1. Introduction
Although strong evidence shows that physical inactivity and sedentary behavior are associated with many adverse health effects, the “global pandemic” of inactive lifestyles is still on the rise [
1,
2]. Sedentary behavior is generally defined as any waking behavior with an energy expenditure ≤ 1.5 METs in a sitting or reclining posture, whereas physical inactivity is characterized by the lack of sufficient moderate- to vigorous-intensity physical activity [
3]. Sedentary behavior can therefore be seen as the lowest edge of the physical activity spectrum. An inactive lifestyle is associated with many adverse health effects including increased risk of coronary heart diseases, hypertension, type 2-diabetes, as well as cancer and reduced life expectancy [
1,
4,
5,
6,
7]. Furthermore, sedentary behavior increases markers associated with inflammation, the risk of obesity, depression, musculoskeletal diseases and osteoporosis risk for women [
8,
9,
10,
11,
12]. Physical inactivity and sedentary behavior cause not only morbidity and mortality, but also create a major economic burden, especially in high-income countries [
13].
A well-known factor associated with physical inactivity is urbanization, which is rapidly increasing worldwide. In 1970, only 36.6% of the world’s population lived in urban settlements. This number had risen to 55.3% in 2018 and is expected to reach 60.4% by 2030 [
14]. People living in urban areas are 26% more likely to have a sedentary lifestyle than people living in rural areas [
15]. Urbanization leads to a change in lifestyle because work and leisure time activities shift to indoor spaces, thus promoting a more sedentary lifestyle. Especially in high income countries, a significant decrease in physical activity was observed between 2001 (31.6%) and 2016 (36.8%). The same study also indicates that 27.5% of the population worldwide exhibits an insufficient physical activity level [
16]. Scientific evidence is growing that physical activity could eliminate or reduce the negative health effects of sedentary behavior, as it reduces the association of sitting time with all-cause mortality and cardiovascular disease mortality [
17]. Furthermore, regular physical activity improves immunosurveillance and immunocompetence, induces an anti-inflammatory effect, thus decreasing the risk of the development of non-communicable diseases, acute infection and even has a neuroprotective effect [
18]. Exercise may also influence the body’s reward system by altering neurotransmitter levels.
Growing cities displace nature and, as a consequence, people living in urban regions have restricted access to nature [
19], which could be in turn a factor in the vicious cycle of physical inactivity [
15]. People who visit local green spaces once a week are four times likelier to reach the recommended amount of physical activity than people who have no access to nature nearby [
20]. There is growing evidence that exposure to natural spaces (e.g., forests, blue and green spaces) has a wide range of positive health effects [
21,
22]. Three main domains of positive health effects through exposure to nature have been identified: (a) reduced exposure to air pollution, heat and noise, (b) restoring capacities, e.g., recovering from stress and (c) building capacities, e.g., encouraging physical activity [
23,
24]. Green exercise combines the synergistic effects of physical exercise and direct exposure to nature. Several studies found superior health effects of green exercise in comparison to indoor exercise, including better quality of life and mood, reduction of stress, improved cardiovascular health, greater enjoyment and less negative feelings like frustration and even a greater intent to repeat the exercise [
25,
26,
27,
28]. However, a recent systematic review could not provide enough high-quality evidence to support the superior health effects of green exercise, and shows the need for further research [
29]. Nevertheless, green exercise has one clear advantage over gym-based exercises as there are no restrictions to opening hours and no membership fees for exercising outdoors.
One popular green exercise activity is mountain hiking. Every year millions of people of all ages spend their holidays in the alpine regions and undertake hiking tours [
30]. Mountain hiking can be described as a long-lasting activity under moderate intensity [
31]. Although rest and recreation are still the main motives for vacation, physical activity during holidays has increased since the end of the 1990s. Hiking especially is gaining more and more popularity and represents an important travel motive [
32]. Looking at the recent fitness trends worldwide and in Europe, personal training is the most popular [
33,
34]. From this trend, it may be concluded that personal interaction and motivation are critical factors in promoting physical activities. Innovative health coaching approaches combining physical activity and coaching elements could be one way to counteract the global inactivity trend.
Health coaching is a valid method of health education and health promotion within a coaching context, to improve well-being and achieve health-related goals [
35]. Besides urbanization, another factor favoring inactivity is the lack of knowledge about the health-promoting effects of physical activity [
15]. In this context, health coaching could provide a valuable input, as health coaching can be seen as a combination of health education and behavioral change theory. It includes the following patient-centered methods: (a) identifying and setting personal goals, (b) self-reflection in personal motivational interviews and (c) explaining specific health-related aspects [
35,
36,
37]. Health coaching is a valid method with a full description of the technique for studies and is also causally related to a positive behavioral outcome [
37]. In recent years, coaching has grown in popularity in different application areas. Yet, there is also a lack of empirical studies that use control group designs to evaluate the effects of coaching programs [
38]. This method especially motivates adults to change their lifestyle, as it supports them in managing their personal goals [
39]. It leads to an improvement of physical and mental health and may enhance the quality of life [
40]. Most studies using health coaching concern chronic diseases such as diabetes type 2 [
39,
41]. So, there is a lack of research on the impact of coaching in people with predominantly sedentary lifestyles and the influence on health parameters, especially in terms of gender and age [
42].
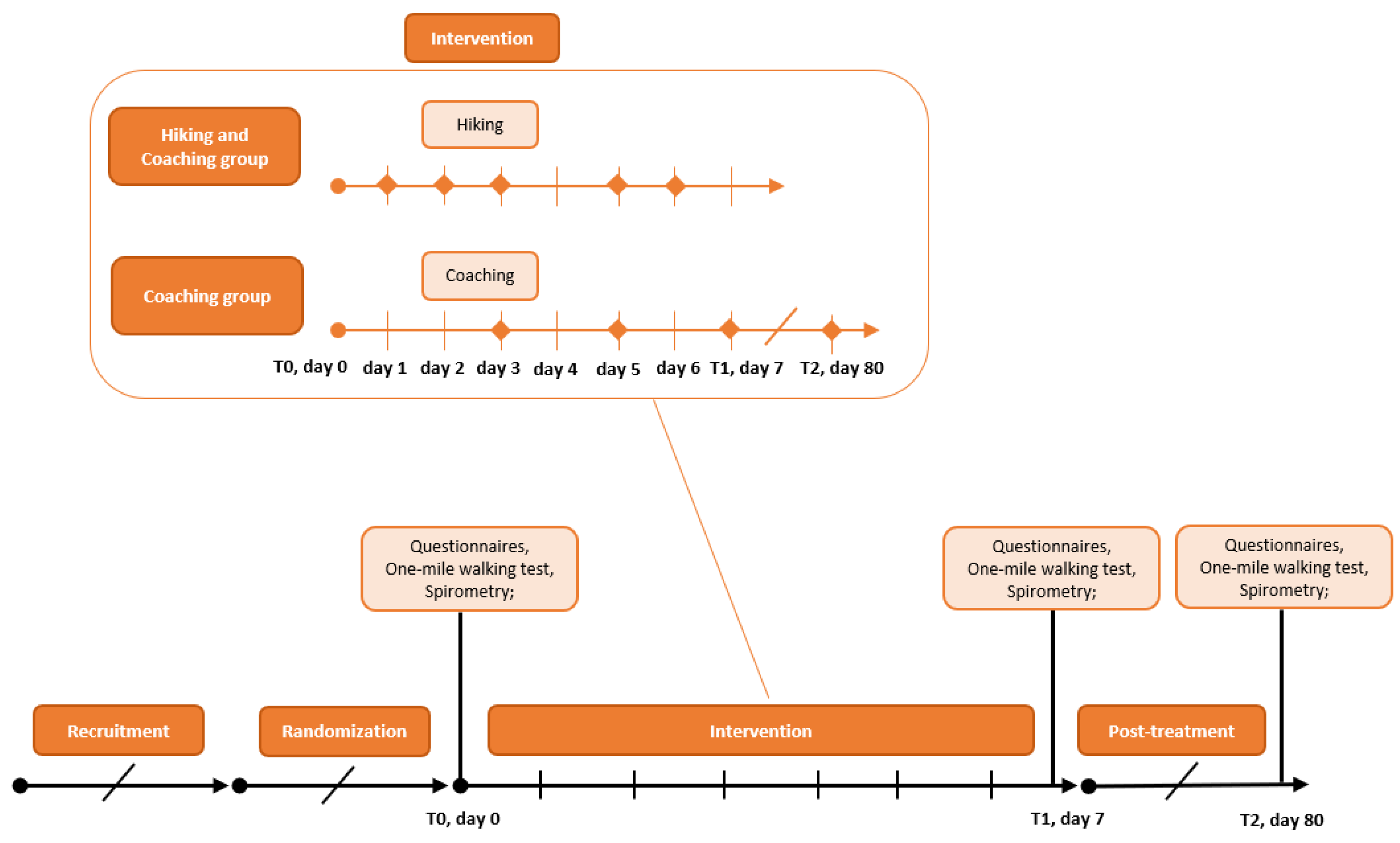
From the aspect that sedentary behavior at work is not sufficiently compensated during leisure time [
43], innovative approaches to promote the enjoyment of physical activity and thus encourage adherence to an active lifestyle supporting a healthy lifespan must be developed. Health coaching in combination with supervised green exercise could initiate long-lasting lifestyle changes. The aim of the presented HICO study was to investigate the effects of a 7-day intervention with green exercise and health coaching on cardiorespiratory fitness and quality of life of sedentary couples. To determine improvements in cardiorespiratory fitness, aerobic capacity and spirometry parameters were measured. For mental health enhancement, questionnaires EQ-5D-5L and SF-36 were provided. Hence, the following hypotheses are approached:
Hypothesis 1 (H1). The combination of hiking and coaching improves the cardiorespiratory fitness after 80 days more sustainably than hiking without coaching.
Hypothesis 2 (H2). The combination of hiking and coaching improves the cardiorespiratory fitness after seven days more than hiking without coaching.
Hypothesis 3 (H3). The combination of hiking and coaching improves the quality of life more than hiking without coaching.
4. Discussion
A wide range of adverse health effects is associated with sedentary behavior and physical inactivity. Urbanization and lifestyle changes promote an inactive lifestyle, leading to a global increase in chronic diseases [
17,
59,
60]. Therefore, new concepts are urgently needed to bring people back to an active and healthy lifestyle. Health coaching together with moderate mountain hiking as a sport that needs little equipment and personal skills could be instrumentalized to induce a more active lifestyle in the working population. The aim of the presented randomized, controlled trial is to examine the effects of moderate green exercise in form of mountain hiking and health coaching and on the cardiorespiratory fitness and quality of life of couples with a sedentary lifestyle.
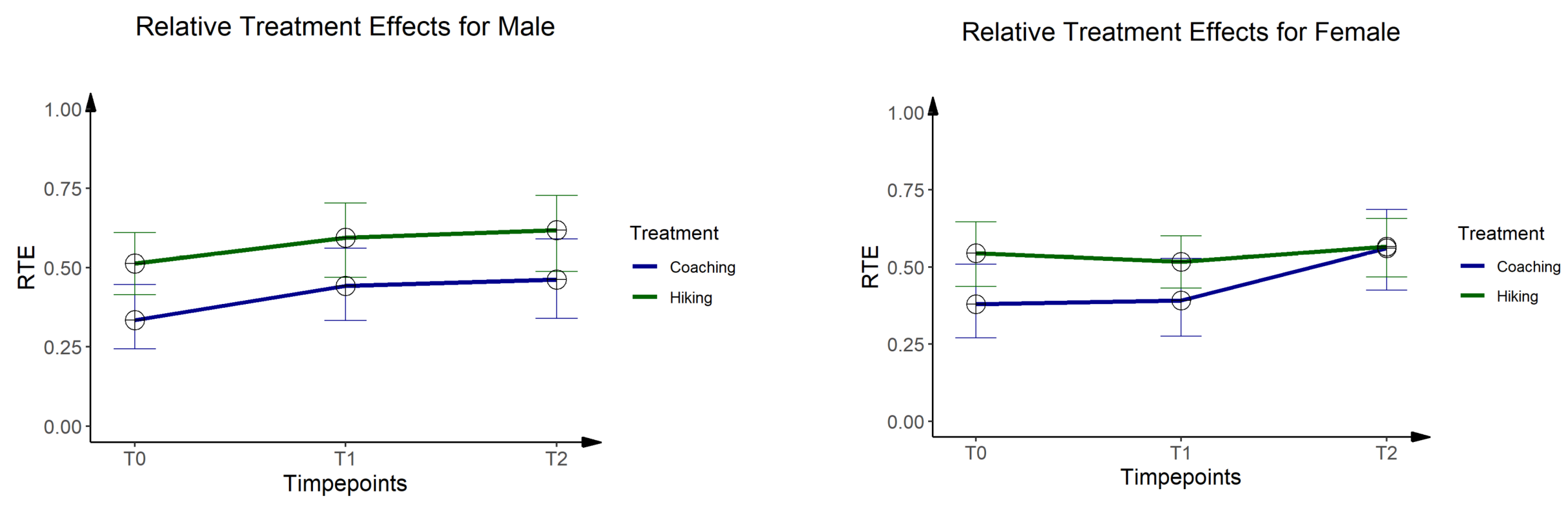
A valid parameter to evaluate cardiorespiratory fitness is spirometry. Within this population of sedentary couples, no significant changes were found for any spirometry parameter, neither as a short-term effect nor a long-term effect. Both groups start with a good lung function and keep this level throughout the intervention and post-treatment phases. As the baseline levels are already above average and the intervention duration is rather short, no relevant changes can be expected either way. Another well-established indicator of cardiorespiratory fitness is aerobic capacity. The direct measurement of aerobic capacity is very time and cost-intensive because of the need for trained staff and technical equipment [
61]. For this reason, we performed a less expensive but well-validated method instead: the one-mile walking test. In this submaximal exercise test, the participants are asked to walk one mile as fast as possible [
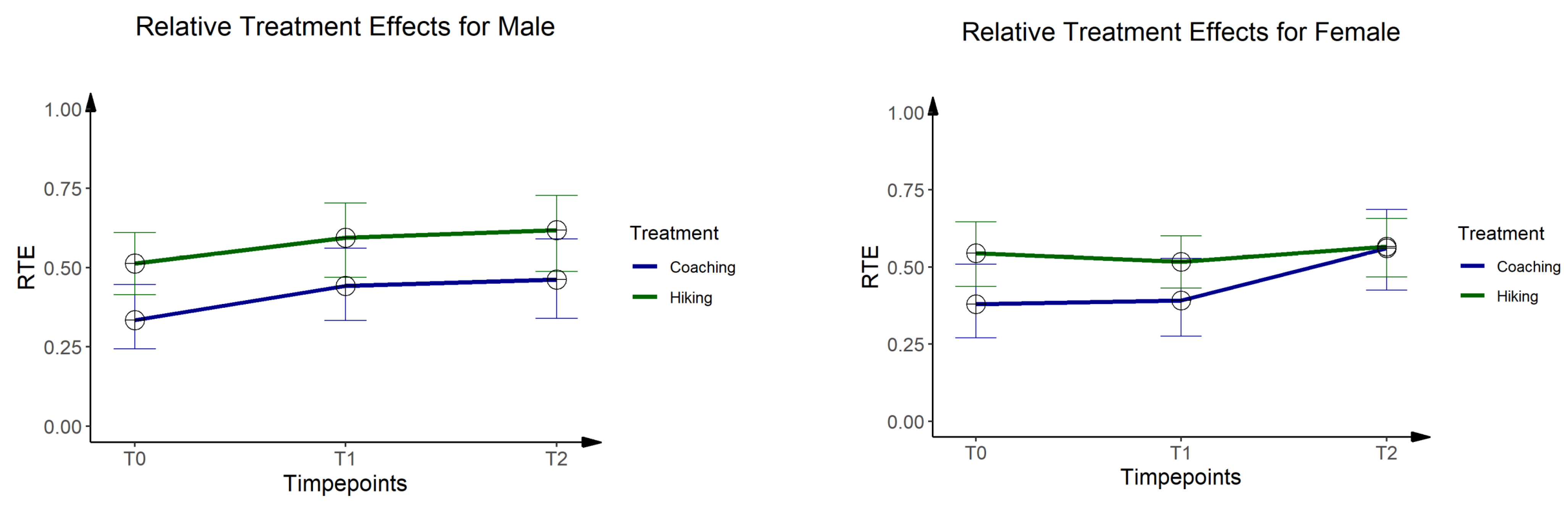
45]. The estimated aerobic capacity was analyzed separately for men and women. Although a significant baseline difference for aerobic capacity was found between the intervention groups, the statistical analysis revealed a significant time effect. The hiking group (9.89 ± 6.35 L/kg × min) starts with a higher aerobic capacity in comparison to the coaching group (44.04 ± 8.94 L/kg × min). During the 7-day intervention, the aerobic capacity is improved in both groups. However, the relative treatment effects indicate a stronger increase in the hiking group, which could be explained by the lower baseline values. Within the female subgroup, a significant time effect was detected, indicating a slight decrease of aerobic capacity in the hiking group during the 7-day intervention, followed by an increase during the post-treatment phase. In contrast, the aerobic capacity of the female participants of the coaching groups improves their aerobic capacity already during the intervention period and shows a clear increase during the post-treatment phase. This different development in the female subgroup is reflected by a significant interaction effect at day 80 (treat × time
p = 0.03). Although the changes in aerobic capacity occur in a minimal amount, it reveals a possible gender effect: females seem to be receptive to the health coaching approach.
Looking at
Hypothesis 1—The combination of hiking and coaching improves the cardiorespiratory fitness more sustainably than hiking without coaching this gender aspect must be considered. Women seem to have a better relation to their feelings and impulses and also tend to attribute their “wrong” behavior to internal causes due to a lack of knowledge and skills [
62]. Furthermore, women accept the activities and health recommendations of the coach more than men do, as Linning et al. [
63] show in their study on the promotion of fitness and health in employees. Thus, it is not unexpected that women rate their personal coaching process outcome more positively than men. Women seem to be more able to establish good working relations with the coach which also had a positive impact on the evaluation of coaching effectiveness [
64]. Other studies also found significant differences in gender because of the interpersonal variation in how people participate in and progress through a health coaching program [
65]. Apart from this gender-based coaching effect, further studies should also include the neurological aspects of (green) as Mason et al. [
66] show that a diet and exercise intervention with physical activity training can reduce reward-driven eating and, consequently, promote weight loss.
Within this study population of sedentary couples, no evidence was found to support Hypothesis 2—Combination of hiking and coaching improves cardiorespiratory fitness more than hiking without coaching. Although the aerobic capacity improves in the male subgroup during the 7-day intervention no superior effects were found for the coaching group. Furthermore, the changes in aerobic capacity are rather small. The baseline levels of spirometry are above average, and the aerobic capacity is also in a normal range. This leaves little space for improvements. However, the questionnaire by Johannsson and Westerterp [
45] should be critically evaluated as an inclusion criterion. In addition, no official German translation exists and the translation by the authors themselves may create a bias.
Besides cardiorespiratory fitness, health-related quality of life is an important patient-centered outcome. The SF-36 and the EQ-5D-5L were used for the measurement of the quality of life. The EQ-5D-5L index clearly shows that both groups rate their health status at baseline as already very good. Considering that the maximum score in the EQ-5D-5L index is 1, the average score of both groups of 0.97 leaves almost no room for improvement. However, a significant time effect (time p = 0.01) can be observed for the visual analogue scale, indicating a comparable improvement in both groups. The SF-36 questionnaire revealed significant changes over time without any relevant group or interaction effects. Significant time effects were observed for General Health (p = 0.01), Role Emotional (p = 0.01), Physical Dimension (p = 0.04), Mental Dimension (p = 0.03) and Total Score (p = 0.03), all indicating comparable improvements in both groups during the 7-day intervention. For the Physical Functioning and Physical Pain subscales, there is a significant group effect, which can be attributed to significant differences between the groups at baseline. For health-related quality of life, no indicators were found to support Hypothesis 3—The combination of hiking and coaching improves the quality of life more than hiking without coaching. Slight improvements in health-related quality of life can be observed in both groups, without any superior effect of coaching.
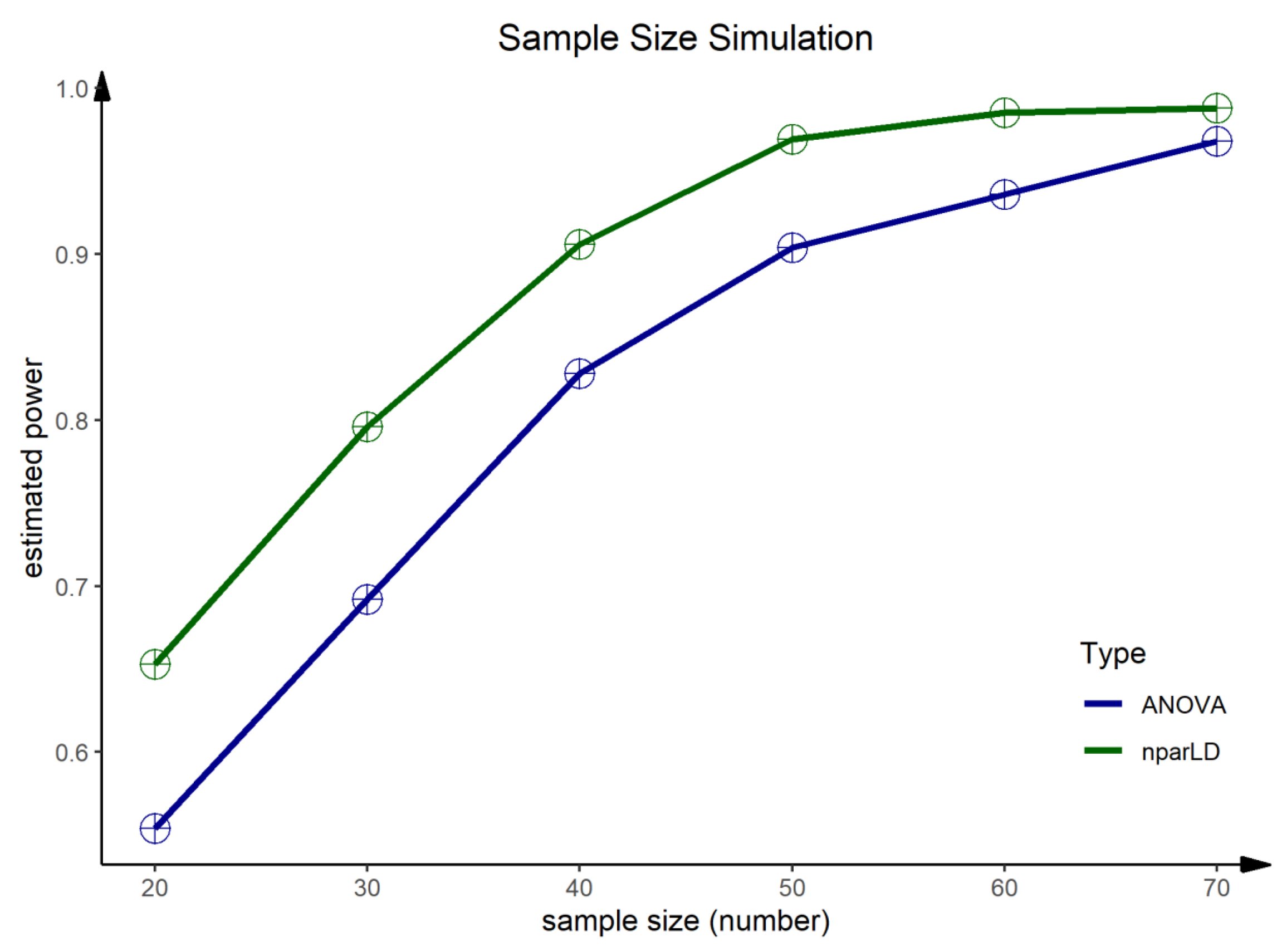
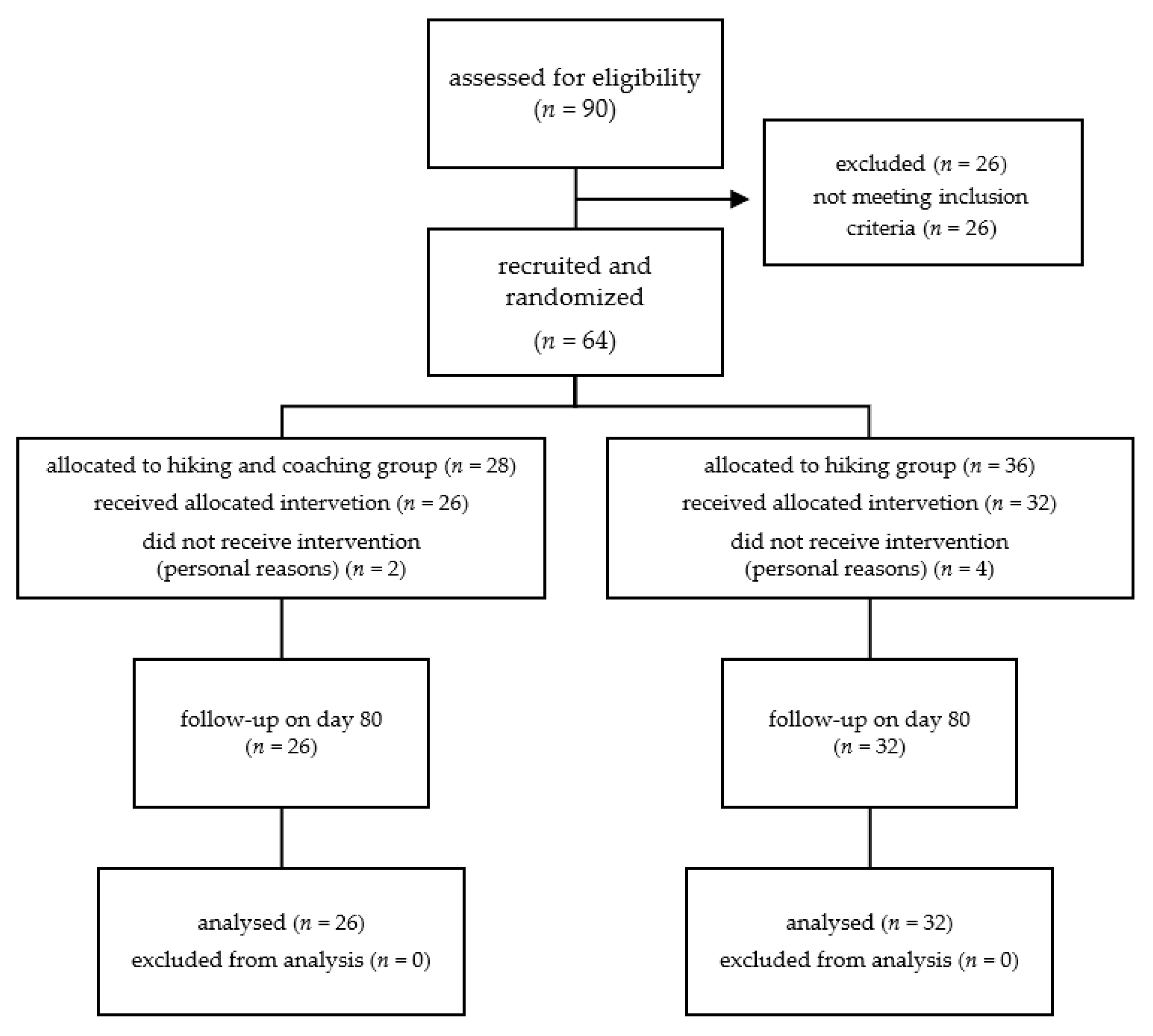
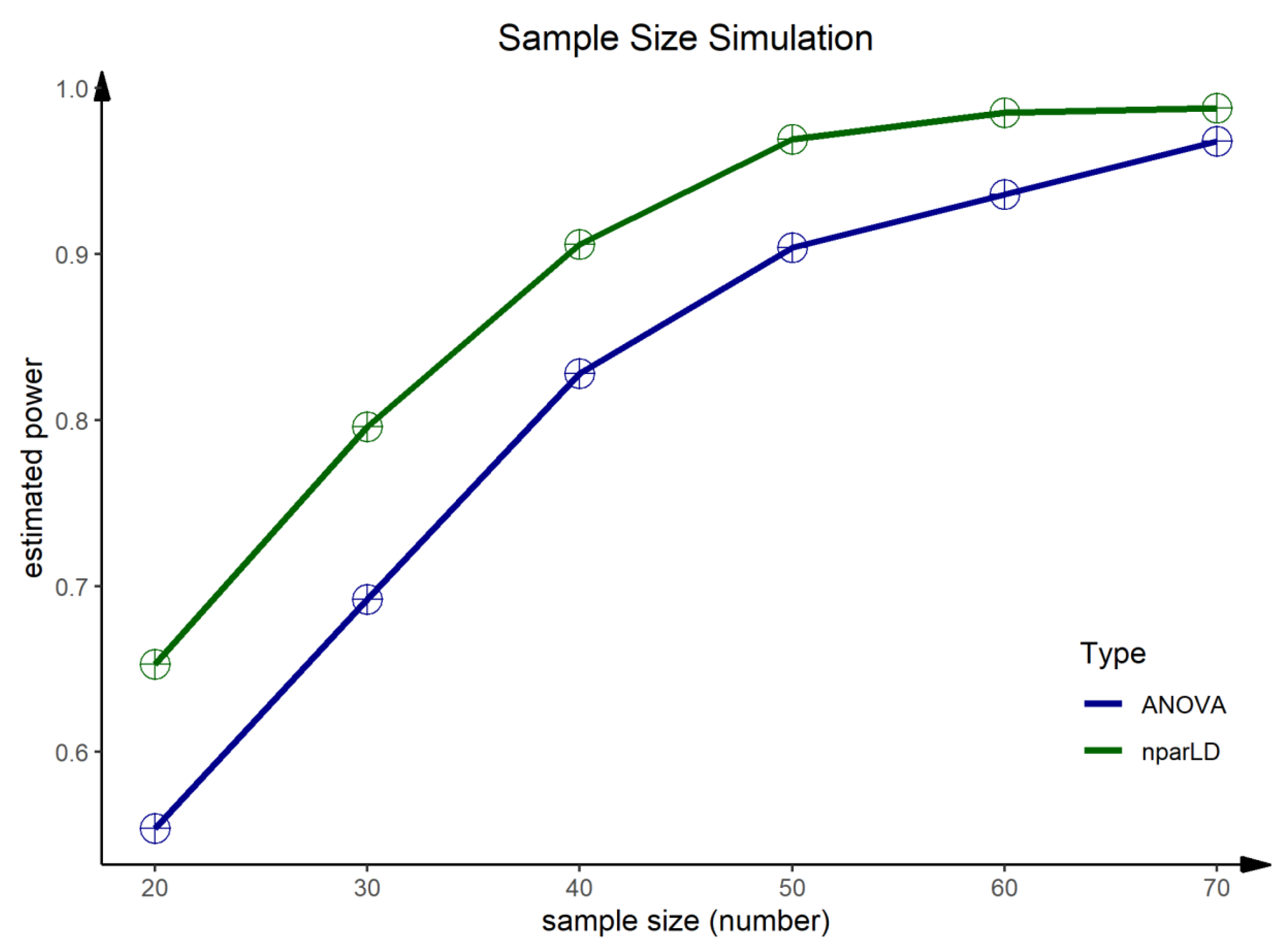
Further research is needed to evaluate the effects of health coaching on improving cardiorespiratory fitness, as our results are limited to a highly functioning sedentary population. Furthermore, the results need to be discussed in the context of the small sample size. As mentioned in the methodology, only two intervention groups were evaluated due to a high dropout rate and recruitment problems in the control group. However, since we have two randomly assigned intervention groups, the study design of a randomized, controlled trial remains. To keep the sample size as high as possible, missing values were reconstructed by the Last Observation Carried Forward Method (LOCF) and the Next Observation Carried Backward Method (NOCB), respectively. Hence, baseline values on day 0 and values on day 7 and day 80 were reconstructed, which might lead to biases in both the short-term and long-term effects due to the small sample size. Another bias within this study is the coaching itself—not only sympathy but also age and gender of the coaches could influence the impact of coaching and the effect of achieving personal goals [
57]. However, the presented data shows the feasibility of such approaches. Furthermore, we performed a post hoc sample size simulation to provide a data-based sample size estimation for further studies. The sample size simulation was performed for aerobic capacity with both nonparametric (F1-LD-F1) and parametric models (ANOVA). A sample size of
n ≥ 60 people should be reached for such study designs to obtain an estimated power of 1 − β ≥ 0.94.



 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}