
Intercostal Muscles Oxygenation and Breathing Pattern during Exercise in Competitive Marathon Runners

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of Study and Participants
2.2. Procedures
2.3. Ergospirometry
2.4. Triphasic Model of Exercise Intensity Determined by Ventilatory Thresholds
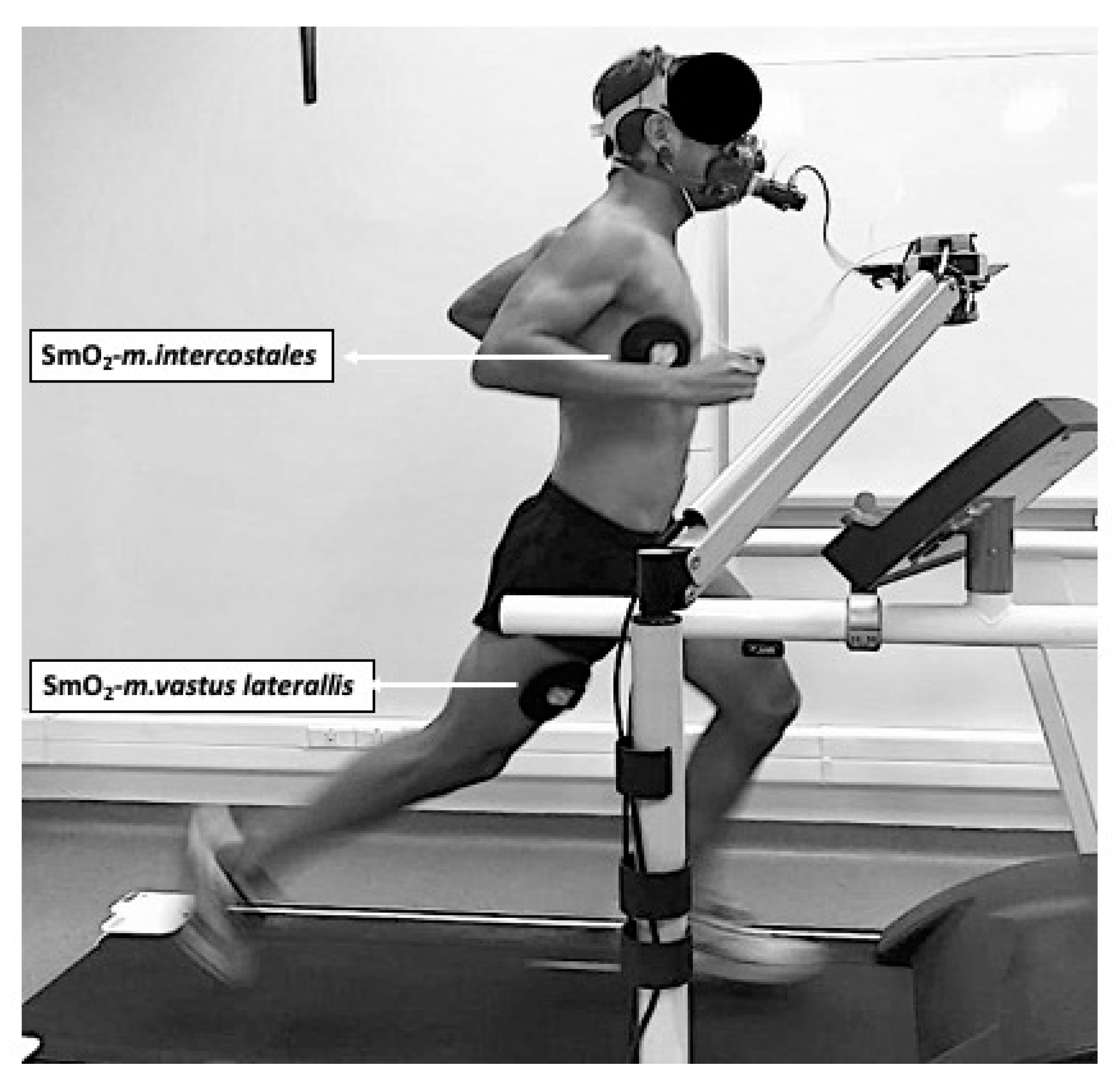
2.5. Measurement of SmO2
2.6. Breathing Pattern
2.7. Data Analysis
2.8. Statistical Analysis
3. Results
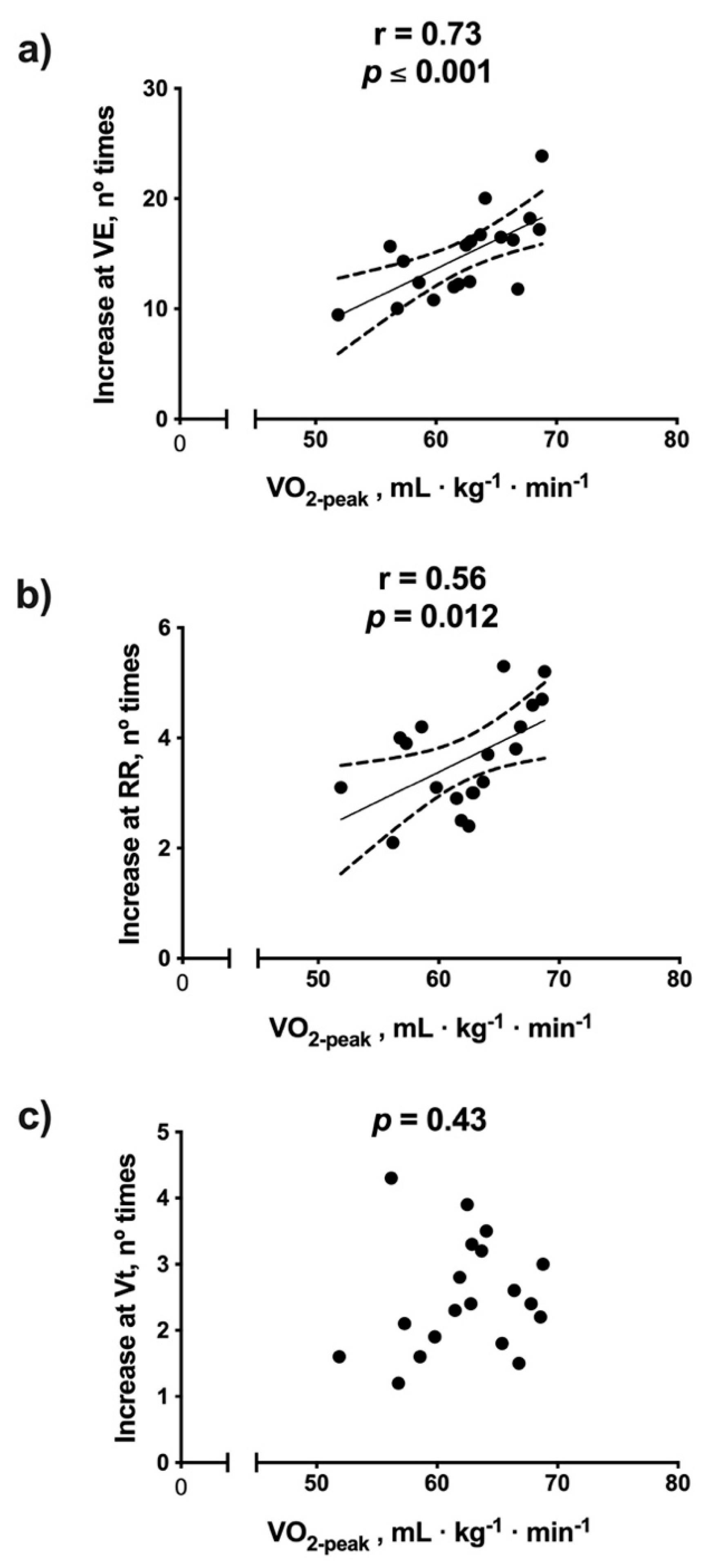
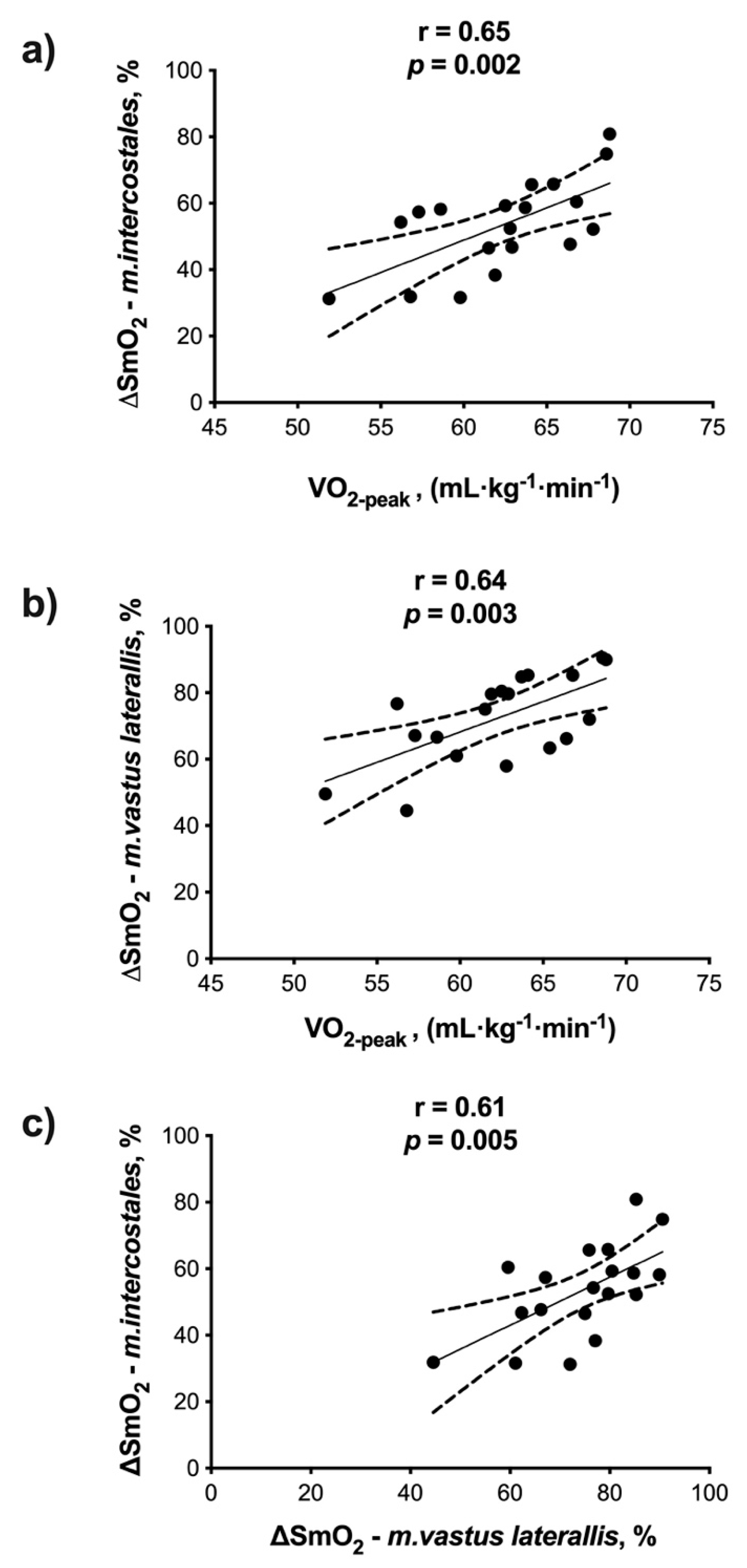
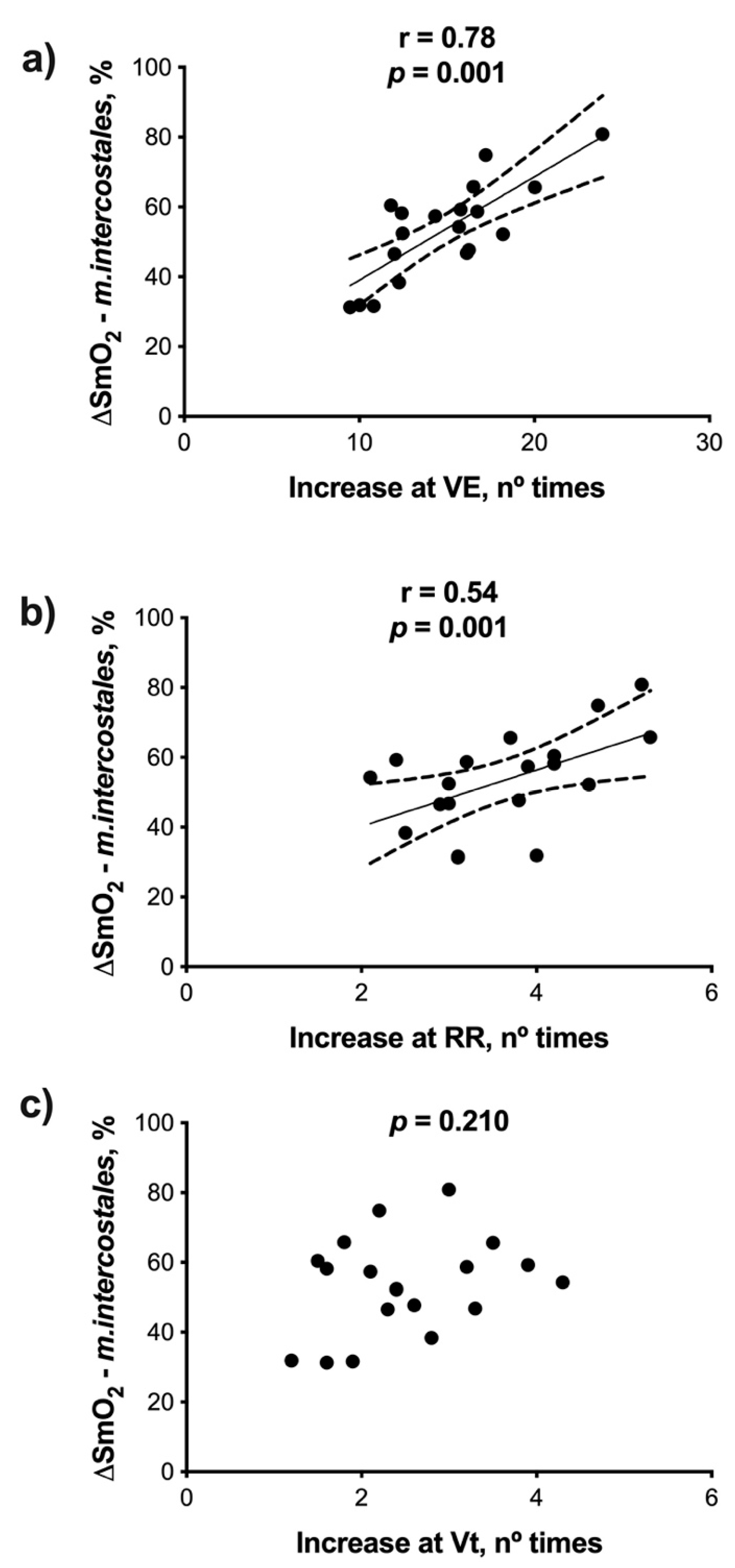
3.1. Correlations
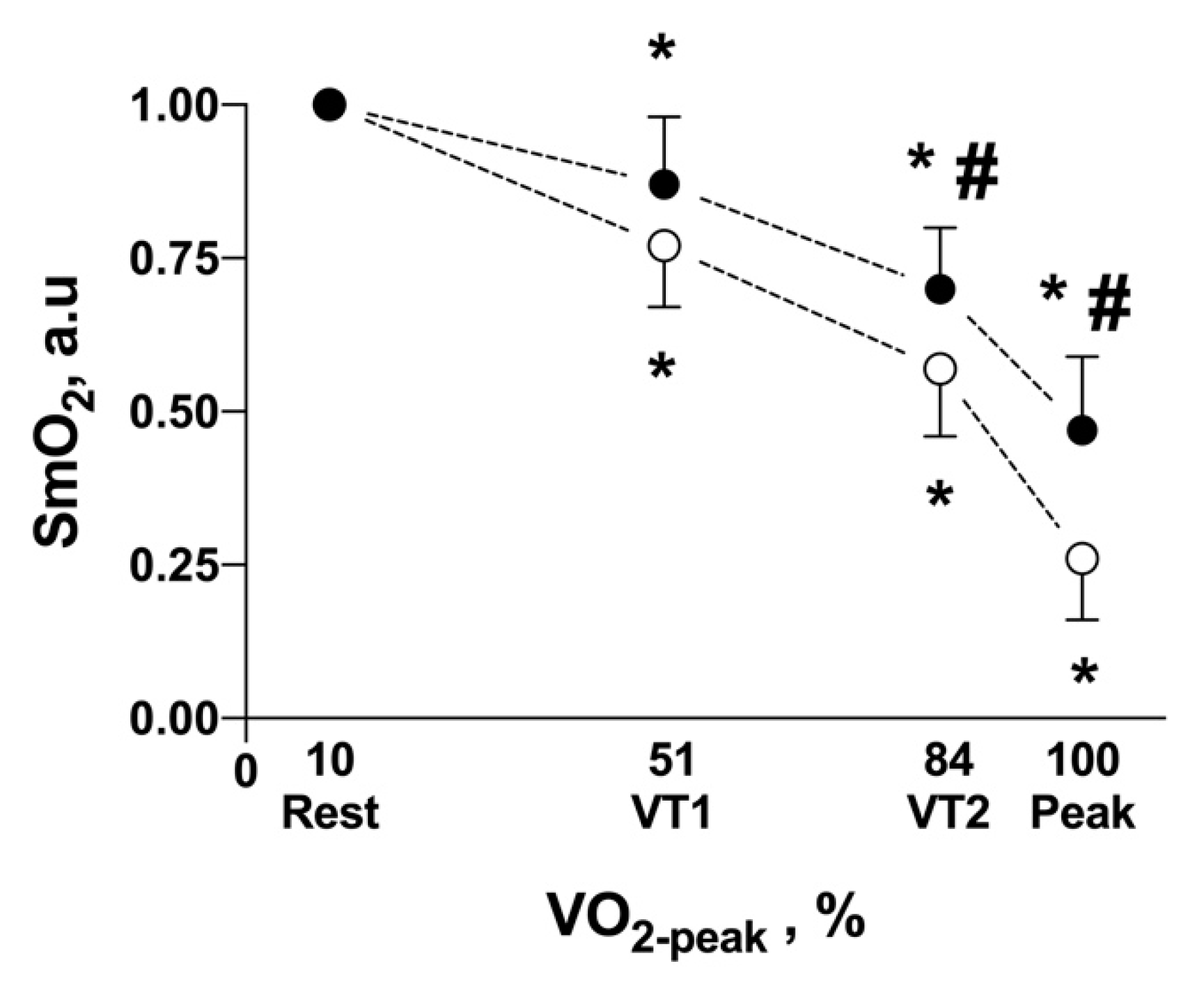
3.2. Triphasic Model of Exercise Intensity and SmO2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Tiller, N.B. Pulmonary and Respiratory Muscle Function in Response to Marathon and Ultra-Marathon Running: A Review. Sports Med. 2019, 49, 1031–1041. [Google Scholar] [CrossRef] [Green Version]
- Dominelli, P.B.; Molgat-Seon, Y.; Griesdale, D.E.G.; Peters, C.M.; Blouin, J.S.; Sekhon, M.; Dominelli, G.S.; Henderson, W.R.; Foster, G.E.; Romer, L.M.; et al. Exercise-induced quadriceps muscle fatigue in men and women: Effects of arterial oxygen content and respiratory muscle work. J. Physiol. 2017, 595, 5227–5244. [Google Scholar] [CrossRef]
- Boushel, R. Muscle metaboreflex control of the circulation during exercise. Acta Physiol. 2010, 199, 367–383. [Google Scholar] [CrossRef]
- Sheel, A.W.; Romer, L.M. Ventilation and respiratory mechanics. Compr. Physiol. 2012, 2, 1093–1142. [Google Scholar]
- Naranjo, J.; Centeno, R.A.; Galiano, D.; Beaus, M. A nomogram for assessment of breathing patterns during treadmill exercise. Br. J. Sports Med. 2005, 39, 80–83. [Google Scholar] [CrossRef] [Green Version]
- Elliott, A.D.; Grace, F. An examination of exercise mode on ventilatory patterns during incremental exercise. Eur. J. Appl. Physiol. 2010, 110, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Tanner, D.A.; Duke, J.W.; Stager, J.M. Ventilatory patterns differ between maximal running and cycling. Respir. Physiol. Neurobiol. 2014, 191, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Alfonsi, E.; Pavesi, R.; Merlo, I.M.; Gelmetti, A.; Zambarbieri, D.; Lago, P.; Arrigo, A.; Reggiani, C.; Moglia, A. Hemoglobin near-infrared spectroscopy and surface EMG study in muscle ischaemia and fatiguing isometric contraction. J. Sports Med. Phys. Fit. 1999, 39, 83–92. [Google Scholar]
- Perrey, S.; Ferrari, M. Muscle Oximetry in Sports Science: A Systematic Review. Sports Med. 2018, 48, 597–616. [Google Scholar] [CrossRef]
- Alvares, T.S.; Oliveira, G.V.; Soares, R.; Murias, J.M. Near-infrared spectroscopy-derived total haemoglobin as an indicator of changes in muscle blood flow during exercise-induced hyperaemia. J. Sports Sci. 2020, 38, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Quaresima, V.; Lepanto, R.; Ferrari, M. The use of near infrared spectroscopy in sports medicine. J. Sports Med. Phys. Fit. 2003, 43, 1–13. [Google Scholar]
- Turner, L.A.; Tecklenburg-Lund, S.; Chapman, R.F.; Stager, J.M.; Duke, J.W.; Mickleborough, T.D. Inspiratory loading and limb locomotor and respiratory muscle deoxygenation during cycling exercise. Respir. Physiol. Neurobiol. 2013, 185, 506–514. [Google Scholar] [CrossRef]
- Dominelli, P.B.; Archiza, B.; Ramsook, A.H.; Mitchell, R.A.; Peters, C.M.; Molgat-Seon, Y.; Henderson, W.R.; Koehle, M.S.; Boushel, R.; Sheel, A.W. Effects of respiratory muscle work on respiratory and locomotor blood flow during exercise. Exp. Physiol. 2017, 102, 1535–1547. [Google Scholar] [CrossRef] [Green Version]
- Guazzi, M.; Adams, V.; Conraads, V.; Halle, M.; Mezzani, A.; Vanhees, L.; Fletcher, G.F.; Forman, D.E.; Kitzman, D.W.; Carl, J.; et al. EACPR/AHA Scientific Statement. Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Circulation 2012, 126, 2261–2274. [Google Scholar] [CrossRef]
- Seiler, K.S.; Kjerland, G.O. Quantifying training intensity distribution in elite endurance athletes: Is there evidence for an “optimal” distribution? Scand. J. Med. Sci. Sports 2006, 16, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Vainshelboim, B.; Rao, S.; Chan, K.; Lima, R.M.; Ashley, E.A.; Myers, J. A comparison of methods for determining the ventilatory threshold: Implications for surgical risk stratification. Can. J. Anaesth. 2017, 64, 634–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, J.R.; Rossiter, H.B.; Coats, E.M.; Skasick, A.; Whipp, B.J. The maximally attainable VO2 during exercise in humans: The peak vs. maximum issue. J. Appl. Physiol. 2003, 95, 1901–1907. [Google Scholar] [CrossRef] [Green Version]
- Austin, K.G.; Daigle, K.A.; Patterson, P.; Cowman, J.; Chelland, S.; Haymes, E.M. Reliability of near-infrared spectroscopy for determining muscle oxygen saturation during exercise. Res. Q. Exerc. Sport 2005, 76, 440–449. [Google Scholar] [CrossRef] [PubMed]
- McManus, C.J.; Collison, J.; Cooper, C.E. Performance comparison of the MOXY and PortaMon near-infrared spectroscopy muscle oximeters at rest and during exercise. J. Biomed. Opt. 2018, 23, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Contreras-Briceno, F.; Espinosa-Ramirez, M.; Hevia, G.; Llambias, D.; Carrasco, M.; Cerda, F.; López-Fuenzalida, A.; García, P.; Gabrielli, L.; Viscor, G. Reliability of NIRS portable device for measuring intercostal muscles oxygenation during exercise. J. Sports Sci. 2019, 37, 2653–2659. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Basoudan, N.; Melo, L.T.; Wickerson, L.; Brochard, L.J.; Goligher, E.C.; Reid, W.D. Deoxygenation of inspiratory muscles during cycling, hyperpnoea and loaded breathing in health and disease: A systematic review. Clin. Physiol. Funct. Imaging 2018, 38, 554–565. [Google Scholar] [CrossRef] [PubMed]
- Tipton, M.J.; Harper, A.; Paton, J.F.R.; Costello, J.T. The human ventilatory response to stress: Rate or depth? J. Physiol. 2017, 595, 5729–5752. [Google Scholar] [CrossRef] [PubMed]
- Nicolo, A.; Girardi, M.; Bazzucchi, I.; Felici, F.; Sacchetti, M. Respiratory frequency and tidal volume during exercise: Differential control and unbalanced interdependence. Physiol. Rep. 2018, 6, e13908. [Google Scholar] [CrossRef] [Green Version]
- Green, D.J.; Spence, A.; Rowley, N.; Thijssen, D.H.; Naylor, L.H. Vascular adaptation in athletes: Is there an “athlete’s artery”? Exp. Physiol. 2012, 97, 295–304. [Google Scholar] [CrossRef] [Green Version]
- Foster, G.E.; Koehle, M.S.; Dominelli, P.B.; Mwangi, F.M.; Onywera, V.O.; Boit, M.K.; Tremblay, J.C.; Boit, C.; Sheel, A.W. Pulmonary mechanics and gas exchange during exercise in Kenyan distance runners. Med. Sci. Sports Exerc. 2014, 46, 702–710. [Google Scholar] [CrossRef]
- Nicolo, A.; Massaroni, C.; Passfield, L. Respiratory Frequency during Exercise: The Neglected Physiological Measure. Front. Physiol. 2017, 8, 922. [Google Scholar] [CrossRef]
- Nicolo, A.; Marcora, S.M.; Sacchetti, M. Time to reconsider how ventilation is regulated above the respiratory compensation point during incremental exercise. J. Appl. Physiol. 2020, 128, 1447–1449. [Google Scholar] [CrossRef] [PubMed]
- Moreno, A.M.; Toledo-Arruda, A.C.; Lima, J.S.; Duarte, C.S.; Villacorta, H.; Nobrega, A.C.L. Inspiratory Muscle Training Improves Intercostal and Forearm Muscle Oxygenation in Patients with Chronic Heart Failure: Evidence of the Origin of the Respiratory Metaboreflex. J. Card Fail. 2017, 23, 672–679. [Google Scholar] [CrossRef]
- Turner, L.A.; Tecklenburg-Lund, S.L.; Chapman, R.; Shei, R.J.; Wilhite, D.P.; Mickleborough, T. The Effect of Inspiratory Muscle Training on Respiratory and Limb Locomotor Muscle Deoxygenation During Exercise with Resistive Inspiratory Loading. Int. J. Sports Med. 2016, 37, 598–606. [Google Scholar] [CrossRef]
- Archiza, B.; Andaku, D.K.; Caruso, F.C.R.; Bonjorno, J.C., Jr.; Oliveira, C.R.; Ricci, P.A.; Amaral, A.C.d.; Mattiello, S.M.; Libardi, C.A.; Phillips, S.A.; et al. Effects of inspiratory muscle training in professional women football players: A randomized sham-controlled trial. J. Sports Sci. 2018, 36, 771–780. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phases | ||||
|---|---|---|---|---|
| Variables | Rest | VT1 | VT2 | O2-peak |
| O2 (mL·kg−1·min−1) | 6.35 ± 0.75 | 31.30 ± 4.15 * | 52.01 ± 3.91 * | 62.32 ± 4.65 * |
| SmO2−m.intercostales (%) | 74.6 ± 10.7 | 65.1 ± 12.6 * | 52.9 ± 11.4 * | 35.2 ± 12.8 * |
| ∆SmO2−m.intercostales (%) | - | - | - | 53.4 ± 13.9 |
| SmO2−m.vastus lateralis (%) | 63.2 ± 10.9 | 48.7 ± 9.6 * | 36.1 ± 10.2 * | 17.1 ± 7.5 * |
| ∆SmO2−m.vastus lateralis (%) | - | - | - | 72.4 ± 13.5 |
| THb m.intercostales (g·dL−1) | 12.4 ± 0.5 | 12.4 ± 0.5 | 12.4 ± 0.5 | 12.3 ± 0.6 |
| THb m.vastus laterallis (g·dL−1) | 12.6 ± 0.4 | 12.5 ± 0.5 | 12.4 ± 0.5 | 12.6 ± 0.6 |
| E (L·min−1) | 10.4 ± 2.5 | 43.2 ± 10.2 * | 99.5 ± 18.1 * | 158.8 ± 18.9 * |
| RR (bpm) | 13.1 ± 1.7 | 25.3 ± 6.7 * | 40.7 ± 7.6 * | 59.3 ± 8.4 * |
| Vt (L) | 0.81 ± 0.20 | 1.75 ± 0.41 * | 2.47 ± 0.43 * | 2.71 ± 0.30 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Contreras-Briceño, F.; Espinosa-Ramírez, M.; Moya-Gallardo, E.; Fuentes-Kloss, R.; Gabrielli, L.; Araneda, O.F.; Viscor, G. Intercostal Muscles Oxygenation and Breathing Pattern during Exercise in Competitive Marathon Runners. Int. J. Environ. Res. Public Health 2021, 18, 8287. https://doi.org/10.3390/ijerph18168287
Contreras-Briceño F, Espinosa-Ramírez M, Moya-Gallardo E, Fuentes-Kloss R, Gabrielli L, Araneda OF, Viscor G. Intercostal Muscles Oxygenation and Breathing Pattern during Exercise in Competitive Marathon Runners. International Journal of Environmental Research and Public Health. 2021; 18(16):8287. https://doi.org/10.3390/ijerph18168287
Chicago/Turabian StyleContreras-Briceño, Felipe, Maximiliano Espinosa-Ramírez, Eduardo Moya-Gallardo, Rodrigo Fuentes-Kloss, Luigi Gabrielli, Oscar F. Araneda, and Ginés Viscor. 2021. "Intercostal Muscles Oxygenation and Breathing Pattern during Exercise in Competitive Marathon Runners" International Journal of Environmental Research and Public Health 18, no. 16: 8287. https://doi.org/10.3390/ijerph18168287