | 3 | 10 | 0 | 0 | 321 | 334 |
| Personal Care and Service | 1 | 2 | 8 | 0 | 1 | 275 | 287 |
| Production | 0 | 1 | 7 | 0 | 1 | 256 | 265 |
| Other | 0 | 3 | 22 | 0 | 0 | 250 | 275 |
| Installation, Maintenance, Repair | 0 | 0 | 11 | 0 | 0 | 155 | 166 |
| Transportation and Material Moving | 0 | 1 | 6 | 1 | 0 | 90 | 98 |
| Buildings and Grounds | 0 | 0 | 9 | 0 | 3 | 76 | 88 |
| Food Preparation and Serving | 0 | 3 | 4 | 0 | 1 | 37 | 45 |
| Farming, Fishing, Forestry | 0 | 0 | 0 | 0 | 0 | 41 | 41 |
| Healthcare | 0 | 1 | 15 | 0 | 11 | 11 | 38 |
| Protective Service | 0 | 0 | 6 | 0 | 1 | 20 | 27 |
| Tourism | 0 | 1 | 2 | 0 | 0 | 10 | 13 |
| Military | 0 | 0 | 1 | 0 | 0 | 4 | 5 |
| Fatalities | N | Percentage | Percentage of Exertion Fatalities |
|---|---|---|---|
| Overall | 4598 | 100% | - |
| Non-Exertion | 4509 | 98.1% | - |
| Accidents * | 2781 | 60.5% | - |
| Non-Accidents ** | 1728 | 37.5% | - |
| Exertion *** | 89 | 1.9% | 100% |
| Heat | 78 | 1.7% | 87.6% |
| Cardiac | 8 | 0.2% | 8.9% |
| Cold | 2 | 0.04% | 2.4% |
| Asthma | 1 | 0.02% | 1.1% |
| Heat | Cardiac | Cold | Asthma | Total * | |
|---|---|---|---|---|---|
| Total | 78 | 8 | 2 | 1 | 89 |
| Yearly Average Fatality Rate [95% CI] ** | 0.0144 [0.0077, 0.011] | 0.0014 [0.0004, 0.0019] | 0.0003 [0.00005, 0.0009] | 0.0001 [0.001, 0.005] | 0.0160 [0.008, 0.0134] |
| US Region | |||||
| Southeast | 26 | 2 | 0 | 0 | 28 |
| Southwest | 23 | 1 | 0 | 0 | 24 |
| Midwest | 13 | 0 | 1 | 1 | 15 |
| West | 11 | 3 | 1 | 0 | 15 |
| Northeast | 5 | 2 | 0 | 0 | 7 |
| Occupation | |||||
| Construction and Excavation | 24 | 0 | 0 | 0 | 24 |
| Farming, Fishing, Forestry | 15 | 2 | 0 | 0 | 17 |
| Personal Services | 9 | 1 | 0 | 0 | 10 |
| Production | 8 | 1 | 0 | 1 | 10 |
| Building and Grounds | 8 | 0 | 0 | 0 | 8 |
| Installation, Maintenance, Repair | 6 | 1 | 0 | 0 | 7 |
| Transportation and Material Moving | 4 | 1 | 0 | 0 | 5 |
| Other | 2 | 1 | 0 | 0 | 3 |
| Protective Services | 1 | 0 | 1 | 0 | 2 |
| Tourism | 1 | 0 | 1 | 0 | 2 |
| Health Care | 0 | 1 | 0 | 0 | 1 |
| Union Status | |||||
| Non-Unionized | 63 | 6 | 2 | 1 | 72 |
| Unionized | 15 | 2 | 0 | 0 | 17 |
| January | February | March | April | May | June | July | August | September | October | November | December | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reported Accident-Related Injuries | ||||||||||||
| 2015 | 610 | 509 | 583 | 565 | 523 | 579 | 588 | 589 | 591 | 578 | 526 | 529 |
| 2016 | 558 | 571 | 529 | 533 | 515 | 628 | 585 | 701 | 607 | 613 | 572 | 564 |
| 2017 | 594 | 592 | 637 | 578 | 609 | 655 | 662 | 663 | 590 | 680 | 573 | 600 |
| 2018 | 651 | 629 | 644 | 636 | 720 | 737 | 705 | 732 | 599 | 712 | 668 | 598 |
| 2019 | 721 | 652 | 681 | 632 | 634 | 594 | 701 | 645 | 663 | 692 | 601 | 590 |
| 2020 | 639 | 574 | 550 | 445 | 499 | 579 | 522 | 544 | - | - | - | - |
| Mean | 629 | 588 | 604 | 565 | 583 | 629 | 627 | 646 | 610 | 655 | 588 | 576 |
| Reported Accident-Related Fatalities | ||||||||||||
| 2017 | 62 | 49 | 52 | 56 | 69 | 63 | 44 | 70 | 62 | 78 | 57 | 54 |
| 2018 | 37 | 45 | 72 | 56 | 70 | 60 | 66 | 74 | 60 | 66 | 44 | 51 |
| 2019 | 46 | 44 | 63 | 78 | 59 | 76 | 77 | 138 | 65 | 59 | 67 | 49 |
| 2020 | 49 | 55 | 51 | 26 | 22 | 41 | 54 | 146 | 53 | 47 | 64 | 51 |
| Mean | 49 | 48 | 60 | 54 | 55 | 60 | 60 | 107 | 60 | 63 | 58 | 51 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morrissey, M.C.; Kerr, Z.Y.; Brewer, G.J.; Tishukaj, F.; Casa, D.J.; Stearns, R.L. Analysis of Exertion-Related Injuries and Fatalities in Laborers in the United States. Int. J. Environ. Res. Public Health 2023, 20, 2683. https://doi.org/10.3390/ijerph20032683
Morrissey MC, Kerr ZY, Brewer GJ, Tishukaj F, Casa DJ, Stearns RL. Analysis of Exertion-Related Injuries and Fatalities in Laborers in the United States. International Journal of Environmental Research and Public Health. 2023; 20(3):2683. https://doi.org/10.3390/ijerph20032683
Chicago/Turabian StyleMorrissey, Margaret C., Zachary Yukio Kerr, Gabrielle J. Brewer, Faton Tishukaj, Douglas J. Casa, and Rebecca L. Stearns. 2023. "Analysis of Exertion-Related Injuries and Fatalities in Laborers in the United States" International Journal of Environmental Research and Public Health 20, no. 3: 2683. https://doi.org/10.3390/ijerph20032683