
Self-Management of Subclinical Common Mental Health Disorders (Anxiety, Depression and Sleep Disorders) Using Wearable Devices


Abstract
:1. Introduction
Health Technology
2. Background
2.1. Defining Common Mental Health Disorders
2.2. The Promise of Telehealth and the Integration of Health Self-Service
3. Review Aims and Objectives
- Analyse the dominant wearable biometrics currently used in wearable devices as described within the current literature.
- Analyse the central purpose of wearable devices as described within the current literature.
- Understand the major machine learning algorithms deployed within these devices.
- Analyse the potential cost-benefit wearable devices have.
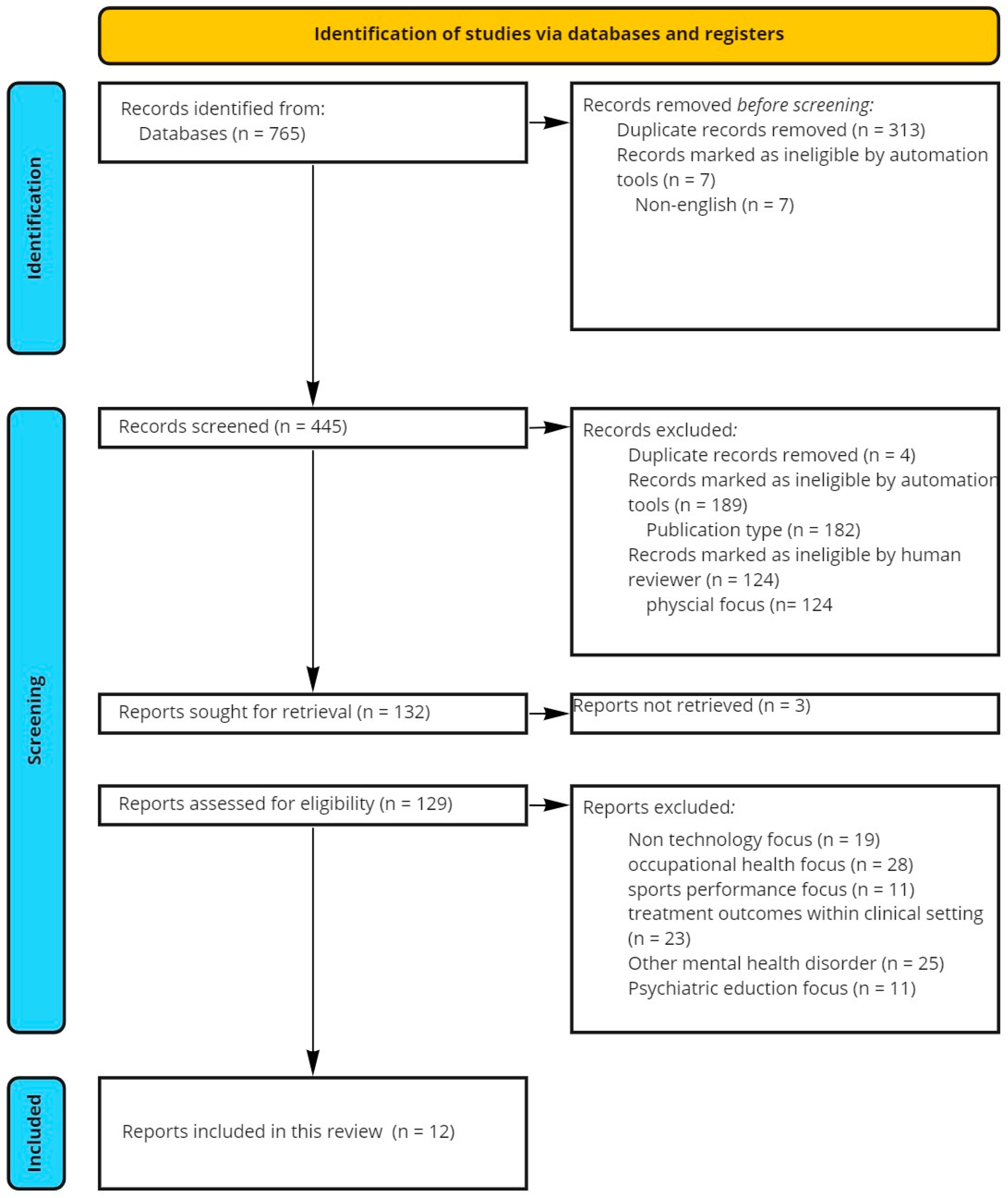
4. Methodology
4.1. Information Sources
4.2. Selection Process
- Included results within the date range 2018–2022. A five-year search window was chosen due to the exponential growth in wearable technology, the speed of technological development, and to capture the influence of COVID-19 in the results.
- Included results were common mental disorders (anxiety or depressive disorder, sleeping disorder) as they were the primary focus.
- Results describe or evaluate e-mental health or wearable technology.
- Returned results outside of 2018–2022.
- Exclude articles with a low number of participants .
- Exclude articles focused on professional practice and the well-being of healthcare workers within the clinical setting or directly related to occupational stress.
- Exclude articles focused on professional performance enhancement within sport.
- Language exclusions: only include English language results.
- Excluded results did not focus on common mental health conditions (anxiety or depression) as the primary focal point i.e., excluded those that considered mental health a secondary factor to patient care.
- Excluded studies focused on the clinical outcomes of sensing as part of treatment.
- Excluded results related to the improvement of psychiatric education practice.
4.3. Data Collection and Analysis
5. Results
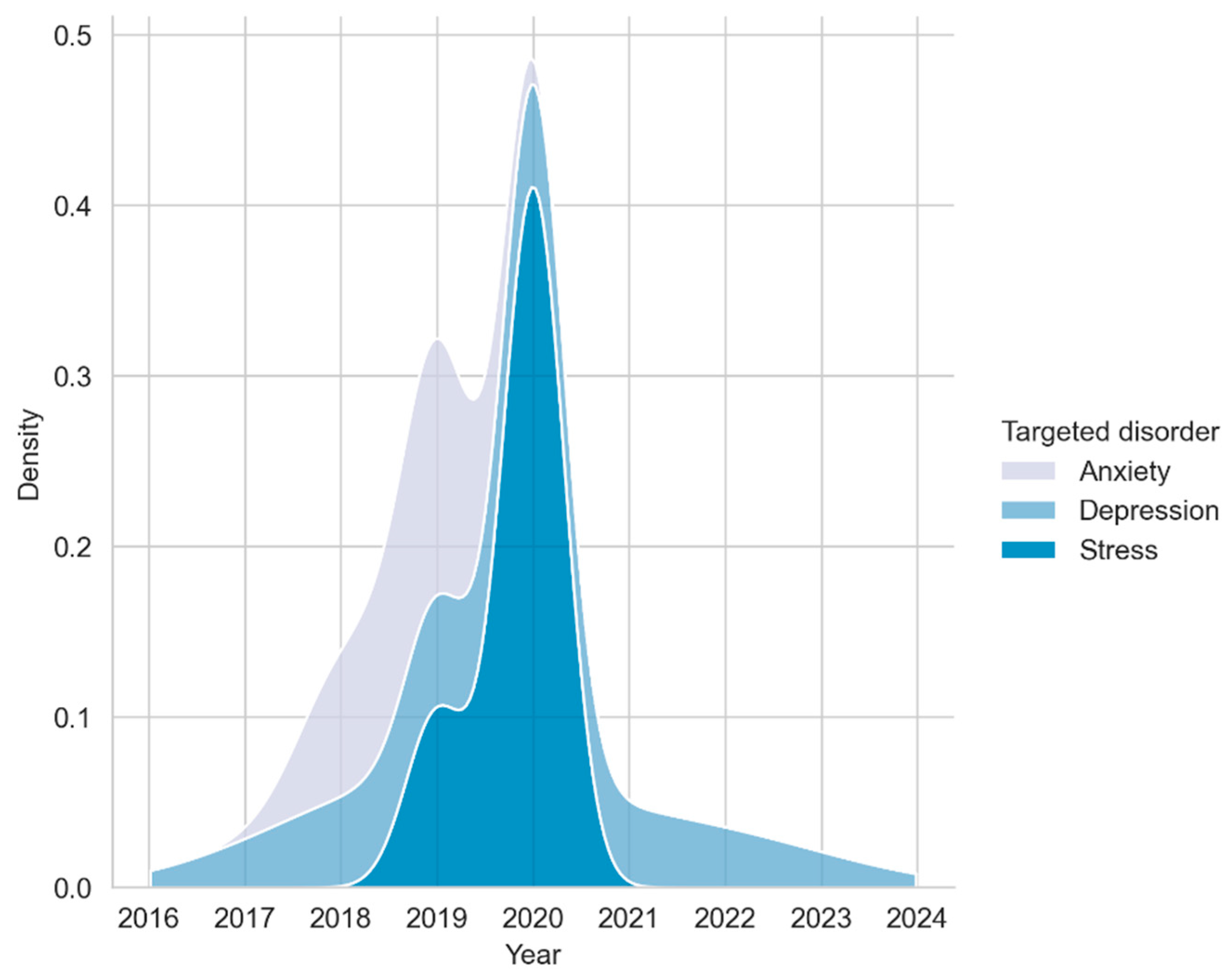
5.1. Study Characteristics
Methodological Quality

{kind=link}
{kind=link}
{kind=link}
| Study | Demographic | Mental Health Disorder | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Sample Size | Participants (Male %) | Participants (Female %) | Participants Age Range | Participant’s Age (Mean) | Target Group | Targeted Disorder | Intended Purpose | Passive Sensing | Intervention |
| [27] | 55 | 0.69 | 0.31 | 18–25 | 23.2 | Young Adults | Anxiety | Well-being (Biofeedback) | N | Y |
| [28] | 55 | 0.88 | 0.12 | 33–59 | 46.5 | Adults | Depression | Detection | Y | N |
| [29] | 183 | 33–59 | Adults | Stress | Self-Monitoring | Y | N | |||
| [30] | 23 | 0.7 | 0.3 | 22–56 | 30.35 | Employees | Stress | Validation | Y | N |
| [31] | 20 | 33–59 | University Students | Depression | Self-Monitoring | Y | N | |||
| [32] | 201 | 0.55 | 0.45 | 18–25 | University Students | Stress, Depression, Anxiety | Self-Monitoring | Y | N | |
| [33] | 82 | 0.35 | 0.65 | 17–38 | University Students | Stress | Self-Monitoring | Y | N | |
| [34] | 169 | 0.45 | 0.55 | 33–59 | 33 | Employees | Stress | Well-being (Biofeedback) | Y | Y |
| [35] | 328 | 0.57 | 0.43 | 33–59 | 38.9 | Employees | Stress | Self-Monitoring | Y | N |
| [36] | 5895 | Depression | Self-Monitoring | Y | N | |||||
| [37] | 80 | 0.50 | 0.50 | 50–70 | Older Adults | Depression | Self-Monitoring | N | N | |
| [38] | 196 | 0.33 | 0.77 | 28.8–48.4 | Employees | Anxiety | Self-Monitoring | Y | N | |
5.2. Wearable Devices and Device Types
5.3. Wearable Device Data Type
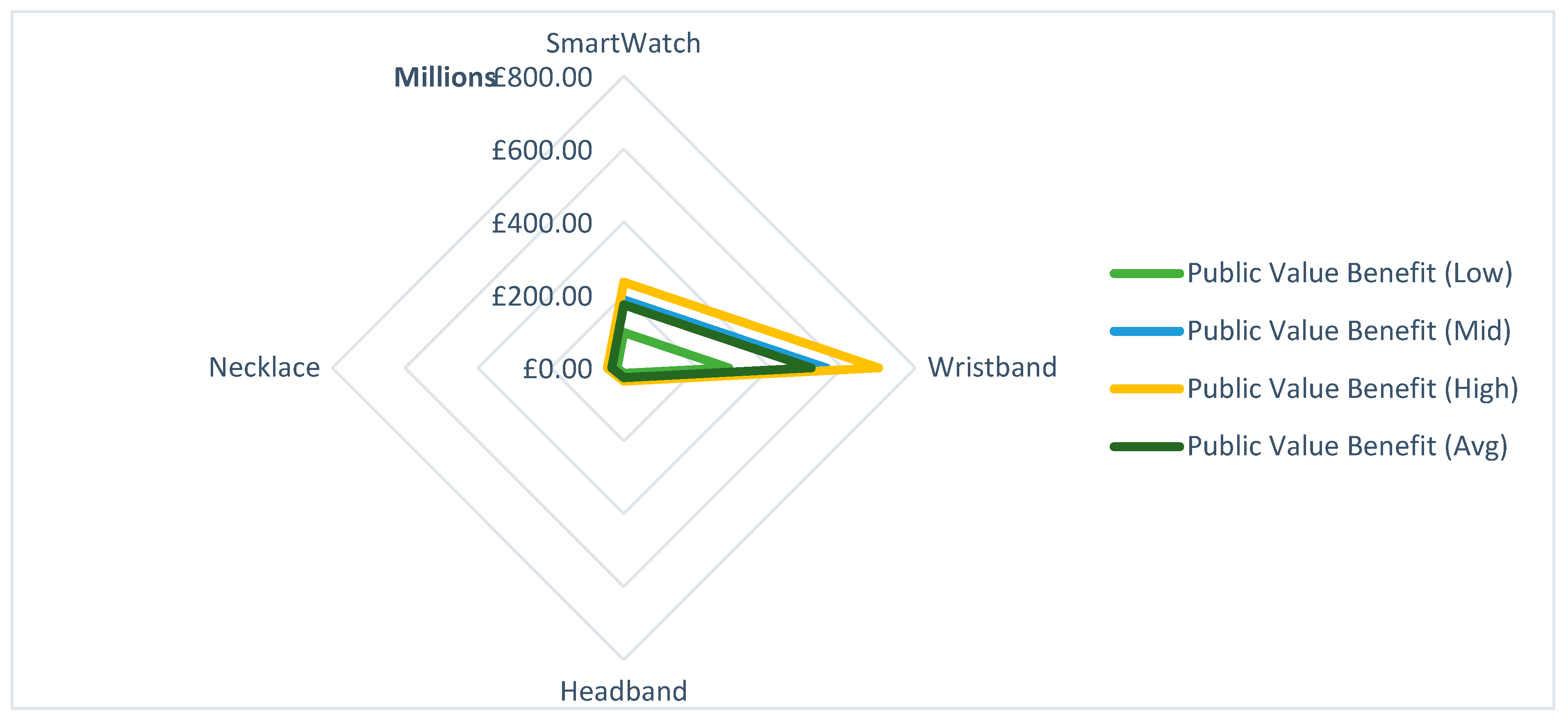
5.4. Economic Analysis of Technologies
5.4.1. Domains
5.4.2. Assumptions
5.4.3. Public Value Benefit
6. Discussion
6.1. Opportunities
6.1.1. Wearables as a Data Collection Platform
6.1.2. Widening Access to Treatments through Wearables
6.1.3. Empowering the Therapeutic Process
6.2. Limitations
6.2.1. The True Economic Case for Wearables
6.2.2. Lack of Evidence Base
6.2.3. Empowering the Already Empowered
6.2.4. Limitations of This Review
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Fusar-Poli, P.; Correll, C.U.; Arango, C.; Berk, M.; Patel, V.; Ioannidis, J.P. Preventive psychiatry: A blueprint for improving the mental health of young people. World Psychiatry 2021, 20, 200–221. [Google Scholar] [CrossRef] [PubMed]
- McDaid, D.; Park, A.-L.; Wahlbeck, K. The Economic Case for the Prevention of Mental Illness. Annu. Rev. Publ. Health 2019, 40, 373–389. [Google Scholar] [CrossRef]
- Schofield, D.J.; Shrestha, R.N.; Percival, R.; E Passey, M.; Callander, E.J.; Kelly, S.J. The personal and national costs of mental health conditions: Impacts on income, taxes, government support payments due to lost labour force participation. Bmc Psychiatry 2011, 11, 72. [Google Scholar] [CrossRef]
- Knapp, J.C.M. The economic case for improved coverage of public mental health interventions. Lancet Psychiatry 2018, 5, 103–105. [Google Scholar]
- Punton, G.; Dodd, A.L.; McNeill, A. ‘You’re on the waiting list’: An interpretive phenomenological analysis of young adults’ experiences of waiting lists within mental health services in the UK. PLoS ONE 2022, 17, e0265542. [Google Scholar] [CrossRef] [PubMed]
- Marvaldi, M.; Mallet, J.; Dubertret, C.; Moro, M.R.; Guessoum, S.B. Anxiety, depression, trauma-related, and sleep disorders among healthcare workers duirng the COVID-19 pandemic: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2021, 126, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Turkington, R.; Mulvenna, M.; Bond, R.; Ennis, E.; Potts, C.; Moore, C.; Hamra, L.; Morrissey, J.; Isaksen, M.; Scowcroft, E.; et al. Behavior of Callers to a Crisis Helpline Before and During the COVID-19 Pandemic: Quantitative Data Analysis. JMIR Ment. Health 2020, 7, e22984. [Google Scholar] [CrossRef]
- Solmi, M.; Radua, J.; Olivola, M.; Croce, E.; Soardo, L.; de Pablo, G.S.; Shin, J.I.; Kirkbride, J.B.; Jones, P.; Kim, J.H.; et al. Age at onset of mental disorders worldwide: Large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatr. 2022, 27, 281–295. [Google Scholar] [CrossRef]
- Liese, B.H.; Gribble RS, F.; Wickremsinhe, M.N. International funding for mental health: A review of the last decade. Int. Health 2019, 11, 361–369. [Google Scholar] [CrossRef]
- Firth, J.; Torous, J.; Carney, R.; Newby, J.; Cosco, T.D.; Christensen, H.; Sarris, J. Digital Technologies in the Treatment of Anxiety: Recent Innovations and Future Directions. Curr. Psychiatry Rep. 2018, 20, 44. [Google Scholar] [CrossRef]
- Naslund, J.A.; Gonsalves, P.P.; Gruebner, O.; Pendse, S.R.; Smith, S.L.; Sharma, A.; Raviola, G. Digital Innovations for Global Mental Health: Opportunities for Data Science, Task Sharing, and Early Intervention. Curr. Treat. Options Psychiatry 2019, 6, 337–351. [Google Scholar] [CrossRef]
- Huckvale, K.; Nicholas, J.; Torous, J.; Larsen, M.E. Smartphone apps for the treatment of mental health conditions: Status and considerations. Curr. Opin. Psychol. 2020, 36, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Onyeaka, H.; Firth, J.; Kessler, R.C.; Lovell, K.; Torous, J. Use of smartphones, mobile apps and wearables for health promotion by people with anxiety or depression: An analysis of a nationally representative survey data. Psychiatry Res. 2021, 304, 114120. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. ICD-11: International Classification of Diseases (11th Revision). 2019. Available online: https://icd.who.int/ (accessed on 11 October 2022).
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. 2017. Available online: https://apps.who.int/iris/handle/10665/254610 (accessed on 11 October 2022).
- World Health Organization. Technical Meeting on Sleep and Health. 2004. Available online: https://www.euro.who.int/__data/assets/pdf_file/0008/114101/E84683.pdf (accessed on 11 October 2022).
- Haller, H.; Cramer, H.; Lauche, R.; Gass, F.; Dobos, G.J. The prevalence and burden of subthreshold generalized anxiety disorder: A systematic review. BMC Psychiatry 2014, 14, 128. [Google Scholar] [CrossRef] [PubMed]
- Baxter, A.J.; Scott, K.M.; Vos, T.; Whiteford, H.A. Global prevalence of anxiety disorders: A systematic review and meta-regression. Psychol. Med. 2013, 43, 897–910. [Google Scholar] [CrossRef]
- Kola, L.; Kohrt, B.A.; Hanlon, C.; Naslund, J.A.; Sikander, S.; Balaji, M.; Benjet, C.; Cheung, E.Y.L.; Eaton, J.; Gonsalves, P.; et al. COVID-19 mental health impact and responses in low-income and middle-income countries: Reimagining global mental health. Lancet Psychiatry 2021, 8, 535–550. [Google Scholar] [CrossRef]
- Deng, J.; Zhou, F.; Hou, W.; Silver, Z.; Wong, C.Y.; Chang, O.; Drakos, A.; Zuo, Q.K.; Huang, E. The prevalence of depressive symptoms, anxiety symptoms and sleep disturbance in higher education students during the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2021, 301, 113863. [Google Scholar] [CrossRef]
- Bhugra, D.; Tasman, A.; Pathare, S.; Priebe, S.; Smith, S.; Torous, J.; Arbuckle, M.R.; Langford, A.; Alarcón, R.D.; Chiu, H.F.K.; et al. The WPA-Lancet Psychiatry Commission on the Future of Psychiatry. Lancet Psychiatry 2017, 4, 775–818. [Google Scholar] [CrossRef]
- Piwek, L.; Ellis, D.A.; Andrews, S.; Joinson, A. The Rise of Consumer Health Wearables: Promises and Barriers. PLOS Med. 2016, 13, e1001953. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- GMCA. Greater Manchester CBA Model; GMCA: Metropolitan County, UK, 2019. [Google Scholar]
- Riva, F.; Triscoli, C.; Lamm, C.; Carnaghi, A.; Silani, G. Emotional Egocentricity Bias Across the Life-Span. Front. Aging Neurosci. 2016, 8, 74. [Google Scholar] [CrossRef]
- Balconi, M.; Fronda, G.; Crivelli, D. Effects of technology-mediated mindfulness practice on stress: Psychophysiological and self-report measures. Stress 2018, 22, 200–209. [Google Scholar] [CrossRef]
- Cao, Z.; Lin, C.-T.; Ding, W.; Chen, M.-H.; Li, C.-T.; Su, T.-P. Identifying Ketamine Responses in Treatment-Resistant Depression Using a Wearable Forehead EEG. IEEE Trans. Biomed. Eng. 2018, 66, 1668–1679. [Google Scholar] [CrossRef]
- Kim, J.; Park, J.; Park, J. Development of a statistical model to classify driving stress levels using galvanic skin responses. Hum. Factor Ergon. Man 2020, 30, 321–328. [Google Scholar] [CrossRef]
- Lucas, B.; Grayson, S.; Hamidu, H.; Han, A.; No, S.; Varghese, A.; Campisi, J. Sex differences in heart rate responses to occupational stress. Stress 2019, 23, 13–18. [Google Scholar] [CrossRef]
- Narziev, N.; Goh, H.; Toshnazarov, K.; Lee, S.A.; Chung, K.-M.; Noh, Y. STDD: Short-Term Depression Detection with Passive Sensing. Sensors 2020, 20, 1396. [Google Scholar] [CrossRef] [PubMed]
- Sano, A.; Taylor, S.; McHill, A.W.; Phillips, A.J.; Barger, L.K.; Klerman, E.; Picard, R. Identifying Objective Physiological Markers and Modifiable Behaviors for Self-Reported Stress and Mental Health Status Using Wearable Sensors and Mobile Phones: Observational Study. J. Med. Internet Res. 2018, 20, e210. [Google Scholar] [CrossRef]
- Silva, E.; Aguiar, J.; Reis, L.P.; Sá, J.O.; Gonçalves, J.; Carvalho, V. Stress among Portuguese Medical Students: The EuStress Solution. J. Med. Syst. 2020, 44, 45. [Google Scholar] [CrossRef]
- Smith, E.N.; Santoro, E.; Moraveji, N.; Susi, M.; Crum, A.J. Integrating Wearables in Stress Management Interventions: Promising Evidence From a Randomized Trial. Int. J. Stress Manag. 2019, 27, 172–182. [Google Scholar] [CrossRef]
- Kraaij, A.W.J.; van Schiavone, G.; Lutin, E.; Claes, S.; Hoof, C.V. Relationship Between Chronic Stress and Heart Rate Over Time Modulated by Gender in a Cohort of Office Workers: Cross-Sectional Study Using Wearable Technologies. J. Med. Internet Res. 2020, 22, e18253. [Google Scholar] [CrossRef]
- Zanella-Calzada, L.A.; Galván-Tejada, C.E.; Chávez-Lamas, N.M.; Gracia-Cortés, M.D.C.; Magallanes-Quintanar, R.; Celaya-Padilla, J.M.; Galván-Tejada, J.I.; Gamboa-Rosales, H. Feature Extraction in Motor Activity Signal: Towards a Depression Episodes Detection in Unipolar and Bipolar Patients. Diagnostics 2019, 9, 8. [Google Scholar] [CrossRef]
- Chattopadhyay, S.; Das, R. Statistical Validation of LENS: Towards Understanding the Empty Nest Syndrome in India using Lyfas, an Optical Biomarker-based Smartphone Biomedical Tool. Research Square 2022. [Google Scholar] [CrossRef]
- Tiwari, A.; Cassani, R.; Narayanan, S.; Falk, T.H. A Comparative Study of Stress and Anxiety Estimation in Ecological Settings Using a Smart-shirt and a Smart-bracelet. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 2213–2216. [Google Scholar]
- Koldijk, S.; Neerincx, M.A.; Kraaij, W. Detecting Work Stress in Offices by Combining Unobtrusive Sensors. IEEE Trans. Affect. Comput. 2016, 9, 227–239. [Google Scholar] [CrossRef]
- Engelniederhammer, A.; Papastefanou, G.; Xiang, L. Crowding density in urban environment and its effects on emotional responding of pedestrians: Using wearable device technology with sensors capturing proximity and psychophysiological emotion responses while walking in the street. J. Hum. Behav. Soc. Environ. 2019, 29, 630–646. [Google Scholar] [CrossRef]
- Hickey, B.A.; Chalmers, T.; Newton, P.; Lin, C.-T.; Sibbritt, D.; McLachlan, C.; Clifton-Bligh, R.; Morley, J.; Lal, S. Smart Devices and Wearable Technologies to Detect and Monitor Mental Health Conditions and Stress: A Systematic Review. Sensors 2021, 21, 3461. [Google Scholar] [CrossRef]
- Kang, M.; Chai, K. Wearable Sensing Systems for Monitoring Mental Health. Sensors 2022, 22, 994. [Google Scholar] [CrossRef]
- Sakamaki, T.; Furusawa, Y.; Hayashi, A.; Otsuka, M.; Fernandez, J. Remote Patient Monitoring for Neuropsychiatric Disorders: A Scoping Review of Current Trends and Future Perspectives from Recent Publications and Upcoming Clinical Trials. Telemed E-health 2022, 28, 1235–1250. [Google Scholar] [CrossRef]
- Sahu, K.S.; Majowicz, S.E.; Dubin, J.A.; Morita, P.P. NextGen Public Health Surveillance and the Internet of Things (IoT). Front. Public Health 2021, 9, 756675. [Google Scholar] [CrossRef]
- Nahavandi, D.; Alizadehsani, R.; Khosravi, A.; Acharya, U.R. Application of artificial intelligence in wearable devices: Opportunities and Challenges. Comput. Meth. Prog. Bio. 2021, 213, 106541. [Google Scholar] [CrossRef] [PubMed]
- Long, N.; Lei, Y.; Peng, L.; Xu, P.; Mao, P. A scoping review on monitoring mental health using smart wearable devices. Math. Biosci. Eng. 2022, 19, 7899–7919. [Google Scholar] [CrossRef]
- Olmedo-Aguirre, J.O.; Reyes-Campos, J.; Alor-Hernández, G.; Machorro-Cano, I.; Rodríguez-Mazahua, L.; Sánchez-Cervantes, J.L. Remote Healthcare for Elderly People Using Wearables: A Review. Biosensors 2022, 12, 73. [Google Scholar] [CrossRef]
- Dewa, L.H.; Lavelle, M.; Pickles, K.; Kalorkoti, C.; Jaques, J.; Pappa, S.; Aylin, P. Young adults’ perceptions of using wearables, social media and other technologies to detect worsening mental health: A qualitative study. PLoS ONE 2019, 14, e0222655. [Google Scholar] [CrossRef] [PubMed]
- Dreisbach, C.; Koleck, T.A.; Bourne, P.E.; Bakken, S. A systematic review of natural language processing and text mining of symptoms from electronic patient-authored text data. Int. J. Med. Inform. 2019, 125, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Muharam, R.; Agiananda, F.; Budiman, Y.F.; Harahap, J.S.; Prabowo, K.A.; Azyati, M.; Putri, Y.I.; Pratama, G.; Sumapraja, K. Menstrual cycle changes and mental health states of women hospitalized due to COVID-19. PLoS ONE 2022, 17, e0270658. [Google Scholar] [CrossRef]
- Elgendi, M.; Menon, C. Assessing Anxiety Disorders Using Wearable Devices: Challenges and Future Directions. Brain Sci. 2019, 9, 50. [Google Scholar] [CrossRef]
- Ajakwe, S.O.; Nwakanma, C.I.; Kim, D.-S.; Lee, J.-M. Key Wearable Device Technologies Parameters for Innovative Healthcare Delivery in B5G Network: A Review. IEEE Access 2022, 10, 49956–49974. [Google Scholar] [CrossRef]
- Li, J.; Silvera-Tawil, D.; Varnfield, M.; Hussain, M.S.; Math, V. Users’ Perceptions Toward mHealth Technologies for Health and Well-being Monitoring in Pregnancy Care: Qualitative Interview Study. JMIR Form. Res. 2021, 5, e28628. [Google Scholar] [CrossRef]
- Pears, M.; Kola-Palmer, S.; Azevedo, L.B.D. The Impact of Sitting Time and Physical Activity on Mental Health during COVID-19 Lockdown. Sport Sci. Health 2022, 18, 179–191. [Google Scholar] [CrossRef]
- Corvo, L.; Pastore, L.; Mastrodascio, M.; Cepiku, D. The social return on investment model: A systematic literature review. Meditari Account. Res. 2022, 30, 49–86. [Google Scholar] [CrossRef]
- Population Estimates—Office for National Statistics. Census. 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates (accessed on 14 September 2022).
- HESA. Higher Education Student Statistics: UK, 2020/21. 2022. Available online: https://www.hesa.ac.uk/news/25-01-2022/sb262-higher-education-student-statistics (accessed on 14 September 2022).
- NatCen. Mental Health of Children and Young People Survey. 2021. Available online: https://natcen.ac.uk/our-research/research/mental-health-of-children-and-young-people-survey/ (accessed on 16 September 2022).
- Cheng, C.; Ebrahimi, O.V.; Lau, Y. Maladaptive coping with the infodemic and sleep disturbance in the COVID-19 pandemic. J. Sleep Res. 2021, 30, e13235. [Google Scholar] [CrossRef]
- NICE. Generalized Anxiety Disorder: How Common Is It? 2022. Available online: https://cks.nice.org.uk/topics/generalized-anxiety-disorder/background-information/prevalence/ (accessed on 17 September 2022).
- Miner, B.; Kryger, M.H. Sleep in the Aging Population. Sleep Med. Clin. 2017, 12, 31–38. [Google Scholar] [CrossRef]
- Age, U.K. Later Life in the United Kingdom. 2019. Available online: https://www.ageuk.org.uk/globalassets/age-uk/documents/reports-and-publications/later_life_uk_factsheet.pdf (accessed on 17 September 2022).
- Jenkins, P.E.; Ducker, I.; Gooding, R.; James, M.; Rutter-Eley, E. Anxiety and depression in a sample of UK college students: A study of prevalence, comorbidity, and quality of life. J. Am. Coll. Health 2020, 69, 813–819. [Google Scholar] [CrossRef]
- Beukenhorst, A.L.; Howells, K.; Cook, L.; McBeth, J.; O’Neill, T.W.; Parkes, M.J.; Sanders, C.; Sergeant, J.C.; Weihrich, K.S.; Dixon, W.G. Engagement and Participant Experiences with Consumer Smartwatches for Health Research: Longitudinal, Observational Feasibility Study. JMIR mHealth uHealth 2020, 8, e14368. [Google Scholar] [CrossRef]
- Mintel. UK Wearable Technology Market Report 2021. 2021. Available online: https://store.mintel.com/report/uk-wearable-technology-market-report (accessed on 6 September 2022).
- Chandrasekaran, R.; Katthula, V.; Moustakas, E. Patterns of Use and Key Predictors for the Use of Wearable Health Care Devices by US Adults: Insights from a National Survey. J. Med. Internet Res. 2020, 22, e22443. [Google Scholar] [CrossRef]
- Millings, A.; Morris, J.; Rowe, A.; Easton, S.; Martin, J.K.; Majoe, D.; Mohr, C. Can the effectiveness of an online stress management program be augmented by wearable sensor technology? Internet Interv. 2015, 2, 330–339. [Google Scholar] [CrossRef]
- Gal, R.; May, A.M.; Overmeeren EJ van Simons, M.; Monninkhof, E.M. The Effect of Physical Activity Interventions Comprising Wearables and Smartphone Applications on Physical Activity: A Systematic Review and Meta-analysis. Sport. Med.-Open 2018, 4, 42. [Google Scholar] [CrossRef]
- Banke-Thomas, A.O.; Madaj, B.; Charles, A.; van den Broek, N. Social Return on Investment (SROI) methodology to account for value for money of public health interventions: A systematic review. BMC Public Health 2015, 15, 582. [Google Scholar] [CrossRef]
- Sadeh-Sharvit, S.; Hollon, S.D. Leveraging the Power of Nondisruptive Technologies to Optimize Mental Health Treatment: Case Study. JMIR Ment. Health 2020, 7, e20646. [Google Scholar] [CrossRef]
- Hunkin, H.; King, D.L.; Zajac, I.T. Wearable devices as adjuncts in the treatment of anxiety-related symptoms: A narrative review of five device modalities and implications for clinical practice. Clin. Psychol. Sci. Pract. 2019, 26, e12290. [Google Scholar] [CrossRef]
- Mitchell, L.M.; Joshi, U.; Patel, V.; Lu, C.; Naslund, J.A. Economic Evaluations of Internet-Based Psychological Interventions for Anxiety Disorders and Depression: A Systematic Review. J. Affect. Disord. 2021, 284, 157–182. [Google Scholar] [CrossRef]
- OFCOM. Adults’ Media Use and Attitudes Report 2020/21; OFCOM: London, UK, 2021. [Google Scholar]
- Iribarren, S.J.; Cato, K.; Falzon, L.; Stone, P.W. What is the economic evidence for mHealth? A systematic review of economic evaluations of mHealth solutions. PLoS ONE 2017, 12, e0170581. [Google Scholar] [CrossRef]
- Newbold, A.; Warren, F.C.; Taylor, R.S.; Hulme, C.; Burnett, S.; Aas, B.; Botella, C.; Burkhardt, F.; Ehring, T.; Fontaine, J.R.J.; et al. Promotion of mental health in young adults via mobile phone app: Study protocol of the ECoWeB (emotional competence for well-being in Young adults) cohort multiple randomised trials. BMC Psychiatry 2020, 20, 458. [Google Scholar] [CrossRef] [PubMed]
- Thornicroft, G.; Rose, D.; Kassam, A.; Sartorius, N. Stigma: Ignorance, prejudice or discrimination? Brit. J. Psychiatry 2007, 190, 192–193. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A.F.; Patten, S.B.; Brugha, T.S.; Mojtabai, R. Has increased provision of treatment reduced the prevalence of common mental disorders? Review of the evidence from four countries. World Psychiatry 2017, 16, 90–99. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Campion, J.; Javed, A.; Sartorius, N.; Marmot, M. Addressing the public mental health challenge of COVID-19. Lancet Psychiatry 2020, 7, 657–659. [Google Scholar] [CrossRef]
- Maulik, P.K.; Thornicroft, G.; Saxena, S. Roadmap to strengthen global mental health systems to tackle the impact of the COVID-19 pandemic. Int. J. Ment. Health Syst. 2020, 14, 57. [Google Scholar] [CrossRef]



| Term | Google Scholar | Web of Science | Scopus | PubMed | Cochrane Library | PsycINFO | Total |
|---|---|---|---|---|---|---|---|
| Review AND (Anxiety OR depression) | 3,110,000 | 105,939 | 156,452 | 95,590 | 6716 | 52,223 | 3,526,920 |
| (“sleep disorders” OR (Common mental health disorders)) | 3,150,000 | 60,990 | 104,776 | 50,117 | 10,706 | 46,173 | 3,422,762 |
| (“self-management” OR “self-care”) | 17,900 | 52,266 | 89,471 | 64,278 | 0 | 30,781 | 254,696 |
| (“subclinical” OR “home management”) | 18,100 | 4661 | 5402 | 3858 | 599 | 1095 | 33,715 |
| (Wearables OR “wearable devices” OR “Smart Devices” OR “measurement device” OR “monitoring device” OR “smart wearables”) | 157,000 | 24,508 | 115,854 | 25,605 | 3469 | 1225 | 327,661 |
| (Remote OR sensor OR “sensing device”) | 7,160,000 | 1,509,175 | 1,877,800 | 301,094 | 12,259 | 19,868 | 10,880,196 |
| Abbreviation | Measurement Scale Full Name | Record Count |
|---|---|---|
| HAM-D | Hamilton depression rating scale | 2 |
| BDI (BDI-II) | Beck Depression Inventory (I, II) | 1 |
| BSI | Brief Symptom Inventory | 1 |
| STAI | State-Trait Anxiety Inventory | 3 |
| PSS | Perceived Stress Scale—PSS | 4 |
| POMS | Profile of mood states | 1 |
| PHQ-9 | Patient Health Questionnaire-9 | 1 |
| EMA | Ecological Momentary Assessment | 1 |
| MASQ | Mood and Anxiety Symptoms Questionnaire | 1 |
| MADRS | Montgomery–Åsberg Depression Rating Scale | 1 |
| SRI | Stress Response Inventory | 1 |
| CDC HRQOL-14 | Centre for Disease Control’s Healthy Days Core and Symptoms Modules | 1 |
| Wearable Device | Algorithm | |||||||
|---|---|---|---|---|---|---|---|---|
| Manufacturer | Wearable Model | Device Type | ML Model(s) | Accuracy | Biometric Signals | Self-Reporting Scales | Evaluation Scales | Reference |
| InteraXon Inc & SmithOptics Inc. | Muse™, Lowdown Focus | Headband, Glasses | 0.77 | EEG, HRV | PSS, POMS, STAI | BDI, BSI | [27] | |
| Eee Holter Technology Co. | Mindo-4S Jellyfish | Headband | SVM RBF | 0.81 | EEG | HAM-D | [28] | |
| Empatica | E4 | Wristband | Binary logistic regression model | 0.85 | GSR | [29] | ||
| Apple | Watch 6 | SmartWatch | HR | [30] | ||||
| Samsung | Gear S3 Frontier | SmartWatch | SVM RF | 0.96 | Physical Activity, HR | EMA, PHQ-9 | BDI-II, STAI | [31] |
| Affectiva | Q-sensor | SmartWatch | SVM RBF | 0.87 | Physical Activity, SC, S-Temp, Ambient light | PSS | [32] | |
| Microsoft | Smartband 2 | SmartWatch | Neural Network (NN) | 0.78 | SC, Sleep, Calorie intake, S-Temp, HR, HRV, PPG, RR | STAI | PSS, SRI | [33] |
| Spire Health | Spire Stone | Necklace | - | - | Respiratory Rate | MASQ | CDC HRQOL-14 | [34] |
| Intelligent Galaxy | Chillband | SmartWatch | Statistical mixed design model | 0.75 | Physical Activity, ECG, SC, S-Temp, HR, Circadian Harmonic | PSS | [35] | |
| Cambridge Neurotechnology Ltd. | Actiwatch | SmartWatch | Feature extraction and RF | 0.89 | Physical Activity | MADRS | [36] | |
| Acculi Labs Pvt. Ltd. | LENS | Bracelet | - | 0.93 | Physical Activity, S-Temp, menstrual cycle, Sp02, Sleep monitoring, PPG | HAM-D | [37] | |
| FitBit, OMsignal | OMsignal smart-shirt, Fitbit Charge 2 | SmartWatch, Smart Shirt | SVM RBF | 0.92 | Physical Activity, HR, HRV, Sleep, ECG, PPG, RR, GSR | daily survey | [38] | |
| Biometric | Collection | Count | Location | Description | Reference |
|---|---|---|---|---|---|
| Physical activity | Auto/Self-reported | 6 | On person | Physical activity is a commonly used metric default in many consumer wearable devices, which includes acceleration and step counts. | [2,14,43] |
| Electrodermal activity (EDA/GSR/SC/Skin Temperature) | Auto | 9 | Wrist | Electrodermal activity (EDA), galvanic skin response (GSR) and skin temperature are measures of skin conductance indicative of sweat gland activity and, therefore, emotional arousal. | [39,40,41,42] |
| Blood oxygen saturation (Sp02) | Auto | 1 | Wrist | Blood oxygen saturation (SP02) is a common biometric within clinical practice and is typically collected via pulse oximetry, reflecting the percentage of oxygen in the blood. | [44,45,46,47] |
| Heart Rate (HR) | Auto | 6 | Wrist | Heart Rate is the number of heart beats per minute | [41,47] |
| Heart Rate Variability (HRV) | Auto | 3 | Wrist | Heart rate variability (HRV) is a variation of the interval between heartbeats. | [41,47] |
| Sleep | Auto/Self-reported | 3 | Wrist | Changes in sleep patterns are commonly associated with signs of mental health deterioration. Therefore, sleep patterns are regular indicators of mental health status. | [43,48,49] |
| Ambient light and audio | Auto | 1 | Wrist | Ambient light or audio is a commonly used metric in conjunction with physical activity and SC to determine sleep activity and quality. | [31,43] |
| Menstrual cycle | Self-reported | 1 | Off person | Psychological stress has a detrimental effect on menstrual cycle regularity. | [50] |
| Photoplethysmography (PPG) | Auto | 3 | Wrist | Commonly used metric to determine the amount of light absorbed by blood vessels in living tissue. PPG can be used as a proxy for blood pressure due to the correlation between arterial blood volume and distention with blood pressure. | [47,51,52] |
| Electrocardiogram (ECG) | Auto | 2 | Wrist | A plot of the heart’s electrical activity is traditionally used to calculate HR and HRV | [46] |
| Electroencephalography (EEG) | Auto | 2 | Head | Electroencephalography (EEG) is a measure of the brains electrical activity over time and is one of the most effective physiological signals for identification of psychological stress. | [41,46] |
| Respiratory Rate | Auto | 2 | Chest | Respiratory patterns, i.e., inspiration/expiration ratio, respiratory pauses, irregularity etc. are influenced by various mental stressors and therefore is a common indicator of mental state. | [42] |
| Calorie intake | Self-reported | 1 | Off person | Calorie intake indicators are typically self-reported and are of interest because food intake is shown to be correlated with depressive symptoms | [31,53] |
| Outcome | Benefit | Recipient |
|---|---|---|
| Improved well-being of individuals | Increased confidence/self-esteem | Individual |
| Reduced isolation | Individual | |
| Positive functioning (autonomy, control, aspirations) | Individual | |
| Emotional well-being | Individual | |
| Improved family well-being | Improved family relationships | Family |
| Positive functioning (autonomy, control, aspirations) | Family | |
| Emotional well-being | Family | |
| Improved community well-being | Sense of trust and belonging | Community |
| Positive functioning (autonomy, control, aspirations) | Community | |
| Improved relationships | Community | |
| Mental health | Reduced health cost of interventions | NHS/Individuals |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robinson, T.; Condell, J.; Ramsey, E.; Leavey, G. Self-Management of Subclinical Common Mental Health Disorders (Anxiety, Depression and Sleep Disorders) Using Wearable Devices. Int. J. Environ. Res. Public Health 2023, 20, 2636. https://doi.org/10.3390/ijerph20032636
Robinson T, Condell J, Ramsey E, Leavey G. Self-Management of Subclinical Common Mental Health Disorders (Anxiety, Depression and Sleep Disorders) Using Wearable Devices. International Journal of Environmental Research and Public Health. 2023; 20(3):2636. https://doi.org/10.3390/ijerph20032636
Chicago/Turabian StyleRobinson, Tony, Joan Condell, Elaine Ramsey, and Gerard Leavey. 2023. "Self-Management of Subclinical Common Mental Health Disorders (Anxiety, Depression and Sleep Disorders) Using Wearable Devices" International Journal of Environmental Research and Public Health 20, no. 3: 2636. https://doi.org/10.3390/ijerph20032636